Princípios Fundamentais da Oncologia Cirúrgica Digestiva
Uma Abordagem Contemporânea e Baseada em Evidências
O Cenário Atual do Câncer Digestivo no Brasil
A Cirurgia do Aparelho Digestivo vive um momento de transformação sem precedentes. Não somos mais apenas “técnicos de ressecção”, mas parte integrante de uma complexa engrenagem multidisciplinar. A relevância deste tema é sublinhada pelos dados epidemiológicos alarmantes. Se no passado nos baseávamos em estimativas modestas, hoje a realidade é desafiadora: segundo a Estimativa 2023-2025 do Instituto Nacional de Câncer (INCA), esperam-se 704 mil casos novos de câncer por ano no Brasil.
Destaque-se que as neoplasias do trato gastrointestinal ocupam posições cimeiras. O câncer colorretal figura como o segundo mais incidente em mulheres e homens na maioria das regiões, com cerca de 45 mil novos casos anuais, seguido de perto pelo câncer de estômago (21 mil casos) e esôfago. Estes números não são apenas estatísticas; representam uma demanda crescente por cirurgiões oncológicos altamente qualificados, capazes de compreender não apenas a anatomia, mas a biologia tumoral.
A Biologia como Norte da Técnica Cirúrgica
Fisiopatologia e Disseminação
O entendimento clássico da cirurgia oncológica, herdado dos princípios de William Halsted no final do século XIX, baseava-se na premissa de que o câncer era uma doença puramente local que se disseminava centrifugamente. Embora a radicalidade (ressecção em bloco) permaneça um pilar, hoje compreendemos a doença como sistêmica desde fases precoces em muitos casos.
A disseminação ocorre por três vias principais que o cirurgião deve dominar:
- Linfática: Predominante em carcinomas (ex: adenocarcinoma gástrico e cólon).
- Hematogênica: Preferencial em sarcomas e carcinomas avançados (fígado e pulmões como sítios-alvo).
- Transcelômica (Peritoneal): Comum em neoplasias gástricas T3/T4, ovário e apêndice, exigindo estratégias específicas como a peritoniectomia.
O Princípio da Radicalidade e Margens (R0)
O objetivo primário da cirurgia oncológica curativa é a ressecção R0 (ausência de doença residual macroscópica e microscópica). A cirurgia R1 (doença microscópica residual) ou R2 (macroscópica) impacta drasticamente o prognóstico.
- Ressecção em Bloco: O tumor nunca deve ser violado. A peça deve ser removida envolta por tecido saudável, respeitando as fáscias anatômicas e os pedículos vasculares na sua origem.
- Linfadenectomia: Não serve apenas para estadiamento, mas tem papel terapêutico. No câncer gástrico, por exemplo, a linfadenectomia D2 é o padrão-ouro em centros especializados, associada a menor recidiva locorregional.
Neoadjuvância vs. Adjuvância
A decisão entre operar primeiro (upfront surgery) ou indicar terapia neoadjuvante é um dos grandes debates atuais.
- Vantagens da Neoadjuvância: Tratamento precoce de micrometástases, redução do tumor (downstaging) facilitando a ressecção R0 e teste in vivo da quimiossensibilidade. É o padrão atual para câncer de esôfago localmente avançado e câncer de reto médio/baixo.
- Vantagens da Adjuvância: Baseada no estadiamento patológico preciso (pTNM), evitando tratamento excessivo em estádios precoces.
Aplicação Prática na Cirurgia Digestiva
A prática moderna exige que o cirurgião diferencie dois conceitos cruciais frequentemente confundidos: Ressecabilidade e Operabilidade.
- Ressecabilidade: É uma característica do tumor (relação com estruturas vitais).
- Operabilidade: É uma característica do paciente (reserva funcional, comorbidades, status performance). Um tumor pode ser ressecável, mas o paciente inoperável.
O Papel da Citorredução e HIPEC
Para a carcinomatose peritoneal, historicamente considerada uma condição terminal, houve uma mudança de paradigma. Em neoplasias selecionadas (como pseudomixoma peritoneal, mesotelioma e alguns casos de câncer colorretal), a combinação de Cirurgia de Citorredução (Peritoniectomia) com Quimioterapia Intraperitoneal Hipertérmica (HIPEC) tem oferecido sobrevida em longo prazo, transformando uma doença fatal em uma condição crônica tratável.
Planejamento Multidisciplinar
O cirurgião oncológico não atua isolado. A discussão em Tumor Boards é mandatória. A indicação cirúrgica deve considerar a biologia molecular (ex: status do gene APC em colorretal, superexpressão de HER2 em gástrico) e a resposta a terapias sistêmicas.
Pontos-Chave para a Prática Cirúrgica
- Estadiamento Preciso: Nunca leve um paciente à sala sem um estadiamento completo. A laparoscopia diagnóstica é fundamental em tumores gástricos e pancreáticos para evitar laparotomias desnecessárias em casos de carcinomatose oculta.
- Margens Cirúrgicas: A margem circunferencial (radial) no câncer de reto e a margem proximal no câncer gástrico e esofágico são preditores independentes de sobrevida.
- Manuseio da Peça (“No-touch technique”): Evite a manipulação direta do tumor. A ligadura vascular prévia e a mobilização cuidadosa previnem a embolização tumoral intraoperatória.
- Documentação: O relatório cirúrgico deve detalhar as cadeias linfáticas dissecadas e as estruturas preservadas ou ressecadas, orientando o patologista e o oncologista clínico.
Perspectivas Futuras
A cirurgia digestiva na sua área de atuação oncológica evoluiu de amputações extensas para procedimentos de precisão, muitas vezes minimamente invasivos (laparoscópicos ou robóticos), sem perder a radicalidade oncológica. O futuro aponta para uma integração ainda maior com a biologia molecular e a imunoterapia. O cirurgião do futuro deverá ser, antes de tudo, um oncologista que opera: alguém que entende que o bisturi é apenas uma das armas, e que saber quando não operar é tão vital quanto a técnica operatória refinada.
Como nos ensinou o pai da cirurgia oncológica moderna:
“O cirurgião deve ser o médico do paciente oncológico, e não apenas o técnico que remove o tumor.” — William Stewart Halsted
Hashtags
#CirurgiaDigestiva #OncologiaCirurgica #EducaçãoMédica #ResidenciaCirurgia #CancerDigestivo
Gostou? ❔ Nos deixe um comentário ✍️, compartilhe em suas redes sociais e/ou mande sua dúvida pelo 💬 Chat Online em nossa DM do Instagram.
Acesso à Oncologia Cirúrgica no Brasil
Desafios e Oportunidades
Introdução
A oncologia cirúrgica desempenha um papel fundamental no tratamento de diversas neoplasias, especialmente no que diz respeito ao aparelho digestivo, onde tumores como os de esôfago, estômago e cólon são comuns. No Brasil, o acesso a serviços de oncologia cirúrgica varia significativamente entre as diferentes regiões do país, refletindo desigualdades socioeconômicas e estruturais. Este texto abordará a situação atual da oncologia cirúrgica no Brasil, analisando os desafios enfrentados e as oportunidades para melhorar o acesso e a qualidade do tratamento.
Contexto Atual da Oncologia Cirúrgica no Brasil
O Brasil enfrenta um cenário complexo em relação ao tratamento do câncer. De acordo com dados do Sistema de Informações sobre Mortalidade (SIM), entre 2002 e 2021, 82,3% das mortes por câncer ocorreram em hospitais, enquanto apenas 17,7% ocorreram em casa. Essa disparidade é alarmante, pois indica que muitos pacientes não estão recebendo o suporte necessário em suas últimas etapas de vida, refletindo a falta de um sistema robusto de cuidados paliativos e a dificuldade de acesso a tratamentos adequados. As regiões do Norte e Nordeste apresentam taxas significativamente mais altas de mortes em casa, com 30,2% e 24,8%, respectivamente, em comparação com 12,2% no Sudeste. Essa situação é agravada pela escassez de recursos e pela falta de equipes de saúde especializadas em cuidados paliativos, o que limita as opções de tratamento e suporte para os pacientes.
Desafios no Acesso à Oncologia Cirúrgica
Os principais desafios enfrentados na oncologia cirúrgica no Brasil incluem:
- Desigualdade Regional: As disparidades no acesso a serviços de saúde são evidentes, com as regiões mais pobres enfrentando dificuldades significativas em obter tratamento cirúrgico adequado. O Índice de Desenvolvimento Humano (IDH) das regiões está diretamente correlacionado com a taxa de mortes em casa, indicando que áreas com menor IDH tendem a ter menos acesso a cuidados de saúde adequados.
- Falta de Infraestrutura: Muitas unidades de saúde carecem de infraestrutura adequada para realizar procedimentos cirúrgicos complexos. Isso resulta em um número elevado de pacientes que não recebem tratamento cirúrgico oportuno, aumentando a mortalidade.
- Educação e Conscientização: A falta de informação sobre os sinais e sintomas do câncer e a importância do diagnóstico precoce contribui para que muitos pacientes busquem atendimento apenas em estágios avançados da doença.
Aplicação na Cirurgia Digestiva
Na cirurgia do aparelho digestivo, a intervenção precoce é crucial para melhorar os resultados e a sobrevida dos pacientes. A realização de cirurgias em estágios iniciais de câncer pode reduzir significativamente a mortalidade. Contudo, a realidade é que muitos pacientes chegam ao tratamento cirúrgico em estágios avançados, onde as opções são limitadas e os resultados são menos favoráveis. Estudos demonstram que a implementação de programas de triagem e educação em saúde pode aumentar a detecção precoce de cânceres digestivos, melhorando a taxa de sobrevivência e reduzindo as complicações associadas a intervenções tardias.
Pontos-Chave
- Desigualdade no Acesso: Há uma necessidade urgente de políticas públicas que abordem as disparidades regionais no acesso à oncologia cirúrgica.
- Educação em Saúde: Aumentar a conscientização sobre câncer e sua detecção precoce é vital para melhorar os resultados.
- Integração de Cuidados: A criação de uma rede de cuidados que inclua oncologia cirúrgica, cuidados paliativos e suporte psicológico pode melhorar a qualidade de vida dos pacientes.
Conclusões
O acesso à oncologia cirúrgica no Brasil é um desafio multifacetado que requer uma abordagem integrada e colaborativa. É fundamental que os cirurgiões digestivos, juntamente com outros profissionais de saúde, trabalhem para promover a conscientização, melhorar a infraestrutura e garantir que todos os pacientes tenham acesso a tratamentos adequados e oportunos. A implementação de políticas públicas focadas na equidade em saúde é essencial para transformar o cenário atual e garantir que todos os brasileiros tenham a oportunidade de receber cuidados de qualidade no tratamento do câncer. Como disse o renomado médico e filósofo Sir William Osler: “A medicina é uma ciência da incerteza e uma arte da probabilidade.”
Gostou ❔ Nos deixe um comentário ✍️, compartilhe em suas redes sociais e|ou mande sua dúvida pelo 💬 Chat On-line em nossa DM do Instagram.
oncologia #cirurgiadigestiva #acessoasaude #cancerdigestivo #saudepublica
Oncologia Cirúrgica
O que causa a Morte dos Pacientes com Câncer?
A mortalidade associada ao câncer é um tema complexo e multifacetado, que vai além da mera presença do tumor. Embora a frase “a metástase é responsável por 90% das mortes por câncer” seja frequentemente citada, essa afirmação simplifica uma realidade muito mais intrincada. Este texto visa explorar as causas de morte em pacientes com câncer, com foco nas implicações para a cirurgia do aparelho digestivo, proporcionando uma visão abrangente e educativa para estudantes de medicina, residentes em cirurgia geral e pós-graduandos em cirurgia do aparelho digestivo.
Introdução
O câncer é uma das principais causas de mortalidade em todo o mundo, afetando milhões de pessoas anualmente. No Brasil, estima-se que as mortes por câncer representem cerca de 17% do total de óbitos, com a taxa de mortalidade aumentando à medida que a doença avança. A compreensão das causas de morte em pacientes oncológicos é essencial para o desenvolvimento de estratégias de tratamento mais eficazes e para a melhoria da qualidade de vida desses pacientes.
Causas Multifatoriais
As causas de morte em pacientes com câncer podem ser agrupadas em três categorias principais: eventos agudos, deterioração gradual e complicações associadas ao tratamento.
- Eventos Agudos: Muitas mortes ocorrem devido a eventos agudos, como tromboembolismo, que pode levar a falência respiratória ou cardíaca. A presença de metástases em órgãos vitais, como o cérebro e os pulmões, pode causar obstruções que resultam em morte súbita. Estudos mostram que até 50% das mortes por câncer podem ser atribuídas a essas causas agudas.
- Deterioração Gradual: A deterioração funcional de órgãos vitais é uma causa significativa de morte. Por exemplo, metástases no fígado podem levar à insuficiência hepática, enquanto a obstrução intestinal é comum em pacientes com câncer gastrointestinal. A deterioração do estado geral do paciente, frequentemente associada à caquexia, também contribui para o aumento da mortalidade.
- Complicações Associadas ao Tratamento: Os tratamentos oncológicos, embora essenciais, podem induzir complicações que afetam a saúde do paciente. A quimioterapia pode causar neutropenia, aumentando o risco de infecções graves. Dados indicam que infecções bacterianas, especialmente pneumonia, são causas comuns de morte em pacientes oncológicos, especialmente aqueles com câncer hematológico.
Aplicação na Cirurgia Digestiva
A cirurgia do aparelho digestivo desempenha um papel crucial no tratamento de muitos tipos de câncer, especialmente aqueles que afetam o trato gastrointestinal. No entanto, a compreensão das causas de morte associadas ao câncer é vital para os cirurgiões digestivos. Os cirurgiões devem estar cientes de que a mortalidade pode não resultar apenas da ressecção tumoral, mas também de complicações pós-operatórias, como infecções e falência de órgãos. A implementação de protocolos de cuidado pós-operatório e a monitorização rigorosa de sinais de complicações são essenciais para melhorar os resultados cirúrgicos.
Pontos-Chave
- Compreensão Multifatorial: A mortalidade em pacientes com câncer é influenciada por uma combinação de fatores, incluindo a localização do tumor, a presença de metástases e as condições de saúde pré-existentes.
- Intervenções Precoces: A identificação e o manejo precoce de complicações podem melhorar significativamente a qualidade de vida e a sobrevida dos pacientes.
- Importância da Pesquisa: A pesquisa contínua sobre as causas de morte em pacientes com câncer é fundamental para o desenvolvimento de novas estratégias terapêuticas e para a melhoria do cuidado ao paciente.
Conclusões Aplicadas à Prática do Cirurgião Digestivo
A análise das causas de morte em pacientes com câncer revela a complexidade do manejo oncológico e a necessidade de uma abordagem integrada. Cirurgiões do aparelho digestivo devem considerar não apenas a ressecção do tumor, mas também as complicações potenciais e as condições subjacentes que podem afetar a mortalidade. A educação contínua e a pesquisa são essenciais para aprimorar as práticas cirúrgicas e, assim, oferecer cuidados mais eficazes e humanizados aos pacientes com câncer.
A frase de Hipócrates, “A arte de curar vem da natureza, não do médico”, nos lembra da importância de compreender a biologia da doença e suas implicações no tratamento.
Gostou ❔ Nos deixe um comentário ✍️, compartilhe em suas redes sociais e|ou mande sua dúvida pelo 💬 Chat On-line em nossa DM do Instagram.
Câncer #CirurgiaDigestiva #TratamentoOncológico #Saúde #EducaçãoMédica
Cirurgia Paliativa do Aparelho Digestivo
Uma Ferramenta Essencial no Cuidado Integral das Doenças Digestivas
Introdução
No complexo cenário dos cuidados cirúrgicos, onde o foco costuma ser em intervenções curativas, a cirurgia paliativa surge como um domínio crucial, embora frequentemente subestimado. Isso é especialmente verdadeiro na cirurgia do aparelho digestivo, onde a carga de malignidades e outras condições intratáveis exige uma abordagem que priorize o alívio dos sintomas e a qualidade de vida. Em um país como o Brasil, onde a incidência de câncer tem aumentado significativamente—estimada em 625.000 novos casos por ano pelo Instituto Nacional de Câncer (INCA)—o papel da cirurgia paliativa não pode ser subestimado. Este artigo explora as nuances da cirurgia paliativa gastrointestinal, abordando suas aplicações, desafios e impacto no cuidado ao paciente.
Importância do Tema
A cirurgia paliativa no sistema digestivo é uma área em evolução, com raízes profundas na história da prática cirúrgica. O principal objetivo da cirurgia paliativa gastrointestinal é aliviar sintomas como obstrução, hemorragia e dor intratável, comuns nos estágios avançados das doenças digestivas, incluindo cânceres de estômago, pâncreas e cólon. Ao contrário da cirurgia curativa, cujo objetivo é remover completamente a doença, a cirurgia paliativa foca em melhorar a qualidade de vida do paciente ao mitigar os sintomas angustiantes da sua doença. No Brasil, os cânceres do aparelho digestivo estão entre as principais causas de mortalidade relacionada ao câncer, com o câncer colorretal ocupando o terceiro lugar em incidência. A necessidade de intervenções paliativas nesses casos é essencial, especialmente considerando que muitos pacientes apresentam a doença em estágio avançado, onde as opções curativas são limitadas. A cirurgia paliativa do aparelho digestivo, portanto, desempenha um papel crítico no manejo abrangente desses pacientes.
Tipos de Cirurgias Paliativas no Aparelho Digestivo
Diversos tipos de cirurgias paliativas são realizadas na prática cirúrgica do aparelho digestivo, cada uma destinada a aliviar sintomas específicos e melhorar a qualidade de vida do paciente. Entre as cirurgias mais comuns, destacam-se:
- Gastrojejunostomia: Utilizada para aliviar a obstrução do trato de saída gástrico em pacientes com câncer gástrico avançado ou câncer pancreático, permitindo que o alimento passe do estômago para o intestino delgado.
- Colectomia e Colostomia: Indicadas para obstruções malignas do cólon, essas cirurgias podem evitar complicações como perfuração ou necrose do cólon, proporcionando alívio significativo dos sintomas.
- Biliodigestivas: Como a hepáticojejunostomia, são indicadas para aliviar a icterícia obstrutiva em cânceres pancreáticos avançados, permitindo a drenagem adequada da bile.
- Bypass intestinal: Usado em obstruções intestinais malignas, onde a remoção direta do tumor não é possível, mas a criação de uma nova rota para o trânsito intestinal pode aliviar os sintomas.
Protocolo CLASS
O protocolo CLASS é uma ferramenta essencial para guiar a comunicação cirúrgica em contextos de cuidados paliativos. Este protocolo consiste em cinco etapas fundamentais:
- Contexto: Criar um ambiente adequado para a conversa, garantindo privacidade e mostrando-se acessível e receptivo.
- Escuta: Demonstrar habilidades de escuta ativa, permitindo que o paciente e seus familiares expressem suas preocupações e compreensões.
- Reconhecimento das emoções: Identificar e validar as emoções expressas pelo paciente, usando respostas empáticas para criar uma conexão significativa.
- Estratégia: Propor um plano de manejo que seja compreensível e que o paciente esteja disposto a seguir.
- Resumo: Encerrar a conversa resumindo os principais pontos discutidos, garantindo que todos tenham compreendido as próximas etapas.
Parâmetros de Pior Prognóstico
Na realização de uma cirurgia paliativa, é fundamental avaliar cuidadosamente o prognóstico do paciente. Alguns parâmetros associados a um pior prognóstico incluem:
- Perda de peso significativa: Historial de perda de peso superior a 10 kg, indicando desnutrição severa.
- Anemia severa: Níveis de hemoglobina abaixo de 10,5 g/dL, associados a piora do estado geral do paciente.
- Hipoalbuminemia: Níveis de albumina sérica abaixo de 3,5 g/dL, refletindo um estado nutricional comprometido.
- PCR elevada: Proteína C-reativa elevada, sugerindo um estado inflamatório significativo.
- Escala de Fadiga do NCI: Escore de fadiga igual ou superior a 1, indicando piora da condição clínica.
- Escala de Karnofsky ou ECOG: Escores elevados nestas escalas indicam uma menor capacidade funcional, o que pode influenciar negativamente o resultado da cirurgia.
Esses fatores ajudam a determinar a viabilidade da cirurgia e a balancear os benefícios e riscos envolvidos.
Pontos-Chave
- Cuidado Centrado no Paciente: A cirurgia paliativa gastrointestinal prioriza o cuidado individualizado, focando no alívio dos sintomas ao invés de prolongar a vida a qualquer custo.
- Abordagem Multidisciplinar: A decisão de realizar uma cirurgia paliativa deve envolver uma equipe de especialistas para garantir que o cuidado seja holístico e alinhado com os valores e objetivos do paciente.
- Contexto Brasileiro: No Brasil, onde o acesso ao cuidado cirúrgico avançado pode ser desigual, o papel da cirurgia paliativa é ainda mais crucial. Cirurgiões precisam tomar decisões que sejam clinicamente sólidas e também socialmente e eticamente informadas.
- Técnicas Avançadas: Com os avanços em técnicas minimamente invasivas, como a cirurgia laparoscópica e robótica, as intervenções paliativas se tornaram menos gravosas para os pacientes, oferecendo alívio dos sintomas com menor tempo de recuperação e menos complicações.
- Medidas de Desfecho: O sucesso na cirurgia paliativa deve ser medido pelo grau de alívio dos sintomas e pela melhoria na qualidade de vida do paciente, conforme destacado em estudos de centros oncológicos brasileiros.
Conclusões
A cirurgia paliativa gastrointestinal ocupa um espaço único e essencial dentro do espectro dos cuidados cirúrgicos. Ela exige uma compreensão aprofundada das necessidades dos pacientes, da progressão da doença e das dimensões éticas das intervenções cirúrgicas. Para estudantes de medicina, residentes e cirurgiões pós-graduados especializados em doenças do aparelho digestivo, dominar os princípios da cirurgia paliativa é crucial. Não se trata apenas de realizar uma operação tecnicamente competente, mas de tomar decisões informadas e compassivas que impactam profundamente os últimos dias do paciente.
No Brasil, onde a carga de cânceres do aparelho digestivo é significativa, a importância da cirurgia paliativa continuará a crescer. Como tal, a educação continuada e a pesquisa nessa área são essenciais para melhorar os desfechos para pacientes com doenças digestivas avançadas. Nas palavras de Dr. William Osler, “O bom médico trata a doença; o grande médico trata o paciente que tem a doença.” Este sentimento captura a essência da cirurgia paliativa no aparelho digestivo, onde o objetivo final é cuidar do paciente como um todo, abordando tanto o sofrimento físico quanto o emocional.
Gostou do conteúdo? Deixe-nos um comentário ✍️, compartilhe nas suas redes sociais, e|ou envie sua pergunta via 💬 Chat Online no nosso DM do Instagram.
CirurgiaPaliativa #CuidadosPaliativos #AparelhoDigestivo #OncologiaCirúrgica #QualidadeDeVida

Fundamentos e Avanços no Tratamento do Câncer Digestivo
O câncer é uma doença complexa caracterizada pelo crescimento descontrolado e desregulado de células, levando à formação de neoplasias malignas. No tratamento cirúrgico do câncer, o objetivo é remover os tumores e controlar a disseminação da doença, proporcionando ao paciente a melhor chance de sobrevivência e qualidade de vida.
Biologia do Câncer
O câncer se origina de alterações genômicas que promovem a replicação celular excessiva ou inibem a morte celular programada (apoptose). Essas mutações podem ativar oncogenes ou desativar genes supressores de tumor, resultando em crescimento celular desordenado. A identificação desses genes pode fornecer informações valiosas sobre a agressividade do tumor e ajudar na personalização dos tratamentos. Por exemplo, a amplificação do oncogene C-erbB-2 está associada a um prognóstico mais reservado no câncer de mama.
Tumores Benignos vs. Malignos
Os tumores benignos permanecem localizados e não invadem tecidos adjacentes. Em contraste, os malignos têm a capacidade de invadir e metastatizar para locais distantes, o que pode levar a complicações graves e à morte. O processo de invasão e metástase é mediado por alterações adicionais nas células cancerígenas, que facilitam a sua propagação para órgãos distantes.
Estatísticas Brasileiras
No Brasil, o câncer é uma das principais causas de morte. De acordo com o Instituto Nacional de Câncer (INCA), estima-se que em 2024 haja aproximadamente 700 mil novos casos de câncer no país. Entre os tipos mais comuns estão os cânceres de mama, próstata e colorretal. A detecção precoce e a intervenção cirúrgica são fundamentais para melhorar as taxas de sobrevivência.
Avanços no Tratamento Cirúrgico
A cirurgia continua a ser um pilar crucial no tratamento do câncer, especialmente quando realizada com técnicas modernas e precisão. A abordagem cirúrgica deve ser cuidadosamente planejada para garantir a remoção completa do tumor e minimizar os riscos de recidiva. O avanço em técnicas como a cirurgia minimamente invasiva e a cirurgia robótica tem permitido melhores resultados com menor impacto para os pacientes.
Aspectos Importantes na Prática Cirúrgica
- Cuidados Pré-operatórios: Avaliações completas e planejamento cuidadoso são essenciais para o sucesso da cirurgia.
- Habilidade Operatória: A execução precisa e a atenção aos detalhes são fundamentais para a remoção eficaz do tumor.
- Controle de Metástases: Monitoramento contínuo e tratamento das metástases são cruciais para o manejo a longo prazo do câncer.
- Recuperação e Reabilitação: O suporte pós-operatório e a reabilitação são importantes para a recuperação do paciente e manutenção da qualidade de vida.
Conclusão
A cirurgia oncológica é uma disciplina dinâmica que exige constante atualização e refinamento das habilidades. O entendimento da biologia do câncer e a aplicação de técnicas avançadas são fundamentais para melhorar os resultados dos tratamentos e proporcionar aos pacientes uma chance maior de sobrevivência e bem-estar.
“A medicina é um ofício que requer habilidades e dedicação constantes. Como disse Sir William Osler, ‘O médico deve ter a mente de um cientista, o coração de um humanista e a habilidade de um artesão’.”
Gostou ❔ Nos deixe um comentário ✍️ , compartilhe em suas redes sociais e|ou mande sua dúvida pelo 💬 Chat On-line em nossa DM do Instagram.
Hashtags: #OncologiaCirúrgica #TratamentoCâncer #CirurgiaDigestiva #CancerNoBrasil #AvançosMédicos
Specific Competence of Surgical Leadership
Surgeons are uniquely prepared to assume leadership roles because of their position in the operating room (OR). Whether they aspire to the title or not, each and every surgeon is a leader, at least within their surgical team. Their clinical responsibilities offer a rich variety of interpretations that prepare them for a broader role in health care leadership. They deal directly with patients and their families, both in and out of the hospital setting, seeing a perspective that traditional health care administrative leaders rarely experience. They work alongside other direct providers of health care, in varied settings, at night, on weekends, as well as during the typical workday. They understand supply-chain management as something more than lines on a spreadsheet.
The Challenges for a Surgical Leader
Surgeons prefer to lead, not to be led. Surgical training has traditionally emphasized independence, self-reliance, and a well-defined hierarchy as is required in the OR. However, this approach does not work well outside the OR doors. With colleagues, nurses, staff, and patients, they must develop a collaborative approach. Surgeons are entrusted with the responsibility of being the ultimate decision maker in the OR. While great qualities in a surgeon in the OR, it hinders their interactions with others. They have near-absolute authority in the OR, but struggle when switching to a persuasive style while in committees and participating in administrative activities. Most surgeons do not realize they are intimidating to their patients and staff. With patients, a surgeon needs to be empathetic and a good listener. A surgeon needs to slow the pace of the discussion so that the patient can understand and accept the information they are receiving. As perfectionists, surgeons demand a high level of performance of themselves. This sets them up for exhaustion and burnout, becoming actively disengaged, going through the motions, but empty on the inside. Given the many challenges surgeons face, it is difficult for them to understand the leadership role, given its complex demands.
Specific Competencies
Authority
Although teams and all team members provide health care should be allowed input, the team leader makes decisions. The leader must accept the responsibility of making decisions in the presence of all situations. They will have to deal with conflicting opinions and advice from their team, yet they must accept that they will be held accountable for the performance of their team. The surgeon–leader cannot take credit for successes while blaming failures on the team. Good teamwork and excellent communication do not relieve the leader of this responsibility.
Leadership Style
A surgeon often has a position of authority based on their titles or status in an organization that allows them to direct the actions of others. Leadership by this sort of mandate is termed “transactional leadership” and can be successful in accomplishing specific tasks. For example, a surgeon with transactional leadership skills can successfully lead a surgical team through an operation by requesting information and issuing directives. However, a leader will never win the hearts of the team in that manner. The team will not be committed and follow through unless they are empowered and feel they are truly heard. A transformational leader is one who inspires each team member to excel and to take action that supports the entire group. If the leader is successful in creating a genuine atmosphere of cooperation, less time will be spent giving orders and dealing with undercurrents of negativity. This atmosphere can be encouraged by taking the time to listen and understand the history behind its discussion. Blame should be avoided. This will allow the leader to understand the way an individual thinks and the group processes information to facilitate the introduction of change. While leadership style does not guarantee results, the leader’s style sets the stage for a great performance. At the same time, they should be genuine and transparent. This invites the team members to participate, creating an emotional connection. Leaders try to foster an environment where options are sought that meet everyone’s desires.
Conflict Management
Conflict is pervasive, even in healthy, well-run organizations and is not inherently bad. Whether conflict binds an organization together or divides it into factions depends on whether it is constructive or destructive. A good leader needs to know that there are four essential truths about conflict. It is inevitable, it involves costs and risks, the strategies we develop to deal with the conflict can be more damaging than the conflict itself, and conflict can be permanent if not addressed. The leader must recognize the type of conflict that exists and deal with the conflict appropriately. Constructive discussion and debate can result in better decision making by forcing the leader to consider other ideas and perspectives. This dialog is especially helpful when the leader respects the knowledge and opinions of team members with education, experience, and perspective different from the leader’s. Honesty, respect, transparency, communication, and flexibility are all elements that a leader can use to foster cohesion while promoting individual opinion. The leader can create an environment that allows creative thinking, mutual problem solving, and negotiation. These are the hallmarks of a productive conflict. Conflict is viewed as an opportunity, instead of something to be avoided.
Communication Skills
Communication is the primary tool of a successful leader. On important topics, it is incumbent on the leader to be articulate, clear, and compelling. Their influence, power, and credibility come from their ability to communicate. Research has identified the primary skills of an effective communicator. They are set out in the LARSQ model: Listening, Awareness of Emotions, Reframing, Summarizing, and Questions. These are not set in a particular order, but rather should move among each other freely. In a significant or critical conversation, it is important for a leader to listen on multiple levels. The message, body language, and tone of voice all convey meaning. You cannot interrupt or over-talk the other side. They need an opportunity to get their entire message out. Two techniques that enhance listening include pausing and the echo statement. Pausing before speaking allows the other conversant time to process what they have said to make sure the statement is complete and accurate. Echo statements reflect that you have heard what has been said and focuses on a particular aspect needing clarification. Good listening skills assure that the leader can get feedback that is necessary for success.
Vision, Strategy, Tactics, and Goals
One of the major tasks of a leader is to provide a compelling vision, an overarching idea. Vision gives people a sense of belonging. It provides them with a professional identity, attracts commitment, and produces an emotional investment. A leader implements vision by developing strategy that focuses on specific outcomes that move the organization in the direction of the vision. Strategy begins with sorting through the available choices and prioritizing resources. Through clarification, it is possible to set direction. Deficits will become apparent and a leader will want to find new solutions to compensate for those shortfalls. For example, the vision of a hospital is to become a world class health care delivery system. Strategies might include expanding facilities, improving patient satisfaction, giving the highest quality of care, shortening length of hospital stay with minimal readmissions, decreased mortality, and a reduction in the overall costs of health care. Tactics are specific behaviors that support the strategy with the aim to achieve success. Tactics for improving patient satisfaction may include reduced waiting time, spending more time with patients, taking time to communicate in a manner that the patient understands, responding faster to patient calls, etc. These tactics will then allow a leader to develop quantitative goals. Patient satisfaction can be measured. The surgical leader can then construct goals around each tactic, such as increasing satisfaction in specific areas. This information allows a surgical leader to identify barriers and they can take steps to remedy problem areas. This analysis helps a leader find the weakest links in their strategies as they continue toward achieving the vision.
Change Management
The world of health care is in continuous change. The intense rate of political, technical, and administrative change may outpace an individual’s and institution’s ability to adapt. Twenty-first century health care leaders face contradictory demands. They must navigate between competing forces. Leaders must traverse a track record of success with the ability to admit error. They also must maintain visionary ideas with pragmatic results. Individual accountability should be encouraged, while at the same time facilitating teamwork. Most leaders do not understand the change process. There are practical and psychological aspects to change. From an institutional perspective, we know that when 5% of the group begins to change, it affects the entire group. When 20% of a group embraces change, the change is unstoppable.
Succession Planning and Continuous Learning
An often-overlooked area of leadership is planning for human capital movement. As health care professionals retire, take leaves of absences, and move locations, turmoil can erupt in the vacuum. Leaders should regularly be engaging in activities to foster a seamless passing of institutional knowledge to the next generation. They also should seek to maintain continuity to the organization. Ways to accomplish this include senior leaders actively exposing younger colleagues to critical decisions, problem solving, increased authority, and change management. Leaders should identify promising future leaders, give early feedback for areas of improvement, and direct them toward available upward career tracks. Mentoring and coaching help prepare the younger colleagues for the challenges the institution is facing. Teaching success at all levels of leadership helps create sustainable high performance.
Postpancreatectomy Hemorrhage
Postoperative complications represent one of the most debated topics in pancreatic surgery. Indeed, the rate of complications following pancreatectomy is among the highest in abdominal surgery, with morbidity ranging between 30 and 60%. They are often characterized by elevated clinical burden, with a consequent challenging postoperative management. Mortality rates can exceed 5%. The impact on patient recovery and hospital stay eventually leads to massive utilization of resources and increases costs for the health system. The International Study Group of Pancreatic Surgery (ISGPS) provides standardized definitions and clinically based classifications for the most common complications after pancreatectomy, including postoperative pancreatic fistula (POPF), post pancreatectomy hemorrhage (PPH), delayed gastric emptying (DGE), bile leakage, and chyle leak.
Post Pancreatectomy Hemorrhage
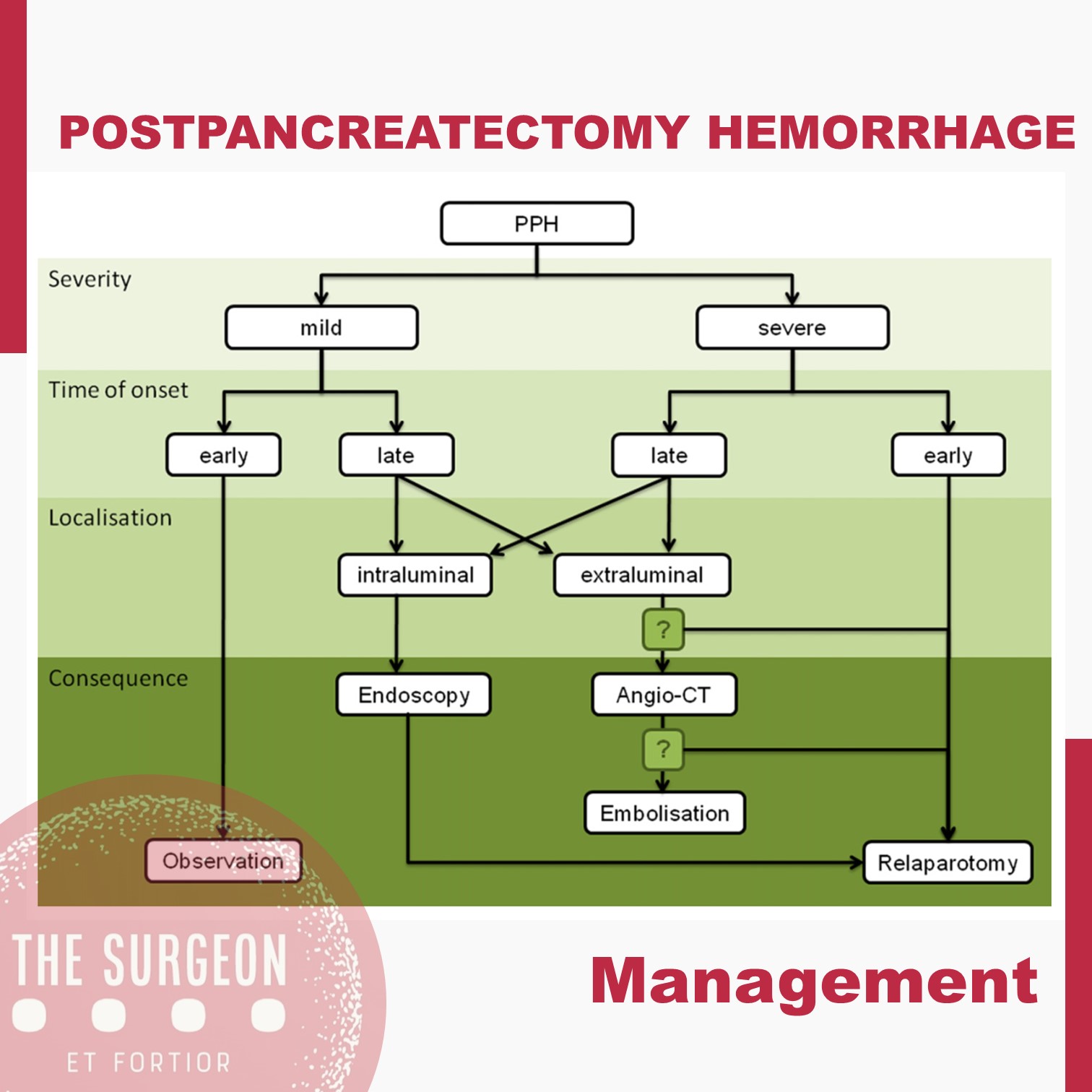
Despite its lower incidence compared with POPF with reported rates of 3–10% after pancreatectomy, PPH remains one of the major of postoperative complications, with mortality rates ranging from 30 to 50%. According to current ISGPS recommendations, PPH is classified in three grades (A, B, and C) based on two main criteria: timing of the hemorrhage and severity of the bleeding. The timing is dichotomized as early, occurring within 24 hours from the index surgery, and late, when it happens afterwards.

Management is tailored according to the clinical picture, the timing of onset, and the presumptive location. Early hemorrhage is generally due to either unsuccessful intraoperative hemostasis or to an underlying coagulopathy. The vast majority of patients are basically asymptomatic, with PPH having no influence on the postoperative course. However, when the bleeding is severe, re-laparotomy is recommended, with the aim of finding and controlling the source of bleeding. This approach usually guarantees an uneventful subsequent course. Late PPH is often challenging and the pathogenesis is diverse. Vascular erosion secondary to POPF or intraabdominal abscess, late failure of intraoperative hemostatic devices, arterial pseudoaneurysm, and intraluminal ulceration are some of the most common causes. In this setting, surgical access to the source of bleeding may be challenging. Angiography (if extraluminal) and endoscopy (if intraluminal) represent the primary approaches to treatment. Surgery is reserved for hemodynamically unstable patients and for those who present with deteriorating condition, multiorgan failure or sepsis. Given these assumptions, except for early mild events, contrast-enhanced abdominal CT is crucial in all cases of PPH, possibly allowing identification of the source and planning the management accordingly. Also, it should be noted that late massive hemorrhages may be preceded by mild self-limiting sentinel bleeds. A prompt abdominal CT scan aimed at excluding vascular lesions is therefore strongly recommended in these cases.
The incidence of complications following pancreatic resection remains high. The ISGPS established standardized definitions and clinical grading systems for POPF, PPH, DGE, and biliary and chyle leak. These classification systems have enabled unbiased comparisons of intraoperative techniques and management decisions. However, the management policies of these complications are most often driven by a patient’s condition and local surgical expertise and is not always based on the available high-level evidence. The development of high-volume specialized units with appropriate resources and multidisciplinary experience in complication management might further improve the evidence and the outcomes.
ORCID

https://orcid.org/0000-0001-5669-4169
Liver Disease and Perioperative Risk
The liver is the biggest intestinal organ and plays a central role in the homeostasis of different physiological systems including nutrition and drug metabolism, the synthesis of plasma proteins and haemostatic factors, as well as the elimination of different endogenous and exogenous substances. Although the liver contributes with only 3% to total body weight, given its major role in homeostasis and high energy consumption, it receives 25% of total cardiac output (CO). Two vessels contribute to the perfusion of the liver. The majority (70%) of the hepatic perfusion is provided by the portal vein, which contributes 50% of the organ’s oxygen demand. The other 50% is provided by the hepatic artery, which makes up around 30% of total liver perfusion. Hepatic arterial blood flow is mainly dependent on the organ’s metabolic demands and controlled via autoregulatory mechanisms, whereas blood supply through the portal vein depends on the perfusion throughout the whole gastrointestinal tract and the spleen. This unique, dual perfusion system provides constant perfusion rates and oxygen supply, which is crucial for adequate liver function. These high oxygen demands are reflected in a hepatic vein saturation of almost 30%.
The liver is also unique in its ability of regeneration, which allows the performance of major surgery including, amongst others, extended resections of liver tumours, living donations and so on. Many patients have normal liver function parameters when they present for liver surgery, especially when the reason for resection is metastasis or a benign liver tumour. The most common causes of liver resections are the hepatocellular carcinoma (HCC) and the cholangiocellular carcinoma (CCC). Hepatocellular carcinoma (HCC) often develops in patients with underlying liver cirrhosis; many of these patients show signs of chronic liver dysfunction (CLD).
As explained previously, the liver plays a central role in a great deal of physiological systems. Therefore, in case of chronic liver dysfunction (CLD) or liver failure, several effects on other organ systems have to be expected. Consequently liver resections and bile duct surgery as having a high risk for perioperative cardiac events, with an estimated 30-day cardiac event rate (cardiac death and myocardial infarction) of more than 5%. Patients undergoing liver surgery pose a significant challenge to treating physicians in the perioperative period. Due to the improvement of surgical techniques, the “liver patient” is becoming more and more complex, confronting surgeons, anaesthetists and intensive care personnel with difficult intra- and postoperative courses, and considerable multiorgan disorders. The cornerstones of an optimal management are careful selection of the patients, appropriate monitoring and protection of the liver and other vital organs.

Vascularização da Árvore Biliar
O Fio da Navalha na Prevenção da Isquemia e Estenose
Autor: Prof. Dr. Ozimo Gama (Tempo de Leitura: 11 minutos)
Introdução
No campo minado que é a cirurgia hepatobiliar, existe um princípio fisiológico que não admite margem para erro: enquanto o parênquima hepático é um órgão privilegiado, nutrido por um duplo suprimento sanguíneo (arterial e venoso portal), a árvore biliar é alimentada exclusivamente pelo sistema arterial. Para o estudante de medicina e o residente de cirurgia, a compreensão desta premissa muda drasticamente a forma como o bisturi e o cautério são manuseados em torno do hilo hepático. A esqueletização excessiva de um ducto biliar não é um sinal de dissecção meticulosa, mas sim a antessala anatómica de uma complicação catastrófica: a isquemia, seguida de necrose e estenose biliar. Neste artigo, dissecaremos a anatomia vascular da árvore biliar, as armadilhas do ducto cístico e os fundamentos anatómicos da cirurgia oncológica da vesícula.
1. A Vesícula Biliar: Topografia e Peculiaridades Histológicas
A vesícula biliar repousa no equador que divide o fígado direito do esquerdo — uma linha imaginária conhecida como Linha de Cantlie (ou linha de Rex-Cantlie), que cursa entre os segmentos IVb e V em direção à veia cava inferior posteriormente.
A vesícula é maioritariamente peritonizada, exceto na sua face posterior, que assenta diretamente na placa cística. No entanto, o seu verdadeiro “Calcanhar de Aquiles” reside na sua histologia: a vesícula biliar não possui muscularis mucosae, não possui submucosa e apresenta uma camada muscular descontínua.
- Implicação Cirúrgica Oncológica: Estas especificidades anatómicas removem as barreiras naturais contra a progressão tumoral, facilitando a invasão direta do cancro da vesícula biliar para o parênquima hepático. É por este motivo que o tratamento cirúrgico curativo exige uma Colecistectomia Radical (que inclui a ressecção em cunha dos segmentos hepáticos IVb e V) sempre que o estadiamento tumoral (T) for superior ou igual a T1b.

2. O Labirinto Anatómico do Ducto Cístico e da Via Biliar Principal
A partir do infundíbulo cónico da vesícula, o ducto cístico estende-se como o limite inferior do triângulo hepatocístico em direção ao hilo, unindo-se ao ducto hepático comum (DHC) para formar o ducto colédoco (VBP). Contudo, na via biliar, a variação anatómica é a regra, não a exceção. O ducto cístico pode correr paralelamente ao DHC, espiralar posteriormente a este e inserir-se na sua face medial. Mais perigoso ainda é quando o cístico se insere no Ducto Setorial Posterior Direito (RPD), uma variação que ocorre em cerca de 4% dos fígados. Esta configuração é notoriamente perigosa, expondo o RPD a um risco altíssimo de secção inadvertida durante uma colecistectomia de rotina. Distalmente, o colédoco entra na cabeça do pâncreas e une-se ao ducto pancreático (Wirsung) para formar a ampola hepatopancreática, controlada pelo Esfíncter de Oddi.
- O Canal Comum Longo: Quando a junção entre o colédoco e o ducto pancreático ocorre de forma anómala (antes do complexo esfincteriano), ocorre o refluxo de enzimas pancreáticas ativadas para a árvore biliar. Este trauma químico crónico é o principal fator de risco para a formação de cistoss do colédoco e para o desenvolvimento de Colangiocarcinoma.
3. O “Tendão de Aquiles”: A Vascularização Arterial da Via Biliar
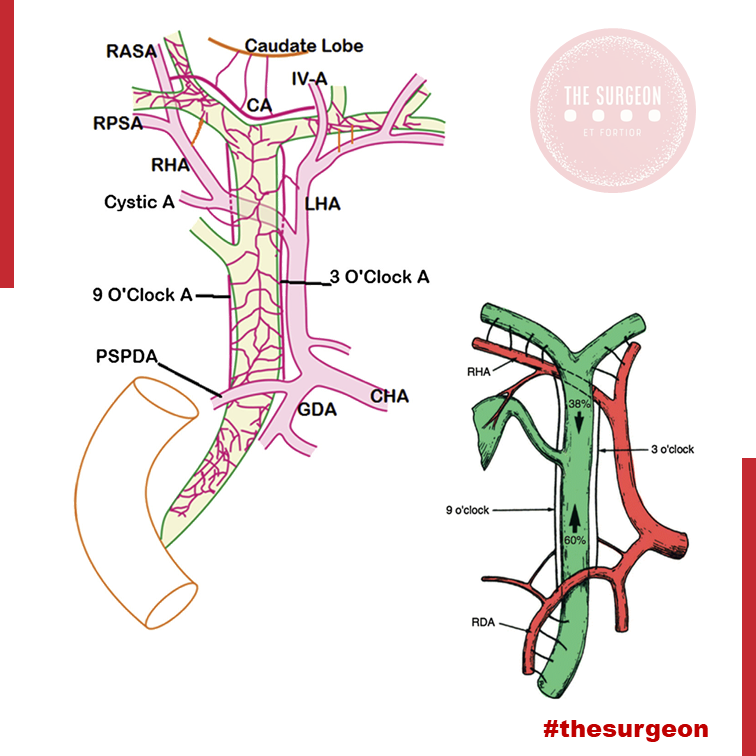
Como mencionado, a árvore biliar depende de um fluxo arterial ininterrupto. O suprimento segue um padrão de perfusão que ascende e descende ao longo dos ductos:
- O Suprimento Distal (Ascendente): O ducto colédoco recebe a sua irrigação inferior a partir de arteríolas emparelhadas provenientes da Artéria Gastroduodenal (GDA) e da Artéria Pancreatoduodenal Superior Posterior (PSPDA). Esta última representa o suprimento arterial mais importante e constante para o colédoco distal.
- O Suprimento Proximal (Descendente): Proximamente, o colédoco é alimentado por arteríolas originadas da artéria hepática direita (AHD).
- As Artérias Marginais: Estes vasos superiores e inferiores anastomosam-se para formar as artérias marginais, que correm paralelamente ao longo do ducto colédoco, situando-se tipicamente nas posições das 3 e 9 horas (lateral e medialmente). Desnudar (esqueletizar) o colédoco deste suprimento arterial para criar uma anastomose ou durante uma linfadenectomia não regrada acarreta um risco altíssimo de isquemia e estenose cicatricial a longo prazo.
4. O Plexo Epicoledociano Hilar e as Variações Arteriais
No interior do hilo hepático, uma rica rede de capilares liga as artérias hepáticas direita e esquerda. Este leito vascular, denominado Plexo Epicoledociano Hilar, fornece uma circulação colateral crítica que pode manter o suprimento arterial para um lado do fígado caso o vaso ipsilateral seja lesado. A preservação deste plexo e do suprimento sanguíneo arterial para o fígado remanescente é absolutamente crucial na criação de uma anastomose biliodigestiva (hepaticojejunostomia). A isquemia hilar resulta na temível colangiopatia isquémica e no desenvolvimento de abcessos hepáticos intratáveis.
O Papel das Variações Arteriais no Colangiocarcinoma Hilar
Na cirurgia do colangiocarcinoma hilar (Tumor de Klatskin), a complexidade aumenta devido às variações arteriais. A artéria hepática direita cruza posteriormente ao ducto hepático na maioria dos casos, mas em 25% cruza anteriormente. Mais relevante ainda é a presença de uma Artéria Hepática Direita Substituída (ou Acessória), com origem na Artéria Mesentérica Superior (AMS). Ao contrário da anatomia clássica, este vaso cursa lateralmente ao ducto colédoco (e não medialmente), estando extremamente vulnerável à iatrogenia se o cirurgião não o identificar durante a dissecção do ligamento hepatoduodenal. Combinações destas variações com a localização exata do tumor ditarão se uma lesão hilar é ressecável ou irresecável.
Pontos-Chave para a Prática Diária
- A Regra das 3 e 9 Horas: Lembre-se sempre de que o suprimento axial do colédoco viaja nos seus flancos laterais. Evite dissecções circunferenciais extensas da via biliar principal.
- Histologia e Neoplasias: A ausência de submucosa na vesícula biliar dita a necessidade de cirurgia hepática radical (ressecção em cunha do leito) em tumores T1b ou superiores.
- Inserções Anómalas do Cístico: A inserção num ducto setorial direito (RPD) é uma armadilha clássica. A Visão Crítica de Segurança (CVS) e a colangiografia são as únicas formas de evitar a transecção de um ducto principal aberrante.
- O Perigo do Canal Comum: A junção biliopancreática anómala exige vigilância ou tratamento cirúrgico devido ao elevado risco de colangiocarcinoma derivado da inflamação enzimática crónica.
Conclusões Aplicadas à Prática do Cirurgião Digestivo
O respeito pela árvore biliar transcende a mera identificação do tubo que transporta a bílis; exige uma veneração profunda pela sua microvascularização. O cirurgião que descasca a via biliar como se tratasse de um cabo elétrico condena o seu doente a um futuro de estenoses isquémicas, colangites de repetição e reintervenções de extrema complexidade. O domínio da variabilidade anatómica vascular (como as artérias substituídas da AMS) e o conhecimento tático do plexo epicoledociano não são meros detalhes de rodapé dos livros de anatomia; são a linha que separa o triunfo cirúrgico oncológico da catástrofe iatrogénica irreparável.
“A anatomia biliar não segue regras absolutas, apenas tendências. Operar no hilo hepático assumindo a normalidade é o primeiro passo para o desastre. O cirurgião deve dissecar com a expectativa constante da variação.” — Aforismo clássico da cirurgia hepatobiliar.
Gostou ❔Deixe-nos um comentário ✍️, partilhe nas suas redes sociais e|ou envie a sua dúvida pelo 💬 Chat On-line na nossa DM do Instagram.
Surgical Management of PANCREATIC CANCER
INTRODUCTION
Pancreatic ductal adenocarcinoma (PDAC) carries one of the poorest overall prognosis of all human malignancies. The 5-year survival in patients with PDAC, for all stages, remains as low as 6–7%. The low survival rate is attributed to several factors, of which the two most important are aggressive tumor biology and late stage at which most patients are diagnosed. Only 10–20% of patients are eligible for resection at presentation, 30–40% are unresectable/locally advanced, and 50–60% are metastatic. Pancreatic cancer without distant metastasis can be divided into three categories: resectable, borderline resectable, and locally advanced. In absence of metastatic disease, the most important factor for improving survival and possibly offer cure is to achieve a margin-negative resection. Even after potential curative resection, most patients develop recurrences eventually, and 5-year survival of completely resected patients is only up to 25%. The aggressive tumor biology and its inherent resistance to chemotherapy and radiotherapy contributes to early recurrence and metastasis.
SURGICAL ADVANCES
Pancreatic cancer surgery has evolved over the past few decades and remains the cornerstone of treatment of resectable and borderline resectable tumors. Advances in modern imaging give precise information on disease extension and vascular involvement that aids in surgical planning in order to achieve a margin-negative resection.
SURGICAL TECHNIQUES
Surgical techniques for pancreatic cancer include pancreaticoduodenectomy, distal pancreatectomy with splenectomy, and total pancreatectomy. Standard lymphadenectomy for pancreatoduodenectomy should include removal of lymph node stations 5, 6, 8a, 12b1, 12b2, 12c, 13a, 13b, 14a, 14b, 17a, and 17b. Involvement of superior mesenteric vein (SMV)/portal vein(PV) was previously considered as a contraindication for resection. However, curative resection along with SMV/PV with vascular reconstruction has now become a standard practice in specialized high-volume centers. To improve margin-negative resections, specially in borderline resectable tumors with proximity to vascular structures, SMA first approach was proposed as a new modification of standard pancreatico-duodenectomy. In a systematic review, SMA first approach was shown to be associated with better perioperative outcomes, such as blood loss, transfusion requirements, pancreatic fistula, delayed gastric emptying, and reduced local and metastatic recurrence rates. In case of arterial involvement, there is no good evidence at present to justify arterial resections for right-sided pancreatic tumors. However, the modified Appleby procedure, which includes en bloc removal of celiac axis with or without arterial reconstruction, when used in appropriately selected patients, offers margin negative resection with survival benefit for locally advanced pancreatic body and tail tumors and should be performed in high-volume centers. Most evidence does not support advantage of more extended resections such as removal of the para-aortic lymph nodes and nerve plexus and multivisceral resections routinely. Such extended resections are associated with compromised quality of life because of associated higher perioperative morbidity and intractable diarrhea. However, in highly selected patients, with preserved performance status and stable or nonprogressive disease on neoadjuvant treatment, such extended resections can provide survival advantage over palliative treatments. Radical surgery in the presence of oligometastatic disease has also been reported to prolong survival in highly selected patients.
Hepatocellular ADENOMA
Benign liver tumours are common and are frequently found coincidentally. Most benign liver lesions are asymptomatic, although larger lesions can cause non-specific complaints such as vague abdominal pain. Although rare, some of the benign lesions, e.g. large hepatic adenomas, can cause complications such as rupture or bleeding. Asymptomatic lesions are often managed conservatively by observation. Surgical resection can be performed for symptomatic lesions or when there is a risk of malignant transformation. The type of resection is variable, from small, simple, peripheral resections or enucleations, to large resections or even liver transplantation for severe polycystic liver disease.
General Considerations
Hepatocellular adenomas (HCA) are rare benign hepatic neoplasms in otherwise normal livers with a prevalence of around 0.04% on abdominal imaging. HCAs are predominantly found in women of child-bearing age (2nd to 4th decade) with a history of oral contraceptive use; they occur less frequently in men. The association between oral contraceptive usage and HCA is strong and the risk for a HCA increases if an oral contraceptive with high hormonal potency is used, and if it is used for over 20 months. Long-term users of oral contraceptives have an estimated annual incidence of HCA of 3–4 per 100000. More recently, an increase in incidence in men has been reported, probably related to the increase in obesity, which is reported as another risk factor for developing HCA. In addition, anabolic steroid usage by body builders and metabolic disorders such as diabetes mellitus or glycogen storage disease type I are associated with HCAs. HCAs in men are generally smaller but have a higher risk of developing into a malignancy. In the majority of patients, only one HCA is found, but in a minority of patients more than 10 lesions have been described (also referred to as liver adenomatosis).
Clinical presentation
Small HCAs are often asymptomatic and found on abdominal imaging being undertaken for other purposes, during abdominal surgery or at autopsy. Some patients present with abdominal discomfort, fullness or (right upper quadrant) pain due to an abdominal mass. It is not uncommon that the initial symptoms of a HCA are acute onset of abdominal pain and hypovolaemic shock due to intraperitoneal rupture. In a series of patients who underwent resection, bleeding was reported in up to 25%. The risk of rupture is related to the size of the adenoma. Exophytic lesions (protruding from the liver) have a higher chance of bleeding compared to intrahepatic or subcapsular lesions (67% vs 11% and 19%, respectively, P<0.001). Lesions in segments II and III are also at higher risk of bleeding compared to lesions in the right liver (35% vs 19%, P = 0.049).
Management
There is no guideline for the treatment of HCAs, although there are general agreements. In men, all lesions should be considered for surgical resection independent of size, given the high risk of malignant transformation, while taking into account comorbidity and location of the lesion. Resection should also be considered in patients with HCAs due to a metabolic disorder. In women, lesions <5 cm can be observed with sequential imaging after cessation of oral contraceptive treatment. In larger tumours, treatment strategies vary. Some clinicians have proposed non-surgical management if hormone therapy is stopped and patients are followed up with serial radiological examinations. The time period of waiting is still under debate, however recent studies indicate that a waiting period of longer than 6 months could be justified.
More recently, the subtypes of the Bordeaux classification of HCA have been studied related to their risk of complications. Some groups report that percutaneous core needle biopsy is of limited value because the therapeutic strategy is based primarily on patient sex and tumour size. Others report a different therapeutic approach based on subtype. Thomeer et al. concluded that there was no evidence to support the use of subtype classification in the stratification and management of individual patients related to risk of bleeding. Size still remains the most important feature to predict those at risk of bleeding during follow-up. However, malignant transformation does seem to be related to differences in subtypes. β-catenin-mutated HCAs trigger a potent mitogenic signalling pathway that is prominent in HCC. Cases of inflammatory HCAs can also show activation of the β-catenin pathway with a risk of developing malignancy. Therefore, β-catenin-mutated and inflammatory HCAs are prone to malignant degeneration, and particularly if >5cm. In these circumstances, invasive treatment should be considered.
POPF after Distal Pancreatectomy
Minimally Invasive Versus Open Techniques
Despite advances in laparoscopic and robotic approaches, the vast majority of distal pancreatectomies continue to be performed via an open approach. Recent retrospective data have demonstrated that minimally invasive distal pancreatectomy is associated with decreased blood loss and shorter hospital stays than open pancreatectomy. A large recent study utilizing the Nationwide Inpatient Sample database suggested, first, that the minimally invasive approach is becoming more widely utilized, increasing from 2.4 to 7.3 % over a study period from 1998 to 2009. Second, that study reported that the minimally invasive approach was associated with decreased length of stay as well as decreased incidence of infectious complications, bleeding complications, and blood transfusions. This population-based study echoes conclusions drawn by a large multi-institutional study performed several years previously. Drawing on a combined patient sample of 667 patients, with 24 % initially attempted laparoscopically, the authors were able to demonstrate lower overall complication rate, decreased blood loss, and shorter hospital stays among patients undergoing laparoscopic approach via a multivariate analysis.
Notably, there was no significant difference in the pancreatic leak rate between the open and laparoscopic approaches, although there was a nonsignificant trend favoring the laparoscopic approach. More recently, the robotic approach has generated significant interest as a technique for performing distal pancreatectomy. Retrospective analysis has suggested that the robotic approach is well suited for pancreatectomy. Fistula rates, however, remain a concern. A retrospective review of patients undergoing robotic pancreatic operations included 83 patients who underwent distal pancreatectomy. About 27 % were identified as having a ISPGF type A pancreatic leak; 12 and 4.8 % were identified as having a grade B or C leak, respectively.
Identifying Risk Factors
For pancreaticoduodenectomy (PTD) , a fistula risk score has been recently developed that has been shown to be highly predictive of POPF. This score assigns points based on gland texture, gland pathology, duct diameter, and intraoperative blood loss. In general, high blood loss, soft gland texture, and smaller duct diameter confer increased risk of POPF, whereas pancreatic adenocarcinoma and pancreatitis as the indication for PTD confer protection for the development of pancreatic fistula versus other diagnoses. Also of note, higher fistula risk scores correlated with greater incidence of clinically relevant (ISGPF grade B or C) fistula. The adaptation of this risk score to patients undergoing distal pancreatectomy is yet to be validated; however, at least one published study indicates that this scoring system may have limitations in the setting of distal pancreatectomy. In that study, risk factors for pancreatic fistula after stapled gland transection in patients undergoing distal pancreatectomy were examined, and in a multivariate analysis, only the presence of diabetes and the use of a 4.1-mm staple cartridge were associated with increased risk of pancreatic fistula formation.
Surgical Management of CHOLANGIOCARCINOMA

Cholangiocarcinoma is an uncommon cancer that occurs within the intrahepatic and extrahepatic portions of the bile duct system. In North America, the incidence of extrahepatic cholangiocarcinoma is 0.5–2 per 100,000 and 0.95 per 100,000 for intrahepatic cholangiocarcinoma. Up to 50% of patients will be lymph node (LN) positive at presentation, 5% are multifocal tumors, and 10–20% will have peritoneal involvement at presentation. Risk factors for cholangiocarcinoma are primary sclerosing cholangitis (PSC) with a lifetime risk 10–40%, parasitic infection, previous sphincteroplasty, congenital anomalies of the biliary tree (choledochal cyst, Caroli’s disease, anomalous pancreaticobiliary duct junction), and chronic biliary inflammatory disease (hepatitis B/C, liver cirrhosis, recurrent pyogenic cholangitis). The most common presentation is painless jaundice and weight loss in the setting of extrahepatic duct involvement. In Western countries, 80% are extrahepatic (20% distal and 60% hilar) and 20% are intrahepatic.
SPECIAL NOTES
Click here and share on TWITTER
• Ca 19–9 can be elevated in up to 85% of patients with cholangiocarcinoma, but is not specific; elevation can also occur in the setting of obstructive jaundice without malignancy. If it remains elevated after biliary decompression, it could indicate the presence of malignancy. Elevated pre- and postoperative Ca 19–9 predict poor survival.
• For perihilar tumors, decisions regarding which side of the liver to resect depend on right- or left-sided dominance, volume of future liver remnant, and the extent of vascular and ductal involvement.
• Some centers report that 30–50% of tumors will be deemed unresectable at the time of surgery, despite accurate preoperative imaging.
• Quality Indicators: Pathologic Analysis—R0 margin, regional lymphadenectomy includes three or more LN.
SURGICAL MANAGEMENT
Intrahepatic cholangiocarcinoma: Surgical resection is the only potential cure with removal of involved liver segments. There is emerging evidence that recommends a routine hilar LN and dissection for its prognostic value, M1 disease includes involvement of celiac,periaortic or caval LN.
Distal bile duct (below the cystic duct): Surgical resection is the only potential cure. Pancreaticoduodenectomy including en bloc resection of extrahepatic bile duct and gallbladder. Regional nodes include: Hilar (CBD, common hepatic, portal, cystic), Posterior and anterior pancreaticoduodenal Nodes along SMV, Nodes along right and lateral wall of SMA.
Hilar (above the cystic duct): En bloc resection of extrahepatic bile duct and gallbladder, including right and left hepatectomy, or extended right/left hepatectomy, Caudate lobe should be removed. Regional nodes include: Hilar (CBD, hepatic,portal, cystic), Pericholedochal nodes in hepatoduodenal ligament.
Liderança Cirúrgica
Tradicionalmente, a marca de um grande cirurgião está relacionada à habilidade técnica, conhecimento e perspicácia diagnóstica, enquanto pouco foco é dado a outras habilidades de Liderança. Hoje, as habilidades não técnicas, como habilidades de comunicação e liderança, acabam se traduzindo em maior segurança do paciente, experiência e resultados. O dia em que o cirurgião inicia seu primeiro trabalho o define como um líder, e isso é particularmente verdadeiro para o cirurgião do Aparelho Digestivo, pois é imediatamente considerado um especialista. Os cirurgiões são líderes preparados para aproveitar as muitas oportunidades de desempenho que as posições acadêmicas fornecem para executar seus interesses fora do atendimento tradicional ao paciente. Algumas pessoas nascem com habilidades de liderança e outras as desenvolvem com o tempo. É claro que esse processo deve começar cedo e que os estudantes de medicina e residentes devem estar preparados para papéis de liderança conforme RODRIGO VIANA explica neste vídeo para ajudar no desenvolvimento das habilidades críticas e não clínicas relacionadas à liderança de uma equipe e ao ensino. Para alguns, os papéis principais podem mudar ou desviar a carreira do atendimento ao paciente. Para outros, um equilíbrio entre as carreiras clínicas e administrativas pode ser cumprido em um papel definido. Independentemente disso, estabelecer metas e trabalhar para alcançá-las dentro da construção de uma equipe é a marca de todos os líderes de sucesso.
Preoperative Biliary Drainage
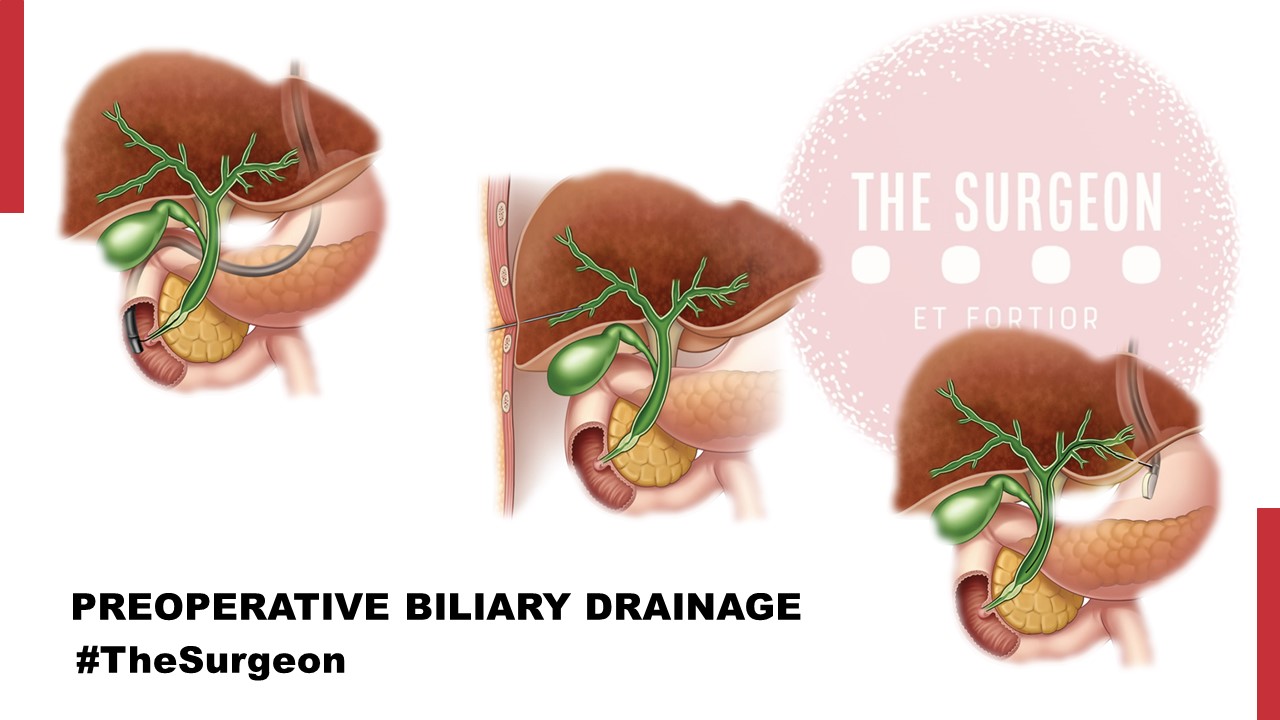
The most common presenting sign for patients with malignancy of the periampullary region is obstructive jaundice. While a significant proportion of these patients will be asymptomatic, the deleterious systemic consequences of uncontrolled hyperbilirubinemia may still occur. Furthermore, symptoms such as pruritus can be debilitating and have a significant impact on the quality of life. Thus, some have advocated preoperative drainage of the biliary system in patients with resectable periampullary malignancies, given widespread availability of endoscopic retrograde cholangiopancreatography and its perceived safety profile. On the other hand, the purported benefits of routine preoperative drainage in this patient population (namely, resolution of symptoms in symptomatic patients while awaiting surgery, restoration of the enterohepatic cycle, and a potential decrease in postoperative morbidity) have proven to be largely theoretical, and now there are high-quality phase III data that demonstrate the deleterious effects of routine stenting. A seminal study originating from the Netherlands in 2010 evaluated this issue in the only modern randomized controlled trial to date evaluating preoperative endoscopic biliary decompression for these patients. In their multicenter study, they randomized 202 patients with newly diagnosed pancreatic head cancer and bilirubin levels between 2.3 and 14.6 mg/dL to preoperative biliary drainage for 4–6 weeks vs. immediate surgery which was to be performed within a week of enrollment. The primary endpoint was the development of serious complications within 120 days after randomization. Serious complications were defined as complications related to the drainage procedure or the surgical intervention that required additional medical, endoscopic, or surgical management, and that resulted in prolongation of the hospital stay, readmission to the hospital, or death. The reported overall rate of serious complications in this study favored the immediate surgery group (39 vs. 74%; RR 0.54–95% [CI], 0.41–0.71; P < 0.001), complications related to surgery were equivalent (37 vs. 47%; P = 0.14), and there was no difference in mortality rates or length of hospital stay. The observed drainage-related complications included a 15% rate of stent occlusion, 30% need for exchange, and 26% incidence of cholangitis.
“Based on these results, the authors concluded that the morbidity associated with the drainage procedure itself had an additive effect on the postoperative morbidity of patients undergoing pancreatic head resection for cancer and recommended against its routine use in this population.“
A Cochrane systematic review of all available randomized studies (including the abovementioned study by van der Gaag et al.) evaluating preoperative biliary drainage was published in 2012. In this study, Fang et al. assessed the impact of this intervention on survival, serious morbidity (defined as Clavien-Dindo grade 3 or 4), and quality of life. Furthermore, they sought to assess differences in total length of hospital stay and cost. They identified six randomized trials of which four used percutaneous transhepatic biliary drainage and the remaining two used endoscopic sphincterotomy and stenting. The pooled analysis of 520 patients (of which 51% underwent preoperative biliary drainage) showed no difference in mortality, but importantly, it showed a significantly higher incidence of serious morbidity in the preoperative drainage group with a rate ratio (RaR) of 1.66 (95% CI 1.28–2.16;P = 0.002). There was no difference in length of hospital stay and not enough data reported for analysis of cost or quality of life.
“Based on the available level 1 data, the authors concluded that there was no evidence to support or refute routine preoperative biliary drainage in patients with obstructive jaundice.“
However, this review also underscored the fact that preoperative biliary drainage may be associated with an increased rate of adverse events and thus questioned the safety of this practice. This Cochrane review included old studies that evaluated patients undergoing percutaneous drainage, a technique used less frequently today for periampullary malignancies. Furthermore, several of these trials included patients with hilar and other types of biliary obstruction. However, the concept of preoperative decompression, as well as its purported benefits and observed results, may be reasonably extrapolated to patients with periampullary lesions.
Surgical Options of Hepatocellular carcinoma
INTRODUCTION
Liver cancer is the sixth most common cancer and, in 2018, was the fourth leading cause of cancer-related death worldwide. The rates of incidence and mortality are approximately 2 to 3 times higher for men than for women. Hepatocellular carcinoma (HCC) is the most common primary liver cancer and accounts for 75% to 85% of diagnoses, followed by intrahepatic cholangiocarcinoma (10%–15%), and other rare liver histologies. The improvement and safety of surgical techniques for liver resection and transplant, and advancements in ablation, transarterial chemoembolization (TACE), and systemic therapies have expanded the treatment options for patients with HCC. Liver transplant is the ideal treatment option for patients with HCC and poorly compensated liver disease because it removes both HCC and damaged liver and reduces the risk for early recurrence. However, shortages in donor liver and long waiting times to transplant are significant barriers to this treatment approach. As such, liver resection remains an effective treatment option for patients with HCC. The use of a multidisciplinary approach and the knowledge of each therapeutic option is critical in the management of patients with HCC.
SURGICAL RESECTION
Minimal future liver remnant requirements
Liver resection remains the treatment of choice for HCC. Two major preoperative considerations for HCC resection are the patient’s liver function and the predicted future liver remnant (FLR). The intrinsic liver function of patients with HCC is often impaired because this patient population generally has chronic liver disease, including viral hepatitis, alcoholic hepatitis, and nonalcoholic steatohepatitis. As such, studies report that more FLR is needed for patients undergoing resection for HCC than for patients undergoing resection of secondary liver cancer (ie, metastatic disease). The minimal requirement of FLR/standardized liver volume (standardized liver volume 5 x 794 1 1267.28 x body surface area) is 30% in patients with hepatic injury and fibrosis and 40% in patients with cirrhosis, whereas it is 20% to 25% for patients with normal liver.
Anatomic resection versus nonanatomic resection
Anatomic resection of Couinaud segment for small HCC was reported in 1981 by Makuuchi and colleagues. HCC frequently invades to the intrahepatic vascular structures and spreads through the portal vein. As such, the complete removal of tumor-bearing portal territory was reported to be theoretically superior to nonanatomic resection. The technique proposed by Makuuchi and colleagues is detailed as follows: (1) under the guidance of intraoperative ultrasonography, the portal vein of interest is identified and punctured using a 22-gauge needle; (2) blue dye is injected into the portal vein; (3) the territory of the dyed surface is marked using electrocautery; and (4) liver resection is performed using ultrasonography guidance and intersegmental hepatic veins are exposed. This technique was recently refined using fluorescence imaging. By using transportal injection or systemic intravenous injection of indocyanine green, the portal vein territory was more clearly visualized on the liver surface compared with the traditional method. Many retrospective studies reported that anatomic resection was associated with better survival and lower recurrence than nonanatomic resection. In contrast, other studies showed that survival did not differ significantly between patients undergoing anatomic resection and those undergoing nonanatomic resection. Therefore, this clinical question remains unanswered and needs to be further elucidated.
Laparoscopic liver resection
Laparoscopic liver resection (LLR) has been increasingly used worldwide. In their systemic review, Nguyen and colleagues reported on the safety of LLR with low rates of morbidity and mortality for both major and minor resections, as well as appropriate oncologic results compared with open liver resection (OLR). These results are most likely caused by patient selection and the advantages of the laparoscopic approach, including a magnified view and the hemostatic effect caused by pneumoperitoneum. Three retrospective studies including more than 200 patients showed that the 5-year overall survival (OS) was not significantly different between patients undergoing LLR for HCC and those undergoing OLR for HCC. However, no randomized controlled trials (RCTs) comparing long-term outcomes in patients undergoing LLR versus OLR for HCC have been reported. For patients with colorectal liver metastases, a recent RCT (Oslo-CoMet study) showed that median OS in patients undergoing LLR was similar to those undergoing OLR: 80 months versus 81 months.
Liver Resection Versus Ablation
It remains unclear whether liver resection or ablation is the most effective treatment of small HCC lesions. To answer this clinical question, 5 RCTs have been reported. Two of these studies showed that liver resection was associated with better survival than radiofrequency ablation and 3 showed that survival did not differ significantly between patients undergoing resection and those undergoing ablation. The shortcomings of these RCTs include insufficient patient follow-up; unclear treatment allocation; and different inclusion criteria, including tumor number, tumor diameter, and Child-Pugh grade. Nonetheless, for patients with small HCCs (ie,<3 cm), the current evidence shows that both resection and ablation can be recommended.
Liver Resection Versus Transarterial Chemoembolization
There has been 1 RCT comparing the outcomes of patients undergoing resection for HCC with those undergoing TACE. For patients outside of Milan criteria, resection was associated with better survival than TACE. The authors found 8 cohort studies comparing outcomes after resection with TACE using the propensity score adjustment. Although the studies had different inclusion criteria, the data show that resection is associated with better survival than TACE in selected patients who have multiple HCCs.
Liver Resection Versus Liver Transplant
Liver transplant is an established treatment option for patients who have early-stage HCC and poorly compensated cirrhosis and/or portal hypertension. However, the preferred treatment of patients who have early-stage HCC and wellcompensated cirrhosis is not established. Several retrospective studies have evaluated outcomes after liver resection for HCC in this setting, comparing them with those of transplant. However, most are limited by small sample sizes and low statistical power. No prospective studies have been performed on this topic given the inability to randomize patients to liver resection versus transplant. The authors found 2 studies including more than 200 patients. They both suggest that transplant is associated with better survival than liver resection in patients within Milan criteria and Child-Pugh A or B. Nonetheless, it should be noted that graft availability and waiting times for transplant differ between countries, which greatly influences the selection of liver resection versus transplant for patients with early-stage HCC.
CONCLUSION
The current evidence suggests that, for patients with small HCC lesions (<3 cm), OS is likely to be similar for patients undergoing liver resection versus ablation. For selected patients with multiple HCCs, liver resection may be associated with better OS than TACE. For the past 10 years, sorafenib has been the only effective medical therapy available for unresectable HCC. Recently, several promising new therapies, including multikinase inhibitors and immunotherapies, have been reported. Perioperative use of these new therapies may further improve outcomes in patients undergoing liver resection for HCC and potentially change the current treatment guidelines.

Laparoscopic Liver Resection
INTRODUCTION
Laparoscopic hepatic resection is an emerging option in the field of hepatic surgery. With almost 3000 laparoscopic hepatic resections reported in the literature for benign and malignant tumors, with a combined mortality of 0.3% and morbidity of 10.5%, there will be an increasing demand for minimally invasive liver surgery. Multiple series have been published on laparoscopic liver resections; however, no randomized controlled trial has been reported that compares laparoscopic with open liver resection. Large series, meta-analyses, and reviews have thus far attested to the feasibility and safety of minimally invasive hepatic surgery for benign and malignant lesions.
THECNICAL ASPECTS
The conversion rate from a laparoscopic approach to an open procedure was 4.1%. The most common type of laparoscopic liver resection performed is a wedge resection or segmentectomy (45%), followed by left lateral sectionectomy (20%). Major anatomic hepatectomies are still less frequently performed: right hepatectomy (9%) and left hepatectomy (7%). Cumulative morbidity and mortality was 10.5% and 0.3%.
BENEFITS OF LAPAROSCOPIC APPROACH
More importantly, almost all the studies comparing laparoscopic with open liver resection consistently showed a significant earlier discharge to home after laparoscopic liver resection. Lengths of stay were variable based on the country of origin of the studies but were consistently shorter for laparoscopic liver resection. Three studies published in the United States presented a length of stay of 1.9 to 4.0 days after laparoscopic liver resection. Studies from Europe showed an average length of stay of 3.5 to 10 days whereas those from Asia reported an average of length of stay of 4 to 20 days after laparoscopic liver resection.
COST ANALYSIS
Vanounou and colleagues used deviation-based cost modeling to compare the costs of laparoscopic with open left lateral sectionectomy at the University of Pittsburgh Medical Center. They compared 29 laparoscopic with 40 open cases and showed that patients who underwent the laparoscopic approach faired more favorably with a shorter length of stay (3 vs 5 days, P<.0001), significantly less postoperative morbidity (P 5 .001), and a weighted-average median cost savings of $1527 to $2939 per patient compared with patients who underwent open left lateral sectionectomy.
SURGICAL MARGINS
Initial concerns about the adequacy of surgical margins and possible tumor seeding prevented the widespread adoption of laparoscopic resection approaches for liver cancers. In comparison studies, there were no differences in margin-free resections between laparoscopic and open liver resection. In addition, no incidence of port-site recurrence or tumor seeding has been reported. With more than 3000 cases of minimally invasive hepatic resection reported in the literature (and no documentation of any significant port-site or peritoneal seeding), the authors conclude that this concern should not prevent surgeons from accepting a laparoscopic approach.
SURVIVAL OUTCOMES
There were no significant differences in overall survival in the 13 studies that compared laparoscopic liver resection with open liver resection for cancer. For example, Cai and colleagues showed that the 1-, 3-, and 5-year survival rates after laparoscopic resection of HCC were 95.4%, 67.5%, and 56.2% versus 100%, 73.8%, and 53.8% for open resection. For resection of colorectal cancer liver metastasis, Ito and colleagues showed a 3-year survival of 72% after laparoscopic liver resection and 56% after open liver resection whereas Castaing and colleagues51 showed a 5-year survival of 64% after laparoscopic liver resection versus 56% after open liver resection.
CONCLUSION
Compared with open liver resections, laparoscopic liver resections are associated with less blood loss, less pain medication requirement, and shorter length of hospital stay. A randomized controlled clinical trial is the best method to compare laparoscopic with open liver resection; however, such a trial may be difficult to conduct because patients are unlikely to subject themselves to an open procedure when a minimally invasive approach has been shown feasible and safe in experienced hands. In addition, many patients would have to be accrued to detect a difference in complications that occur infrequently. Short of a large randomized clinical trial, meta-analysis and matched comparisons provide the next best option to compare laparoscopic with open liver resection. For laparoscopic resection of HCC or colorectal cancer metastases, there has been no difference in 5-year overall survival compared with open hepatic resection. In addition, from a financial standpoint, the minimally invasive approach to liver resection may be associated with higher operating room costs; however, the total hospital costs were offset or improved due to the associated shorter length of hospital stay with the minimally invasive approach.
Medically-Necessary, Time Sensitive: (MeNTS) Score
Operating During The COVID-19 Coronavirus Pandemic
“At the University of Chicago, members of the Department of Surgery decided to investigate this issue more precisely. As stay-at-home restrictions in some states are easing, and as non-emergency medical care is being reconsidered, how does one possibly triage the thousands upon thousands of patients whose surgeries were postponed? Instead of the term “elective,” the University of Chicago’s Department of Surgery chose the phrase “Medically-Necessary, Time Sensitive” (MeNTS). This concept can be utilized to better assess the acuity and safety when determining which patients can get to the operating room in as high benefit/low risk manner as possible. And unlike in any recent time in history, risks to healthcare staff as well as risks to the patient from healthcare staff, are now thrown into the equation. The work was published in the April issue of the Journal of the American College of Surgeons.
On March 17, 2020, the American College of Surgeons recommended that all “elective” surgeries be canceled indefinitely. These guidelines were published, stating that only patients with “high acuity” surgical issues, which would include aggressive cancers and severely symptomatic disease, should proceed. Based on the Elective Surgery Acuity Scale (ESAS), most hospitals were strongly encouraged to cancel any surgery that was not high acuity, including slow-growing cancers, orthopedic and spine surgeries, airway surgeries, and any other surgeries for non-cancerous tumors. Heart surgeries for stable cardiac issues were also put on hold. Patients and surgeons waited. Some patients did, indeed undergo non-Covid-19-related surgeries. But most did not. Redeployment is gradually turning to re-entry.
The re-entry process for non-urgent (yet necessary) surgeries is a complicated one. Decisions and timing, based on a given hospital’s number and severity of Covid-19 patients, combined with a given city or state’s current and projected number of Covid-19 cases, how sick those patients will be, and whether or not a second surge may come, involves a fair amount of guesswork. As we have all seen, data manipulation has become a daily sparring match in many arenas. The authors of the study created an objective surgical risk scoring system, in order to help hospitals across this country, as well as others across the world, better identify appropriate timing regarding which surgeries can go ahead sooner rather than later, and why. They factored several variables into their equation, to account for the multiple potential barriers to care, including health and safety of hospital personnel. They created scoring systems based on three factors: Procedure, Disease and Patient Issues.
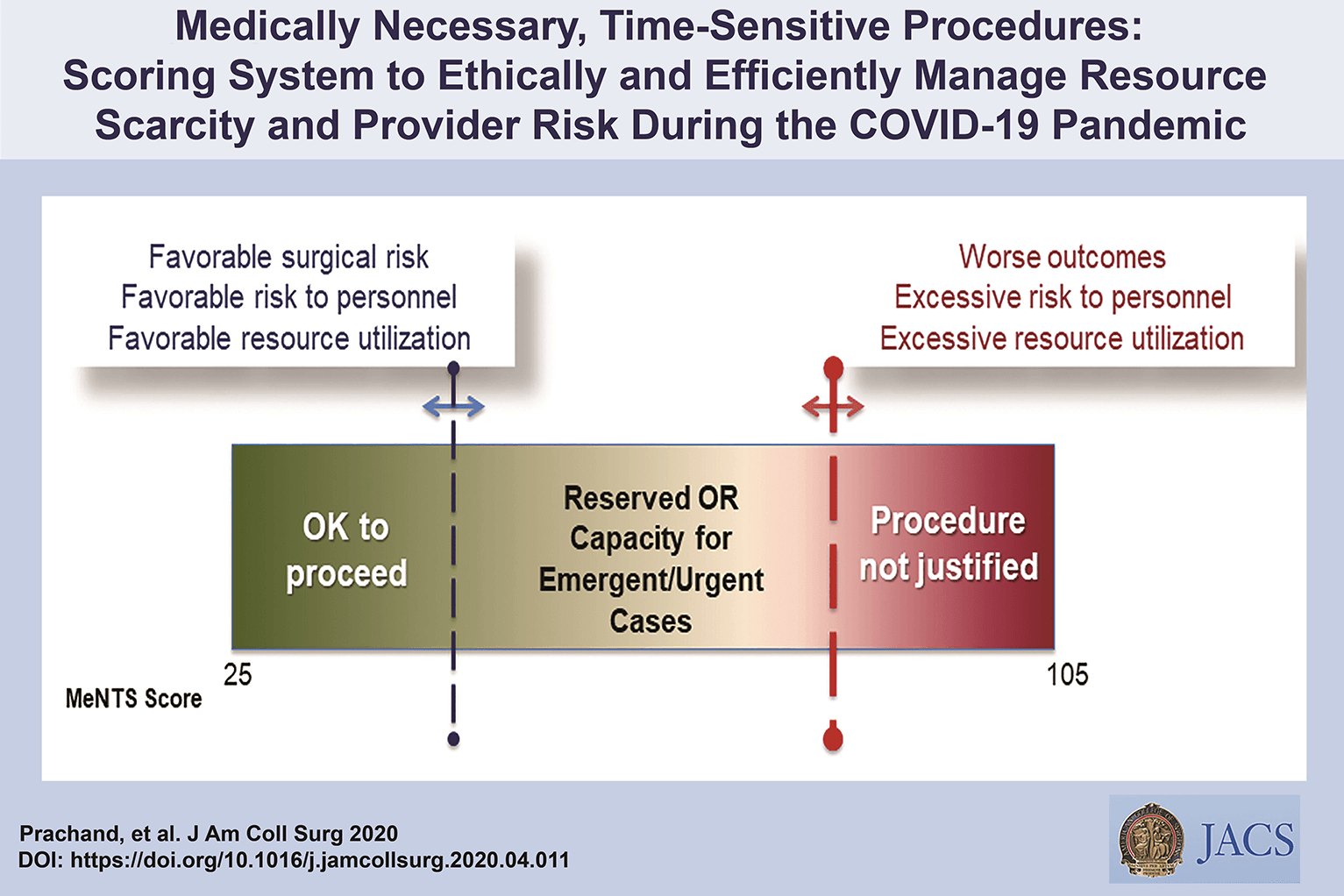
CALCULATE MeNTS SCORE HERE
The authors of the study created an objective surgical risk scoring system, in order to help hospitals across this country, as well as others across the world, better identify appropriate timing regarding which surgeries can go ahead sooner rather than later, and why. They factored several variables into their equation, to account for the multiple potential barriers to care, including health and safety of hospital personnel. Each patient would receive an overall conglomerate score, based on all of these factors, with the lower risks giving them more favorable scores to proceed with surgery soon, and the higher risks giving patients a higher score, or higher risk regarding proceeding with surgery, meaning it may be safest, for now, to wait.
Dr. Jeffrey Matthews, senior author of the paper, and Department Chair at the University of Chicago, stated that this model is reproducible across hospital systems, in urban, rural, and academic settings. And in the event of potential unpredictable surges of Covid-19 cases, the scoring system “helps prioritize cases not only from the procedure/disease standpoint but also from the pandemic standpoint with respect to available hospital resources such as PPE, blood, ICU beds, and [regular hospital] beds.”
The scoring system is extremely new, and the coming weeks will reveal how patients, surgeons and hospitals are faring as patients without life-and-death emergencies and/or Covid-19 complications gradually begin filling the operating rooms and hospital beds. In addition, and perhaps just as important, the study authors note that creating systems whereby healthcare resources, safety, and impact on outcomes need to be considered more carefully for each patient intervention, the larger impact of each intervention on public health will be better understood: not only for today’s pandemic, but also in future, as yet unknown, global events.”
Source: Nina Shapiro, 2020
Discover our surgical video channel and lectures associated with the surgeon blog.
Share and Join: https://linktr.ee/TheSurgeon
Covid-19 and Digestive Surgery
The current world Covid-19 pandemic has been the most discussed topic in the media and scientific journals. Fear, uncertainty, and lack of knowledge about the disease may be the significant factors that justify such reality. It has been known that the disease presents with a rapidly spreading, it is significantly more severe among the elderly, and it has a substantial global socioeconomic impact. Besides the challenges associated with the unknown, there are other factors, such as the deluge of information. In this regard, the high number of scientific publications, encompassing in vitro, case studies, observational and randomized clinical studies, and even systematic reviews add up to the uncertainty. Such a situation is even worse when considering that most healthcare professionals lack adequate knowledge to critically appraise the scientific method, something that has been previously addressed by some authors. Therefore, it is of utmost importance that expert societies supported by data provided by the World Health Organization and the National Health Department take the lead in spreading trustworthy and reliable information.
Discover our surgical video channel and lectures associated with the surgeon blog.
Share and Join: https://linktr.ee/TheSurgeon
#Medicine #Surgery #GeneralSurgery #DigestiveSurgery
#TheSurgeon #OzimoGama
Laparoscopic JEJUNOSTOMY
Many oncological patients with upper gastrointestinal (GI) tract tumours, apart from other symptoms, are malnourished or cachectic at the time of presentation. In these patients feeding plays a crucial role, including as part of palliative treatment. Many studies have proved the benefits of enteral feeding over parenteral if feasible. Depending on the tumour’s location and clinical stage there are several options of enteral feeding aids available. Since the introduction of percutaneous endoscopic gastrostomy (PEG) and its relatively easy application in most patients, older techniques such as open gastrostomy or jejunostomy have rather few indications.
The majority of non-PEG techniques are used in patients with upper digestive tract, head and neck tumours or trauma that renders the PEG technique unfeasible or unsafe for the patient. In these patients, especially with advanced disease requiring neoadjuvant chemotherapy or palliative treatment, open gastrostomy and jejunostomy were the only options of enteral access. Since the first report of laparoscopic jejunostomy by O’Regan et al. in 1990 there have been several publications presenting techniques and outcomes of laparoscopic feeding jejunostomy. Laparoscopic jejunostomy can accompany staging or diagnostic laparoscopy for upper GI malignancy when the disease appears advanced, hence avoiding additional anaesthesia and an operation in the near future.
In this video the author describe the technique of laparoscopic feeding jejunostomy applied during the staging laparoscopy in patient with advanced upper gastrointestinal tract cancer with co-morbid cachexy, requiring enteral feeding and neoadjuvant chemotherapy.
Welcome and get to know our Social Networks through the following link
Ozimo Gama’s Social Medias
#AnatomiaHumana #CirurgiaGeral #CirurgiaDigestiva #TheSurgeon
Enhanced Recovery After Liver Surgery
The first postoperative fast-track protocols, also called “enhanced recovery after surgery” (ERAS), were instituted by colorectal surgeons almost three decades ago in order to modulate surgical stress and hasten recovery. Since then, the implementation of enhanced recovery programs has had an exponential expansion across most surgical specialties, including gynecology, urology, breast, vascular, and orthopedic surgery.
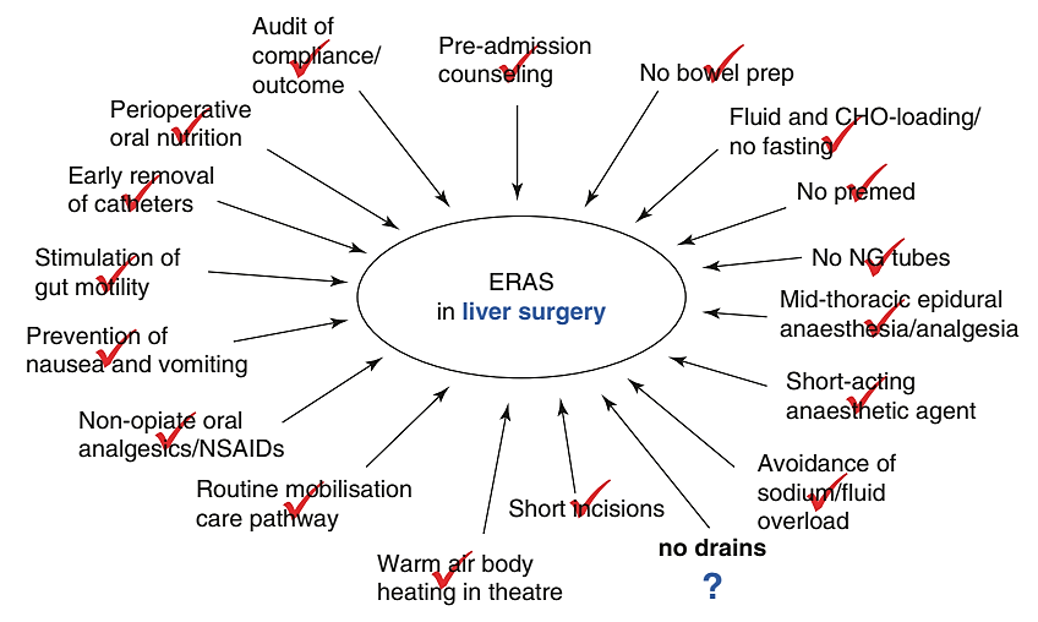
“Enhanced recovery after liver surgery” (ERLS) was first introduced in 2008 and has incrementally gained acceptance as being an integral part of perioperative care for hepatectomy patients. Several outcome metrics have shown to be improved with the adoption of a multimodal evidencebased strategy in liver surgery, many of which are also shared by other surgical specialties practicing in an enhanced recovery framework.
Improved clinical outcomes such as length of stay, morbidity rates, and hospital costs tend to support implementation of fast-track programs in general, but other metrics specific to liver surgery and to patients with colorectal liver metastases (CLM) further endorse this strategy when managing CLM. The implementation of an ERLS program represents a collaborative approach in which the different team players, including anesthesia, surgery, nutrition, pharmacy, nursing, and most importantly the patient and his/her family, engage actively in the perioperative pathway, in an evidence-based, patient-centered approach. The development of such programs also requires dedicated continuing education for the team members, flexibility in terms of perioperative management and decisionmaking by the health-care providers, support from the hospital administration, and systematic quality control measures to ensure implementation and accurate reporting. This review study the different core elements of ERLS and discuss different outcomes associated with this system-based approach, with an emphasis on oncological patients.
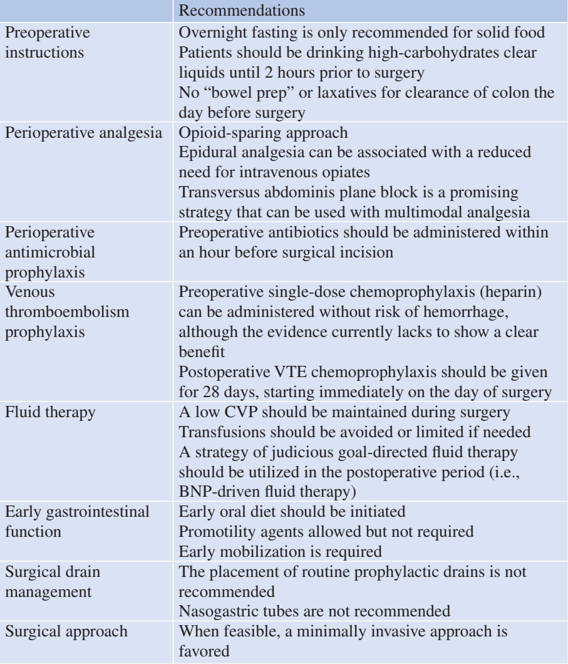
Interference with oncological treatment plans can negatively affect patients’ longterm outcomes but can also be detrimental to quality of life and overall functional status. Patient-reported outcomes (PROs) attempt to capture the patients’ perspective for a given intervention or treatment strategy, which are particularly important in oncological patients. Day et al. reported that the implementation of ERLS was beneficial for patients in terms of functional recovery, and although no significant differences were detected in terms of symptom burden, the impact of ERLS was shown to accelerate functional recovery by returning to baseline interference earlier. This positive effect from ERLS seems more pronounced in patients undergoing open hepatectomy over those already benefiting from minimally invasive surgery.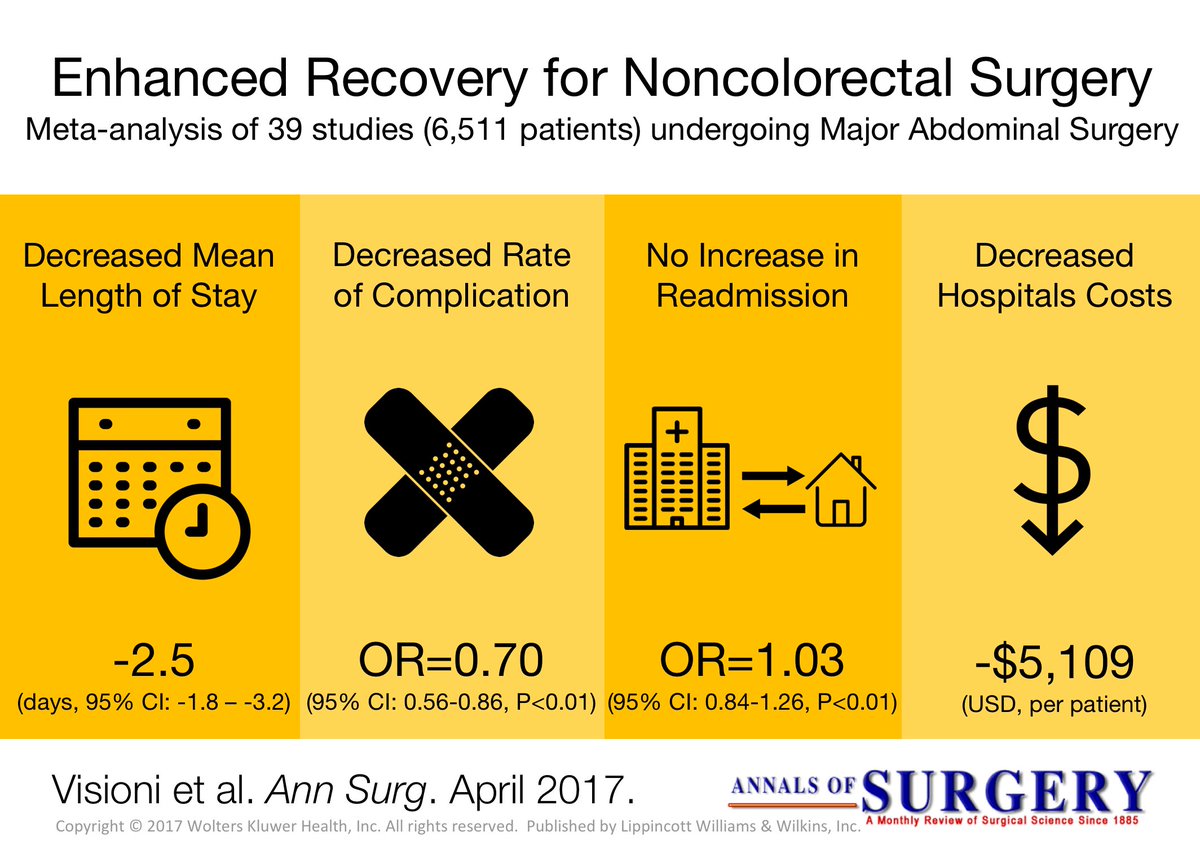
Metastatic Colorectal Cancer
Over 50% to 60% of patients diagnosed with colorectal cancer will develop hepatic metastases during their lifetime. Resection for hepatic metastases has been a routine part of treatment for colorectal cancer since the publication of a large single-center experience demonstrating its safety and efficacy.
Predictors of poor outcome in that study included node-positive primary, disease-free interval <12 months, more than one tumor, tumor size >5 cm, and carcinoembryonic antigen level >200 ng/mL.
Traditional teaching suggested that hepatic resection for metastatic colorectal cancer to the liver, if technically feasible,should be performed only for fewer than four metastases. However, later studies challenged this paradigm. In a series of 235 patients who underwent hepatic resection for metastatic colorectal cancer, the 10-year survival rate of patients with four or more nodules was 29%, nearly comparable to the 32% survival rate of patients with only a solitary tumor metastasis.
In the Memorial Sloan-Kettering Cancer Center series of 98 patients with four or more colorectal hepatic metastases who underwent resection between 1998 and 2002, the 5-year actuarial survival was 33%. Furthermore, improved chemotherapeutic regimens and surgical techniques have produced aggressive strategies for the management of this disease.
Many groups now consider volume of future liver remnant and the health of the background liver, and not actual tumor number, as the primary determinants in selection for an operative approach. Hence, resectability is no longer defined by what is actually removed, but indications for hepatic resection now center on what will remain after resection.
Use of neoadjuvant chemotherapy, portal vein embolization, twostage hepatectomy, simultaneous ablation, and resection of extrahepatic tumor in select patients have increased the number of patients eligible for a surgical approach.
Oncologic Principles for GASTRIC CANCER Surgery
Good surgery for gastric cancer can be summarized in the mnemonic “OPERATIONS”: Oncologic Principles, Good Exposure, Understanding Anatomy, Comprehensive Total Approach, Meticulous Lymph Node Dissection, and Patients’ Safety. Surgery is as much an art as a technique, and the surgeon’s philosophy is an important component of practice. The surgeon should see the surgery, first and foremost, as for the patient’s benefit and have the same concern and regard for the patient as for a family member. The patient with gastric cancer has only one chance to be cured by surgery. Often this requires innovation and the adaptation of new technology by the surgeon. However, innovations must always honor accepted oncologic principles and practices a nd be based on sound scientific rationale.
ONCOLOGIC PRINCIPLES
There are fundamental differences between surgery performed in patients with cancer and in patients with other benign conditions. Protocols based on oncological principles must be followed throughout surgical procedures on cancer patients to prevent contamination with, or dissemination of, the cancer cells. The fundamental goal of cancer surgery is complete surgical resection of tumor, en bloc lymph node dissection, and careful hemostasis. If this goal is not achieved, cancer cells can be disseminated through broken lymphatics and vessels. The extent of gastric resection should be decided upon based on the location of tumor in the stomach and the safety resection margin so that microscopic tumors are not left in remaining stomach. The “no-touch” technique should be used during the entire procedure. The no-touch technique entails wrapping the primary tumor. This is especially important in cases of serosa-positive gastric cancer, in which it is of utmost importance to prevent iatrogenic peritoneal seeding through the surgeon’s hands. Unnecessary manipulation and dissection should be avoided as mitogenic factors for wound healing could be produced in response to the surgery; these could stimulate the proliferation of undetected micrometastatic tumors that remained after surgery.
Ischaemic Preconditioning applied to LIVER SURGERY
- INTRODUCTION
The absence of oxygen and nutrients during ischaemia affects all tissues with aerobic metabolism. Ischaemia of these tissues creates a condition which upon the restoration of circulation results in further inflammation and oxidative damage (reperfusion injury). Restoration of blood flow to an ischaemic organ is essential to prevent irreversible tissue injury, however reperfusion of the organ or tissues may result in a local and systemic inflammatory response augmenting tissue injury in excess of that produced by ischaemia alone. This process of organ damage with ischaemia being exacerbated by reperfusion is called ischaemia-reperfusion (IR). Regardless of the disease process, severity of IR injury depends on the length of ischaemic time as well as size and pre-ischaemic condition of the affected tissue. The liver is the largest solid organ in the body, hence liver IR injury can have profound local and systemic consequences, particularly in those with pre-existing liver disease. Liver IR injury is common following liver surgery and transplantation and remains the main cause of morbidity and mortality.
2. AETIOLOGY
The liver has a dual blood supply from the hepatic artery (20%) and the portal vein (80%). A temporary reduction in blood supply to the liver causes IR injury. This can be due to a systemic reduction or local cessation and restoration of blood flow. Liver resections are performed for primary or secondary tumours of the liver and carry a substantial risk of bleeding especially in patients with chronic liver disease. Significant blood loss is associated with increased transfusion requirements, tumour recurrence, complications and increased morbidity and mortality. Several methods of hepatic vascular control have been described in order to minimise blood loss during elective liver resection. The simplest and most common method is inflow occlusion by applying a tape or vascular clamp across the hepatoduodenal ligament (Pringle Manoeuvre). This occludes both the arterial and portal vein inflow to the liver and leads to a period of warm ischaemia (37 °C) to the liver parenchyma resulting in ‘warm’ IR injury when the temporary inflow occlusion is relieved. In major liver surgery, extensive mobilisation of the liver itself without inflow occlusion results in a significant reduction in hepatic oxygenation.

3. PATOPHYSIOLOGY and RISK FACTORS
A complex cellular and molecular network of hepatocytes, Kupffer cells, liver sinusoidal endothelial cells (LSEC), leukocytes and cytokines play a role in the pathogenesis of IR injury. In general, both warm and cold ischaemia share similar mechanisms of injury. Hepatocyte injury is a predominant feature of warm ischaemia, whilst endothelial cells are more susceptible to cold ischaemic injury. There are currently no proven treatments for liver IR injury. Understanding this complex network is essential in developing therapeutic strategies in prevention and treatment of IR injury. Identifying risk factors for IR injury are extremely important in patient selection for liver surgery and transplantation. The main factors are the donor or patient age, the duration of organ ischaemia, presence or absence of liver steatosis and in transplantation whether the donor organ has been retrieved from a brain dead or cardiac death donor.
4. PREVENTION and TREATMENT
There is currently no accepted treatment for liver IR injury. Several pharmacological agents and surgical techniques have been beneficial in reducing markers of hepatocyte injury in experimental liver IR, however, they are yet to show clinical benefit in human trials. The following is an outline of current and future strategies which may be effective in reducing the detrimental effects of liver IR injury in liver surgery and transplantation.
4.1 SURGICAL STRATEGIES
Inflow occlusion or portal triad clamping (PTC) can be continuous or intermittent; alternating between short periods of inflow occlusion and reperfusion. Intermittent clamping (IC) increases parenchymal tolerance to ischaemia. Hence, prolonged continuous inflow occlusion rather than short intermittent periods results in greater degree of post-operative liver dysfunction. IC permits longer total ischaemia times for more complex resections. Alternating between 15 min of inflow occlusion and 5 min reperfusion cycles can be performed safely for up to 120 min total ischaemia time. There is a potential risk of increased blood loss during the periods of no inflow occlusion. However, these intervals provide an opportunity for the surgeon to check for haemostasis and control small bleeding areas from the cut surface of the liver. The optimal IC cycle times are not clear, although intermittent cycles of up to 30 min inflow occlusion have also been reported with no increase in morbidity, blood loss or liver dysfunction compared to 15 min cycles. IC is particularly beneficial in reducing post-operative liver dysfunction in patients with liver cirrhosis or steatosis.
In liver surgery, IPC ( Ischaemic Preconditioning) involves a short period of ischaemia (10 min) and reperfusion (10 min) intraoperatively by portal triad clamping prior to parenchymal transection during which a longer continuous inflow occlusion is applied to minimise blood loss. It allows continuous ischaemia times of up to 40 min without significant liver dysfunction. However, the protective effect of IPC decreases with increasing age above 60 years old and compared to IC it is less effective in steatotic livers. Moreover, IPC may impair liver regeneration capacity and may not be tolerated by the small remnant liver in those with more complex and extensive liver resections increasing the risk of post-operative hepatic insufficiency.
In order to avoid direct ischaemic insult to the liver by inflow occlusion, remote ischaemic preconditioning (RIPC) has been used. RIPC involves preconditioning a remote organ prior to ischaemia of the target organ. It has been shown to be reduce warm IR injury to the liver in experimental studies. A recent pilot randomised trial of RIPC in patients undergoing major liver resection for colorectal liver metastasis used a tourniquet applied to the right thigh with 10 min cycles of inflation-deflation to induce IR injury to the leg for 60 min. This was performed after general anaesthesia prior to skin incision. A reduction in post-operative transaminases and improved liver function was shown without the use of liver inflow occlusion. These results are promising but require validation in a larger trial addressing clinical outcomes.
5. FUTURE PERSPECTIVES
Hepatic IR injury remains the main cause of morbidity and mortality in liver surgery and transplantation. Despite over two decades of research in this area, therapeutic options to treat or prevent liver IR are limited. This is primarily due to the difficulties in translation of promising agents into human clinical studies. Recent advances in our understanding of the immunological responses and endothelial dysfunction in the pathogenesis of liver IR injury may pave the way for the development of new and more effective and targeted pharmacological agents.
Surgical Management of CHRONIC PANCREATITIS

Chronic pancreatitis (CP) is a progressive, destructive, inflammatory process that ends in total destruction of the pâncreas and results in malabsorption, diabetes mellitus, and severe pain. The incidence and prevalence of CP are increasing in the worldwide and incidence is between 1.6 and 23 per 100 000 with increasing prevalence. The treatment of CP is complex; in the majority of cases na interdisciplinary approach is indicated that includes conservative, endoscopic, and surgical therapy. The surgical treatment of CP is based on two main concepts:preservation of tissue via drainage aims to protect against further loss of pancreatic function, and pancreatic resection is performed for nondilated pancreatic ducts, pancreatic head enlargement,or if a pancreatic carcinoma is suspected in the setting of CP.
RESECTIVE PROCEDURES
The vast majority of patients are seen with a ductal obstruction in the pancreatic head, frequently associated with an inflammatory mass. In these patients, pancreatic head resection is the procedure of choice; The partial pancreatoduodenectomy (PD) or Kausch-Whipple procedure, in its classic or pylorus-preserving variant, has been the procedure of choice for pancreatic head resection in CP for many years (Jimenez et al, 2003). The duodenum-preserving pancreatic head resections and its variants—the Beger (1985), Frey (1987), and Bern procedures (Gloor et al, 2001)—represent less invasive, organsparing techniques with equal long-term results. Only very few patients come to medical attention with smallduct disease (diameter of the pancreatic duct ❤ mm) and no mass in the pancreatic head. Possibly, a large majority of those patients from former series had unknown autoimmune pancreatitis. In these cases, a V-shaped excision of the anterior aspect of the pancreas is a safe approach, with effective pain management (Yekebas et al, 2006). In the rare case of a patient seen with segmental CP in the pancreatic body or tail, such as that seen as a result of posttraumatic ductal stenosis, a middle segment pancreatectomy or a pancreatic left resection may be the best approach.
CONCLUSION
The adequate therapy of CP is adjusted to the symptoms of the patient, the stage of the disease, and the morphology of pathologic changes of the pancreas. The surgical technique must be adjusted to the pathomorphologic changes of the pancreas. For patients with CP and an inflammatory mass in the head of the pancreas, the DPPHR is less invasive than a PD and is associated with comparable long-term results. The Bern modification of the DPPHR represents a technical variation that is equally effective but technically less demanding. Whether total pancreatectomy with islet cell transplantation is a viable therapy of CP remains to be proved by further studies. Surgical therapy provides effective long-term pain relief and improvement of quality of life, but it may not stop the decline of endocrine or exocrine pancreatic function. Strategies to improve or maintain endocrine and exocrine function in CP remain an interesting field of research.
Laparoscopic distal PANCREATECTOMY
Laparoscopic distal pancreatectomy has become a relatively standard operation and has been approached by a similar technique by multiple groups since its original description. Generally, four or five trocars are used to gain entrance to the abdominal cavity, but three-trocar LPD has been described. A “clockwise” technique results in an efficient, reliable, and uniform approach for removing the vast majority of lesions that are located to the left of the neck of the pancreas (Asbun & Stauffer, 2011). The technique begins with the positioning of the patient in a modified right lateral decubitus position. The degree of lateral positioning depends on the patient’s body habitus and the location of the lesion, as well as the tilting capabilities of the operative bed. The use of gravity assisted retraction with the patient in a reverse Trendelenburg position with the left flank elevated is a key component to successful exposure of the tail of the pancreas and the spleen. Four mid- to left-sided abdominal trocars are placed in a semicircle around the body and tail of the pancreas, including two 12 mm and two 5 mm trocars, and a five step clockwise method is used.
Step 1: Mobilization of the splenic flexure of the colon
and exposure of the pancreas
The first step is mobilization of the splenic flexure of the colon. The lateral attachments, splenocolic ligament, and gastrocolic ligament are succes-sively transected to allow access to the lesser sac. If the spleen is to be removed, the dissection proceeds cranially, and the short gastric vessels are transected up to the superior pole of the spleen. Sufficient mobilization of the colon allows for gravity-assisted retraction of the colon, and the stomach is completely freed from the anterior aspect of the body and tail of the pancreas. Infrequently, an additional trocar or tacking stitch is required to elevate the stomach to the anterior abdominal wall off the pancreas and out of the operative field.
Step 2: Dissection along the inferior edge of the pancreas
and choosing the site for pancreatic division
The second step is to identify the inferior border of the pancreas and create a window in the fibroadipose tissue plane between the retroperitoneum and the pancreas. This dissection is carried medially toward the lesion of interest. Intraoperative ultrasound is performed to clearly identify the lesion and the planned site of division of the pancreas.
Step 3: Pancreatic parenchymal division and ligation
of the splenic vein and artery
The third step is pancreatic parenchymal division and ligation of the splenic artery and vein. After dissecting around the pancreas in 360 degrees, a Penrose drain or suture is placed around the proposed site of division of the pancreas and is used to elevate the pancreas from the retroperitoneum. A band passer instrument is helpful for this part of the procedure. For distal pancreatectomy, the splenic vessels will often be dissected, ligated, and divided en bloc with the parenchyma. For subtotal resections with division of the pancreas at the neck, the underlying superior mesenteric vein and splenic vein are dissected away from the posterior aspect of the pancreas, and the celiac trunk is identified individually and dissected free from the neck and proximal body of the pancreas. Parenchymal transection is performed with a linear stapling device by using a slow, gradual, and stepwise compression technique. Thick tissue staples (open staple height of approximately 4 mm) with staple line reinforcement is preferred for almost any pancreas consistency, and the stapler is gradually closed in a stepwise manner over the course of several minutes to allow for parenchymal compression. Parenchymal transection and splenic vessel division are done individually for subtotal pancreatectomy for lesions located between the gastroduodenal artery and the celiac trunk.
Step 4: Dissection along the superior edge of the pancreas
The fourth step is to sweep the pancreas inferiorly and anteriorly off the retroperitoneum toward the splenic hilum. A deeper dissection plane that includes Gerota fascia and the left adrenal gland may be chosen for malig-nancies that appear to have posterior invasion from the pancreas.
Step 5: Mobilization of the spleen and specimen removal
The fifth step is the mobilization of the spleen from its diaphragmatic and retroperitoneal attachments and placement of the specimen within a bag for exteriorization. Major complications were seen in less than 10% of patients, and both the conversion rate and the clinically significant pancreatic fistula (grade B/C) rate by using the gradual stepwise compression stapled technique was seen in fewer than 5%. Operative drains were rarely placed.
Outcomes
The minimally invasive approach to resection of the left-sided pancreas by distal or subtotal pancreatectomy has gained acceptance and been used with an increasing frequency worldwide during the past decade. Multiple systematic reviews have demonstrated the safety of LDP and its superiority versus open distal pancreatectomy (ODP) for selected outcomes, such as blood loss, transfusion rates, and hospital stays; it must be remembered, however, that all these studies are retrospective in nature and therefore severely limited by significant selection bias. All studies showed similar reoperation rates and mortality, but most found a lower overall morbidity for the laparoscopic approach. Some studies identified lower rates of specific complications, such as wound infection and even pancreatic fistula. Although oncologic clearance was similar, most studies have shown that ODP is often the surgery of choice for larger tumors.
How to Make a Good STOMA

INTRODUCTION: Few other surgical procedures adversely affect a patient’s quality of life as much as a poorly functioning stoma. An ideal stoma meets two criteria: (1) The site is optimally matched to a patient’s variability in body form, physical ability and activities. (2) The construction minimises complications that relate to the use of stomal appliances and minimises technical failings such as parastomal hernia or prolapse.
SURGICAL ASPECTS
1.The Skin and Subcutaneous Incision
A circular stomal opening is generally preferred, though for temporary stomata a linear incision minimises skin loss and may improve cosmesis after closure. We favour making a cruciate incision with cutting electrocautery, each quadrant being excised in a curved fashion with electrocautery or curved (Mayo) scissors to prevent charring.
2.Muscle Fascia
A cruciate incision of the muscle fascia is generally used, mirroring that for the skin incision but without excision. It is common practice during laparotomy to align the muscle fasciotomy and skin incision by medial retraction of the rectus sheath using tissue-grasping forceps (e.g. Lanes’). This may reduce angulation of the bowel through the abdominal wall, though is unlikely to affect the duration of paralytic ileus in the post-operative phase and has little effect on eventual function.
3.Muscle
A muscle-splitting incision through rectus abdominis is advocated, though this may simply be a necessary anatomical consequence reflecting the preference for an anterior stoma distant from the umbilicus, iliac crest and midline wounds. Stomal formation lateral to rectus abdominis does not actually seem to increase the risk of para-stomal hernia formation. This is unsurprising, since muscle division and correct closure at apppendicectomy rarely leads to hernia formation.
4.Choice of Bowel for the Construction of a Stoma
The principles of good anastamotic healing apply equally to stomal construction. Attention to tissue handling, vascularity and lack of tension encourage primary healing at the muco-cutaneous junction. Poor technique risks separation of the muco-cutaneous junction and prolonged healing by granulation, leading to stenosis. Tension may worsen stomal or spout retraction and can lead to difficulties in attaching stomal appliances to a concave stoma, particularly if a tight limb of the stoma gives a skin fold crease. Similarly, impaired vascularity can turn stomata a worrying colour, particularly if inotropes are required for a critically ill patient, and although frank necrosis is rare, stenosis may result in the longer term.
“Patients often judge a surgeon’s technical ability by the external appearance of scars, and may also judge a surgeon’s care and precision by the appearance and function of an abdominal stoma.”
Tumor Markers in HPB Cancers

The “ideal” tumor marker is economical, easy to estimate in easily accessible body fluids like blood or urine, has high sensitivity and specificity, can be used to screen for a cancer, has prognostic and predictive value at diagnosis, and is reliable during treatment and follow-up. It does not exist as of now. Commonly used tumor markers in gastrointestinal, liver, biliary tract, and pancreatic cancers are alpha fetoprotein (AFP), CA19.9, carcinoembryonic antigen (CEA), and chromogranin A (CgA).
Alpha Fetoprotein (AFP)
Alpha fetoprotein (AFP) is a glycoprotein that is produced in the yolk sac and the fetal liver. It is the most commonly used tumor marker for hepatocellular carcinoma (HCC). AFP may be raised in gonadal tumors, gastric cancer, and benign states like pregnancy, viral hepatitis, and cirrhosis caused by hepatitis C. The normal range is 10–20 ng/ml. Values above 400 ng/ml or a steady rise in serial estimation (even if lower than 400 ng/ml) is highly suggestive of HCC in a patient at risk of developing HCC. Persistent elevation of AFP is more significant than fluctuating levels. AFP levels are usually normal in the fibrolamellar variety of HCC. AFP is a heterogeneous molecule with respect to the carbohydrate moiety. Different AFP glycoforms can be separated and characterized by their affinity for lectins. Lectins are carbohydrate-binding proteins.

AFP level >500 ng/ml predicts high recurrence rate after transplantation, and such patients are not listed in the USA. Rise of AFP while on the wait list is also a poor prognostic factor. AFP >1000 ng/ml appears to be related to poor prognostic factors like microvascular invasion, portal vein invasion, bile duct invasion, and intrahepatic metastasis. In 2012 a French paper reported a model that added AFP to Milan criteria which improved prediction of recurrence and survival after liver transplantation for HCC.
CA 19-9
CA 19-9 is the abbreviation for carbohydrate antigen or cancer antigen 19-9. This tumor marker belongs to the family of mucinous markers. These have a transmembrane protein skeleton and an extracellular side that has glycosylated oligosaccharides. It is a sialylated Lewis blood group antigen. Mucus glands in the pancreas, biliary tree, salivary glands, stomach, colon, and endometrium physiologically secrete CA 19-9, and this is present in small quantities in serum. Higher levels are observed in inflammatory conditions of the pancreas and biliary tree like acute pancreatitis, biliary obstruction, and cholangitis. Overall mean sensitivity and specificity of serum CA 19-9 for diagnosis of pancreatic cancer are 81% and 90% according to one recent review. This study reported these results using 37 KU/l as cutoff of CA 19-9. Serum CA 19-9 seems to fare very poorly and is unsuitable as a screening modality for pancreatic cancer.
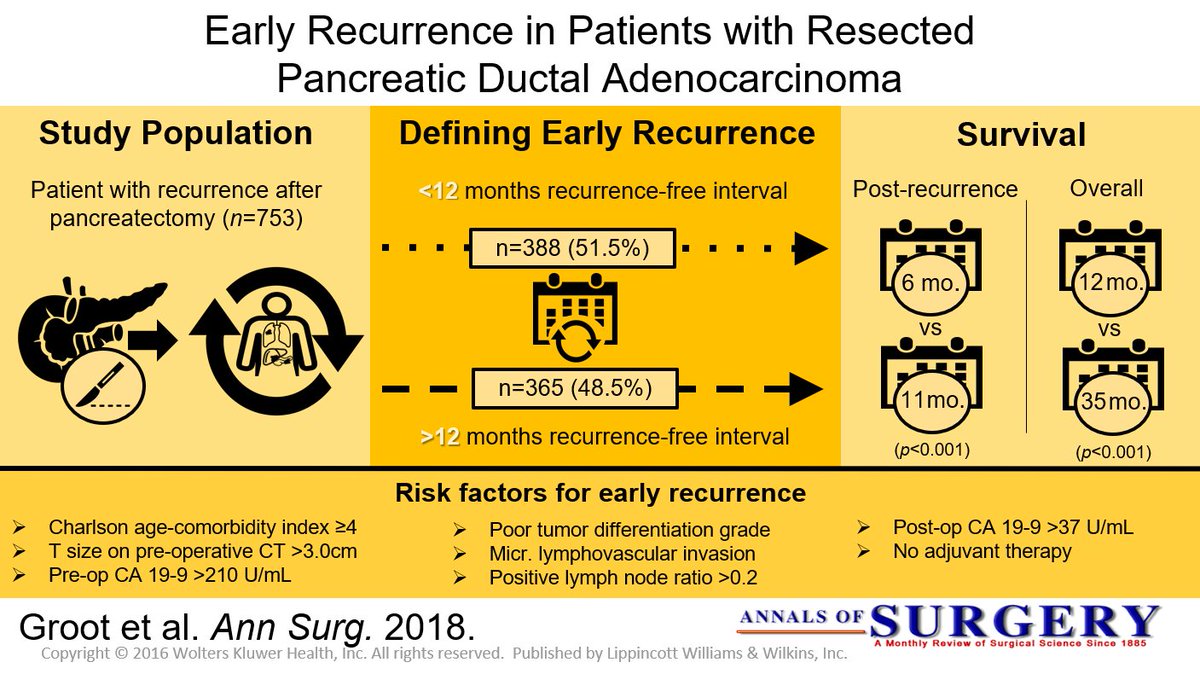
In one of the largest reviews of data, positive predictive value for diagnosis of pancreatic cancer was only 0.9%. Another study from Mumbai used CA 19-9 to predict operability in 49 patients with pancreatic cancer. When CA 19-9 was more than twice the normal (37 U/l), 88% were unresectable. Out of the 29 patients considered resectable after contrast-enhanced CT scan of abdomen, 5 patients were found unresectable at operation due to subcentimeter liver or peritoneal metastasis. All these five patients had CA 19-9 level more than three times the normal limit. These investigators suggest that diagnostic/ staging laparoscopy should be used to avoid a non-therapeutic laparotomy if CA 19-9 is more than thrice the normal limit.
Chromogranin A (CgA)
CgA is an acidic glycoprotein that is ubiquitously present in almost all endocrine and neuroendocrine cells of the human body. They are synthesized in these cells, stored along with other hormones /neurotransmitters in vesicles and released from the cells by exocytosis along with other hormones. The granin family consists of eight different substances of which chromogranin A is the best known and the one in clinical use for several decades now. CgA is thus a universal marker for neuroendocrine cell differentiation and activity. Testing its serum level is a marker of neuroendocrine secretory activity in the body. There are numerous limitations for the use of serum chromogranin A for diagnosis or follow-up of gastroenteropancreatic neuroendocrine tumors (GEP-NETs). However, it still remains the preferred tumor marker in these conditions, as it is widely available and less cumbersome to perform and retains a reasonable sensitivity and specificity provided the clinician applies all necessary recommended precautions in performance of the test and interpretation of the results.

Highest levels of CgA in GEP-NETs are obtained in midgut neuroendocrine tumors, previously termed as “carcinoid tumors.” In ileal carcinoids with liver metastasis, level as high as 200 times upper normal limit is reported. GEP-NETs in MEN-1 syndrome could result in chromogranin A values of about 150 times the upper normal limit. CgA levels in pancreatic NETs are about 60–80 times upper normal limit. CgA is elevated in 100% of gastrinomas and 70% of pancreatic NETs. In gastrinoma, very high levels are reported even in the absence of liver metastasis. CgA level of more than 5000 μg/l was found to be an independent prognostic factor for midgut NETs. Median survival was 33 and 57 months below and above the 5000 μg/l cutoff, respectively. This interpretation of CgA level cannot be generalized to all GEP-NETs. Typical exception of high level without any metastatic disease is gastrinoma as mentioned earlier. CgA level does not correlate with the degree of differentiation of GEP-NETs. Diagnostic accuracy of CgA was 73% in well-differentiated NETs and 50% in poorly differentiated NETs. This is probably related to loss of secretory function of poorly differentiated NETs, where this tumor marker is less reliable. CgA level has been reported to fall after all forms of therapy for GEP-NETs. This could be resection of the tumor, liver transplantation for metastatic disease, radionuclide therapy, or treatment with receptor blockade like everolimus.
Pancreatic Neuroendocrine Tumours

Neuroendocrine tumours (NETs) are neoplasia that can exhibit a range of features such as the production of neuropeptides, the presence of large dense-core secretory vesicles, and the lack of neural structures. NETs can be found in many body regions including the head, neck, lungs, and abdomen. Gastroenteropancreatic (GEP) NETs can be functioning or nonfunctioning, depending on whether hormones are secreted. While the majority of NETs are sporadic, a smaller portion can be related to genetic syndromes such as multiple endocrine neoplasia (MEN), von Hippel-Lindau (VHL), and neurofibromatosis (NF). Compared with their epithelial counterparts, NETs have usually better outcomes. Surgical resections, ranging from enucleation to standard pancreatectomy and lymphadenectomy, play a key role in the management of these lesions, even in advanced disease. Long-term outcomes are correlated with the grading of the disease. Among GEP-NETs, small intestinal NETs (Si-NETs) have a higher incidence than pancreatic neuroendocrine tumours (PanNETs).
SURGICAL MANAGEMENT
Along with incidental diagnosis, tumour size and tumour grading are the most powerful predictors of long-term survival and recurrence. Based on this data, the ENETS guidelines suggested active surveillance rather than surgery for patients with incidental NF-PanNETs that are <2 cm. A recent systematic review demonstrated that surveillance of asymptomatic small NF-PanNETs is safe at least in selected patients although the quality of available studies is still too low to draw firm conclusions. Regardless the size of the primary tumour and the absence of symptoms, a G2 or G3 PanNET/Cs should be treated with resection. Surgery still remains the gold standard in patients with NF-PanNET >2 cm.
The type of resection depends on the location of the lesion. In the presence of head lesions, Whipple’s procedure is the treatment of choice, while distal pancreatectomy and splenectomy is recommended in body-tail lesions. Regardless the type of surgery, a standard lymphadenectomy should be performed. The role of lymphadenectomy during surgical resection for PanNETs is still unclear; however, several authors have shown that the presence of lymph node metastases is associated with poor prognosis; therefore, lymphadenectomy is very helpful in the staging of the disease, but there is no evidence to support an extended lymphadenectomy. The risk of lymph node metastases increases with the increasing size of the primary lesion. Therefore, a standard lymphadenectomy which consists of peripancreatic lymph node dissection along major pancreatic vessels, should always be performed. Recent evidence on the role of conservative management of small PanNETs and the risk of node involvement in PanNETs >2 cm have now significantly limited the role of PSP in NF-PanNETs. These procedures that include enucleation and MP are now limited to patients with small, asymptomatic PanNETs in whom a conservative approach is contraindicated because of young age or for patient’s willingness. Despite a clear benefit in terms of long-term risk of developing pancreatic insufficiency, PSP has a similar morbidity and mortality to standard pancreatic resections.
UPDATE 2020
For non-functioning pancreatic tumors, a surgical procedure is usually recommended. Exception occurs in patients with MEN-1 and who have tumors <2 cm, when the operation is not consensually recommended. For some authors and societies, observation and follow-up should be performed when the tumor is <1 cm, asymptomatic and incidental. The decision for surgical treatment should be made based on the estimated surgical risk, tumor location and comorbidities. The surgical choice may vary between enucleation, distal pancreatectomy and duodenopancreatectomy always associated with regional nodal resection due to the real chances of lymph node metastasis, even in tumors with a size between 1-2 cm. For patients with tumors >2 cm, the choice is tumor cell excision. The location is indicative for the choice of technique, which may range from duodenopancreatectomy to the distal pancreatectomy associated with splenectomy. Both should be accompanied by lymph node resection due to the risk of metastases. Complete resection R0 should always be the primary endpoint. Regardless of tumor size, there is no evidence to support adjuvant systemic therapy for pNET and optimal follow-up of patients undergoing surgical treatment remains unknown.
Surgery for Breast Cancer Liver Metastases

Liver resection offers the only chance of cure in patients with a variety of primary and secondary liver tumors. For breast cancer, the natural history of this condition is poorly defined and the management remains controversial. Most physicians view liver metastases from breast cancer with resignation or attempt palliation with hormones and chemotherapy. Proper patient selection is crucial to ensure favorable long-term results. Although results of hepatic resection for metastatic colorectal cancer have been reported extensively, the experience with liver resection of metastases from breast cancer is limited. In 1991, the first series reporting hepatectomy for breast cancer patients was published.
A large series by Adam et al. reported the experience of 41 French centers regarding liver resection for noncolorectal, nonendocrine liver metastases. Among the 1452 patients who were studied, 454 (32%) were breast cancer patients. Mean age was 52 years (range 27–80 years). Most patients received adjuvant chemotherapy (58%), as few were downstaged by neoadjuvant chemotherapy. Delay between the treatment of the primary breast tumor and metastases was 54 months, with metachronous metastases in more than 90% of cases. There was a single metastasis in 56% of cases and less than three metastases in 84%. Only 8% were nonresectable. Most patients (77% of cases) underwent anatomical major resections (>3 segments). Negative margins were obtained in 82% of cases. Operative mortality was 0.2% during the 2 months following surgery. Fewer than 10% of the patients developed a local or systemic complication. With a median follow-up of 31 months, the overall survival was 41% at 5 years and 22% at 10 years, with a median of 45 months. Five- and 10-year recurrencefree survival rates were 14% and 10%, respectively.
Poor survival was associated with four factors determined by multivariate analysis: time to metastases, extrahepatic location, progression under chemotherapy treatment, and incomplete resection. At the UTMDACC, breast cancer patients who present with isolated synchronous liver metastases are treated initially with systemic chemotherapy. In responders,
hepatic resection is only contemplated if no other disease becomes evident during initial systemic treatment. Most candidates for hepatic resection undergo treatment for metachronous disease and only undergo resection for metastatic disease confined to the liver.
Surgical Technique of Liver Resection for the Treatment of HCC
The incidence of HCC is increasing in the worldwide. Surgery in the form of liver resection or transplantation remains the mainstay of curative treatment for HCC, even though selected patients with small tumours may also be cured with ablation. Liver resection and transplantation are not necessarily two binary choices in most patients and, despite all the debates, are often complementary treatment modalities ideally suited to different patient groups. Thus characterisation of patient and tumour characteristics to guide decision making is vital to achieve the best outcome for patients.
1.Anatomical Resection or Not?
The aim of liver resection in patients with HCC and CLD is that it should be curative with resection of tumour vascular territories and also preserve as much liver volume as possible to prevent postoperative liver failure. EASL guidelines recommend anatomical resection of HCC, whereby the lines of resection match the limits of one or more functional segments of the liver. This is based on evidence suggesting superior oncological outcomes in addition to a reduction in the risk of bleeding and biliary fistula. Although there are no randomised data, a meta-analysis including 2000 patients from 12 non-randomised comparative trials did not show any benefit of anatomical compared with non-anatomical resection in 1-, 3- and 5-year survival, recurrence rate, postoperative morbidity or blood loss . It is practice to perform an anatomical resection for tumours >2 cm, and for smaller tumours in anatomically favourable positions, a wedge with adequate margin is often sufficient. Modifying techniques to maximise parenchymal preservation preserving adequate margins are often the key in these patients.
2. Anterior Approach
The anterior approach, as described by Professor Belghiti , has been advocated for large right-sided tumours. This technique involves transection of the liver parenchyma to the IVC without mobilisation of the liver with the theoretical advantage of less tumour seeding. A prospective randomised controlled trial compared the anterior and conventional approach on 120 patients with large (>5 cm) HCCs. The anterior approach group had less blood transfusion requirements and a significantly longer overall survival (68.1 v 22.6 months; p = 0.006).
3.Parenchymal Transection
As in liver resection for other indications, there is no good evidence to indicate that a single method of parenchymal transection, application of fibrin sealants or intermittent inflow occlusion is beneficial in surgery for HCC. There is also no evidence to suggest that using special equipment for liver resection is of any benefit in decreasing the mortality, morbidity, or blood transfusion requirements. Surgeons should use techniques in which they have been trained and can demonstrate acceptable outcomes.
4. Laparoscopic Approach
Laparoscopic HCC resections are gaining popularity as the approach is more widely adopted across centres. It is important that patients for laparoscopic resection are selected based on the technical capabilities of the surgeon and centre, and the proper mentoring takes place during the learning curve. A summary of published metaanalyses concluded that the laparoscopic approach was associated with improved short-term outcomes (blood loss, complication rates and hospital length of stay) without compromising long-term oncological outcomes. It is worth noting that there are no randomised data; however a number of trials are in progress. Furthermore,their analysis suggested that the incidence of postoperative ascites and liver failure is decreased in the selected group of laparoscopic liver resections . A further metaanalysis of cirrhotic patients up to Child-Pugh B undergoing laparoscopic compared with open liver resection for HCC confirmed these perioperative benefits .
5. Robotic Approach
Although still very much in its infancy, the application of robotic surgery to HCC resection can theoretically yield similar advantages in short-term outcomes to the laparoscopic technique. The only comparative study between robotic and open liver resection for HCC included 183 patients undergoing robotic hepatectomy who were compared using propensity scoring with a cohort of 275 open resections. The robotic group required longer operating time (343 vs 220 min), shorter hospital stays (7.5 vs 10.1 days) and lower dosages of postoperative patient-controlled analgesia (350 vs 554 ng/kg). The 3-year disease-free survival of the robotic group was comparable with that of the open group (72.2% vs 58.0%; p = 0.062), as was the 3-year overall survival (92.6 vs 93.7%; p = 0.431). The associated financial costs of robotic surgery still pose a limitation to its adoption, and it is unclear if this approach is associated with any significant advantages over laparoscopic rather than open resection.
6. Associating Liver Partition with Portal Vein Ligation for Staged
Hepatectomy (ALPPS)/TAE/PVE
ALPPS is still considered an experimental technique in which a first-stage procedure consisting of physical liver splitting and portal vein ligation is followed by a second stage of resection of the HCC and associated liver segments. The advantage seen in colorectal liver metastases is that of rapid hypertrophy for the FLR. There are only limited data describing outcomes of ALPPS for HCC; however an analysis of 35 patients in the international ALPPS registry showed an impressive FLR hypertrophy of 47% following the first stage of the procedure that was associated with a 31% perioperative mortality rate. The majority of these patients were in the intermediate-stage category of the BCLC algorithm. Further evaluation is required prior to routine use of ALPPS for HCC resection, and it is the view of the authors that ALPPS may be a procedure best reserved for carefully selected patients who have bilateral disease.
7. Combined Resection with RFA for Bilobar HCC
For patients with multiple or bilobar HCC in whom resection is contraindicated due to inadequate FLR, combined resection and radiofrequency ablation (RFA) may yield better results than alternative treatments. A single-centre study compared patients with bilobar liver HCCs who underwent resection (n = 89), combination of resection and RFA (n = 114) and TACE (n = 161). The results showed that 1-, 3- and 5-year survival was better in both resection and combined resection, and RFA groups compared with TACE and survival and disease-free survival were comparable between both surgical groups. They concluded that resection combined with RFA provided a chance for cure in patients with bilobar HCC, and provided liver function is preserved, aggressive treatment can improve prognosis.
Anatomia Cirúrgica Pancreática
A anatomia cirúrgica do pâncreas é um dos tópicos mais fascinantes e desafiadores da cirurgia do aparelho digestivo. Conhecer detalhadamente a estrutura e a topografia do pâncreas é crucial para a realização de procedimentos cirúrgicos seguros e eficazes. Neste artigo, vamos explorar os aspectos mais importantes da anatomia pancreática, abordando pontos-chave para estudantes de medicina e residentes de cirurgia do aparelho digestivo.
Estrutura Anatômica do Pâncreas
O pâncreas é uma glândula retroperitoneal situada transversalmente no abdome, na altura das vértebras L1-L2, abrangendo os principais vasos sanguíneos e a coluna vertebral. Ele é composto por cinco partes principais: cabeça, colo, corpo, cauda e processo uncinado.
- Cabeça: Localizada à direita da linha média, cercada pelo duodeno. A cabeça do pâncreas possui uma extensão inferior chamada processo uncinado, que está intimamente relacionada com a veia mesentérica superior e a artéria mesentérica superior.
- Colo: Uma parte estreita entre a cabeça e o corpo, situada anteriormente à veia porta, definida pela localização anatômica anterior à formação da veia porta, geralmente pela confluência das veias mesentérica superior e esplênica.
- Corpo: Estende-se para a esquerda, posterior ao estômago, com a superfície anterior coberta pelo peritônio, formando parte da parede posterior do saco menor.
- Cauda: Parte terminal que se estende até o hilo esplênico, confinada entre as camadas do ligamento esplenorrenal juntamente com a artéria esplênica e a origem da veia esplênica.
- Processo Uncinado: Considerado uma parte distinta do pâncreas devido à sua origem embriológica diferente, estendendo-se posteriormente aos vasos mesentéricos superiores.
Peso e Dimensões Normais
Em um adulto saudável, o pâncreas tem um peso médio de aproximadamente 80 a 120 gramas. As dimensões normais do pâncreas variam, mas geralmente medem cerca de 15 a 20 cm de comprimento, 4 a 5 cm de largura na cabeça, e 1,5 a 2,5 cm de espessura.
Vascularização do Pâncreas
A vascularização do pâncreas é complexa e vital para a compreensão cirúrgica. As principais artérias que irrigam o pâncreas são:
- Artéria Pancreatoduodenal Superior: Ramo da artéria gastroduodenal que irriga a cabeça do pâncreas.
- Artéria Pancreatoduodenal Inferior: Ramo da artéria mesentérica superior que também fornece sangue à cabeça do pâncreas.
- Ramos Pancreáticos da Artéria Esplênica: Irrigam o corpo e a cauda do pâncreas.
As veias pancreáticas drenam para a veia esplênica, veia mesentérica superior e, eventualmente, para a veia porta.
Ductos Pancreáticos
O pâncreas possui dois principais ductos: o ducto pancreático principal (ducto de Wirsung) e o ducto pancreático acessório (ducto de Santorini).
- Ducto Pancreático Principal (Ducto de Wirsung): Começa na cauda do pâncreas e percorre o corpo até a cabeça, onde geralmente se junta ao ducto biliar comum na ampola de Vater, regulada pelo esfíncter de Oddi. O diâmetro normal do ducto pancreático principal varia de 1 mm na cauda até 3 mm na cabeça.
- Ducto Pancreático Acessório (Ducto de Santorini): Corre superior e paralelo ao ducto de Wirsung, drenando parte da cabeça do pâncreas na papila duodenal menor.
O esfíncter de Oddi é uma estrutura única de fibras musculares lisas que regula o fluxo das secreções biliares e pancreáticas para o duodeno e impede o refluxo do conteúdo intestinal para o sistema ductal pancreatobiliar.
Considerações Cirúrgicas
Entender a anatomia pancreática é essencial para evitar complicações durante procedimentos cirúrgicos. Algumas das considerações importantes incluem:
- Ressecção Pancreática: Procedimentos como a pancreatoduodenectomia (procedimento de Whipple) requerem um conhecimento detalhado das relações anatômicas para garantir a remoção eficaz do tumor com a menor morbidade possível.
- Drenagem Biliar: A proximidade do pâncreas com o ducto biliar comum exige precisão ao evitar danos durante as cirurgias.
- Anastomoses Pancreáticas: A criação de anastomoses seguras entre o pâncreas e o intestino é crítica para prevenir complicações pós-operatórias, como fístulas pancreáticas.
Variações Anatômicas
As variações anatômicas do pâncreas e dos ductos pancreáticos são comuns e podem impactar significativamente a abordagem cirúrgica. Uma compreensão detalhada dessas variações é essencial para a personalização do plano cirúrgico. Por exemplo, o pâncreas anular é uma condição em que o tecido pancreático forma um anel ao redor do duodeno, podendo causar estenose duodenal.
Conclusão
A anatomia cirúrgica pancreática é um campo complexo e detalhado que exige estudo e prática contínuos. Compreender as nuances dessa anatomia é fundamental para qualquer cirurgião do aparelho digestivo. Como disse o renomado anatomista Andreas Vesalius: “A anatomia é a fundação de todas as ciências médicas.”
Gostou? Nos deixe um comentário ✍️, ou mande sua dúvida pelo 💬 Chat On-line em nossa DM do Instagram.
Hashtags
#AnatomiaPancreática #CirurgiaDigestiva #EstudantesDeMedicina #ResidentesDeCirurgia #Pancreas

Surgical Management of Retroperitoneal Sarcoma
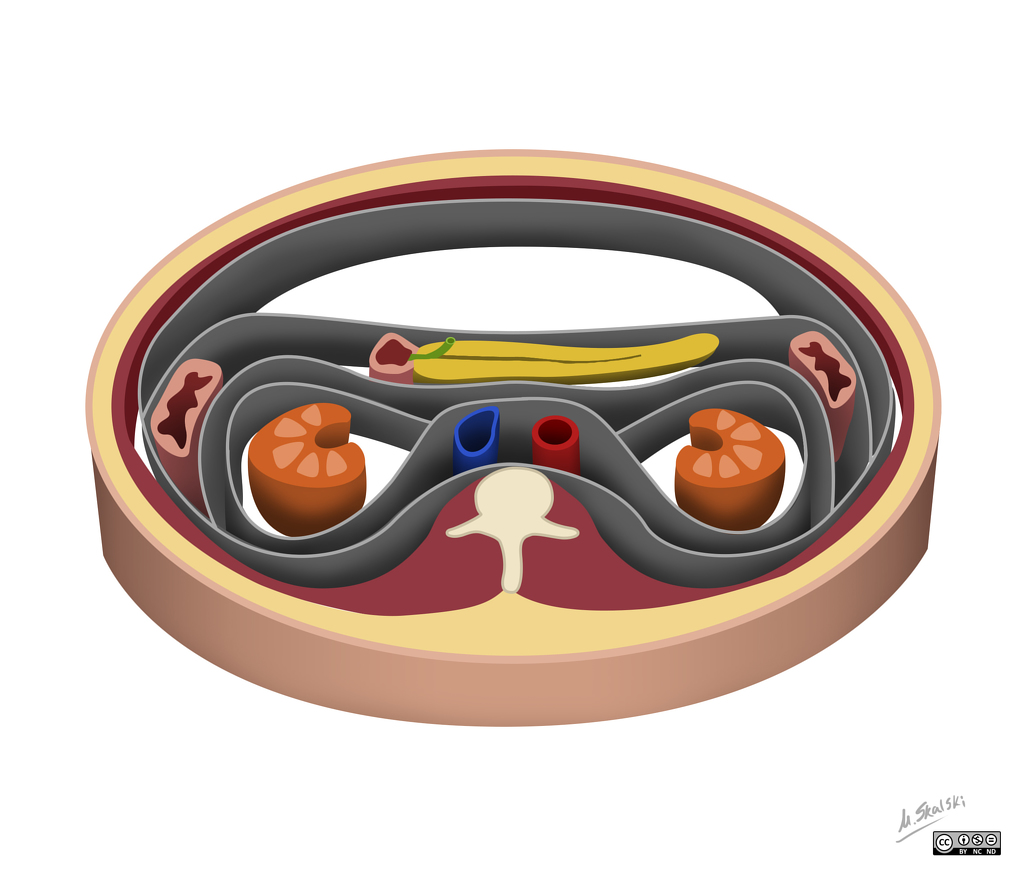
The most critical component of the treatment of Retroperitineal Sarcoma (RPS) remains the surgical excision, and the best chance for cure is at the time of primary surgery. Surgery should achieve a macroscopically complete excision of the tumor (R0 or R1), minimizing marginality, ideally through an en-bloc resection of all potentially involved structures as determined by careful preoperative imaging in combination with intraoperative findings.
Operative planning also includes the functional assessment of critical organs—eg, the function of each kidney. Contraindications to primary resection are believed to be bilateral renal involvement; encasement of the superior mesenteric artery, celiac axis, and porta hepatis; and spinal cord involvement.
When planning for surgery, it is paramount to take into consideration the histology of the RPS as well as its predicted behavior pattern, as these differ widely. Indeed, the largest transatlantic multi-institutional series identified histologic subtype as a predictor of patterns of local and distant recurrence. Moreover, analysis of a large, single-institution database demonstrated that histologic subtype is the strongest predictor of disease-specific death and affects both local and distant recurrence. Of greater interest, the patterns of contiguous organ involvement are also heavily dependent on histologic subtype.
In light of these data, surgeons oncologists should decide the extent of surgical resection in a multidisciplinary setting at a specialized center after review of imaging and pathology, given that the pattern of growth and prognostic risks vary broadly among the different histologic subtypes. For example, liposarcoma is the histologic subtype with the highest recurrence rate. In addition, it is the one with the least clear separation from normal retroperitoneal fat, given that the well-differentiated component of liposarcoma is virtually undistinguishable from normal fat. As a consequence, the extent of surgery should be aimed at removing all ipsilateral retroperitoneal fat en bloc with the mass at the price of sacrificing at least the ipsilateral kidney and colon and part of or the entire psoas muscle.
A staged approach can be followed in virtually all cases. The stages include:
A. Generous laparotomy, exploration, and retraction.
B. Division of the gastrocolic ligament, division of the transverse colon (plus distal ileum if on the right side), and assessment of the duodenum/head of the pancreas if on the right side, or body/tail of the pancreas and spleen if on the left side.
C. Liberation of duodenum/head of the pancreas if on the right side or body/tail of the pancreas and spleen and duodenojejunal junction if on the left side (when possible) and partial duodenal resection or pancreaticoduodenectomy (< 5% of right-sided retroperitoneal sarcomas) if on the right side or distal pancreatectomy and splenectomy if on the left (40%–50% of left-sided retroperitoneal sarcomas), when too adherent/invaded by the tumor.
D. Dissection of the inferior vena cava (IVC) if on the right side or aorta if on the left side, ligating ipsilateral renal vessels and other collaterals and dissection of the iliac vessels.
E. Peritonectomy, resection of the psoas muscle in the pelvis (plus rectal resection if on the left side) after identification and liberation of the femoral nerve (unless directly invaded) and possibly of the femoral cutaneous branch, while the genitofemoralis and ilioinguinal nerves are usually resected, as these lie between the tumor and the psoas fascia.
F. Section of the origin of the psoas major from the spine, sparing the roots of the femoral nerve and possibly the iliohypogastric nerve, liberation/resection of the costodiaphragmatic fold, and removal of the specimen.
Subcapsular liver dissection or partial hepatectomy are rarely needed for tumors located on the right side, whereas a complete liberation of the right liver lobe is usually of help. Similarly, sleeve gastrectomy or proximal gastrectomy is rarely required for tumors located on the left side. Finally, vascular resections (predominantly iliac vessels on either side and IVC on the right side) are required in 4% of cases.
Leiomyosarcoma and other rarer histologic subtypes such as solitary fibrous tumor are much more well-defined tumors. Their border can be clearly separated from retroperitoneal fat/structures. A wide resection is still required but not necessarily involving the adjacent organs if these are not clearly invaded.
Extended surgery may raise concern for added morbidity. A recent multi-institutional collaboration, however, found that a radical resection is safe and is associated with low 30-day mortality (1.8%). Severe complications were associated with increased age, transfusion requirements, and organ resection score, with a more pronounced risk in patients undergoing splenectomy and pancreatectomy and Whipple procedure.
Although major vascular resection (MVR) is associated with higher morbidity, vascular involvement does not preclude resection because it can be safely performed in specialized centers. MVR may be necessary either due to the origin of the RPS, as is the case for leiomyosarcoma of the IVC, or due to local invasion and involvement. Whereas multiple strategies for approaching MVR can be used, a good understanding of the vasculature and collaterals is critical prior to attempting resection and reconstruction, given that IVC resections are well tolerated if a good network of collaterals is present.
In essence, resection of RPS requires technical expertise in multiple sites throughout the abdominal and pelvic cavity, including the handling of large vessels. Single organ/site expertise is not sufficient. The ability to orchestrate a team of complementary surgical experts is critical to successful management of RPS patients. To minimize the risk of intraoperative and perioperative morbidity, RPS resection should be undertaken by surgical teams with expertise in specific aspects of the anatomy of the retroperitoneal space—for example, expertise in retroperitoneal autonomic and somatic nerves, the lymphatic system, paravertebral vessels, and organs of the gastrointestinal tract.
Required expertise also includes experience with additional procedures, such as full-thickness thoracoabdominal wall resection and reconstruction, diaphragmatic resection and reconstruction, major vascular resection and reconstruction, and bone resection. Surgical teams with these abilities, which may accrue from prior participation in multidisciplinary surgical teams, can achieve macroscopically complete tumor resection in the majority of patients.
Surgical management of GASTRIC CANCER
Laparoscopic versus Open gastrectomy
Surgery is the only curative therapy for gastric cancer but most operable gastric cancer presents in a locally advanced stage characterized by tumor infiltration of the serosa or the presence of regional lymph node metastases. Surgery alone is no longer the standard treatment for locally advanced gastric cancer as the prognosis is markedly improved by perioperative chemotherapy. The decisive factor for optimum treatment is the multidisciplinary team specialized in gastric cancer. However, despite multimodal therapy and adequate surgery only 30% of gastric cancer patients are alive at 3 years.
Principles
The same principles that govern open surgery is applied to laparoscopic surgery. To ensure the same effectiveness of laparoscopic gastrectomy (LG) as conventional open gastrectomy, all the basic principles such as properly selected patients, sufficient surgical margins, standardized D2 lymphadenectomy, no-touch technique, etc., should be followed.
Indications
LG may be considered as a safe procedure with better short-term and comparable long-term oncological results compared with open gastrectomy. In addition, there is HRQL advantages to minimal access surgery. There is a general agreement that a laparoscopic approach to the treatment of gastric cancer should be chosen only by surgeons already highly skilled in gastric surgery and other advanced laparoscopic interventions. Furthermore, the first procedures should be carried out during a tutoring program. Diagnostic laparoscopy is strongly recommended as the first step of laparoscopic as well as open gastrectomies. The advantage of early recovery because of reduced surgical trauma would allow earlier commencement of adjuvant chemotherapy and the decreased hospital stay and early return to work may offset the financial costs of laparoscopic surgery.
The first description of LG was given by Kitano, Korea in 1994 and was initially indicated only for early gastric cancer patients with a low-risk lymph node metastasis. As laparoscopic experience has accumulated, the indications for LG have been broadened to patients with advanced gastric cancer. However, the role of LG remains controversial, because studies of the long-term outcomes of LG are insufficient. The Japanese Gastric Cancer Association guidelines in 2004 suggested endoscopic mucosal resection or endoscopic submucosal dissection for stage 1a (cT1N0M0) diagnosis; patients with stage 1b (cT1N1M0) and cT2N0M0) were referred for LG. Totally laparoscopic D2 radical distal gastrectomy using Billroth II anastomosis with laparoscopic linear staplers for early gastric cancer is considered to be safe and feasible. Laparoscopy-assisted total gastrectomy shows better short-term outcomes compared with open total gastrectomy in eligible patients with gastric cancer.
There was a significant reduction of intraoperative blood loss, a reduced risk of postoperative complications, and a shorter hospital stay. Western patients are relatively obese and there is an increased risk of bleeding if lymphadenectomy is performed. LG is technically difficult in the obese than in the normal weight due to reduced visibility, difficulty retracting tissues, dissection plane hindered by adipose tissue, and difficulty with anastomosis. Open gastrectomy is thus preferable for the obese. However, obesity is not a risk factor for survival of patients but it is independently predictive of postoperative complications. Careful approach is being needed, especially for male patients with high body mass index.
Robotic surgery
Robotic surgery will become an additional option in minimally invasive surgery. The importance of performing effective extended lymph node dissection may provide the advantage of using robotic systems. Such developments will improve the quality of life of patients following gastric cancer surgery. A multicenter study with a large number of patients is needed to compare the safety, efficacy, value (efficacy/cost ratio) as well as the long-term outcomes of robotic surgery, traditional laparoscopy, and the open approach.
Classroom: Surgical Management of Gastric Cancer
Principles of Surgical Resection of Hepatocellular Carcinoma
INTRODUCTION
There has been significant improvement in the perioperative results following liver resection, mainly due to techniques that help reduce blood loss during the operation. Extent of liver resection required in HCC for optimal oncologic results is still controversial. On this basis, the rationale for anatomically removing the entire segment or lobe bearing the tumor, would be to remove undetectable tumor metastases along with the primary tumor.
SIZE OF TUMOR VERSUS TUMOR FREE-MARGIN
Several retrospective studies and meta-analyses have shown that anatomical resections are safe in patients with HCC and liver dysfunction, and may offer a survival benefit. It should be noted, that most studies are biased, as non-anatomical resections are more commonly performed in patients with more advanced liver disease, which affects both recurrence and survival. It therefore remains unclear whether anatomical resections have a true long-term survival benefit in patients with HCC. Some authors have suggested that anatomical resections may provide a survival benefit in tumors between 2 and 5 cm. The rational is that smaller tumors rarely involve portal structures, and in larger tumors presence of macrovascular invasion and satellite nodules would offset the effect of aggressive surgical approach. Another important predictor of local recurrence is margin status. Generally, a tumor-free margin of 1 cm is considered necessary for optimal oncologic results. A prospective randomized trial on 169 patients with solitary HCC demonstrated that a resection margin aiming at 2 cm, safely decreased recurrence rate and improved long-term survival, when compared to a resection margin aiming at 1 cm. Therefore, wide resection margins of 2 cm is recommended, provided patient safety is not compromised.
THECNICAL ASPECTS
Intraoperative ultrasound (IOUS) is an extremely important tool when performing liver resections, specifically for patients with HCC and compromised liver function. IOUS allows for localization of the primary tumor, detection of additional tumors, satellite nodules, tumor thrombus, and define relationship with bilio-vascular structures within the liver. Finally, intraoperative US-guided injection of dye, such as methylene-blue, to portal branches can clearly define the margins of the segment supplied by the portal branch and facilitate safe anatomical resection.
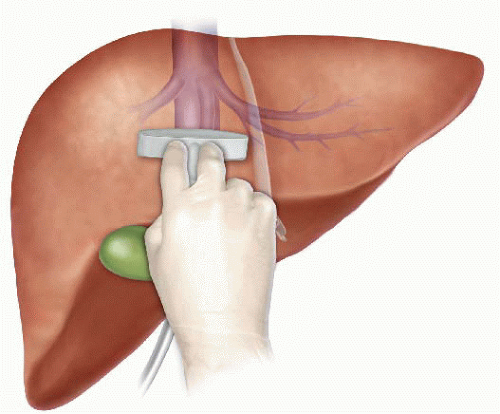
The anterior approach to liver resection is a technique aimed at limiting tumor manipulation to avoid tumoral dissemination, decrease potential for blood loss caused by avulsion of hepatic veins, and decrease ischemia of the remnant liver caused by rotation of the hepatoduodenal ligament. This technique is described for large HCCs located in the right lobe, and was shown in a prospective, randomized trial to reduce frequency of massive bleeding, number of patients requiring blood transfusions, and improve overall survival in this setting. This approach can be challenging, and can be facilitated by the use of the hanging maneuver.

Multiple studies have demonstrated that blood loss and blood transfusion administration are significantly associated with both short-term perioperative, and long-term oncological results in patients undergoing resection for HCC. This has led surgeons to focus on limiting operative blood loss as a major objective in liver resection. Transfusion rates of <20 % are expected in most experienced liver surgery centers. Inflow occlusion, by the use of the Pringle Maneuver represents the most commonly performed method to limit blood loss. Cirrhotic patients can tolerate total clamping time of up to 90 min, and the benefit of reduced blood loss outweighs the risks of inflow occlusion, as long as ischemia periods of 15 min are separated by at least 5 min of reperfusion. Total ischemia time of above 120 min may be associated with postoperative liver dysfunction. Additional techniques aimed at reducing blood loss include total vascular isolation, by occluding the inferior vena cava (IVC) above and below the liver, however, the hemodynamic results of IVC occlusion may be significant, and this technique has a role mainly in tumors that are adjacent to the IVC or hepatic veins.

Anesthesiologists need to assure central venous pressure is low (below 5 mmHg) by limiting fluid administration, and use of diuretics, even at the expense 470 N. Lubezky et al. of low systemic pressure and use of inotropes. After completion of the resection, large amount of crystalloids can be administered to replenish losses during parenchymal dissection.
LAPAROSCOPIC RESECTIONS
Laparoscopic liver resections were shown to provide benefits of reduced surgical trauma, including a reduction in postoperative pain, incision-related morbidity, and shorten hospital stay. Some studies have demonstrated reduced operative bleeding with laparoscopy, attributed to the increased intra-abdominal pressure which reduces bleeding from the low-pressured hepatic veins. Additional potential benefits include a decrease in postoperative ascites and ascites-related wound complications, and fewer postoperative adhesions, which may be important in patients undergoing salvage liver transplantation. There has been a delay with the use of laparoscopy in the setting of liver cirrhosis, due to difficulties with hemostasis in the resection planes, and concerns for possible reduction of portal flow secondary to increased intraabdominal pressure. However, several recent studies have suggested that laparoscopic resection of HCC in patients with cirrhosis is safe and provides improved outcomes when compared to open resections.

Resections of small HCCs in anterior or left lateral segments are most amenable for laparoscopic resections. Larger resections, and resection of posterior-sector tumors are more challenging and should only be performed by very experienced surgeons. Long-term oncological outcomes of laparoscopic resections was shown to be equivalent to open resections on retrospective studies , but prospective studies are needed to confirm these findings. In recent years, robotic-assisted liver resections are being explored. Feasibility and safety of robotic-assisted surgery for HCC has been demonstrated in small non-randomized studies, but more experience is needed, and long-term oncologic results need to be studied, before widespread use of this technique will be recommended.
ALPPS: Associating Liver Partition with Portal vein ligation for Staged hepatectomy
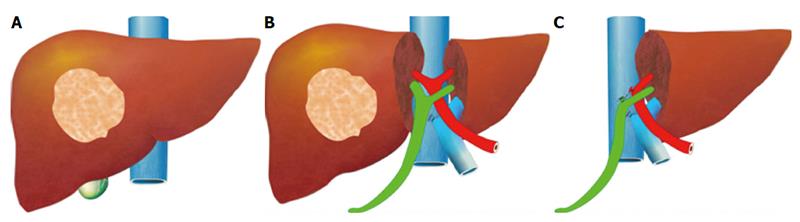
The pre-operative options for inducing atrophy of the resected part and hypertrophy of the FLR, mainly PVE, were described earlier. Associating Liver Partition with Portal vein ligation for Staged hepatectomy (ALPPS) is another surgical option aimed to induce rapid hypertrophy of the FLR in patients with HCC. This technique involves a 2-stage procedure. In the first stage splitting of the liver along the resection plane and ligation of the portal vein is performed, and in the second stage, performed at least 2 weeks following the first stage, completion of the resection is performed. Patient safety is a major concern, and some studies have reported increased morbidity and mortality with the procedure. Few reports exist of this procedure in the setting of liver cirrhosis. Currently, the role of ALPPS in the setting of HCC and liver dysfunction needs to be better delineated before more widespread use is recommended.
Pringle Maneuver
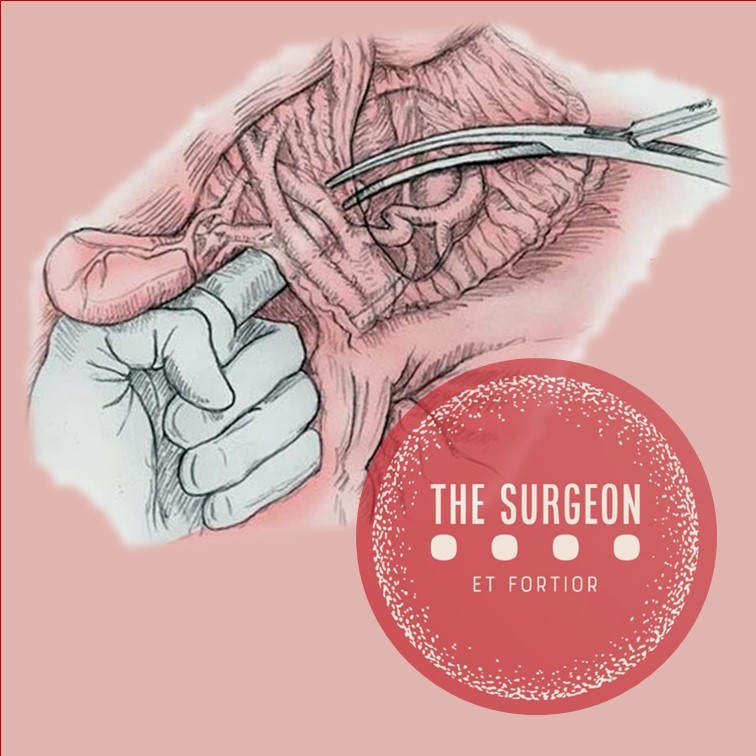
After the first major hepatic resection, a left hepatic resection, carried out in 1888 by Carl Langenbuch, it took another 20 years before the first right hepatectomy was described by Walter Wendel in 1911. Three years before, in 1908, Hogarth Pringle provided the first description of a technique of vascular control, the portal triad clamping, nowadays known as the Pringle maneuver. Liver surgery has progressed rapidly since then. Modern surgical concepts and techniques, together with advances in anesthesiological care, intensive care medicine, perioperative imaging, and interventional radiology, together with multimodal oncological concepts, have resulted in fundamental changes. Perioperative outcome has improved significantly, and even major hepatic resections can be performed with morbidity and mortality rates of less than 45% and 4% respectively in highvolume liver surgery centers. Many liver surgeries performed routinely in specialized centers today were considered to be high-risk or nonresectable by most surgeons less than 1–2 decades ago.Interestingly, operative blood loss remains the most important predictor of postoperative morbidity and mortality, and therefore vascular control remains one of the most important aspects in liver surgery.
“Bleeding control is achieved by vascular control and optimized and careful parenchymal transection during liver surgery, and these two concepts are cross-linked.”
First described by Pringle in 1908, it has proven effective in decreasing haemorrhage during the resection of the liver tissue. It is frequently used, and it consists in temporarily occluding the hepatic artery and the portal vein, thus limiting the flow of blood into the liver, although this also results in an increased venous pressure in the mesenteric territory. Hemodynamic repercussion during the PM is rare because it only diminishes the venous return in 15% of cases. The cardiovascular system slightly increases the systemic vascular resistance as a compensatory response, thereby limiting the drop in the arterial pressure. Through the administration of crystalloids, it is possible to maintain hemodynamic stability.

In the 1990s, the PM was used continuously for 45 min and even up to an hour because the depth of the potential damage that could occur due to hepatic ischemia was not yet known. During the PM, the lack of oxygen affects all liver cells, especially Kupffer cells which represent the largest fixed macrophage mass. When these cells are deprived of oxygen, they are an endless source of production of the tumour necrosis factor (TNF) and interleukins 1, 6, 8 and 10. IL 6 has been described as the cytokine that best correlates to postoperative complications. In order to mitigate the effects of continuous PM, intermittent clamping of the portal pedicle has been developed. This consists of occluding the pedicle for 15 min, removing the clamps for 5 min, and then starting the manoeuvre again. This intermittent passage of the hepatic tissue through ischemia and reperfusion shows the development of hepatic tolerance to the lack of oxygen with decreased cell damage. Greater ischemic tolerance to this intermittent manoeuvre increases the total time it can be used.
Management of gallbladder cancer

Gallbladder cancer is uncommon disease, although it is not rare. Indeed, gallbladder cancer is the fifth most common gastrointestinal cancer and the most common biliary tract cancer in the United States. The incidence is 1.2 per 100,000 persons per year. It has historically been considered as an incu-rable malignancy with a dismal prognosis due to its propensity for early in-vasion to liver and dissemination to lymph nodes and peritoneal surfaces. Patients with gallbladder cancer usually present in one of three ways: (1) advanced unresectable cancer; (2) detection of suspicious lesion preoperatively and resectable after staging work-up; (3) incidental finding of cancer during or after cholecystectomy for benign disease.
SURGICAL MANAGEMENT
Although, many studies have suggested improved survival in patients with early gallbladder cancer with radical surgery including en bloc resection of gallbladder fossa and regional lymphadenectomy, its role for those with advanced gallbladder cancer remains controversial. First, patients with more advanced disease often require more extensive resections than early stage tumors, and operative morbidity and mortality rates are higher. Second, the long-term outcomes after resection, in general, tend to be poorer; long-term survival after radical surgery has been reported only for patients with limited local and lymph node spread. Therefore, the indication of radical surgery should be limited to well-selected patients based on thorough preoperative and intra-operative staging and the extent of surgery should be determined based on the area of tumor involvement.
Surgical resection is warranted only for those who with locoregional disease without distant spread. Because of the limited sensitivity of current imaging modalities to detect metastatic lesions of gallbladder cancer, staging laparoscopy prior to proceeding to laparotomy is very useful to assess the
abdomen for evidence of discontinuous liver disease or peritoneal metastasis and to avoid unnecessary laparotomy. Weber et al. reported that 48% of patients with potentially resectable gallbladder cancer on preoperative imaging work-up were spared laparotomy by discovering unresectable disease by laparoscopy. Laparoscopic cholecystectomy should be avoided when a preoperative cancer is suspected because of the risk of violation of the plane between tumor and liver and the risk of port site seeding.
The goal of resection should always be complete extirpation with microscopic negative margins. Tumors beyond T2 are not cured by simple cholecystectomy and as with most of early gallbladder cancer, hepatic resection is always required. The extent of liver resection required depends upon whether involvement of major hepatic vessels, varies from segmental resection of segments IVb and V, at minimum to formal right hemihepatectomy or even right trisectionectomy. The right portal pedicle is at particular risk for advanced tumor located at the neck of gallbladder, and when such involvement is suspected, right hepatectomy is required. Bile duct resection and reconstruction is also required if tumor involved in bile duct. However, bile duct resection is associated with increased perioperative morbidity and it should be performed only if it is necessary to clear tumor; bile duct resection does not necessarily increase the lymph node yield.
Hepatic Surgery: Portal Vein Embolization

INTRODUCTION
Portal vein Embolizations (PVE) is commonly used in the patients requiring extensive liver resection but have insufficient Future Liver Remanescent (FLR) volume on preoperative testing. The procedure involves occluding portal venous flow to the side of the liver with the lesion thereby redirecting portal flow to the contralateral side, in an attempt to cause hypertrophy and increase the volume of the FLR prior to hepatectomy.
PVE was first described by Kinoshita and later reported by Makuuchi as a technique to facilitate hepatic resection of hilar cholangiocarcinoma. The technique is now widely used by surgeons all over the world to optimize FLR volume before major liver resections.
PHYSIOPATHOLOGY
PVE works because the extrahepatic factors that induce liver hypertrophy are carried primarily by the portal vein and not the hepatic artery. The increase in FLR size seen after PVE is due to both clonal expansion and cellular hypertrophy, and the extent of post-embolization liver growth is generally proportional to the degree of portal flow diversion. The mechanism of liver regeneration after PVE is a complex phenomenon and is not fully understood. Although the exact trigger of liver regeneration remains unknown, several studies have identified periportal inflammation in the embolized liver as an important predictor of liver regeneration.

THECNICAL ASPECTS
PVE is technically feasible in 99% of the patients with low risk of complications. Studies have shown the FLR to increase by a median of 40–62% after a median of 34–37 days after PVE, and 72.2–80% of the patients are able to undergo resection as planned. It is generally indicated for patients being considered for right or extended right hepatectomy in the setting of a relatively small FLR. It is rarely required before extended left hepatectomy or left trisectionectomy, since the right posterior section (segments 6 and 7) comprises about 30% of total liver volume.
PVE is usually performed through percutaneous transhepatic access to the portal venous system, but there is considerable variability in technique between centers. The access route can be ipsilateral (portal access at the same side being resected) with retrograde embolization or contralateral (portal access through FLR) with antegrade embolization. The type of approach selected depends on a number of factors including operator preference, anatomic variability, type of resection planned, extent of embolization, and type of embolic agent used. Many authors prefer ipsilateral approach especially for right-sided tumors as this technique allows easy catheterization of segment 4 branches when they must be embolized and also minimizes the theoretic risk of injuring the FLR vasculature or bile ducts through a contralateral approach and potentially making a patient ineligible for surgery.
However, majority of the studies on contralateral PVE show it to be a safe technique with low complication rate. Di Stefano et al. reported a large series of contralateral PVE in 188 patients and described 12 complications (6.4%) only 6 of which could be related to access route and none precluded liver resection. Site of portal vein access can also change depending on the choice of embolic material selected which can include glue, Gelfoam, n-butyl-cyanoacrylate (NBC), different types and sizes of beads, alcohol, and nitinol plus. All agents have similar efficacy and there are no official recommendations for a particular type of agent.
RESULTS
Proponents of PVE believe that there should be very little or no tumor progression during the 4–6 week wait period for regeneration after PVE. Rapid growth of the FLR can be expected within the first 3–4 weeks after PVE and can continue till 6–8 weeks. Results from multiple studies suggest that 8–30% hypertrophy over 2–6 weeks can be expected with slower rates in cirrhotic patients. Most studies comparing outcomes after major hepatectomy with and without preoperative PVE report superior outcomes with PVE. Farges et al. demonstrated significantly less risk of postoperative complications, duration of intensive care unit, and hospital stay in patients with cirrhosis who underwent right hepatectomy after PVE compared to those who did not have preoperative PVE. The authors also reported no benefit of PVE in patients with a normal liver and FLR >30%. Abulkhir et al. reported results from a meta-analysis of 1088 patients undergoing PVE and showed a markedly lower incidence of Post Hepatectomy Liver Failure (PHLF) and death compared to series reporting outcomes after major hepatectomy in patients who did not undergo PVE. All patients had FLR volume increase, and 85% went on to have liver resection after PVE with a PHLF incidence of 2.5% and a surgical mortality of 0.8%. Several studies looking at the effect of systemic neoadjuvant chemotherapy on the degree of hypertrophy after PVE show no significant impact on liver regeneration and growth.
VOLUMETRIC RESPONSE

The volumetric response to PVE is also a very important factor in understanding the regenerative capacity of a patient’s liver and when used together with FLR volume can help identify patients at risk of poor postsurgical outcome. Ribero et al. demonstrated that the risk of PHLF was significantly higher not only in patients with FLR ≤ 20% but also in patients with normal liver who demonstrated ≤5% of FLR hypertrophy after PVE. The authors concluded that the degree of hypertrophy >10% in patients with severe underlying liver disease and >5% in patients with normal liver predicts a low risk of PHLF and post-resection mortality. Many authors do not routinely offer resection to patients with borderline FLR who demonstrate ≤5% hypertrophy after PVE.
Predicting LIVER REMNANT Function
Careful analysis of outcome based on liver remnant volume stratified by underlying liver disease has led to recommendations regarding the safe limits of resection. The liver remnant to be left after resection is termed the future liver remnant (FLR). For patients with normal underlying liver, complications, extended hospital stay, admission to the intensive care unit, and hepatic insufficiency are rare when the standardized FLR is >20% of the TLV. For patients with tumor-related cholestasis or marked underlying liver disease, a 40% liver remnant is necessary to avoid cholestasis, fluid retention, and liver failure. Among patients who have been treated with preoperative systemic chemotherapy for more than 12 weeks, FLR >30% reduces the rate of postoperative liver insufficiency and subsequent mortality.
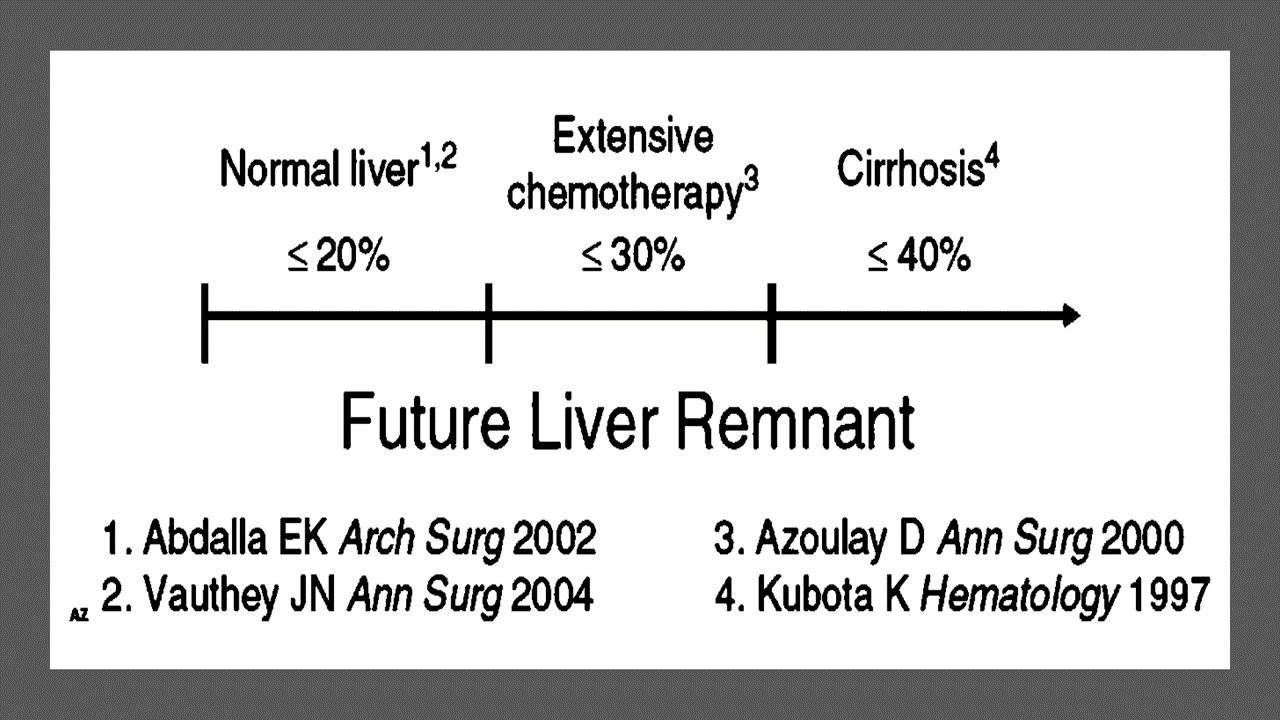
When the liver remnant is normal or has only mild disease, the volume of liver remnant can be measured directly and accurately with threedimensional computed tomography (CT) volumetry. However, inaccuracy may arise because the liver to be resected is often diseased, particularly in patients with cirrhosis or biliary obstruction. When multiple or large tumors occupy a large volume of the liver to be resected, subtracting tumor volumes from liver volume further decreases accuracy of CT volumetry. The calculated TLV, which has been derived from the association between body surface area (BSA) and liver size, provides a standard estimate of the TLV. The following formula is used:
TLV (cm3) = –794.41 + 1267.28 × BSA (square meters)
Thus, the standardized FLR (sFLR) volume calculation uses the measured FLR volume from CT volumetry as the numerator and the calculated TLV as the denominator: Standardized FLR (sFLR) = measured FLR volume/TLV Calculating the standardized TLV corrects the actual liver volume to the individual patient’s size and provides an individualized estimate of that patient’s postresection liver function. In the event of an inadequate FLR prior to major hepatectomy, preoperative liver preparation may include portal vein embolization (PVE).
Classroom: Principles of Hepatic Surgery
Videos of Surgical Procedures

This page provides links to prerecorded webcasts of surgical procedures. These are actual operations performed at medical centers in the Brazil. Please note that you cannot send in questions by email, though the webcast may say that you can, because you are not seeing these videos live. The videos open in a second window. If you have a pop-up blocker, you will need to disable it to view the programs.
Videos of Surgical Procedures
Surgical Management of Cholangiocarcinoma
Cholangiocarcinoma (CCA) is a rare but lethal cancer arising from the bile duct epithelium. As a whole, CCA accounts for approximately 3 % of all gastrointestinal cancers. It is an aggressive disease with a high mortality rate. Unfortunately, a significant proportion of patients with CCA present with either unresectable or metastatic disease. In a retrospective review of 225 patients with hilar cholangiocarcinoma, Jarnagin et al. reported that 29 % of patients had either unresectable disease were unfit for surgery. Curative resection offers the best chance for longterm survival. Whereas palliation with surgical bypass was once the preferred surgical procedure even for resectable disease, aggressive surgical resection is now the standard.
Classroom: Surgical Management of Cholangiocarcinoma
Abdominal Surgical Anatomy
The abdomen is the lower part of the trunk below the diaphragm. Its walls surround a large cavity called the abdominal cavity. The abdominal cavity is much more extensive than what it appears from the outside. It extends upward deep to the costal margin up to the diaphragm and downward within the bony pelvis. Thus, a considerable part of the abdominal cavity is overlapped by the lower part of the thoracic cage above and by the bony pelvis below. The abdominal cavity is subdivided by the plane of the pelvic inlet into a larger upper part, i.e., the abdominal cavity proper, and a smaller lower part, i.e., the pelvic cavity. Clinically the importance of the abdomen is manifold. To the physician, the physical examination of the patient is never complete until he/she thoroughly examines the abdomen. To the surgeon, the abdomen remains an enigma because in number of cases the cause of abdominal pain and nature of abdominal lump remains inconclusive even after all possible investigations. To summarize, many branches of medicine such as general surgery and gastroenterology are all confined to the abdomen.
Classroom: Abdominal Surgical Anatomy
IPMN Surgical Management

INTRODUCTION
IPMNs were first recognized in 1982 by Ohashi, but the term IPMN was not officially used until 1993. IPMNs are defined in the WHO Classification of Tumors of the Digestive System as an intraductal, grossly visible epithelial neoplasm of mucin-producing cells. Using imaging and histology, IPMNs can be classified into three types based on duct involvement:
1. Main-duct IPMN (approximately 25% of IPMNs): Segmental or diffuse dilation of the main pancreatic duct (>5 mm) in the absence of other causes of ductal obstruction.
2. Branch-duct IPMN (approximately 57% of IPMNs): Pancreatic cysts (>5 mm) that communicate with the main pancreatic duct.
3. Mixed type IPMN (approximately 18% of IPMNs): Meets criteria for both main and branch duct.
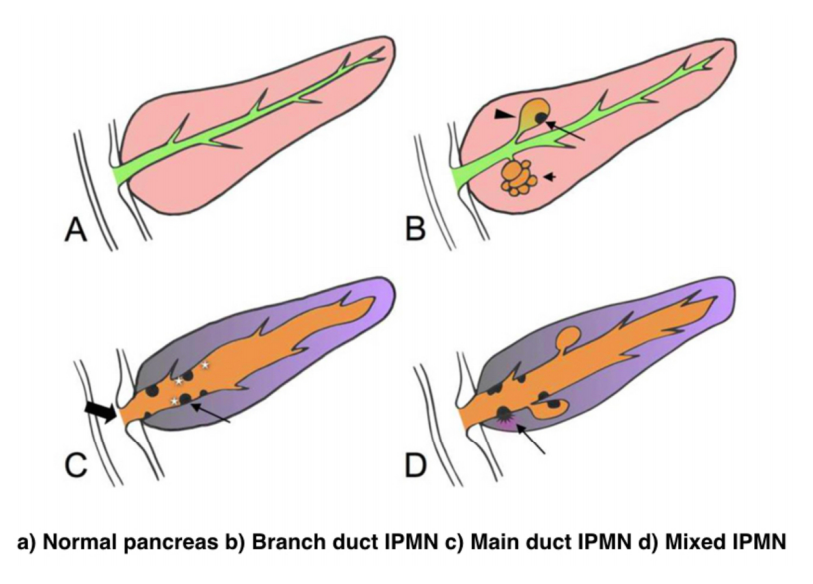
Due to the asymptomatic nature of the disease, the overall incidence of IPMNs is difficult to define but is thought to account for approximately 3% to 5% of all pancreatic tumors. Most IPMNs are discovered as incidental lesions from the workup of an unrelated process by imaging or endoscopy. IPMNs are slightly more prevalent in males than in females, with a peak incidence of 60 to 70 years of age. Branch-duct IPMNs tend to occur in a slightly younger population and are less associated with malignancy compared with main-duct or mixed variants.
Because a majority of IPMNs are discovered incidentally, most are asymptomatic. When symptoms do occur, they tend to be nonspecific and include unexplained weight loss, anorexia, abdominal pain, and back pain. Jaundice can occur with mucin obstructing the ampulla or with an underlying invasive carcinoma. The obstruction of the pancreatic duct can also lead to pancreatitis. IPMNs may represent genomic instability of the entire pancreas. This concept, known as a “field defect,” has been described as a theoretical risk of developing a recurrent IPMN or pancreatic adenocarcinoma at a site remote from the original IPMN. The three different types of IPMNs, main duct, branch duct, and mixed duct, dictate different treatment algorithms.
MAIN DUCT IPMNs
Main-duct IPMNs should be resected in all patients unless the risks of existing comorbidities outweigh the benefits of resection. The goal of operative management of IPMNs is to remove all adenomatous or potentially malignant epithelium to minimize recurrence in the pancreas remnant. There are two theories on the pathophysiologic basis of IPMNs. The first groups IPMNs into a similar category as an adenocarcinoma, a localized process involving only a particular segment of the pancreas. The thought is that removal of the IPMN is the only treatment necessary. In contrast, some believe IPMNs to represent a field defect of the pancreas. All of the ductal epithelium remains at risk of malignant degeneration despite removal of the cyst. Ideally, a total pancreatectomy would eliminate all risk, but this is a radical procedure that is associated with metabolic derangements and exocrine insufficiency. Total pancreatectomy should be limited to the most fit patients, with a thorough preoperative assessment and proper risk stratification prior to undertaking this surgery.
There is less uncertainty with treatment of main-duct IPMNs. The high incidence of underlying malignancy associated with the IPMNs warrants surgical resection. IPMNs localized to the body and tail (approximately 33%) can undergo a distal pancreatectomy with splenectomy. At the time of surgery, a frozen section of the proximal margin should be interpreted by a pathologist to rule out high-grade dysplasia. A prospective study identified a concordance rate of 94% between frozen section and final pathologic examination. If the margin is positive (high-grade dysplasia, invasion) additional margins may be resected from the pancreas until no evidence of disease is present. However, most surgeons will proceed to a total pancreatectomy after two subsequent margins demonstrate malignant changes. This more extensive procedure should be discussed with the patient prior to surgery, and the patient should be properly consented regarding the risks of a total pancreatectomy.
IPMNs localized to the head or uncinate process of the pancreas should undergo a pancreaticoduodenectomy. A frozen section of the distal margin should be analyzed by pathology for evidence of disease. As mentioned before, after two additional margins reveal malignant changes, a total pancreatectomy is usually indicated (approximately 5%). The absence of abnormal changes in frozen sections does not equate to negative disease throughout the pancreas remnant. Rather, skip lesions involving the remainder of the pancreas can exist and thus patients ultimately still require imaging surveillance after successful resection. A prophylactic total pancreatectomy is rarely performed because the subsequent pancreatic endocrine (diabetes mellitus) and exocrine deficits (malnutrition) carry an increased morbidity.
BRANCH DUCT IPMNs
Localized branch-duct IPMN can be treated with a formal anatomic pancreatectomy, pancreaticoduodenectomy, or distal pancreatectomy, depending on the location of the lesion. However, guidelines were established that allow for nonoperative management with certain branch- type IPMN characteristics.
These include asymptomatic patients with a cyst size less than 3 cm and lack of mural nodules. The data to support this demonstrate a very low incidence of malignancy (approximately 2%) in this patient group. Which nearly matches the anticipated mortality of undergoing a formal anatomic resection. In approximately 20% to 30% of patients with branch- duct IPMNs, there is evidence of multifocality. The additional IPMNs can be visualized on high-resolution CT or MRI imaging. Ideally, patients with multifocal branch-duct IPMNs should undergo a total pancreatectomy. However, as previously mentioned, the increased morbidity and lifestyle alterations associated with a total pancreatectomy allows for a more conservative approach. This would include removing the most suspicious or dominant of the lesions in an anatomic resection and follow-up imaging surveillance of the remaining pancreas remnant. If subsequent imaging demonstrates malignant charac- teristics, a completion pancreatectomy is usually indicated.
RECURRENCE RATES
Recurrence rates with IPMNs are variable. An anatomic resection of a branch-duct IPMN with negative margins has been shown to be curative. The recurrence of a main- duct IPMN in the remnant gland is anywhere from 0% to 10% if the margins are negative and there is no evidence of invasion. Most case series cite a 5-year survival rate of at least 70% after resection of noninvasive IPMNs. In contrast, evidence of invasive disease, despite negative margins, decreases 5-year survival to 30% to 50%. The recurrence rate in either the pancreatic remnant or distant sites approaches 50% to 90% in these patients. Histopathologic subtype of the IPMN is correlated with survival. The aggressive tubular subtype has a 5-year survival ranging from 37% to 55% following surgical resection, whereas the colloid subtype has 5-year survival ranging from 61% to 87% post resection. Factors associated with decreased survival include tubular subtype, lymph node metastases, vascular invasion, and positive margins. IPMNs with evidence of invasion should be treated similar to pancreatic adenocarcinomas. Studies show that IPMNs tend to have better survival than pancreatic adenocarcinoma. This survival benefit may be secondary to the less aggressive tumor biology or the earlier diagnosis of IPMNs.
SURVEILLANCE
All patients who have a resected IPMN should undergo imaging surveillance. There is continual survival benefit with further resection if an IPMN does recur. International Consensus Guidelines published in 2017 offer recom- mendations for the frequency and modality of imaging surveillance after resection. Routine serum measurement of CEA and CA 19-9 has a limited role for detection of an IPMN recurrence. Of note, a new pancreatic lesion discovered on imaging after resection could represent a postoperative pseudocyst, a recurrence of the IPMN from inadequate resection, a new IPMN, or an unrelated new neoplastic process. IPMNs may also be associated with extrapancreatic neoplasms (stomach, colon, rectum, lung, breast) and pancreatic ductal adenocarcinoma. It is unclear if this represents a true genetic syndrome. However, patients with IPMNs should have a discussion about the implications of their disease with their physician and are encouraged to undergo colonoscopy to exclude a synchronous neoplastic process.
The incidence of PANCREATIC CYSTIC LESIONS will continue to increase as imaging technology improves. EUS, cytology, and molecular panels have made differentiating the type of PCN less problematic. The importance of an accurate preoperative diagnosis ensures that operative management is selectively offered to those with high-risk lesions. Management beyond surgery, including adjuvant therapy and surveillance, continue to be active areas of research.
Perioperative Medicine

Surgery and anesthesia profoundly alter the normal physiologic and metabolic states. Estimating the patient’s ability to respond to these stresses in the postoperative period is the task of the preoperative evaluation. Perioperative complications are often the result of failure, in the preoperative period, to identify underlying medical conditions, maximize the patient’s preoperative health, or accurately assess perioperative risk. Sophisticated laboratory studies and specialized testing are no substitute for a thoughtful and careful history and physical examination. Sophisticated technology has merit primarily in confirming clinical suspicion.
Classroom: Perioperative Medicine
Hepatocellular Carcinoma: Resection Versus Transplantation

Hepatocellular carcinoma is the second most common cause of cancer mortality worldwide and its incidence is rising in North America, with an estimated 35,000 cases in the U.S. in 2014. The best chance for cure is surgical resection in the form of either segmental removal or whole organ transplantation although recent survival data on radiofrequency ablation approximates surgical resection and could be placed under the new moniker of “thermal resection”. The debate between surgical resection and transplantation focuses on patients with “within Milan criteria” tumors, single tumors, and well compensated cirrhosis who can safely undergo either procedure. Although transplantation historically has had better survival outcomes, early diagnosis, reversal of liver disease, and innovations in patient selection and neo-adjuvant therapies have led to similar 5-year survival. Transplantation clearly has less risk of tumor recurrence but exposes recipients to long term immunosuppression and its side effects. Liver transplantation is also limited by the severe global limit on the supply of organ donors whereas resection is readily available. The current data does not favor one treatment over the other for patients with minimal or no portal hypertension and normal synthetic function. Instead, the decision to resect or transplant for HCC relies on multiple factors including tumor characteristics, biology, geography, co-morbidities, location, organ availability, social support and practice preference.
Resection Versus Transplantation
The debate between resection and transplantation revolves around patients who have well compensated cirrhosis with Milan criteria resectable tumors. Patients within these criteria represent a very small proportion of those who initially present with HCC. This is especially true in western countries where hepatitis C is the most common cause of liver failure and HCC is a result of the progressive and in most cases advanced cirrhosis.
Given the need for a large number of patients to show statistical significance, it would be difficult to perform a high-quality prospective randomized controlled trial comparing resection and transplantation. In fact the literature revealed that no randomized controlled trials addressing this issue exist. Instead, outcomes of surgical treatment for HCC stem from retrospective analyses that have inherent detection, selection and attrition biases.
Given the numerous articles available on this subject, several meta-analyses have been published to delineate the role of transplantation and resection for treatment of HCC. However, there is reason to be wary of these meta-analyses because they pool data from heterogeneous populations with variable selection criteria and treatment protocols. One such meta-analysis by Dhir et al. focused their choice of articles to strict criteria which excluded studies with non-cirrhotic patients, fibrolamellar HCC and hepato-cholangiocarcinomas but included those with HCC within Milan criteria and computation of 5-year survival; between 1990 and 2011 they identified ten articles that fit within these criteria, of which six were ITT analyses, six included only well-compensated cirrhotics (Child-Pugh Class A without liver dysfunction) and three were ITT analyses of well-compensated cirrhotics.
Analysis of the six ITT studies that included all cirrhotics (n = 1118) (Child-Pugh Class A through C) showed no significant difference in survival at 5 years (OR = 0.600, 95 % CI 0.291– 1.237 l; p=0.166) but ITT analysis of only well-compensated cirrhotics (Child- Pugh Class A) revealed that patients undergoing transplant had a significantly higher 5-year survival as compared to those with resection (OR=0.521, 95 % CI 0.298–0.911; p=0.022).
A more recent ITT retrospective analysis from Spain assessed long-term survival and tumor recurrence following resection or transplant for tumors <5 cm in 217 cirrhotics (Child-Pugh Class A, B and C) over the span of 16 years. Recurrence at 5 years was significantly higher in the resection group (71.6 % vs. 16 % p<0.001) but survival at 4 years was similar (60 % vs. 62 %) which is likely explained by the evolving role of adjuvant therapies to treat post-resection recurrence.
Conclusions
- Patients with anatomically resectable single tumors and no cirrhosis or Child-Pugh Class A cirrhosis with normal bilirubin, HVPG (<10 mmHg), albumin and INR can be offered resection (evidence quality moderate; strong recommendation).
- Patients with Milan criteria tumors in the setting of Child- Pugh Class A with low platelets and either low albumin or high bilirubin or Child-Pugh Class B and C cirrhosis, especially those with more than one tumor, should be offered liver transplantation over resection (evidence quality moderate; strong recommendation).
- Those with Milan criteria tumors and Child-Pugh Class A cirrhosis without liver dysfunction should be considered for transplantation over resection (evidence quality low; weak recommendation).
- No recommendation can be made in regard to transplanting tumors beyond Milan criteria (evidence quality low) except to follow regional review board criteria.
- Pre-transplant therapies such as embolic or thermal ablation are safe and by expert opinion considered to be effective in decreasing transplant waitlist dropout and bridging patients to transplant (evidence quality low, weak recommendation). These interventions should be considered for those waiting longer than 6 months (evi- dence quality low, moderate recommendation).
- Living donor liver transplantation is a safe and effective option for treatment of HCC that are within and exceed Milan criteria (evidence quality moderate, weak recommendation).

POST-HEPATECTOMY ADVERSE EVENTS

Hepatectomia Esquerda – Metástase CR
Hepatic resection had an impressive growth over time. It has been widely performed for the treatment of various liver diseases, such as malignant tumors, benign tumors, calculi in the intrahepatic ducts, hydatid disease, and abscesses. Management of hepatic resection is challenging. Despite technical advances and high experience of liver resection of specialized centers, it is still burdened by relatively high rates of postoperative morbidity and mortality. Especially, complex resections are being increasingly performed in high risk and older patient population. Operation on the liver is especially challenging because of its unique anatomic architecture and because of its vital functions. Common post-hepatectomy complications include venous catheter-related infection, pleural effusion, incisional infection, pulmonary atelectasis or infection, ascites, subphrenic infection, urinary tract infection, intraperitoneal hemorrhage, gastrointestinal tract bleeding, biliary tract hemorrhage, coagulation disorders, bile leakage, and liver failure. These problems are closely related to surgical manipulations, anesthesia, preoperative evaluation and preparation, and postoperative observation and management. The safety profile of hepatectomy probably can be improved if the surgeons and medical staff involved have comprehensive knowledge of the expected complications and expertise in their management.
Classroom: Hepatic Resections
The era of hepatic surgery began with a left lateral hepatic lobectomy performed successfully by Langenbuch in Germany in 1887. Since then, hepatectomy has been widely performed for the treatment of various liver diseases, such as malignant tumors, benign tumors, calculi in the intrahepatic ducts, hydatid disease, and abscesses. Operation on the liver is especially challenging because of its unique anatomic architecture and because of its vital functions. Despite technical advances and high experience of liver resection of specialized centers, it is still burdened by relatively high rates of postoperative morbidity (4.09%-47.7%) and mortality (0.24%-9.7%). This review article focuses on the major postoperative issues after hepatic resection and presents the current management.
REVIEW_ARTICLE_HEPATECTOMY_COMPLICATIONS
Review of POSTGASTRECTOMY SYNDROMES

The first postgastrectomy syndrome was noted not long after the first gastrectomy was performed: Billroth reported a case of epigastric pain associated with bilious vomiting as a sequel of gastric surgery in 1885. Several classic treatises exist on the subject; we cannot improve on them and merely provide a few references for the interested reader. Surgical procedures on the stomach, performed for reasons such as peptic ulcer disease, cancer, obesity, or gastroesophageal reflux disease, can result in various post-gastrectomy syndromes. These syndromes include chronic symptoms that range from mild discomfort to life-altering conditions. This guide covers the most common syndromes and their characteristics.
GASTRECTOMY VIDEO SURGERY
Dumping Syndrome
Dumping Syndrome is characterized by gastrointestinal and vasomotor symptoms that occur after food intake due to rapid gastric emptying. This syndrome can occur after surgeries that alter the regulation of gastric emptying or gastric compliance, such as gastrectomy, proximal vagotomy, sleeve gastrectomy, fundoplication, pyloroplasty, and gastrojejunostomy (GJ). Depending on the speed of emptying and the osmolarity of gastric contents, symptoms can vary.
- Early Dumping: Occurs within 30 minutes after food intake and is characterized by palpitations, tachycardia, fatigue, a need to lie down after meals, flushing or pallor, sweating, dizziness, hypotension, headache, and possibly syncope. Abdominal symptoms include early satiety, epigastric fullness, abdominal pain, bloating, hypermotility, and splenic blood pooling.
- Late Dumping: Appears 1 to 3 hours after eating, due to reactive hypoglycemia caused by an initially high glucose load leading to an inappropriately high insulin response. Symptoms include sweating, faintness, difficulty concentrating, and altered levels of consciousness.
Diagnosis is confirmed through an oral glucose tolerance test or a gastric emptying scintigraphy study.
Post-Vagotomy Diarrhea
Post-vagotomy diarrhea is a common complication after vagotomy, characterized by frequent episodes of watery diarrhea. It can be attributed to changes in intestinal motility and bile secretion.
Gastric Stasis
Gastric stasis or delayed gastric emptying can occur due to disruption of normal gastric motility. Symptoms include nausea, vomiting, and a feeling of fullness. Diagnosis is confirmed through gastric emptying studies.
Bile Reflux Gastritis
Bile reflux gastritis is caused by the reflux of bile into the stomach, resulting in epigastric pain and bilious vomiting. Diagnosis can be confirmed through upper endoscopy and gastric pH monitoring.
Afferent and Efferent Loop Syndromes
Afferent loop syndrome occurs after Billroth II reconstruction and is characterized by abdominal pain, bilious vomiting, and distention. Efferent loop syndrome occurs when there is an obstruction of the efferent loop, leading to similar symptoms.
Roux Syndrome
Roux syndrome is a complication of Roux-en-Y procedures, characterized by postprandial abdominal pain and vomiting. Diagnosis is made through a contrast gastrointestinal transit study.
Therapeutic Approach
Management of post-gastrectomy syndromes includes dietary modifications, such as eating small frequent meals, separating liquids and solids, increasing protein and fat intake, and reducing simple sugars. In some cases, additional pharmacological or surgical interventions may be necessary. Understanding these syndromes and their therapeutic approaches is crucial to providing effective care and improving the quality of life for post-gastrectomy patients.
This article focuses on the small proportion of patients with severe, debilitating symptoms; these symptoms can challenge the acumen of the surgeon who is providing the patient’s long-term follow-up and care.










