Impacto dos Análogos de GLP-1 nas Emergências Cirúrgicas
Desafios Diagnósticos e Manejo de Eventos Adversos Abdominais Graves
Autor: Prof. Dr. Ozimo Gama
Categoria: Emergências Cirúrgicas / Cirurgia do Aparelho Digestivo / Segurança do Paciente
Tempo de Leitura: 13 minutos
Introdução
A incorporação dos agonistas do receptor de GLP-1 (como semaglutida e liraglutida) no Sistema Único de Saúde (SUS) representa um marco histórico no combate à obesidade e ao Diabetes Mellitus Tipo 2 (DM2) no Brasil. No entanto, a democratização do acesso e o uso em grande escala dessas medicações trouxeram um novo cenário epidemiológico para as Unidades de Pronto Atendimento (UPAs) e hospitais terciários de emergência. Para nós, cirurgiões do aparelho digestivo, o abdome agudo na era dos “emagrecedores injetáveis” tornou-se um desafio propedêutico complexo. Os efeitos colaterais gastrointestinais habituais dessas drogas — como náuseas, vômitos e dor abdominal — mimetizam ou mascaram afecções cirúrgicas graves. É imperativo que o estudante de medicina, o residente de cirurgia geral e o plantonista de urgência dominem os principais eventos adversos graves associados ao GLP-1 para evitar tanto laparotomias desnecessárias quanto o atraso catastrófico no diagnóstico de complicações reais.
Três Síndromes Clínicas na Urgência
Os análogos de GLP-1 atuam retardando o esvaziamento gástrico e desacelerando o peristaltismo intestinal. Quando essa ação fisiológica extrapola os limites terapêuticos, surgem as complicações de interesse cirúrgico.
1. Gastroparesia Severa e Obstrução Intestinal Funcional
O retardo extremo do esvaziamento gástrico pode evoluir para quadros de gastroparesia grave, mimetizando uma síndrome de obstrução pilórica ou obstrução intestinal alta. O paciente se apresenta com vômitos repetitivos, distensão em andar superior do abdome e dor em cólica.
- O Desafio Diagnóstico: O exame físico pode revelar propulsão gástrica, simulando um abdome agudo obstrutivo mecânico. A tomografia computadorizada (TC) de abdome frequentemente demonstrará um estômago maciçamente distendido, com grande quantidade de resíduo alimentar e líquido, mesmo após períodos prolongados de jejum (frequentemente superiores a 24 ou 48 horas).
2. Doença Biliar Calculosa Aguda (Colecistite e Colangite)
A perda ponderal rápida (frequentemente superior a 1% a 2% do peso corporal por semana) induzida pelos análogos de GLP-1 altera drasticamente a composição da bile. Ocorre um aumento da saturação de colesterol e uma redução drástica da contratilidade da vesícula biliar devido ao menor estímulo de esvaziamento.
- Estatísticas e Impacto: O risco de desenvolvimento de colelitíase, lama biliar e, consequentemente, colecistite aguda ou coledocolitíase triplica em pacientes sob perda de peso acelerada. Na emergência, observamos um influxo crescente de pacientes jovens, sem fatores de risco clássicos prévios, apresentando-se com quadros de urgência biliar e colangite obstrutiva.
3. Pancreatite Aguda Induzida por Drogas
Embora o nexo causal definitivo ainda seja alvo de debates acadêmicos, os grandes ensaios clínicos e o monitoramento pós-comercialização apontam para um risco aumentado de pancreatite aguda em usuários de GLP-1. A estimulação crônica das células acinares e a estase biliar secundária são mecanismos propostos.
- A Armadilha Clínica: O paciente com pancreatite por GLP-1 pode apresentar dor abdominal atípica. Como a própria medicação causa náuseas crônicas, o diagnóstico pode ser negligenciado inicial ou erroneamente atribuído a uma simples dispepsia, retardando a instituição da reposição volêmica vigorosa.
Aplicação na Cirurgia Digestiva: O Protocolo de Abordagem na Urgência
Diante de um paciente na emergência em uso de análogos de GLP-1, a conduta cirúrgica deve ser guiada por uma triagem tática rigorosa para gerenciar a incerteza.
Diferenciação Tática no Abdome Agudo
| Achado Clínico/Tomográfico | Suspeitar de Efeito Colateral Fisiológico/Gastroparesia | Suspeitar de Complicação Cirúrgica Real |
| Dor Abdominal | Difusa, leve a moderada, sem sinais de peritonite. | Localizada (ex: hipocôndrio direito), súbita, com defesa abdominal ou sinal de Blumberg. |
| Imagem (TC de Abdome) | Estômago retencionista isolado, sem parada de eliminação de flatos; ausência de líquido livre. | Borramento da gordura peripancreática, espessamento da parede vesicular, distensão de alças com nível hidroaéreo verdadeiro. |
| Laboratório | Leucograma e PCR normais; amilase/lipase normais. | Leucocitose com desvio, PCR elevada, Amilase/Lipase > 3x o limite superior. |
O Perigo Catastrófico: O Estômago Cheio no Perioperatório
Para o cirurgião digestivo que precisa indicar uma laparotomia ou laparoscopia de urgência (por exemplo, por apendicite aguda ou trauma) em um paciente que faz uso de GLP-1, o risco de aspiração broncopulmonar (Síndrome de Mendelson) na indução anestésica é altíssimo. Mesmo que o paciente jure estar em jejum há mais de 8 ou 12 horas, o estômago deve ser considerado biologicamente “cheio”. A passagem de uma sonda nasogástrica calibrosa para esvaziamento gástrico antes da indução e a intubação em sequência rápida com pressão cricóide (manobra de Sellick) são obrigatórias na urgência.
Pontos-Chave
- Anamnese Dirigida: Perguntar ativamente sobre o uso de medicações injetáveis para emagrecimento (muitos pacientes omitem por não considerarem “remédio tradicional”).
- Esvaziamento Retardado: Assumir estômago cheio em qualquer cenário de urgência anestésico-cirúrgica, independentemente do tempo de jejum relatado.
- Triagem Biliar: Elevar o índice de suspeição para colecistite aguda e coledocolitíase em pacientes que perderam peso rapidamente com a medicação.
- Amilase e Lipase: Devem ser dosadas em qualquer paciente com dor abdominal em andar superior sob uso de GLP-1, afastando precocemente a pancreatite aguda.
- Evitar Laparotomias Brancas: Diferenciar a dor e os vômitos da gastroparesia medicamentosa de uma obstrução mecânica verdadeira através de TC de abdome com triplo contraste.
Conclusões Aplicadas à Prática
A chegada massiva dos análogos de GLP-1 ao SUS exige uma atualização imediata dos algoritmos de atendimento nas salas de emergência brasileiras. O cirurgião do aparelho digestivo moderno não pode mais avaliar o abdome agudo com os mesmos olhos de uma década atrás. Devemos atuar como um filtro crítico de precisão. Reconhecer que a medicação distorce a semiologia abdominal clássica é o primeiro passo para evitar erros terapêuticos. Ao unirmos a vigilância epidemiológica ao conhecimento fisiopatológico profundo, garantimos que os benefícios imensos dessas medicações no controle da obesidade não sejam eclipsados por desfechos desfavoráveis nas salas de urgência. No teatro de operações da emergência, a informação correta é a nossa melhor linha de defesa.
“O cirurgião que não acompanha a evolução da farmacologia clínica está condenado a operar as complicações que ele não compreende ou a negligenciar as urgências que ele confunde.” — Adaptado dos aforismos de liderança cirúrgica contemporânea.
Gostou ❔Nos deixe um comentário ✍️ , compartilhe em suas redes sociais e|ou mande sua dúvida pelo 💬 Chat On-line em nossa DM do Instagram.
Colecistectomia: O perigo da falsa “Simplicidade”
A cirurgia de retirada da vesícula biliar é a mais comum da especialidade digestiva, mas a percepção de que é um procedimento “simples” esconde riscos catastróficos que exigem uma nova cultura de segurança.
Todos conhecemos alguém que já “tirou a vesícula”. No Brasil, apenas pelo Sistema Único de Saúde (SUS), são realizadas mais de 200 mil colecistectomias anualmente. A introdução da técnica laparoscópica — a cirurgia por vídeo — na década de 1990, trouxe benefícios inquestionáveis: cicatrizes mínimas, menos dor e um retorno quase imediato ao trabalho. No entanto, essa aura de facilidade criou uma armadilha perigosa tanto para pacientes quanto para cirurgiões: a banalização de um procedimento que, em segundos, pode transformar uma patologia benigna em uma tragédia crônica.
O paradoxo é alarmante. Apesar do avanço tecnológico e da vasta experiência acumulada em três décadas, a incidência de lesão da via biliar (LVB) — o dano aos canais que transportam a bile do fígado ao intestino — permanece obstinadamente estável, ocorrendo em cerca de 0,3% a 0,5% dos casos por vídeo. Surpreendentemente, esta taxa é superior à da antiga era da cirurgia aberta. O que a literatura médica qualifica como a “lesão clássica” não é, em regra, fruto de imperícia manual ou falta de conhecimento anatômico, mas sim de uma “ilusão de percepção visual”.
Estudos seminais indicam que 97% das lesões ocorrem porque o cérebro do cirurgião, enganado pela tração e pela inflamação, identifica o ducto biliar principal como se fosse o ducto cístico. É um erro cognitivo, não técnico. Por isso, a colecistectomia não pode ser tratada como um procedimento de “entrada” ou de menor importância. Ela exige o que chamamos de Visão Crítica de Segurança (CVS), uma doutrina sistematizada pelo cirurgião Steven Strasberg que obriga a identificação cabal de estruturas antes de qualquer corte. Sem CVS, não há segurança; há apenas sorte.
A banalização também se manifesta na resistência em adotar as chamadas “manobras de resgate” (bailout). Diante de uma vesícula hostil, com inflamação severa que impede a visão clara da anatomia, o cirurgião prudente deve ter a humildade e a sabedoria de interromper a dissecação clássica. Técnicas como a colecistectomia subtotal — onde parte do órgão é deixada para preservar a via biliar — devem ser vistas como um sinal de maturidade clínica e “sabedoria cirúrgica”, e não como um fracasso. O objetivo final nunca deve ser “tirar a vesícula a qualquer custo”, mas sim “não lesar o paciente”.
O custo humano de uma lesão biliar é imenso. O paciente, outrora saudável, pode tornar-se o que a literatura tragicamente apelida de “aleijado biliar”, enfrentando múltiplas reoperações, internações prolongadas e o risco de cirrose biliar secundária. O impacto médico-legal e o custo para o sistema de saúde são igualmente devastadores.
Felizmente, estamos em uma nova fronteira. O uso de fluorescência com verde de indocianina (ICG), que permite “enxergar” os canais biliares através do tecido, e a integração da Inteligência Artificial como um “segundo par de olhos” no monitor, prometem reduzir a margem para o erro humano. Todavia, a tecnologia sozinha não basta.
É preciso consolidar uma Cultura de Segurança em Colecistectomia (COSIC). Isso envolve desde a documentação fotográfica rigorosa dos passos cirúrgicos até a coragem de pedir ajuda ou converter o procedimento quando a anatomia se torna um enigma. A colecistectomia laparoscópica é uma vitória da medicina moderna, mas sua eficácia depende do reconhecimento de que, sob sua aparente simplicidade, reside uma das operações mais perigosas da cirurgia abdominal. Respeitar essa complexidade é o primeiro passo para proteger a vida de milhares de brasileiros que passam por nossas mesas de operação todos os dias.
Prof. Dr. Ozimo Gama | Cirurgião Digestivo
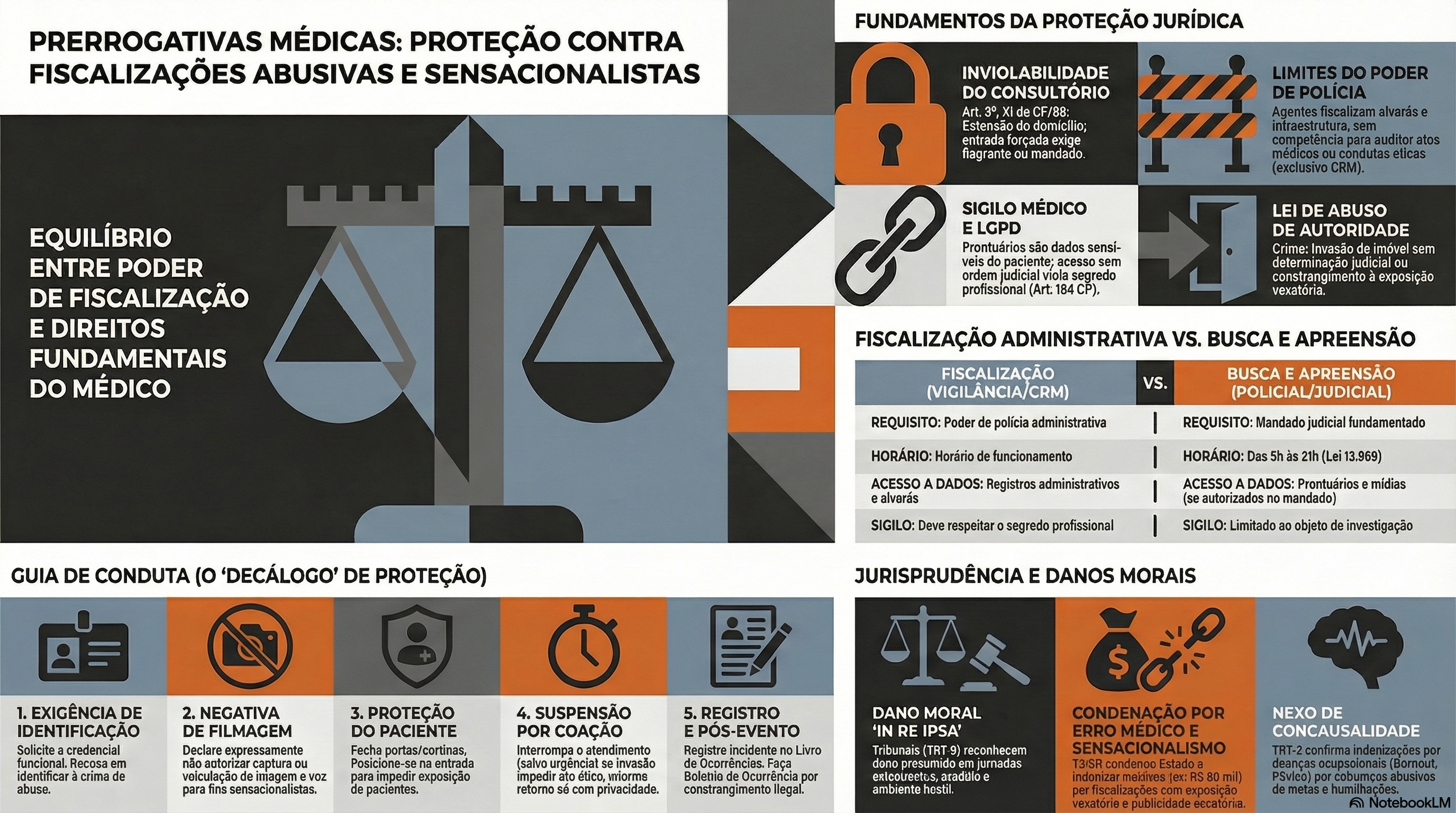
Proteção Médica contra Fiscalizações Invasivas e Sensacionalistas
No atual cenário das unidades de urgência e emergência, observa-se uma crescente e indevida ingerência de agentes externos que, sob o pretexto do escrutínio midiático, submetem o corpo clínico — em especial os profissionais em início de carreira — a constrangimentos e intimidações. Tais condutas, frequentemente pautadas pelo sensacionalismo digital, não apenas desestabilizam o ato médico, como violam preceitos basilares da Bioética e do Direito, notadamente o sigilo profissional e a dignidade do paciente. Diante desse panorama de vulnerabilidade técnica e jurídica, o presente Decálogo de Proteção Profissional Médica emerge como um instrumento essencial de salvaguarda, transpondo a dogmática jurídica para a práxis cotidiana. Este guia oferece diretrizes objetivas de conduta e interlocução, permitindo ao médico exercer sua autonomia com o rigor técnico, a polidez e a segurança jurídica que a complexidade do ambiente hospitalar exige.

I. Manutenção da Postura Ética e Prevenção do Conflito O médico deve manter o controle emocional, adotando postura polida e técnica. É imperativo evitar qualquer embate físico ou agressão verbal com os invasores, neutralizando o objetivo sensacionalista da ação.
- Fundamentação Jurídica e Ética: Código de Ética Médica (Resolução CFM nº 2.217/2018), Capítulo I, Inciso II; Art. 5º, inciso X, da Constituição Federal.
- O que fazer e o que falar: Respire fundo, cruze os braços ou mantenha as mãos visíveis (evitando qualquer gesto que possa ser interpretado como agressão). Não tente tomar o celular ou a câmera do invasor.
- Fala: “Boa noite/dia. Por favor, peço que mantenham a calma e baixem o tom de voz. Estamos em um ambiente hospitalar de respeito e cuidado.”
II. Exigência de Identificação e Recusa Expressa de Filmagem O profissional deve solicitar a identificação da autoridade e declarar, em bom tom (para que fique registrado na própria gravação), que não autoriza o uso, captura ou veiculação de sua imagem e voz.
- Fundamentação Jurídica e Ética: Art. 5º, inciso X, da Constituição Federal; Art. 20 do Código Civil.
- O que fazer e o que falar
- Ação: Olhe diretamente para a pessoa (e não para a câmera). Adote um tom de voz firme, porém sem gritar.
- Fala: “Sou o médico plantonista responsável neste momento. Por gentileza, identifiquem-se. Deixo expressamente claro, e peço que fique registrado em sua gravação, que não autorizo a captura, o uso ou a veiculação da minha imagem e da minha voz.”
III. Acionamento Imediato da Cadeia de Comando Institucional A gestão do fluxo de pessoas não é atribuição do médico assistente. Deve-se delegar a um membro da equipe (enfermagem/técnicos) o acionamento urgente da Segurança Patrimonial, da Chefia de Plantão e do Diretor Técnico da instituição.
- Fundamentação Jurídica e Ética: Resolução CFM nº 2.147/2016.
- O que fazer e o que falar
- Ação: Vire-se calmamente para um colega da equipe multidisciplinar e delegue a função, sem dar as costas totalmente aos invasores.
- Fala: “Enfermeiro(a) [Nome], por favor, acione imediatamente a segurança do hospital, a chefia de plantão e comunique o Diretor Técnico de que temos pessoas não autorizadas e com câmeras no setor.”
IV. Isolamento Físico e Proteção da Intimidade do Paciente A prioridade máxima é salvaguardar o paciente em atendimento. O médico deve fechar portas, fechar cortinas e posicionar-se fisicamente na entrada de consultórios ou enfermarias, bloqueando o acesso visual das câmeras aos enfermos.
- Fundamentação Jurídica e Ética: Art. 5º, inciso X, da Constituição Federal; Art. 73 do Código de Ética Médica.
- O que fazer e o que falar:
- Ação: Caminhe de forma decidida até a porta do consultório ou enfermaria, feche-a e coloque-se à frente dela como um obstáculo físico pacífico.
- Fala: “Os senhores não podem entrar aqui. Temos pacientes desnudos e vulneráveis em atendimento. Exijo que respeitem a privacidade e a intimidade dos enfermos.”
V. Evocação Expressa do Sigilo Médico e Profissional Diante da tentativa de invasão em áreas assistenciais, o médico deve declarar que está sob o imperativo legal do sigilo e que a presença de terceiros não autorizados munidos de câmeras configura quebra indireta de confidencialidade.
- Fundamentação Jurídica e Ética: Art. 154 do Código Penal Brasileiro; Art. 73, parágrafo único, do Código de Ética Médica.
- O que fazer e o que falar:
- Ação: Ignore perguntas médicas ou clínicas sobre qualquer paciente (“por que fulano está esperando?”, “o que aquele paciente tem?”).
- Fala: “Como médico, sou regido pela lei do sigilo absoluto. Não responderei a perguntas sobre casos clínicos e não permitirei filmagens nesta área, pois isso configura crime de quebra de confidencialidade médica.”
VI. Negativa Peremptória de Acesso a Prontuários Médicos O profissional deve negar a entrega, leitura ou auditoria de prontuários por parte de parlamentares ou fiscais não vinculados aos Conselhos de Medicina, informando que o documento pertence exclusivamente ao paciente.
- Fundamentação Jurídica e Ética: Resolução CFM nº 1.638/2002; Art. 89 do Código de Ética Médica.
- O que fazer e o que falar:
- Ação: Feche pastas de prontuários físicos ou bloqueie a tela do computador/sistema eletrônico.
- Fala: “O prontuário é um documento legal e de propriedade exclusiva do paciente. Sem a autorização expressa e por escrito dele, ou sem ordem judicial, os senhores não terão acesso a nenhum documento médico.”
VII. Esclarecimento dos Limites da Competência Fiscalizatória O médico deve esclarecer à autoridade que o exercício de “poder de polícia” parlamentar se restringe à infraestrutura e à administração pública, não abrangendo a fiscalização do ato médico ou da conduta ética, que possuem foro específico.
- Fundamentação Jurídica e Ética: Lei nº 3.268/1957.
- O que fazer e o que falar:
- Ação: Mantenha a compostura caso o político tente dar “ordens” ou fazer “ameaças” usando o cargo.
- Fala: “Reconheço o seu cargo, mas o senhor tem competência para fiscalizar a estrutura administrativa. A fiscalização do ato médico e da conduta profissional é prerrogativa exclusiva do Conselho Regional de Medicina (CRM). Por favor, dirija suas demandas ao Diretor da unidade.”
VIII. Suspensão do Atendimento sob Coação (Garantia de Condições Dignas) Caso as câmeras adentrem o recinto de atendimento e os invasores se recusem a sair, o médico deve suspender temporariamente o ato médico — desde que não seja caso de urgência/emergência — informando que só retornará quando a privacidade for restabelecida.
- Fundamentação Jurídica e Ética: Código de Ética Médica, Capítulo II, Inciso IV (Direitos dos Médicos).
- O que fazer e o que falar:
- Ação: Caso invadam a sala de forma ríspida, interrompa a consulta (se não houver risco de morte), sente-se na cadeira, afaste-se do paciente e aguarde em silêncio a retirada dos invasores pela segurança.
- Fala: “Diante da invasão e da coação com câmeras, informo que não possuo condições dignas e éticas para exercer a medicina neste momento. Retomarei o atendimento imediatamente após os senhores se retirarem e a segurança do paciente for garantida.”
IX. Registro Documental Exaustivo do Incidente Tão logo a situação seja normalizada, o médico deve registrar o fato detalhadamente no Livro de Ocorrências do plantão. Caso a invasão tenha prejudicado ou atrasado o atendimento de algum paciente, tal interferência externa deve constar no prontuário do mesmo.
- Fundamentação Jurídica e Ética: Art. 87 do Código de Ética Médica; Art. 299 do Código Penal.
- O que fazer e o que falar:
- Ação: Escreva de forma objetiva, descrevendo fatos (sem adjetivos emocionais). Cite os nomes dos invasores, a recusa em parar de filmar e os horários exatos.
- Fala (orientação mental e à equipe): “Precisamos registrar tudo. Vamos anotar o nome do vereador/político, o horário exato da invasão, o que foi dito e as paralisações geradas no atendimento para colocar no livro do plantão agora mesmo.”
X. Acionamento das Autoridades Policiais e Desagravo Institucional Ao término do plantão, é fundamental registrar Boletim de Ocorrência Policial e enviar comunicação oficial (Ofício) ao Diretor Técnico e ao Conselho Regional de Medicina (CRM) relatando o constrangimento.
- Fundamentação Jurídica e Ética: Decreto-Lei nº 3.688/1941, Art. 42; Art. 150 do Código Penal; Código de Ética Médica, Capítulo II, Inciso V.
- O que fazer e o que falar:
- Ação: Dirija-se a uma delegacia (ou delegacia virtual) e, nos dias subsequentes, contrate um advogado e/ou assessoria jurídica institucional e/ou do sindicato médico.
- Fala (na Delegacia / no Ofício): “Desejo registrar um Boletim de Ocorrência por constrangimento ilegal, perturbação do ambiente de trabalho e quebra tentada de sigilo médico contra o invasor. Solicitarei também, via ofício, o desagravo público junto ao CRM.”
A nossa missão máxima será sempre a defesa da saúde e da dignidade do doente. Que as orientações sirvam para garantir que nenhum profissional permita a usurpação do seu local de trabalho, assegurando que a nobre arte da Medicina seja sempre exercida em condições de absoluta segurança, privacidade e respeito mútuo.
Prof. Dr. Ozimo Gama
Prevenção Jurídica na Cirurgia Digestiva
As bases das Boas Práticas Jurídicas para o Cirurgião Moderno
Autor: Prof. Dr. Ozimo Gama (Tempo de Leitura: 10 minutos)
Introdução
A prática da cirurgia do aparelho digestivo evoluiu exponencialmente com o advento da cirurgia minimamente invasiva e da robótica. Contudo, essa evolução técnica foi acompanhada por um fenômeno igualmente complexo: a crescente judicialização da medicina. Dados recentes do Conselho Nacional de Justiça (CNJ) apontam um aumento alarmante nas ações judiciais envolvendo supostos erros médicos no Brasil, sendo as especialidades cirúrgicas (incluindo a cirurgia bariátrica e a cirurgia geral) alvos frequentes. Para o estudante de medicina, o residente e o cirurgião já estabelecido, a excelência técnica no centro cirúrgico não é mais suficiente. A proteção jurídica e a gestão de riscos tornaram-se competências inegociáveis. Este artigo traduz as melhores evidências em compliance e prevenção de responsabilidade profissional para a nossa realidade clínica e cirúrgica.
Os Pilares da Proteção Jurídica
A literatura jurídica e de gestão de risco em saúde não prescreve uma “fórmula mágica”, mas estabelece padrões consistentes de governança. A defesa do cirurgião baseia-se na proatividade, ou seja, em ações tomadas antes que o dano ou o litígio ocorram. A mitigação ativa de riscos envolve desde a estruturação de fluxos de atendimento até o amparo em apólices de seguros, garantindo que o profissional exerça sua vocação com autonomia, segurança e paz de espírito.
Práticas Fundamentais
Como aplicamos esses conceitos abstratos na rotina de um serviço de cirurgia digestiva? Abaixo, detalho as boas práticas essenciais baseadas em evidências:
1. Documentação Inatacável e o TCLE
O prontuário médico é a principal (e muitas vezes a única) testemunha de defesa do cirurgião. A documentação deve ser clara, tempestiva e exaustiva. Na cirurgia digestiva, isso se traduz em:
- Descrição Cirúrgica Detalhada: Não economize palavras ao descrever aderências severas, variações anatômicas do trato biliar ou a qualidade dos tecidos ao realizar uma anastomose intestinal.
- Termo de Consentimento Livre e Esclarecido (TCLE): Um TCLE genérico não tem valor jurídico. Ele deve ser individualizado. Vai operar um câncer gástrico? O paciente deve estar ciente (e assinar) sobre os riscos de fístula do coto duodenal, necessidade de CTI e mortalidade associada. O diálogo prévio bem documentado anula a alegação de “falta de informação”.
2. Adesão à Lex Artis e aos Protocolos Clínicos
Agir de acordo com a Lex Artis significa atuar conforme as práticas médicas consagradas e atualizadas. A adesão a diretrizes técnicas (Guidelines) de sociedades como o CBCD, SBCBM ou protocolos internacionais (como o ERAS – Enhanced Recovery After Surgery) é a forma mais eficaz de afastar a culpa (negligência, imprudência ou imperícia).
- Exemplo prático: O uso sistemático do Checklist de Cirurgia Segura da OMS previne a catástrofe médico-legal da cirurgia em paciente ou local errado, além de garantir a profilaxia antimicrobiana no tempo correto.
3. A Comunicação como Escudo Protetor
A ampla maioria dos processos por erro médico nasce de uma quebra na relação médico-paciente. Quando ocorre uma complicação grave — como uma deiscência de anastomose após uma retossigmoidectomia —, a postura do cirurgião dita o desfecho legal. A comunicação proativa, empática, transparente e não conflituosa com o paciente e seus familiares reduz drasticamente o ímpeto litigioso. Abandonar o paciente aos cuidados exclusivos do médico plantonista da UTI após uma complicação é o caminho mais rápido para um tribunal.
4. Governança de Dados e a LGPD
A Lei Geral de Proteção de Dados (LGPD) transformou a gestão de informações médicas. Os controles técnicos de privacidade são mandatórios.
- Cuidado com imagens: Fotografar peças cirúrgicas (como vesículas, tumores) ou exames de imagem e compartilhar em grupos de WhatsApp, mesmo que com intenção didática, sem a anonimização estrita ou o consentimento expresso do paciente, constitui grave infração ética e legal.
5. Seguro de Responsabilidade Profissional e Assessoria Especializada
Operar sem um seguro de responsabilidade civil profissional é expor o patrimônio pessoal a um risco imensurável. É vital compreender as coberturas da apólice, especialmente a cláusula de tail coverage (cobertura de cauda), que garante proteção contra processos instaurados anos após a ocorrência do fato gerador. Além disso, ao primeiro sinal de notificação administrativa (CRM) ou citação judicial, a prática de agir sem o suporte de advogados especialistas em Direito Médico é temerária. A confidencialidade e a estratégia da relação advogado-cliente são irrenunciáveis.
Pontos-Chave para a Prática Diária
- O Prontuário Médico não é apenas uma obrigação burocrática; é a sua armadura legal.
- TCLE é um processo de comunicação, não apenas um pedaço de papel a ser assinado na porta do bloco cirúrgico.
- Aderir estritamente aos Guidelines e Protocolos estabelece um padrão de cuidado defensável.
- Nunca subestime o poder de uma Relação Médico-Paciente baseada na confiança, empatia e presença contínua, especialmente nas adversidades.
Conclusões Aplicadas
A complexidade inerente à cirurgia do aparelho digestivo nos expõe diariamente a riscos biológicos imponderáveis. Fístulas, sangramentos e infecções podem ocorrer mesmo quando a técnica cirúrgica é executada com perfeição. O que diferencia a complicação inerente do ato cirúrgico (o risco aceitável) do ilícito civil ou ético é, fundamentalmente, a nossa conduta preventiva, a clareza da nossa documentação e o rigor ético no trato com o paciente. A proteção jurídica não deve gerar uma “medicina defensiva” prejudicial ao doente (que gera exames e intervenções desnecessárias), mas sim uma medicina preventiva, baseada em compliance, transparência e excelência documental.
“As complicações fazem parte da cirurgia, mas o abandono do paciente e a negligência na documentação são escolhas exclusivas do cirurgião. A verdadeira destreza opera tanto com o bisturi quanto com a caneta.” — Adaptado de preceitos de grandes mestres da cirurgia contemporânea.
Gostou ❔Nos deixe um comentário ✍️ , compartilhe em suas redes sociais e|ou mande sua dúvida pelo 💬 Chat On-line em nossa DM do Instagram.
Evolução da Medicina Operacional
Lições Eternas para a Logística de Saúde Militar
Prof. Dr. Ozimo Gama
1. O Elo entre o Passado e a Prontidão Operacional
A Medicina Operacional transcende a mera assistência de retaguarda; ela se consolida como um multiplicador de poder de combate indispensável para a manutenção do efetivo combatente. No cenário de defesa contemporâneo, a preservação da integridade física e psíquica da tropa é o fiel da balança que sustenta a viabilidade de campanhas em ambientes de conectividade limitada e logística hostil, como a Região Amazônica, ou em missões sob a égide de organismos internacionais. Aprender com a história militar não é um exercício diletante, mas um imperativo para a Prontidão Operacional. O objetivo é garantir que o apoio de saúde seja resiliente o suficiente para operar sob o atrito do combate, assegurando a “Manutenção do Poder de Combate” — princípio basilar para que o soldado retorne à linha de fogo com a celeridade que a manobra exige. Embora as tecnologias cinéticas evoluam, os princípios de salvar vidas sob fogo permanecem como constantes doutrinárias desde a Antiguidade.
2. Das Cruzadas ao Campo de Batalha Primitivo: O Nascimento do Cuidado sob Fogo
Os conflitos da Idade Média, notadamente as Cruzadas, forçaram a Medicina a migrar do conforto clerical para a brutalidade das intervenções cirúrgicas de campanha. Um exemplo emblemático da “Medicina Operacional” rudimentar ocorreu em agosto de 1097, quando o Duque Godofredo de Bouillon, ao enfrentar um urso selvagem próximo a Antioquia, feriu gravemente a própria perna com sua espada. O sangramento arterial massivo exigiu que os médicos da época agissem minuto a minuto sob extrema pressão. Utilizando técnicas de cauterização com ferro em brasa — inspiradas nos ensinamentos de Albucasis — os cirurgiões estancaram a hemorragia, permitindo que o líder sobrevivesse para retomar o comando meses depois. A organização dos hospitais pela Ordem de São João (Hospitaleiros) em Jerusalém e Acre representou o embrião da triagem e da higiene militar. Estes “xenodóquios” separavam pacientes por diagnóstico, demonstrando que a gestão de leitos e a separação de feridos traumáticos de doentes infectocontagiosos eram vitais para a sustentabilidade da força.
Inteligência Técnica Imediata e Sensível (ITIS): O episódio de Godofredo de Bouillon ilustra que o sucesso do apoio de saúde depende da capacidade de decisão técnica sob estresse. Para o oficial moderno, a lição é clara: sem intervenção imediata no ponto de ferimento, a taxa de retorno ao serviço é nula. A sustentabilidade das campanhas de longo prazo nas Cruzadas só foi possível devido a essa estruturação de cuidados que, embora rudimentar, já visava a preservação do componente humano como recurso estratégico.

3. A Revolução de Dominique Jean Larrey: O Surgimento da Logística Moderna
O Barão Dominique Jean Larrey, cirurgião-chefe da Guarda Imperial de Napoleão, é legitimamente o “pai da medicina operativa moderna”. Sua visão transformou o apoio de saúde de um serviço passivo na Zona de Retaguarda (ZRE) para uma força de intervenção proativa na vanguarda.
- Inovação das Ambulances Volantes: Larrey revolucionou a Evacuação de Feridos (Evoz) ao criar ambulâncias leves que retiravam os feridos ainda sob o fogo inimigo, combatendo a “inatividade administrativa” que abandonava soldados no campo.
- Cirurgia de Urgência e Técnica: Defensor do débridement précoce (debridamento precoce) e das feridas laissées ouvertes (deixadas abertas) para prevenir a gangrena gasosa, Larrey era dotado de uma velocidade técnica prodigiosa, capaz de realizar a desarticulação de um ombro em apenas dois minutos — perícia vital em um Posto de Socorro (PS) operando sem anestesia moderna.
- Ética e Neutralidade: Precursor da Cruz Vermelha, Larrey estabeleceu o “Hôpital destiné à l’ennemi” em Valladolid, tratando prisioneiros espanhóis e ingleses com a mesma dignidade que os franceses.
Napoleão reconheceu sua importância ao declarar: “O homem mais honesto que já conheci… uma imagem do verdadeiro homem de bem”.
ITIS: : A mobilidade de Larrey alterou o moral da tropa (segurança psicológica). No Exército Brasileiro, essa herança reflete-se na busca pela “Hora de Ouro”. O legado de Larrey ensina que o oficial médico deve ser um “chirurgien combattant de l’avant”, integrado à manobra e não apenas um espectador na retaguarda.

4. Século XIX à Era Contemporânea: Da Enfermagem de Nightingale à Evacuação Aeromédica
A Guerra da Crimeia trouxe Florence Nightingale e a revolução da sanidade, mas foi a inovação técnica de Antonius Mathijsen, em 1851, com o gesso (Plaster of Paris), que transformou a logística de saúde. A estabilização eficaz de fraturas permitiu que a Cadeia de Evacuação se tornasse mais resiliente e longa; fraturas estáveis reduziam o risco de embolia gordurosa e trauma secundário durante o transporte, permitindo fluxos logísticos mais audazes. No século XX, o advento dos Mobile Army Surgical Hospitals (MASH) e do helicóptero na Coreia e Vietnã redefiniu a velocidade do apoio. Atualmente, o protocolo Tactical Combat Casualty Care (TCCC) padroniza intervenções salvadoras de vida no ponto de ferimento, focando na tríade: controle de hemorragia, manejo de via aérea e prevenção de hipotermia.
ITIS”: A evolução tecnológica, da tração animal ao Medevac, exige uma coordenação logística impecável de insumos críticos, como sangue e oxigênio. A lição para o planejamento atual é que a tecnologia só é eficaz se houver uma rede de suprimento integrada que acompanhe a velocidade do transporte.

5. O Cenário Brasileiro: Doutrina e o Papel das Forças Armadas
No Brasil, a doutrina é balizada pelo manual MD42-M-04 (Logística de Saúde em Operações Conjuntas), que estabelece os Níveis de Apoio e a interoperabilidade entre o Exército, a Marinha e a Força Aérea. O Corpo de Fuzileiros Navais (CFN), através do seu Batalhão Logístico (BtlLogFuzNav), opera unidades de saúde móveis com alta capacidade expedicionária, aplicando os princípios de Larrey em ambientes litorâneos e ribeirinhos. Na Amazônia, o planejamento exige o uso intensivo de Inteligência Médica (conforme a doutrina NATO AJMEDP-3). Isso significa mais do que tratar doenças; implica mapear a “capacidade hospitalar local” em municípios remotos e monitorar “vetores endêmicos” (como a malária e a leishmaniose). Sem a Inteligência Médica para antecipar ameaças sanitárias, uma força pode ser dizimada antes mesmo do primeiro contato cinético com o inimigo.
ITIS”: A Inteligência Médica é uma ferramenta de antecipação estratégica. Em operações na selva, conhecer o terreno e o perfil epidemiológico local permite ao oficial de saúde dimensionar a Cadeia de Evacuação de forma a garantir que a distância não seja uma sentença de morte para o combatente.

6. Planejamento Logístico Atual
- A Proximidade do Apoio (O Legado do PS): A estabilização deve ocorrer no Nível 1 de apoio, o mais próximo possível da linha de contato, para maximizar a sobrevivência e o retorno à linha de fogo.
- Mobilidade e Evoz: O sistema de saúde deve ser tão ágil quanto a força de manobra. O apoio estático é apoio vulnerável.
- Triagem como Decisão Ética e Tática: Em situações de baixas em massa (MASCAL), a triagem rápida e imparcial é a única ferramenta capaz de otimizar recursos limitados.
- Inteligência Médica (AJMEDP-3): Antecipar ameaças ambientais e mapear a infraestrutura civil local é essencial para a resiliência logística em teatros de operações isolados.
- Unicidade da Cadeia Logística: Do suprimento de sangue à evacuação aeromédica, a logística de saúde deve ser tratada como um sistema unitário e ininterrupto.
7. A Missão Continua
A Medicina Operacional é uma ciência de adaptação, coragem e sacrifício. Do cirurgião que operava sob o frio da Berezina ao oficial médico que planeja o apoio em um Pelotão Especial de Fronteira na Amazônia, o compromisso com a vida do combatente permanece o mesmo. A logística de saúde é o sistema circulatório da força; seu sucesso garante que o Brasil disponha de militares prontos, resilientes e protegidos.
Leitura Recomendada
- BRASIL. Ministério da Defesa. MD42-M-04: Logística de Saúde em Operações Conjuntas. Brasília: MD, 2015.
- GABRIEL, R. A.; METZ, K. S. A History of Military Medicine. New York: Greenwood Press, 1992.
- LARREY, Dominique Jean. Mémoires de chirurgie militarie et campagnes. Baltimore: Joseph Cushing, 1814.
- MCCALLUM, Jack E. Military Medicine: From Ancient Times to the 21st Century. Santa Barbara: ABC-CLIO, 2008.
- MITCHELL, Piers D. Trauma and Surgery in the Crusades. London: University of London, 2002.
- ORGANIZAÇÃO DO TRATADO DO ATLÂNTICO NORTE (NATO). AJMEDP-3: Allied Joint Medical Doctrine for Medical Intelligence. Brussels: NATO Standardization Office, 2015.
- SOUBIRAN, A. Le Baron Larrey: Chirurgien de Napoléon. Paris: Fayard, 1966.
- VAYRE, P.; FERRANDIS, J. J. Dominique Larrey (1766-1842), Chirurgien militaire – Baron d’Empire. e-mémoires de l’Académie Nationale de Chirurgie, v. 3, n. 1, p. 37-46, 2004.
Comunicação Cirúrgica
Padrões, Tensões e Implicações para a Segurança do Paciente na Cirurgia Digestiva
Introdução
A comunicação cirúrgica constitui elemento fundamental da prática operatória contemporânea. Mais do que mera troca de informações técnicas, ela representa o mecanismo central de coordenação relacional entre cirurgião, anestesista, instrumentador, circulante e demais membros da equipe. Na cirurgia digestiva — campo marcado por procedimentos de alta complexidade, como gastrectomias, hepatectomias e colectomias — a qualidade da comunicação influencia diretamente os desfechos clínicos, a formação de residentes e a cultura de segurança do paciente.
Estudos observacionais e revisões sistemáticas recentes demonstram que falhas comunicativas contribuem para mais de 70% dos eventos sentinelas em saúde, conforme dados da The Joint Commission. Na sala de operação, análises de 421 interações revelaram falhas em aproximadamente 30% das trocas entre membros da equipe, gerando ineficiência, tensão e risco aumentado ao paciente (Dingley et al., 2008). Neste artigo examinaremos algunmas evidências científicas sobre o tema, com ênfase em três investigações paradigmáticas, visando oferecer subsídios educativos para cirurgiões digestivos e equipes multidisciplinares.
Padrões de Comunicação Observados em Equipes Cirúrgicas
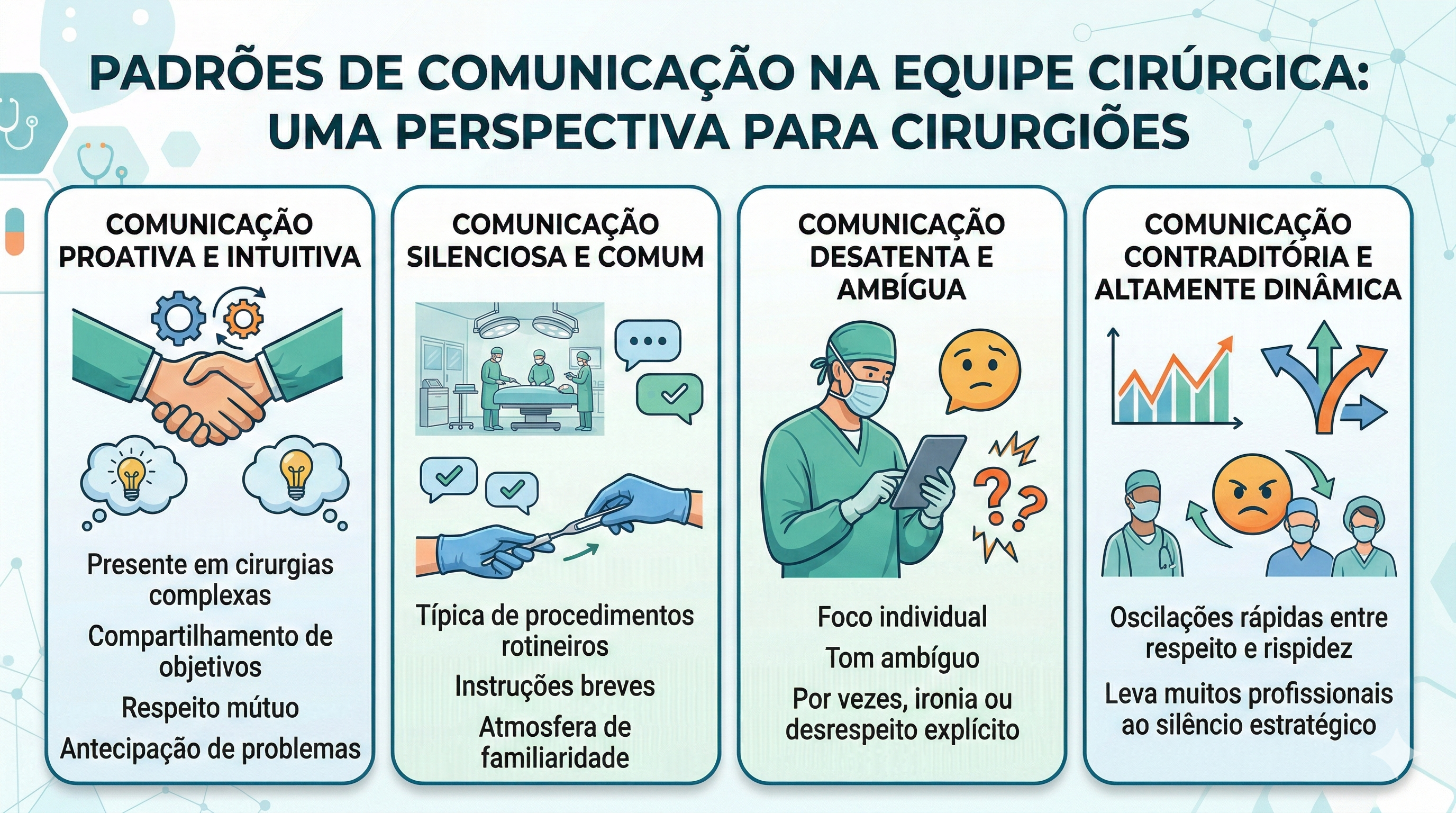
Pesquisa etnográfica conduzida por Tørring et al. (2019), que acompanhou 39 equipes cirúrgicas (85 profissionais) durante substituições de quadril e joelho — procedimentos com paralelos diretos à cirurgia digestiva —, identificou quatro padrões distintos de interação:
- Comunicação proativa e intuitiva: presente em cirurgias complexas, caracterizada por compartilhamento de objetivos, respeito mútuo e antecipação de problemas.
- Comunicação silenciosa e comum: típica de procedimentos rotineiros, marcada por instruções breves e atmosfera de familiaridade.
- Comunicação desatenta e ambígua: marcada por foco individual, tom ambíguo e, por vezes, ironia ou desrespeito explícito.
- Comunicação contraditória e altamente dinâmica: oscilações rápidas entre respeito e rispidez, levando muitos profissionais ao silêncio estratégico.
Esses padrões ilustram que a comunicação eficaz transcende palavras: envolve linguagem corporal, tom de voz e alinhamento de expectativas coletivas.
Locais de Tensão Comunicativa e Seus Efeitos Formativos
Lingard et al. (2002), em estudo com 128 horas de observação em 35 procedimentos cirúrgicos, mapearam cinco temas recorrentes de tensão: tempo, segurança/esterilidade, recursos (equipamentos), papéis da equipe e controle da situação. Tais tensões surgem com frequência entre cirurgião sênior e equipe de enfermagem, impactando diretamente os novatos. Os residentes e estudantes reagem predominantemente de duas formas: imitação (mimicry) do estilo autoritário ou retirada (withdrawal), silenciando-se. Ambas as respostas perpetuam ciclos de conflito interprofissional em vez de promover resolução colaborativa. Na cirurgia digestiva, onde o tempo de isquemia, sangramento e integridade anastomótica são críticos, tais dinâmicas podem comprometer a qualidade assistencial e o aprendizado.
Aspectos Emocionais e o Clima da Sala Cirúrgica
Revisão de escopo realizada por Lee et al. (2023), que analisou 10 estudos qualitativos e quantitativos, reforça que o centro cirúrgico é ambiente emocionalmente carregado. O tom e a atitude do líder — geralmente o cirurgião — definem o “clima” da sala. Cultura hierárquica e estresse inibem o speaking up, especialmente entre enfermeiros e residentes. Quando o cirurgião manifesta frustração por meio de gritos ou culpas, instalam-se medo, redução da moral e falhas comunicativas que elevam o risco de eventos adversos. A revisão destaca que o controle emocional não é aspecto acessório, mas competência clínica essencial. Em cirurgias digestivas de grande porte, onde a pressão temporal e a complexidade técnica são elevadas, a regulação emocional do cirurgião torna-se fator protetor da segurança do paciente.
Implicações Práticas para a Cirurgia Digestiva Atual
A integração dos achados demonstra que competência técnica isolada é insuficiente. O cirurgião digestivo contemporâneo deve cultivar inteligência emocional e habilidade retórica para fomentar coordenação relacional. Estratégias como briefing pré-operatório, debriefing estruturado e treinamento em comunicação não-técnica (CRM — Crew Resource Management) reduzem significativamente as falhas identificadas nos estudos citados. Na prática diária, reconhecer os padrões descritos por Tørring, mitigar tensões mapeadas por Lingard e gerir o clima emocional destacado por Lee constitui caminho direto para melhores desfechos, menor burnout da equipe e formação mais robusta de novos cirurgiões.
Conclusão
A comunicação cirúrgica não é mero instrumento operacional; é o alicerce da segurança do paciente e da excelência assistencial na cirurgia digestiva. Os estudos analisados evidenciam que padrões comunicativos saudáveis, gestão de tensões e controle emocional reduzem riscos, otimizam processos e fortalecem o desenvolvimento profissional. Investir nesse domínio representa avanço científico e ético irrenunciável.
“A cirurgia não é um desempenho individual, mas um trabalho de equipe.” Sir Berkeley Moynihan (1865-1936)
Gostou ❔Nos deixe um comentário ✍️ , compartilhe em suas redes sociais e|ou mande sua dúvida pelo 💬 Chat On-line em nossa DM do Instagram.
Prof. Dr. Ozimo Gama
Cirurgião do Aparelho Digestivo
Editor Científico – The Surgeon: A Cirurgia Digestiva Atual
Engenharia de Prompt na Educação Médica
Dissecando a Nova Fronteira Tecnológica na Cirurgia Digestiva
1. A Evolução do Estetoscópio ao Algoritmo
A prática médica contemporânea atravessa uma metamorfose digital que exige mais do que a simples adaptação: exige o domínio da técnica. A ascensão dos Modelos de Linguagem Gerativa (GLMs), como o ChatGPT e o Google Bard, não representa apenas a disponibilidade de novos bancos de dados, mas sim uma mudança sísmica na síntese do conhecimento clínico. Neste contexto, a Engenharia de Prompt emerge como a competência estratégica definitiva para o médico do século XXI. Conforme definido por Heston e Khun (2023), trata-se de uma abordagem sistemática de comunicação com IAs para obter resultados de alta precisão. Não se trata de uma conversa informal, mas de uma instrumentação precisa da inteligência artificial.
Para compreendermos o “salto qualitativo” desta ferramenta, basta observar a evolução técnica: o GPT-1 (2018) operava com 117 milhões de parâmetros; o GPT-4 (2023) é estimado em 1 trilhão. Essa expansão colossal mudou o paradigma da simples busca por informação (o modelo “indexador”) para a síntese complexa de conhecimento. Para o cirurgião, isso significa que a IA deixou de ser um dicionário para se tornar um consultor de lógica, exigindo que a instrução dada pelo médico seja tão precisa quanto o plano de clivagem em uma dissecção oncológica.
Esta transição da intuição para a estrutura técnica é o que separa o uso recreativo da IA da sua aplicação acadêmica e clínica de alto nível.
2. A Anatomia de um Prompt de Alta Precisão: Estrutura e Componentes
Na sala de operação, a improvisação é o terreno do erro; na Engenharia de Prompt, a vagueza é a raiz da alucinação. Estruturar uma entrada para a IA não é meramente fazer uma pergunta, mas sim redigir um protocolo de intenção. Podemos comparar a precisão de um prompt bem construído ao rigor técnico necessário em uma colecistectomia: cada componente tem seu “tempo cirúrgico” e função específica.
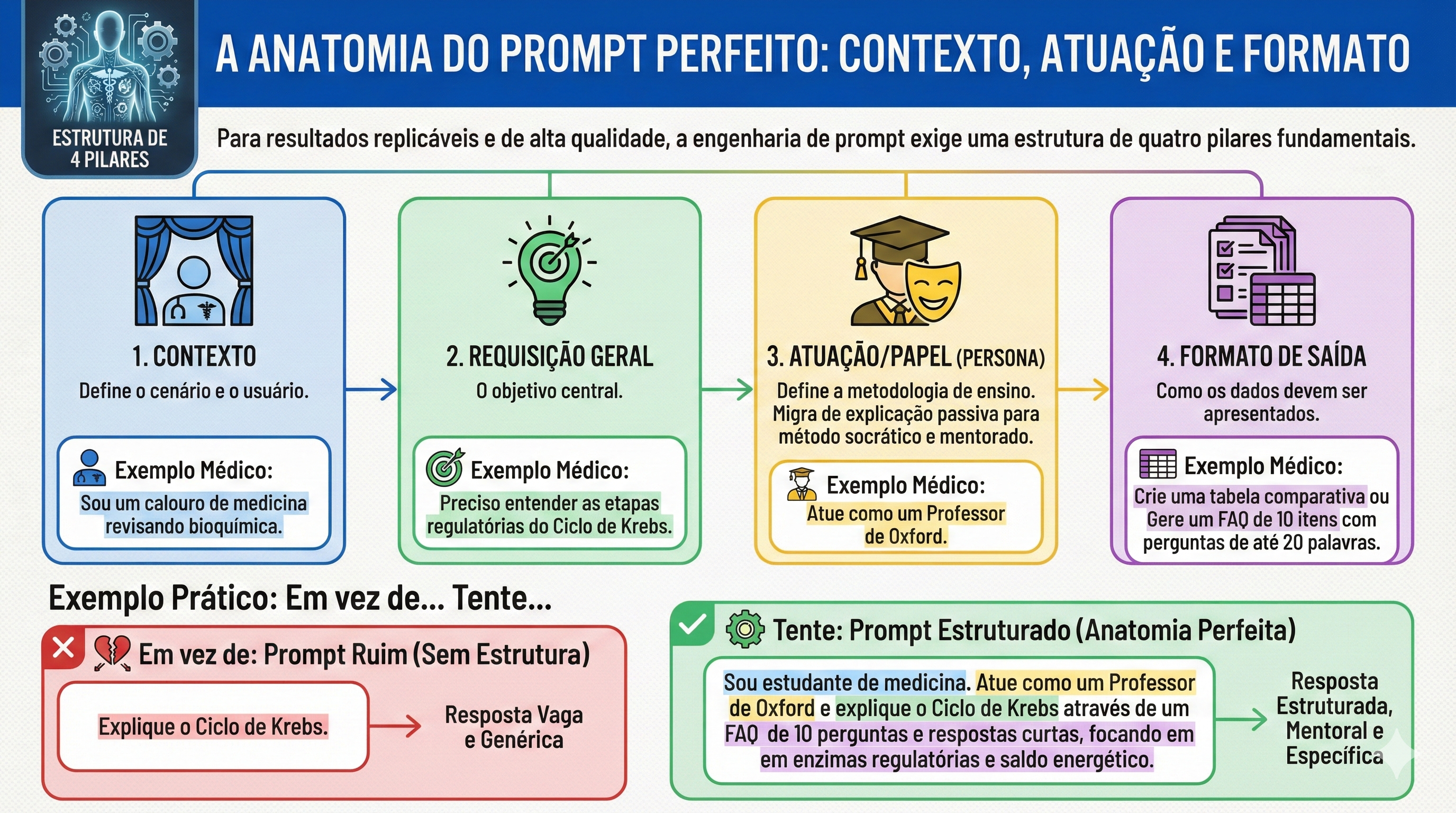
Para garantir resultados consistentes, um prompt estruturado deve conter quatro pilares fundamentais:
- Contexto: A descrição de quem está perguntando (ex: “Sou um preceptor de residência em cirurgia digestiva”).
- Solicitação Geral: O objetivo macro da interação (ex: “Necessito de uma revisão de condutas”).
- Persona/Papel: Como a IA deve se comportar (ex: “Atue como um Professor Titular de Gastroenterologia Cirúrgica”).
- Formato de Saída: A estrutura final do dado (ex: “Gere uma lista de verificação,” “tabela comparativa,” ou “resumo em tópicos”).
Comparativo de Eficiência: Prompts Vagos vs. Alta Precisão
| Tipo de Prompt | Exemplo Vago | Exemplo de Alta Precisão (Padrão Ouro) |
| Objetivo | Informação Geral | FAQ de Estadiamento Acadêmico |
| Entrada | “Fale sobre câncer gástrico.” | “Como Professor Doutor de Cirurgia, forneça um FAQ de 10 itens sobre o estadiamento do adenocarcinoma gástrico para residentes do R3. Foque no TNM 8ª edição, critérios de ressecabilidade e manejo perioperatório do paciente bariátrico. Entregue em formato de tabela.” |
| Resultado | Texto genérico e superficial. | Guia técnico, hierarquizado e pronto para discussão em round clínico. |
Essa estrutura permite que a IA realize uma triagem interna em seu vasto banco de parâmetros, ajustando o nível de complexidade para a realidade do interlocutor, seja ele um estudante de graduação ou um cirurgião experiente.
3. Níveis de Complexidade: Do Zero-Shot à Decomposição Lógica
No cotidiano acadêmico, a sofisticação da resposta da IA é diretamente proporcional à técnica de prompting utilizada. Podemos escalonar a interação em níveis que desafiam a capacidade de processamento do modelo:
- Zero-Shot vs. Few-Shot: O Zero-Shot é uma solicitação sem exemplos prévios. O Few-Shot é o fornecimento de modelos de comportamento dentro do prompt (ex: “Crie um caso clínico de isquemia mesentérica seguindo rigorosamente este modelo: [Exemplo]”).
- Hierarquia de Lawton (Níveis 1 a 4): Evoluímos de perguntas simples (Nível 1) até o Nível 4, definido como a desconstrução de solicitações complexas em componentes lógicos (Chain of Thought).
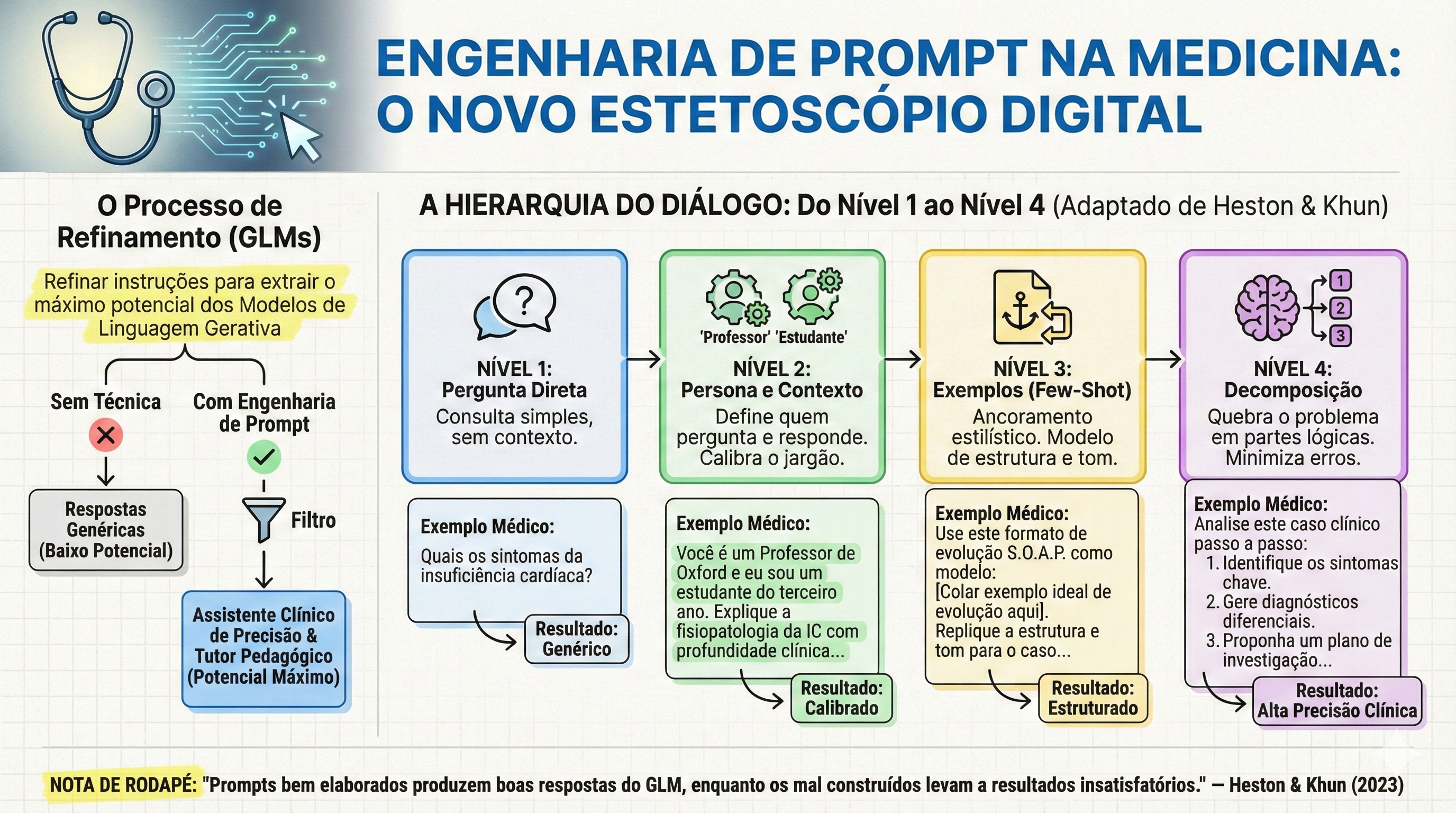
O impacto clínico mais relevante desta última técnica, ativada pelo comando “Pense passo a passo” (Think step by step), é a mitigação de erros catastróficos. Um exemplo clássico do texto de Heston e Khun (2023) ilustra isso: ao perguntar sobre um malabarista que tem 16 bolas, sendo que metade são bolas de golfe e metade das bolas de golfe são azuis, o GPT-3.0 pode falhar se responder instantaneamente. Ao ser instruído a pensar passo a passo, a IA decompõe o problema: total (16) -> metade são golfe (8) -> metade das de golfe são azuis (4). No ambiente cirúrgico, essa lógica é o que previne a iatrogenia em cálculos farmacológicos complexos ou em lógicas de estadiamento multinível.
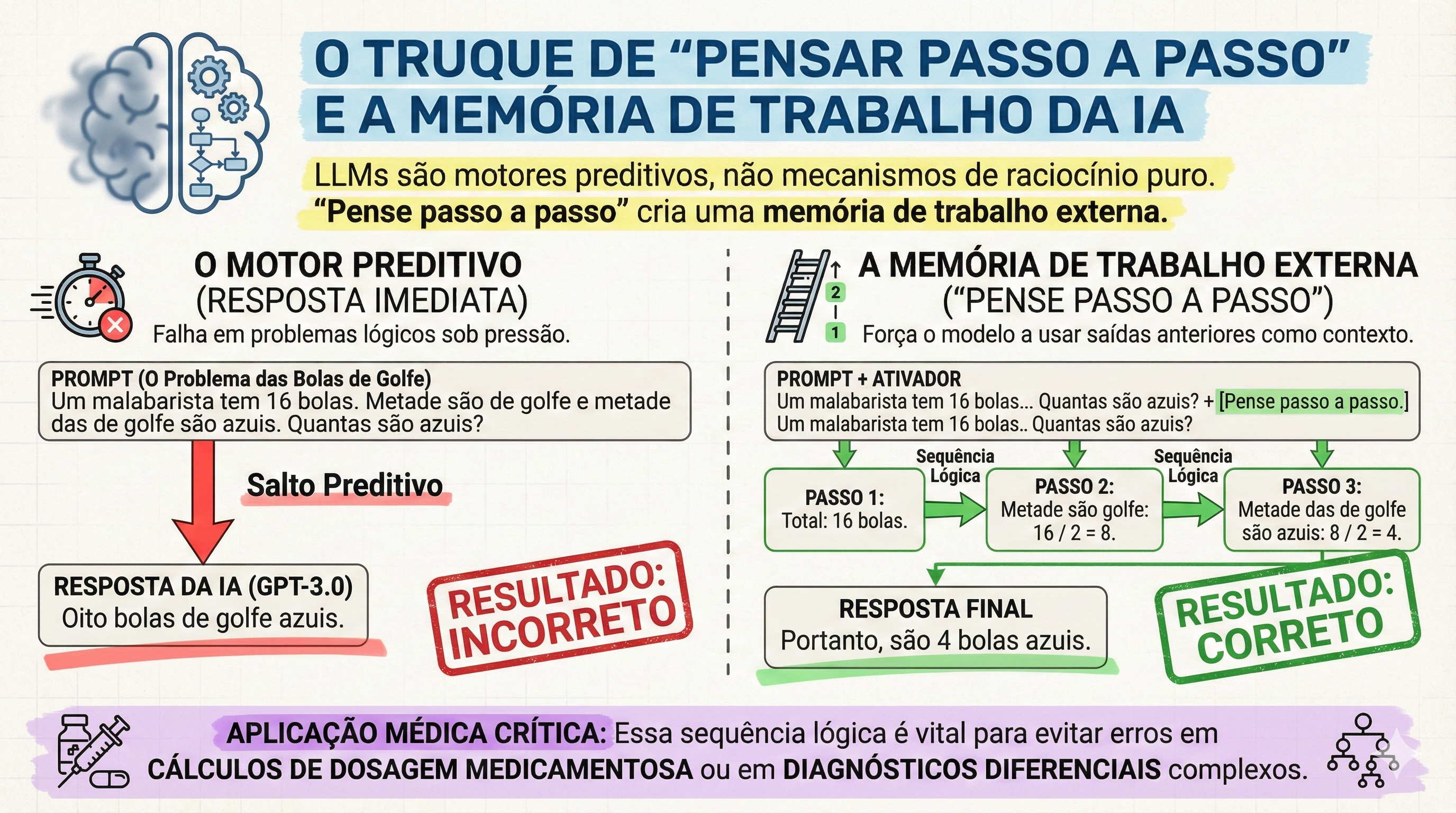
A eficácia do aprendizado, portanto, não reside em receber a resposta pronta, mas em observar o “raciocínio” da máquina, permitindo ao estudante identificar falhas lógicas e consolidar o conhecimento.
4. Aplicação no Ensino-Aprendizado e a Realidade Brasileira (Enare/Enamed)
No cenário brasileiro, marcado pela altíssima competitividade do Enare (Exame Nacional de Residência) e do Enamed, a IA deve ser encarada como um “cérebro periférico”. A densidade do conteúdo cirúrgico exige ferramentas que otimizem a densidade temporal do estudo.
Aplicações Práticas para o Estudante de Alto Desempenho:
- Mnemônicos Cirúrgicos: Criação de fórmulas personalizadas para critérios de gravidade em pancreatite aguda ou escalas de Alvarado.
- Simulação de Pacientes Realistas: Uso de GLMs para simular “Virtual Patients”, permitindo que o estudante treine a anamnese antes do contato real (conforme princípios da AAMC).
- Bancos de Questões De Novo: Geração de simulados inéditos baseados nos exames anteriores do MEC.
A realidade curricular está mudando drasticamente. Segundo dados do Curriculum SCOPE Survey (AAMC), houve um crescimento acentuado na inserção de IA nos currículos das escolas médicas entre 2023 e 2024. No Brasil, essa tendência impacta diretamente a competitividade: o candidato que domina a Engenharia de Prompt processa evidências científicas com uma agilidade que os métodos tradicionais de leitura passiva não conseguem acompanhar. Contudo, este potencial exige uma advertência: a tecnologia deve fortalecer a mente, não atrofiar o raciocínio clínico original.
5. Riscos, Alucinações e a Ética na Medicina Digital
A precisão cirúrgica exige o reconhecimento dos riscos. O maior perigo dos GLMs são as “alucinações”, onde a IA gera informações falsas com um tom de autoridade inquestionável, incluindo referências bibliográficas totalmente inventadas no formato Vancouver.
Checklist de Segurança de Dados e Integridade:
- Verificação de Citações: Jamais utilize uma referência gerada sem conferir o DOI ou a base primária.
- Privacidade: É imperativo nunca inserir dados identificáveis de pacientes reais em prompts de IA.
- Senso Crítico: O cirurgião nunca deve abdicar de sua responsabilidade ética em favor do algoritmo.
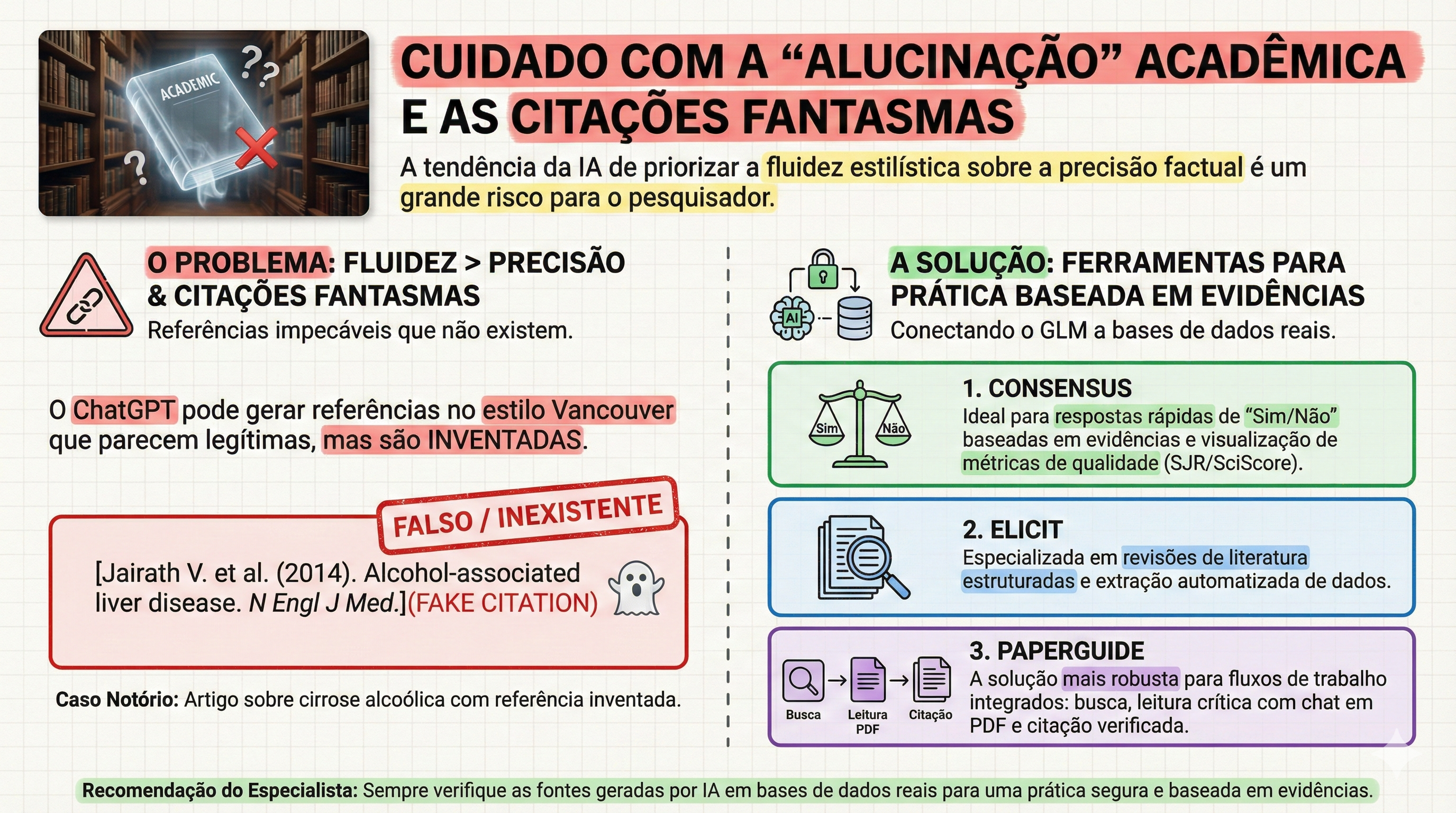
Para o fluxo de trabalho do pesquisador, é vital diferenciar as ferramentas. Modelos de chat puro (como o ChatGPT) são excelentes para síntese, mas para revisões sistemáticas, deve-se integrar ferramentas de evidência real como Elicit e Consensus. Especial destaque deve ser dado ao Paperguide: uma ferramenta “all-in-one” que, além de busca semântica, oferece suporte a múltiplos idiomas — uma vantagem estratégica para o estudante brasileiro que precisa transitar entre a literatura internacional e a prática local. O uso institucional da IA deve, portanto, ser pautado por uma cultura de ética inegociável.
6. Conclusões e Perspectivas Futuras
A Engenharia de Prompt deixará de ser um diferencial para se tornar um requisito básico, tão essencial ao cirurgião digestivo quanto o domínio da estatística básica ou do inglês técnico. Ela é a ponte entre a explosão de dados médicos e a aplicação prática à beira do leito. A mensagem central é clara: a IA deve ser utilizada para fortalecer a compreensão humana, mitigando a falha e ampliando o cuidado, sem jamais criar dependência ou o que chamamos de “pensamento fraco”. O futuro da nossa especialidade pertence àqueles que souberem interrogar a realidade — e a inteligência artificial — com a maior clareza e precisão.
#EngenhariaDePrompt #EducacaoMedica #CirurgiaDigestiva #IAnaMedicina #ResidenciaMedica
——————————————————————————–
“O sucesso da educação médica não reside apenas na transferência de fatos, mas na formação de uma mente capaz de interrogar a realidade com precisão.” — Adaptado dos princípios de William Osler
Gostou ❔ Nos deixe um comentário ✍️ , compartilhe em suas redes sociais e|ou mande sua dúvida pelo 💬 Chat On-line em nossa DM do Instagram.
A Cirurgia Digestiva Atual
Autoridade Cirúrgica
A Prerrogativa da Autoridade Cirúrgica sob a Égide da Incerteza Fiscal: Uma Reflexão sobre a Evolução do Prestígio e a Prática Contemporânea
Por: Prof. Dr. Ozimo Gama
O Conceito de Autoridade e a Evolução do Prestígio Médico
O prestígio da profissão médica, historicamente alicerçado em um modelo de prática liberal e em um paternalismo inquestionável, atravessa uma metamorfose estrutural profunda. Sob a égide da contemporaneidade, o cenário de autonomia plena foi substituído por um ambiente de pressões administrativas e incerteza fiscal. Como salientou o Dr. Jesse M. Ehrenfeld, ex-presidente da American Medical Association (AMA), a transição das práticas independentes para os sistemas corporativos é emblemática do estresse econômico enfrentado pela classe. Urge salientar que essa evolução é indissociável da realidade financeira da formação médica. Enquanto na década de 1980 — como recorda o Dr. Weigel — o custo total de quatro anos de medicina girava em torno de US32.000, o cirurgião hodierno egressa com um endividamento médio de US 246.659, podendo ultrapassar os US$ 300.000 em instituições privadas. Concomitantemente, a “Autoridade Cirúrgica” deve ser ressignificada: ela não representa mero poder hierárquico, mas uma responsabilidade derivada da expertise técnica e de um contrato de confiança renovado, essencial para a subsistência ética da especialidade.
Desafios Econômicos e a Realidade da Prática Médica
A análise da medicina atual revela uma insatisfação latente quanto à valorização profissional. Segundo o Medscape Physician Compensation Report 2025, a remuneração média subiu apenas 2,9%, acompanhando parcamente a inflação, enquanto 52% dos médicos manifestam não se sentirem compensados de forma justa. A disparidade entre gerações é notória: em 1985, a vasta maioria dos médicos era proprietária de seu próprio negócio, gerindo equipes e processos. Hoje, o cirurgião é, majoritariamente, um elo em grandes sistemas de saúde, onde a autonomia administrativa é mitigada por métricas corporativas. Os principais vetores de estresse e erosão do prestígio incluem:
• Incerteza Fiscal e Econômica: Oscilações que dificultam o planejamento de carreira a longo prazo.
• Cortes Estatutários de Pagamento: Reduções em sistemas de reembolso (como o Medicare) que não acompanham a complexidade dos atos.
• Burocracia Administrativa e Custos Operacionais: Uma carga intrusiva que desvia o cirurgião de sua atividade fim, exacerbada pelo aumento constante dos custos de manutenção das práticas.
A Autoridade na Cirurgia do Aparelho Digestivo: Expertise e Autonomia
Dentro da hierarquia nosocomial, a Cirurgia do Aparelho Digestivo preserva um “clout” (influência política e social) diferenciado. No entanto, é necessário compreender que esse poder político, como observa Barnett, está profundamente enraizado em um sistema de reembolso não baseado estritamente na saúde da população, mas na valorização de procedimentos de alta complexidade que geram receita crítica para os sistemas hospitalares. A fundamentação da autoridade do cirurgião repousa sobre sua “expertise esotérica”. Jenkins, em suas pesquisas, demonstrou que cirurgiões que operam neonatos de 500g ou realizam duodenopancreatectomias complexas desfrutam de um nível de confiança pública superior. Diferente do pediatra geral, que muitas vezes enfrenta questionamentos constantes sobre condutas rotineiras — como a segurança de vacinas —, o cirurgião digestivo lida com situações de risco vital onde as decisões são técnicas e imediatas. Essa especificidade confere maior autonomia organizacional e confiança do paciente, resultando em um paradoxo interessante: embora o cirurgião trabalhe mais horas e em maior intensidade, os índices de burnout tendem a ser menores do que em especialidades menos procedimentais. A valorização social e a percepção de utilidade crítica atuam como um escudo psicossocial para o especialista.
A Nova Configuração do Contrato Médico-Paciente
O declínio do modelo “Marcus Welby” de paternalismo médico deu lugar a uma era de consumismo em saúde e ceticismo científico, exacerbada pela democratização desenfreada da informação via internet. O contrato médico, outrora um pacto sagrado entre indivíduos, foi reescrito pela burocracia e pelo big business. A autoridade contemporânea deve, portanto, acolher a diversidade e a inclusão como pilares de sua legitimidade. O prestígio moderno não se mede mais pela deferência cega, mas pela busca de equilíbrio, sustentabilidade e autopreservação do profissional.
Aplicação na Prática e Pontos-Chave
No cenário brasileiro, o desafio é análogo. O endividamento do recém-formado em instituições privadas pode variar entre R500.000 e R 800.000, criando uma pressão financeira imediata. Com aproximadamente 5.000 especialistas titulados em Cirurgia do Aparelho Digestivo, enfrentamos uma severa saturação nos grandes centros, o que demanda uma gestão de carreira mais estratégica e técnica.
Pontos-Chave para o Residente e Pós-Graduando:
• Expertise Técnica: O domínio de procedimentos complexos e de alto risco é o fundamento de sua soberania clínica e influência hospitalar.
• Gestão da Autonomia: É imperativo aprender a navegar em sistemas corporativos preservando a integridade da decisão médica frente às pressões administrativas.
• Relação de Confiança: Substitua o paternalismo obsoleto por uma transparência baseada na erudição técnica, gerenciando as expectativas do paciente-consumidor.
• Sustentabilidade da Carreira: A longevidade profissional depende de uma prática que valorize a autopreservação e o equilíbrio ético-financeiro.
Em última análise, a missão do cirurgião permanece como um chamado de serviço. Devemos retomar a visão de Weigel, sentindo-nos como “pastores de nosso rebanho”, responsáveis diretos por vidas que nos são confiadas em momentos de extrema vulnerabilidade. A medicina evoluiu, e o prestígio agora exige mais do que títulos; exige resiliência e adaptação. Como preconizou Theodor Billroth, mestre da cirurgia digestiva:
“O cirurgião deve ter o coração de um leão e as mãos de uma dama.”
A autoridade reside, precisamente, na virtude de equilibrar a força da decisão técnica com a delicadeza do compromisso ético.
The Surgeon – A Cirurgia Digestiva Atual – Et Fortior
Gostou ❔Nos deixe um comentário ✍️ , compartilhe em suas redes sociais e|ou mande sua dúvida pelo 💬 Chat On-line em nossa DM do Instagram.
#CirurgiaDigestiva #ResidenciaMedica #AutoridadeCirurgica #EducaçãoMédica #TheSurgeon
Estilo e Brio Cirúrgico
A Ciência da Comunicação Não Verbal na Liderança Cirúrgica
1. A Ontologia do Brio no Bloco Operatório
No teatro de alta complexidade que caracteriza a cirurgia do aparelho digestivo, a excelência técnica, embora imperativa, é apenas o estrato basal da competência. O que verdadeiramente distingue o mestre do técnico é o “Surgical Panache” — ou brio cirúrgico. Longe de ser um adereço estético, o brio é uma competência transformadora fundamentada na ciência da comunicação não verbal. A literatura contemporânea em liderança cirúrgica e comportamento organizacional sublinha que os seres humanos possuem um imperativo biológico para processar mensagens não verbais com extrema celeridade, realizando julgamentos sociais eficientes antes mesmo da primeira incisão. A eficácia de um líder depende da congruência: o alinhamento absoluto entre o rigor do discurso técnico e a presença executiva. É fundamental desmistificar a interpretação vulgar do modelo de Mehrabian: embora as palavras sejam o veículo das instruções técnicas, o canal não verbal domina 93% do clima emocional e da percepção de confiança da equipe. Sem essa harmonia, a confiança organizacional se dissolve, e a comunicação ineficaz manifesta-se não como um erro acessório, mas como uma complicação clínica gravíssima.
2. A Dualidade da Liderança: Receptividade e Formidabilidade
A mobilização do contingente humano em procedimentos complexos exige o domínio da teoria dos sinais de status, conforme a estrutura de Keating. O cirurgião deve projetar uma imagem binária que ative simultaneamente dois sistemas motivacionais na equipe:
• Receptividade (Calor e Atratividade): Sinaliza abertura e convite à colaboração (sistema de approach). É a vertente que garante a segurança psicológica, permitindo que um instrumentador ou anestesista comunique intercorrências sem temor de retaliação.
• Formidabilidade (Competência e Poder): Transmite agência, autoridade e domínio técnico (sistema de avoidance). É a projeção de distância profissional necessária para manter a hierarquia e o rigor em momentos críticos.
O carisma cirúrgico reside na capacidade de transitar entre esses sinais duplos. Um líder puramente formidável silencia a equipe; um líder exclusivamente receptivo compromete o tempo operatório. A maestria está em ser, simultaneamente, um porto seguro e uma autoridade inquestionável.
3. Kinésica e Oculésica: A Arquitetura da Autoridade e Espaço
A taxonomia dos sinais não verbais oferece diretrizes práticas para o refinamento da postura operatória:
• Kinésica (Postura e Gestual): A adoção de posturas expansivas comunica controle. De acordo com o estudo de Holler e Beatie, o uso de gestos intencionais e fluidos aumenta o valor da mensagem falada em 60%. Deve-se eliminar comportamentos nervosos (fidgeting), que corroem a credibilidade.
• Oculésica (O Olhar): O olhar é o regulador supremo da interação. Aplico rigorosamente a regra de manter contato visual durante 50% do tempo ao falar e 70% ao ouvir. Isso estabelece persuasão e engajamento, permitindo “ler o ar” da sala.
• Vocalização (Vocalics): A gestão paralinguística é vital. Em uma intercorrência hemorrágica durante uma duodenopancreatectomia, o cirurgião deve contra-atacar a sobrecarga do sistema nervoso simpático da equipe através de uma voz de tom grave, volume controlado e ritmo pausado. A calma do líder deve ser auditível para ser contagiante.
4. Aplicação na Cirurgia Digestiva e a Realidade Brasileira
A segurança do paciente é o objetivo teleológico de toda comunicação. Estatísticas globais revelam que 86% das falhas no ambiente de trabalho são atribuídas à comunicação ineficaz. Na cirurgia do aparelho digestivo, onde procedimentos como esofagectomias demandam sincronia absoluta, esse dado é alarmante. No contexto brasileiro, classificado como uma cultura de alto contexto (High-Context), a habilidade de interpretar pistas sutis e nuanças não verbais é ainda mais vital do que em ambientes anglo-saxões ou germânicos. No Brasil, a liderança é exercida através do relacionamento e da percepção de brio; o silêncio de um assistente pode significar uma dúvida técnica que o cirurgião deve ser capaz de decifrar visualmente. Ademais, a educação médica continuada em 2026 exige o domínio da “presença digital”. Em boards clínicos virtuais, a Chronemics (gestão do tempo) e a pontualidade tornaram-se indicadores de prioridade organizacional. O enquadramento da câmera deve ser preciso, mantendo o olhar na lente e as mãos visíveis para preservar a transparência e a autoridade virtual.
5. Pontos-Chave para a Prática do Cirurgião Digestivo
Para os alunos, residentes e pós-graduandos sob minha orientação, estabeleço as seguintes prerrogativas:
1. Domínio do Quadro: “Seja dono da sala”. Use posturas expansivas e movimentos deliberados para sinalizar que o ambiente está sob controle técnico e emocional.
2. Estratégia Dual: Não busque ser apenas amado ou apenas temido. Seja formidável na competência e receptivo na colaboração.
3. Monitoramento Ativo: Realize a “análise muda” de suas performances. Assista a vídeos de suas cirurgias sem áudio para identificar vícios gestuais e falhas de congruência.
4. Inteligência Cultural: Adapte sua comunicação ao estrato da equipe. Em culturas de alto contexto, o brio cirúrgico é o que preenche as lacunas do que não foi dito, mas precisa ser compreendido.
6. O Cirurgião como Líder Corporificado
O brio não é um dom estático, mas uma disciplina dinâmica refinada pela autoconsciência e pelo rigor. Projetar uma presença física autêntica, confiante e empática é o diferencial definitivo para a liderança de alto impacto. O cirurgião que negligencia sua comunicação não verbal é apenas um executor de técnicas; o cirurgião que domina seu brio é um comandante de destinos, capaz de tratar a falha de comunicação com o mesmo rigor científico com que trata uma fístula anastomótica.
——————————————————————————–
“O cirurgião deve ter mãos de dama, olhos de águia e coração de leão; contudo, é a sua presença que confere à equipe a têmpera necessária para a vitória sobre a patologia.” — Baseado no legado de William Stewart Halsted
Gostou ❔ Nos deixe um comentário ✍️ , compartilhe em suas redes sociais e|ou mande sua dúvida pelo 💬 Chat On-line em nossa DM do Instagram.
The Surgeon A Cirurgia Digestiva Atual Et Fortior
#CirurgiaDigestiva #BrioCirurgico #LiderançaMedica #EducacaoMedica #TheSurgeon
Segurança em Foco
A Evolução da Cultura de Segurança e o Desafio da Burocratização na Cirurgia do Aparelho Digestivo
1. A Gênese do Risco na Medicina e Cirurgia
A gênese da prática cirúrgica moderna está intrinsecamente vinculada a uma audácia que, aos olhos contemporâneos, beira a temeridade. Em seus primórdios, a medicina não dispunha de comitês de ética, protocolos de conduta ou salvaguardas administrativas; o progresso era esculpido em tempo real, frequentemente à beira do leito e sob um custo humano excruciante. A introdução de tecnologias disruptivas como o éter e o clorofórmio exemplifica essa tensão dialética: embora tenham viabilizado a revolução do ato operatório, enfrentaram resistências ferrenhas sob o pretexto de serem substâncias perigosas e incontroláveis. Esse padrão de rejeição institucional repetiu-se com Ignaz Semmelweis, cuja demonstração empírica da eficácia da higiene das mãos foi ignorada por desafiar identidades profissionais e normas vigentes. Aquela era, magistralmente retratada na série The Knick, exibe uma medicina criativa e heróica, porém caótica e, por vezes, deletéria. Aprendemos, por meio de um processo histórico doloroso, que a inovação desmedida gera danos, mas reconhecemos que, naquele período de obscuridade técnica, a assunção do risco era o único vetor possível para o avanço da ciência.
2. O Surgimento da Segurança como Bússola Moral
Como resposta necessária ao caos da era heróica, a segurança emergiu como a bússola moral da medicina do século XX. A transição para a era da padronização e dos protocolos buscou transformar a arte cirúrgica em uma ciência de alta confiabilidade. O advento do Checklist Cirúrgico consolidou-se como o marco definitivo desta evolução, mitigando erros catastróficos, como intervenções em locais incorretos, e reduzindo drasticamente as complicações evitáveis. A segurança estabeleceu-se como nossa âncora ética sob o aforismo Primum non nocere. Contudo, observamos hoje que este preceito tem sido distorcido: em vez de guiar a prudência clínica, é frequentemente invocado para justificar a inação diante de riscos calculados e necessários. A medicina não deve ser a busca utópica pela anulação do risco a qualquer custo, mas sim o sopesamento rigoroso entre danos e benefícios, sempre pautado pela soberania dos valores do paciente.
3. Quando a Segurança se Torna Burocracia
Assistimos, na atualidade, a uma patologia sistêmica de ordem administrativa: a “fossilização” da segurança em estruturas burocráticas estáticas. O que deveria proteger o paciente transmutou-se em mecanismos de proteção institucional e conformidade legal. Um sintoma alarmante dessa realidade foi o caso de um residente sênior norte-americano que, a seis meses de sua graduação, jamais havia realizado uma drenagem de tórax de forma autônoma — um reflexo direto de sistemas que priorizam a ausência de intercorrências administrativas em detrimento da formação de competência técnica real. No cenário brasileiro, essa estagnação é agravada por infraestruturas hospitalares rígidas e prontuários eletrônicos (EHRs) deficientes, que impõem as seguintes consequências:
• Dreno de Intelecto: Residentes de Cirurgia do Aparelho Digestivo e de Terapia Intensiva gastam, em média, 50% de sua jornada diária em tarefas clericais e documentação redundante, sacrificando o raciocínio clínico e o treinamento em técnica cirúrgica.
• Engessamento da Pesquisa: Processos de governança para estudos de baixo risco podem levar meses ou anos para aprovação, priorizando a prevenção de riscos hipotéticos sobre o aprendizado derivado de pacientes reais.
• Desvio de Finalidade: A documentação clínica passou a servir mais ao faturamento e à auditoria do que à comunicação entre a equipe e ao cuidado direto.
4. O “Stress Test” da Inteligência Artificial (IA) na Prática Cirúrgica
A Inteligência Artificial atua hoje como um teste de estresse que revela as falhas de governança do nosso sistema de saúde. A barreira para a adoção da IA não é de ordem técnica, mas sim uma incapacidade de adaptação das instâncias decisórias. O paradoxo é flagrante: algoritmos de IA são prontamente implementados quando o objetivo é otimizar códigos de faturamento e captura de receita. No entanto, ferramentas de IA como escribas clínicos, que reduzem a carga documental, ou sistemas de suporte ao raciocínio clínico e triagem de imagens, enfrentam barreiras instransponíveis sob o pretexto da privacidade — ainda que sejam mais seguros do que os “atalhos” improvisados por cirurgiões em seus dispositivos pessoais para contornar sistemas hospitalares obsoletos. A resistência atual é uma falha de governança disfarçada de segurança do paciente.
5. Aplicação Prática na Cirurgia Digestiva
Para o cirurgião do aparelho digestivo em formação, o conceito de “Custo do Atraso” deve ser central. Estatísticas demonstram que, em média, transcorrem 14 anos para que uma evidência científica consolidada chegue efetivamente ao leito do paciente. Para um residente que inicia sua trajetória hoje, esse hiato significa que ele poderá estar na metade de sua carreira antes de dominar as inovações que já estão disponíveis agora. É imperativo compreender que a inação não é um porto seguro; ela possui consequências invisíveis, mas mensuráveis. A espera por uma segurança absoluta e estática é, em si, uma forma de dano. Na residência médica e na pós-graduação, a inovação tecnológica deve ser integrada não como um acessório, mas como um pilar da segurança do paciente e da eficiência clínica.
6. Pontos-Chave para o Residente e Pós-Graduando
1. A segurança deve ser adaptativa, não estática: Protocolos que não evoluem com a tecnologia tornam-se obstáculos ao exercício da excelência cirúrgica.
2. Inação também gera dano: O perigo invisível da espera e o atraso na adoção de novas técnicas são formas reais de prejuízo ao paciente.
3. O cirurgião como avaliador e tradutor: O cirurgião não é um usuário passivo, mas um filtro crítico que absorve incertezas para que o sistema de saúde possa aprender e evoluir com segurança.
7. Perspectivas Futuras
A segurança que não evolui torna-se, inexoravelmente, insegura. O desafio da Cirurgia Digestiva contemporânea é resgatar a coragem intelectual de nossos predecessores, temperada pelo rigor científico atual. Devemos atuar como early adopters responsáveis, integrando novas ferramentas de forma monitorada e contínua. A tradição, que outrora serviu para proteger o enfermo, não pode ser reduzida a um mecanismo que protege as instituições contra a mudança. Somente através de uma cultura de aprendizado contínuo e da superação da burocracia fóssil poderemos assegurar que a próxima geração de cirurgiões esteja plenamente capacitada para os desafios de sua era.
Como bem asseverou Lord Lister, o mestre da antissepsia: “O sucesso de uma operação depende da atenção cuidadosa a cada detalhe.” Que essa atenção aos detalhes transcenda o campo operatório e alcance a gestão crítica da tecnologia e dos sistemas que regem nossa profissão. O zelo pelo paciente exige, agora mais do que nunca, zelo pela evolução do sistema.
Gostou ❔Nos deixe um comentário ✍️ , compartilhe em suas redes sociais e|ou mande sua dúvida pelo 💬 Chat On-line em nossa DM do Instagram.
The Surgeon A Cirurgia Digestiva Atual Et Fortior
#CirurgiaDigestiva #SegurancaDoPaciente #EducacaoMedica #IAnaMedicina #ResidenciaMedica
A Revolução da Inteligência Artificial no Aprendizado e na Pesquisa em Cirurgia do Aparelho Digestivo
1. O Novo Paradigma da Educação Médica
A evolução da Inteligência Artificial (IA) no seio da medicina contemporânea transcendeu a mera aplicação subsidiária em diagnósticos por imagem para consolidar-se como um pilar epistemológico na pesquisa e no aprendizado. O cirurgião moderno defronta-se com um desafio multifacetado, por vezes sísifo: a imperiosa necessidade de conciliar uma extenuante carga operatória com a produção científica de alto impacto e a gestão de um volume oceânico de literatura especializada. Neste cenário, a Inteligência Artificial Generativa (GenAI) e os Modelos de Linguagem de Grande Escala (LLMs) emergem não como substitutos do intelecto, mas como catalisadores de um fluxo de trabalho otimizado. É fundamental compreendermos que a maestria cirúrgica hoje exige, além da destreza manual, a competência digital para navegar nesta nova fronteira tecnológica com idoneidade e rigor acadêmico.
2. Ferramentas de IA e Categorização Funcional
A fundamentação científica para a adoção dessas tecnologias repousa em evidências recentes e robustas. O estudo seminal de Valencia-Coronel et al. (2026) realizou uma avaliação qualitativa rigorosa de 43 plataformas de IA, fornecendo um arcabouço para a seleção criteriosa de ferramentas no pipeline da pesquisa cirúrgica.
Dentre as categorias funcionais identificadas, destacam-se:
• Mecanismos de Busca Acadêmica: Superando os buscadores genéricos, plataformas como Consensus AI, Elicit e EvidenceHunt focam na síntese de evidências baseadas em revisão por pares. Ressalto a relevância do Manus AI, projetado especificamente para lidar com tópicos cirúrgicos complexos e desfechos heterogêneos, auxiliando inclusive na estruturação de protocolos e tabelas prontas para publicação.
• Interação com Documentos: Ferramentas como AskYourPDF e ChatPDF permitem um diálogo heurístico com manuscritos complexos, facilitando a extração de dados técnicos e a análise metodológica profunda.
• Análise de Literatura: A visualização de redes de citações através de algoritmos (ex: Connected Papers e Litmaps) permite mapear a trajetória de um tema e identificar conexões semânticas fundamentais.
• Assistentes de Escrita e Síntese: Modelos como ChatGPT (em sua versão GPT-4) e ClaudeAI auxiliam na estruturação de rascunhos. Para sínteses profundas, o modo “Deep Research” do Perplexity AI destaca-se por realizar varreduras exaustivas em múltiplos repositórios. No design, o Napkin AI converte conceitos complexos em diagramas técnicos precisos.
O ganho de eficiência é estatisticamente substancial. Conforme demonstrado no estudo de Trad et al. (2024), a aplicação de fluxos baseados em LLM reduziu o tempo de triagem em revisões sistemáticas de 564,4 para 25,5 horas. Mais relevante que a celeridade é a precisão: o estudo reportou um índice de falso-negativo de 0% e uma especificidade de 99,6%, superando o crivo humano em termos de consistência.
3. Aplicação Prática na Cirurgia do Aparelho Digestivo
Para o residente ou o pós-graduando em Cirurgia do Aparelho Digestivo, a integração destas ferramentas deve ser metódica. Imaginemos o preparo para um Journal Club: o acadêmico pode utilizar o Consensus AI para identificar o estado da arte sobre uma técnica de anastomose, empregar o Litmaps para visualizar a rede de citações do ensaio clínico seminal e, finalmente, interpelar a metodologia do artigo através do ChatPDF para identificar possíveis vieses.
O fluxo de trabalho idealizado integra ciclicamente: (1) Busca em mecanismos especializados; (2) Interação conversacional com documentos para extração de dados; (3) Análise de redes de citações para contextualização histórica; (4) Escrita assistida por modelos generativos e (5) Design gráfico para comunicação visual dos resultados.
4. O Papel da Supervisão Humana
Embora a tecnologia seja fascinante, o rigor acadêmico nos impõe cautela. Devemos atentar para o conceito de “débito cognitivo”. Pesquisas conduzidas por Kosmyna et al. (2024) revelam que a dependência excessiva e exclusiva de IAs reduz o engajamento neural e a retenção de conteúdo. Em contrapartida, a sequência “cérebro primeiro, IA depois” — em que a conceituação inicial e o esboço partem do cirurgião — resulta em um aumento de 50% a 200% na conectividade neural através de bandas de EEG, preservando a capacidade de recordação e o pensamento crítico.
No âmbito ético, as diretrizes de entidades como ICMJE, COPE e WAME são peremptórias:
1. Veto à Autoria: Sistemas de IA não possuem personalidade jurídica ou intelectual para figurar como autores.
2. Transparência Radical: Todo uso de GenAI deve ser declarado explicitamente na seção de Métodos ou Agradecimentos.
3. Auditoria e Registros: Seguindo as orientações da JAMA Network, o pesquisador deve manter um registro de todos os prompts (comandos) relevantes utilizados, para fins de auditoria ética e científica.
A IA jamais substituirá o julgamento clínico soberano ou a responsabilidade ética do cirurgião sobre o dado publicado.
BOX DE DESTAQUE: ESSENCIAL PARA A PRÁTICA ACADÊMICA
• Eficiência Paradigmática: Redução drástica no tempo de triagem bibliográfica com precisão cirúrgica (0% de falso-negativos).
• Rigor Científico: Obrigatoriedade de verificação manual das referências para mitigar “alucinações” do modelo.
• Metodologia “Brain-First”: Priorizar a reflexão intelectual antes da assistência tecnológica para evitar o débito cognitivo.
• Ética e Transparência: Registro de prompts e declaração formal do uso de ferramentas conforme diretrizes internacionais.
6. Conclusões Aplicadas à Prática
A Inteligência Artificial é um catalisador de produtividade sem precedentes na história da medicina. Contudo, o cirurgião deve permanecer como o árbitro final da precisão científica. O futuro da educação médica continuada no Brasil exige o desenvolvimento de habilidades digitais que permitam ao médico não apenas consumir tecnologia, mas governá-la sob a égide do rigor científico. Dominar estas ferramentas é, hoje, um requisito para a excelência acadêmica e clínica.
“O cirurgião que conhece apenas a técnica é um artesão; o que domina a ciência por trás dela é um mestre. A IA é nossa nova ferramenta de maestria.”
Gostou? ❔ Nos deixe um comentário ✍️ , compartilhe em suas redes sociais e/ou mande sua dúvida pelo 💬 Chat On-line em nossa DM do Instagram.
——————————————————————————–
Palavras-chave: Inteligência Artificial na Cirurgia, Educação Médica, Cirurgia do Aparelho Digestivo, Pesquisa Cirúrgica, LLMs na Medicina, Residência Médica.
Hashtags: #CirurgiaDigestiva #InteligenciaArtificial #MedicinaAcademica #TheSurgeon #EducacaoMedica
PROF. DR. OZIMO GAMA
The Surgeon
A Cirurgia Digestiva Atual
Et Fortior
A Origem da Cirurgia Abdominal
A História da Primeira Laparotomia de Sucesso

1.0 Um Olhar Sobre o Abismo do Passado Cirúrgico
Hoje, um cirurgião pode remover um grande tumor ovariano em um procedimento seguro, utilizando um eletrocautério para uma cirurgia sem sangue e clipes de plástico para ligar os vasos. É um feito notável, mas que se torna assombroso quando contrastado com a brutal realidade cirúrgica de 1809. Naquele mundo, o interior do abdômen era um santuário inviolável. O que aconteceu na cidade fronteiriça de Danville, Kentucky, não foi uma evolução, mas uma metamorfose. Foi, nas palavras de Shakespeare, “a sea change into something rich and strange” — uma transformação profunda e maravilhosa.
Voltemos a esse tempo. Não existia anestesia — o éter só seria usado 33 anos depois. Os princípios da antissepsia de Joseph Lister só surgiriam em 1865. Transfusões de sangue eram algo para mais de um século no futuro, e a penicilina de Alexander Fleming só seria descoberta em 1928. Qualquer tentativa de abrir a cavidade abdominal era considerada uma sentença de morte.
Foi neste cenário desolador que um cirurgião visionário, Dr. Ephraim McDowell, e uma paciente de coragem extraordinária, Jane Todd Crawford, se uniram para realizar o impossível. Juntos, eles conduziram um “experimento” que não apenas salvou uma vida, mas fundou a cirurgia abdominal. Esta é a crônica desse evento marcante — uma lição fundamental de inovação, diagnóstico e coragem para todos os estudantes e cirurgiões contemporâneos.
2.0 A Crônica de um Milagre Cirúrgico
2.1 O Cenário Cirúrgico do Século XIX: O Dogma da Peritonite Fatal
No início do século XIX, a comunidade médica, especialmente a europeia, operava sob um dogma inabalável: qualquer violação da cavidade peritoneal resultaria invariavelmente em peritonite e morte. Cirurgiões renomados, como o anatomista escocês William Hunter, consideravam a remoção de ovários uma prática incurável e perigosa. Desafiar essa crença não exigia uma evolução do pensamento, mas uma completa revolução. Apesar do medo paralisante, a ideia já havia sido aventada. John Bell, professor de McDowell e um dos cirurgiões mais famosos da Europa, havia falado sobre a possibilidade teórica de tal operação em suas aulas, embora nunca tenha ousado tentar realizá-la. O abismo entre a teoria e a prática era, até então, intransponível.
2.2 Os Protagonistas: Um Cirurgião Visionário e uma Paciente de Coragem Extraordinária
Dr. Ephraim McDowell: Nascido em 1771, McDowell era um cirurgião competente e respeitado na fronteira americana. Sua formação incluiu um aprendizado com o Dr. Alexander Humphreys e estudos na Universidade de Edimburgo, onde foi influenciado por John Bell. Ao retornar para Danville, estabeleceu uma reputação por realizar cirurgias complexas para a época, como a remoção de cálculos vesicais de 23 pacientes sem uma única fatalidade. Um desses pacientes foi um jovem chamado James K. Polk, que mais tarde se tornaria o 11º presidente dos Estados Unidos.

Jane Todd Crawford: Nascida em 1763, Jane era uma mulher de 45 anos, mãe de quatro filhos, que vivia em uma cabana de toras a 60 milhas (quase 100 km) de Danville. Por meses, ela sofreu com um inchaço abdominal persistente e enorme. Seus médicos locais, perplexos, diagnosticaram-na erroneamente como estando em uma gravidez gemelar que já havia passado do tempo. Sua coragem e fortitude seriam postas à prova de uma forma que ninguém poderia imaginar.
2.3 O Diagnóstico e a Decisão Audaciosa
Em 13 de dezembro de 1809, McDowell cavalgou até a casa de Crawford. Seu relato do encontro demonstra uma impressionante acuidade clínica. Ele escreveu:
“Ao exame, per vaginam, não encontrei nada no útero, o que me induziu à conclusão de que deveria ser um ovarium aumentado.”
Sem nenhuma tecnologia, apenas com seu conhecimento de anatomia e o exame físico, McDowell descartou a gravidez e diagnosticou corretamente um tumor ovariano gigante. O passo seguinte foi ainda mais notável. Em um dos primeiros exemplos de consentimento informado, ele explicou a Crawford sua perigosa situação e que a única chance, uma operação, seria um “experimento” nunca antes realizado com sucesso. Ele prometeu tentar se ela estivesse disposta a ir até sua casa em Danville.
A resposta de Jane Todd Crawford foi um ato de coragem monumental. Durante o rigoroso inverno do Kentucky, ela viajou as 60 milhas a cavalo, uma jornada de vários dias, equilibrando o enorme tumor sobre a sela de seu cavalo para se submeter a um procedimento que muito provavelmente a mataria.
2.4 A Operação: Um Marco na História em 25 de Dezembro de 1809
No dia de Natal de 1809, em um quarto no andar de cima da casa de McDowell, a cirurgia foi realizada. Não havia anestesia; a mesa de operação era uma mesa comum de madeira. Para se acalmar durante o procedimento de 25 minutos, Jane Todd Crawford recitava salmos e cantava hinos. A cena, conforme descrita por McDowell, desafia a imaginação moderna. Ele realizou uma incisão de 9 polegadas no lado esquerdo do abdômen, realizando a primeira laparotomia eletiva da história. Com a súbita liberação da pressão, os intestinos “correram para fora sobre a mesa”. Preenchido pelo tumor, o abdômen não podia contê-los. As alças intestinais, segundo o próprio McDowell, “permaneceram de fora por cerca de vinte minutos e, sendo dia de Natal, ficaram tão frias” que ele precisou lavá-las com água morna antes de recolocá-las. Em meio a esse caos controlado, ele passou uma ligadura forte na trompa de Falópio, incisou o tumor, removeu 15 libras de “substância gelatinosa suja” e, em seguida, o saco tumoral de 7,5 libras. Finalmente, fechou a incisão com sutura interrompida, deixando a ponta da ligadura para fora. A recuperação de Crawford foi tão milagrosa quanto a cirurgia. Cinco dias depois, McDowell a encontrou “fazendo sua cama”. Em 25 dias, ela estava saudável o suficiente para fazer a viagem de 60 milhas de volta para casa, novamente a cavalo. Jane Todd Crawford viveu por mais 33 anos, superando seu cirurgião em 12 anos.

2.5 Publicação e Reconhecimento Tardio
Com modéstia, McDowell só publicou seu feito em 1817, no Eclectic Repertory and Analytical Review, após realizar com sucesso mais duas operações semelhantes. A reação da comunidade médica europeia foi de ceticismo e desprezo. James Johnson, editor do influente London Medico-Chirurgical Review, expressou sua incredulidade com um desdém mordaz: “Credat Judoeus, non ego” (Conte isso a outra pessoa, não a mim). Anos depois, ao relutantemente aceitar o feito, sua retratação revelou o preconceito geográfico e racial que McDowell enfrentava: “…todas as mulheres operadas no Kentucky, exceto uma, eram negras, e como essas pessoas suportam cortes com quase, se não total, impunidade como cães e coelhos, nossa admiração diminui…”. O reconhecimento de McDowell como o “Pai da Cirurgia Abdominal” veio postumamente, em grande parte devido aos esforços do Dr. Samuel D. Gross.
3.0 Aplicação e Legado para a Cirurgia Digestiva
Qual a importância deste evento para nós, cirurgiões do aparelho digestivo? A resposta é simples e profunda: tudo. O feito de McDowell foi a refutação prática e definitiva do dogma de que a cavidade peritoneal era intocável. Sua coragem não criou apenas um novo procedimento; ela criou a possibilidade de toda a nossa especialidade. A cirurgia de estômago, fígado, pâncreas e intestino simplesmente não existiria sem aquele primeiro passo revolucionário. É crucial também clarificar a terminologia. O procedimento não foi uma “ovariotomia” — termo que tecnicamente significa apenas incisar o ovário. O que McDowell realizou foi uma laparotomia (a abertura da cavidade abdominal) com uma salpingo-ooforectomia (a extração do ovário e da trompa de Falópio). Usar o termo impreciso diminui a magnitude de seu feito, que não foi apenas remover um órgão, mas sim invadir e manejar com sucesso o santuário proibido do abdômen. A ousadia de McDowell ressoa em sua própria voz, vinte anos depois do evento, em uma carta de 1829:
“Portanto, parece-me uma mera bobagem sobre o perigo da inflamação peritoneal tão falada pela maioria dos cirurgiões.”
4.0 Pontos-Chave para a Prática do Cirurgião Digestivo
A história de McDowell e Crawford oferece lições atemporais para a prática médica moderna:
- Inovação Contra o Dogma: A medicina avança quando profissionais questionam verdades estabelecidas. McDowell transcendeu o “padrão de cuidado” de sua época, confiando em seu julgamento clínico e conhecimento anatômico para fazer o que era considerado impossível.
- A Primazia do Diagnóstico Clínico: A habilidade de McDowell em realizar um diagnóstico preciso baseado unicamente no exame físico e no raciocínio clínico é uma lição poderosa. É um lembrete contundente de que, na ausência de tecnologia, a verdadeira excelência reside no raciocínio anatômico e na sensibilidade do exame clínico — habilidades que jamais devem ser atrofiadas.
- A Aliança Cirurgião-Paciente: O sucesso da empreitada dependeu de uma confiança mútua extraordinária. O consentimento informado de Crawford, mesmo em sua forma mais rudimentar, foi o pilar que sustentou a realização de um procedimento de altíssimo risco.
- Coragem e Responsabilidade: McDowell demonstrou a coragem necessária para ser o primeiro, assumindo total responsabilidade pelo resultado. Ele sabia que, em caso de falha, o peso do fracasso recairia inteiramente sobre ele.
5.0 O Legado Imortal de McDowell e Crawford
A cirurgia realizada em um quarto de uma cidade fronteiriça não foi um avanço evolutivo; foi um salto revolucionário. Nasceu da visão de um homem e da coragem de uma mulher, que juntos mudaram o curso da história da medicina. Não foi o produto de uma “escola” cirúrgica ou de anos de pesquisa, mas um ato de genialidade e audácia que surgiu de novo. Com sua genialidade, Ephraim McDowell devolveu a vida a Jane Todd Crawford; ela, em troca, garantiu-lhe a imortalidade. O que eles realizaram juntos foi, de fato, o início de uma nova era para a medicina.
#HistóriaDaMedicina #CirurgiaAbdominal #Laparotomia #EphraimMcDowell #CirurgiaDigestiva
Além do Bisturi: A Filosofia Cirúrgica de René Leriche e a Revolução Fisiológica
Na história da medicina, existem cirurgiões famosos por suas mãos ágeis e outros lembrados por suas mentes inquietas. René Leriche (1879-1955) pertence, indubitavelmente, à segunda categoria. Embora fosse um operador exímio, seu verdadeiro bisturi era o intelecto. Autor da obra seminal “La chirurgie, discipline de la connaissance” (A cirurgia, disciplina do conhecimento), Leriche não via a sala de operações apenas como um local de reparo mecânico, mas como um laboratório vivo de fisiologia. Para ele, operar era interrogar a vida. Neste artigo, revisitamos a filosofia deste gigante francês e como ele transformou a cirurgia de um ofício anatômico para uma ciência biológica.
Da Anatomia Estática à Fisiologia Dinâmica
Até o início do século XX, a cirurgia era predominantemente “anatômica”. O cirurgião era visto como um encanador de luxo: removia-se o que estava podre, costurava-se o que estava rasgado, drenava-se o que estava infectado. O foco era a lesão estrutural visível. Leriche desafiou esse paradigma. Ele argumentava que a lesão anatômica era frequentemente o fim da doença, não o começo. A verdadeira patologia residia no distúrbio funcional invisível que precedia a lesão.
“A doença é, antes de tudo, um drama funcional que se desenrola no silêncio dos tecidos.”
Essa visão deu origem ao conceito de Cirurgia Fisiológica. O objetivo não deveria ser apenas a extirpação do órgão doente (uma “confissão de fracasso”, segundo ele), mas a restauração da função normal, muitas vezes através da manipulação do sistema nervoso autônomo e da vascularização.
A Cirurgia como “Vivissecção Terapêutica”
Leriche elevou o status epistemológico da cirurgia. Ele afirmava que o cirurgião possuía um privilégio que o anatomista e o patologista não tinham: o acesso à patologia viva. Enquanto a anatomia patológica estuda as “cinzas do incêndio” (o tecido morto), a cirurgia observa o “fogo” (a doença em evolução). Portanto, a cirurgia deveria ser uma “disciplina do conhecimento”, onde cada intervenção serve para entender a fisiopatologia humana. Para Leriche, um cirurgião que não raciocina fisiologicamente é apenas um técnico manual, fadado à obsolescência.
A Dor como Doença (La Douleur-Maladie)
Talvez a contribuição mais humanística de Leriche tenha sido sua guerra contra a dor. Rompendo com a tradição estoica que via a dor como um mecanismo de defesa útil ou um aviso benéfico, Leriche a classificou como um erro biológico. Ele cunhou o termo “A Dor-Doença”. Na visão dele, a dor crônica não protege; ela destrói. Ela altera a personalidade, esgota as reservas vitais e cria um ciclo vicioso simpático que perpetua o sofrimento. Suas pesquisas sobre a causalgia e o papel do sistema simpático na dor abriram as portas para a moderna medicina da dor e a neuromodulação. Foi neste contexto que ele nos legou sua definição poética e precisa de saúde:
“A saúde é a vida no silêncio dos órgãos.”
O Legado de Leriche na Cirurgia Moderna
Por que ler René Leriche em pleno século XXI? Porque a cirurgia moderna é, em essência, a realização do sonho de Leriche. Quando realizamos uma cirurgia metabólica para tratar diabetes (e não apenas para reduzir o estômago), estamos praticando a cirurgia fisiológica de Leriche. Quando utilizamos bloqueios nervosos ou estimulação medular, estamos seguindo seus passos no controle da dor. Quando buscamos a preservação de órgãos em vez da amputação, honramos sua filosofia. René Leriche nos ensinou que a técnica é indispensável, mas é a fisiologia que deve guiar a mão do cirurgião. O virtuosismo técnico sem base científica é perigoso; a ciência sem técnica é impotente. O cirurgião completo, portanto, é aquele que opera com as mãos, mas corta com a mente.
Gostou desta reflexão histórica? Acompanhe o The Surgeon para mais conteúdos sobre a arte, a ciência e a filosofia da cirurgia.
A Dualidade da Humanização Cirúrgica
Era da Inteligência Artificial e da Robótica: Desafios e Perspectivas
Por Prof. Dr. Ozimo Gama
Coordenador do Curso de Medicina da Universidade Federal do Maranhão
O Cenário Atual e a Necessidade do “Toque Humano”
A prática da cirurgia do aparelho digestivo vive um momento de paradoxo fascinante. Por um lado, testemunhamos avanços tecnológicos sem precedentes, com a cirurgia robótica e a inteligência artificial (IA) redefinindo os limites do possível. Por outro, enfrentamos uma crise silenciosa na relação médico-paciente. No Brasil, segundo dados do DATASUS e do Conselho Federal de Medicina, realizamos milhões de procedimentos cirúrgicos anuais pelo Sistema Único de Saúde (SUS), onde a alta demanda muitas vezes colide com a necessidade de um atendimento individualizado.
A “humanização” não é apenas um conceito abstrato ou uma “soft skill” desejável; é um imperativo clínico. Estudos epidemiológicos demonstram que pacientes que estabelecem uma relação de confiança sólida com seus cirurgiões apresentam melhor adesão ao tratamento pós-operatório, menores índices de litígios médicos e, subjetivamente, uma percepção de dor reduzida.
O desafio contemporâneo, como bem alertava o Prof. Alcino Lázaro da Silva, é evitar que o “fascínio das máquinas e dos botões” transforme o jovem cirurgião em um “sectário ou robô”. Precisamos integrar a tecnologia sem permitir que ela congele nossos sentimentos ou desqualifique a essência da nossa profissão: o cuidado com o ser humano.
Tecnologia, Ontoética e Controvérsias
A Inteligência Artificial e a Despersonalização
A IA chegou para auxiliar na tomada de decisão, predizendo complicações e otimizando fluxos em centros cirúrgicos. No entanto, existe o risco real da “atrofia da empatia”. Quando confiamos excessivamente em algoritmos para o prognóstico, corremos o risco de tratar o paciente como um conjunto de dados biométricos, e não como uma biografia. A tecnologia deve ser uma ferramenta de meio, nunca de fim. O cirurgião que se esconde atrás da tela do computador perde a oportunidade de exercer a “Ontoética” — a ética do ser, o respeito intrínseco à vida humana que transcende a técnica.
Aspectos Médico-Legais e o Consentimento
A humanização tem implicações jurídicas diretas. O Prof. Milton Glezer destaca que o paciente tem o direito de recusar tratamento (salvo risco iminente de morte) e de ter acesso irrestrito ao seu prontuário. No Brasil, a judicialização da medicina tem crescido exponencialmente. Uma parte significativa desses processos não decorre de erro técnico (imperícia), mas de falha na comunicação. O Consentimento Livre e Esclarecido não deve ser apenas um formulário burocrático assinado na admissão. Ele deve ser um processo contínuo de diálogo, onde o cirurgião traduz o “tecniquês” para a realidade do doente, respeitando sua autonomia e dignidade.
Controvérsias Filosóficas
A controvérsia reside na formação médica atual. Os currículos de graduação e residência muitas vezes privilegiam a técnica em detrimento da humanística. Criamos excelentes técnicos capazes de realizar gastrectomias complexas, mas que, por vezes, falham em comunicar um diagnóstico de câncer gástrico com a compaixão necessária. A escola médica deve ensinar que o doente prefere, acima do tecnocrata, o amigo; acima do executor de procedimentos, o médico que orienta e acolhe.
Aplicação Prática na Cirurgia do Aparelho Digestivo
Na nossa especialidade, a humanização possui facetas muito específicas e impactantes:
- Ostomias e Imagem Corporal: Ao indicar uma colostomia definitiva, por exemplo, o cirurgião digestivo não está apenas alterando a anatomia, mas a autoimagem e a vida social do paciente. A abordagem humanizada exige preparar este paciente psicologicamente, envolvendo a equipe multidisciplinar e a família antes mesmo do ato cirúrgico.
- Oncologia Cirúrgica: O diagnóstico de neoplasias do trato gastrointestinal carrega um estigma de mortalidade. A forma como a notícia é dada (protocolo SPIKES, por exemplo) é tão crucial quanto a linfadenectomia realizada.
- Cirurgia Bariátrica: O paciente obeso muitas vezes carrega anos de preconceito, inclusive dentro do sistema de saúde. A humanização aqui significa enxergar a obesidade como doença crônica, despindo-se de julgamentos morais e oferecendo um suporte que vai além da perda de peso.
Pontos-Chave para a Prática Diária
Para o residente e o jovem cirurgião, a humanização se traduz em atos concretos:
- Olho no Olho: A tecnologia (computadores, tablets) não deve ser uma barreira física durante a consulta. Sente-se, olhe para o paciente e escute ativamente antes de examinar.
- Identificação Clara: Como preconizado nas diretrizes hospitalares, apresente-se, diga sua função e certifique-se de que o paciente sabe quem é o responsável pelo seu tratamento (titularidade médica).
- Gestão da Expectativa: Explique riscos e benefícios reais. A frustração do paciente muitas vezes nasce de uma expectativa irrealista não corrigida pelo cirurgião no pré-operatório.
- O “Não” Terapêutico: Saber a hora de não operar (obstinação terapêutica) em casos de carcinomatose ou doenças terminais é, talvez, a maior prova de humanidade e ética cirúrgica.
Perspectivas Futuras
O futuro da Cirurgia do Aparelho Digestivo não será definido apenas pela precisão dos robôs ou pela acurácia dos algoritmos de IA, mas pela nossa capacidade de manter a essência humana em um ambiente cada vez mais digital. A “Ontoética” deve guiar nossas mãos tanto quanto a anatomia.
Precisamos formar cirurgiões “híbridos”: exímios operadores da tecnologia, mas profundos conhecedores da alma humana. Como discutido nos textos bases, o hospital deve buscar trazer esperança, e o médico deve lembrar que, ao tratar um doente, está lidando com uma unidade indivisível de medos, histórias e sentimentos. A tecnologia passa, a máquina obsoleta é trocada, mas o impacto de um atendimento humano perdura na memória do paciente e de seus familiares.
#CirurgiaDigestiva #HumanizaçãoMédica #Bioética #EducaçãoMédica #OncologiaCirurgica
“O único meio de combater a praga da impessoalidade e da frieza na medicina moderna é cultivar as humanidades no médico, pois o segredo do cuidado com o paciente é importar-se com o paciente.” — Adaptado de Francis Peabody (embora clínico, sua máxima é a pedra angular para a humanização cirúrgica moderna).
Gostou? ❔ Nos deixe um comentário ✍️, compartilhe em suas redes sociais e/ou mande sua dúvida pelo 💬 Chat Online em nossa DM do Instagram.
Princípios Fundamentais da Oncologia Cirúrgica Digestiva
Uma Abordagem Contemporânea e Baseada em Evidências
O Cenário Atual do Câncer Digestivo no Brasil
A Cirurgia do Aparelho Digestivo vive um momento de transformação sem precedentes. Não somos mais apenas “técnicos de ressecção”, mas parte integrante de uma complexa engrenagem multidisciplinar. A relevância deste tema é sublinhada pelos dados epidemiológicos alarmantes. Se no passado nos baseávamos em estimativas modestas, hoje a realidade é desafiadora: segundo a Estimativa 2023-2025 do Instituto Nacional de Câncer (INCA), esperam-se 704 mil casos novos de câncer por ano no Brasil.
Destaque-se que as neoplasias do trato gastrointestinal ocupam posições cimeiras. O câncer colorretal figura como o segundo mais incidente em mulheres e homens na maioria das regiões, com cerca de 45 mil novos casos anuais, seguido de perto pelo câncer de estômago (21 mil casos) e esôfago. Estes números não são apenas estatísticas; representam uma demanda crescente por cirurgiões oncológicos altamente qualificados, capazes de compreender não apenas a anatomia, mas a biologia tumoral.
A Biologia como Norte da Técnica Cirúrgica
Fisiopatologia e Disseminação
O entendimento clássico da cirurgia oncológica, herdado dos princípios de William Halsted no final do século XIX, baseava-se na premissa de que o câncer era uma doença puramente local que se disseminava centrifugamente. Embora a radicalidade (ressecção em bloco) permaneça um pilar, hoje compreendemos a doença como sistêmica desde fases precoces em muitos casos.
A disseminação ocorre por três vias principais que o cirurgião deve dominar:
- Linfática: Predominante em carcinomas (ex: adenocarcinoma gástrico e cólon).
- Hematogênica: Preferencial em sarcomas e carcinomas avançados (fígado e pulmões como sítios-alvo).
- Transcelômica (Peritoneal): Comum em neoplasias gástricas T3/T4, ovário e apêndice, exigindo estratégias específicas como a peritoniectomia.
O Princípio da Radicalidade e Margens (R0)
O objetivo primário da cirurgia oncológica curativa é a ressecção R0 (ausência de doença residual macroscópica e microscópica). A cirurgia R1 (doença microscópica residual) ou R2 (macroscópica) impacta drasticamente o prognóstico.
- Ressecção em Bloco: O tumor nunca deve ser violado. A peça deve ser removida envolta por tecido saudável, respeitando as fáscias anatômicas e os pedículos vasculares na sua origem.
- Linfadenectomia: Não serve apenas para estadiamento, mas tem papel terapêutico. No câncer gástrico, por exemplo, a linfadenectomia D2 é o padrão-ouro em centros especializados, associada a menor recidiva locorregional.
Neoadjuvância vs. Adjuvância
A decisão entre operar primeiro (upfront surgery) ou indicar terapia neoadjuvante é um dos grandes debates atuais.
- Vantagens da Neoadjuvância: Tratamento precoce de micrometástases, redução do tumor (downstaging) facilitando a ressecção R0 e teste in vivo da quimiossensibilidade. É o padrão atual para câncer de esôfago localmente avançado e câncer de reto médio/baixo.
- Vantagens da Adjuvância: Baseada no estadiamento patológico preciso (pTNM), evitando tratamento excessivo em estádios precoces.
Aplicação Prática na Cirurgia Digestiva
A prática moderna exige que o cirurgião diferencie dois conceitos cruciais frequentemente confundidos: Ressecabilidade e Operabilidade.
- Ressecabilidade: É uma característica do tumor (relação com estruturas vitais).
- Operabilidade: É uma característica do paciente (reserva funcional, comorbidades, status performance). Um tumor pode ser ressecável, mas o paciente inoperável.
O Papel da Citorredução e HIPEC
Para a carcinomatose peritoneal, historicamente considerada uma condição terminal, houve uma mudança de paradigma. Em neoplasias selecionadas (como pseudomixoma peritoneal, mesotelioma e alguns casos de câncer colorretal), a combinação de Cirurgia de Citorredução (Peritoniectomia) com Quimioterapia Intraperitoneal Hipertérmica (HIPEC) tem oferecido sobrevida em longo prazo, transformando uma doença fatal em uma condição crônica tratável.
Planejamento Multidisciplinar
O cirurgião oncológico não atua isolado. A discussão em Tumor Boards é mandatória. A indicação cirúrgica deve considerar a biologia molecular (ex: status do gene APC em colorretal, superexpressão de HER2 em gástrico) e a resposta a terapias sistêmicas.
Pontos-Chave para a Prática Cirúrgica
- Estadiamento Preciso: Nunca leve um paciente à sala sem um estadiamento completo. A laparoscopia diagnóstica é fundamental em tumores gástricos e pancreáticos para evitar laparotomias desnecessárias em casos de carcinomatose oculta.
- Margens Cirúrgicas: A margem circunferencial (radial) no câncer de reto e a margem proximal no câncer gástrico e esofágico são preditores independentes de sobrevida.
- Manuseio da Peça (“No-touch technique”): Evite a manipulação direta do tumor. A ligadura vascular prévia e a mobilização cuidadosa previnem a embolização tumoral intraoperatória.
- Documentação: O relatório cirúrgico deve detalhar as cadeias linfáticas dissecadas e as estruturas preservadas ou ressecadas, orientando o patologista e o oncologista clínico.
Perspectivas Futuras
A cirurgia digestiva na sua área de atuação oncológica evoluiu de amputações extensas para procedimentos de precisão, muitas vezes minimamente invasivos (laparoscópicos ou robóticos), sem perder a radicalidade oncológica. O futuro aponta para uma integração ainda maior com a biologia molecular e a imunoterapia. O cirurgião do futuro deverá ser, antes de tudo, um oncologista que opera: alguém que entende que o bisturi é apenas uma das armas, e que saber quando não operar é tão vital quanto a técnica operatória refinada.
Como nos ensinou o pai da cirurgia oncológica moderna:
“O cirurgião deve ser o médico do paciente oncológico, e não apenas o técnico que remove o tumor.” — William Stewart Halsted
Hashtags
#CirurgiaDigestiva #OncologiaCirurgica #EducaçãoMédica #ResidenciaCirurgia #CancerDigestivo
Gostou? ❔ Nos deixe um comentário ✍️, compartilhe em suas redes sociais e/ou mande sua dúvida pelo 💬 Chat Online em nossa DM do Instagram.
A Importância da Competência em Endoscopia Flexível na Formação e Prática do Cirurgião do Aparelho Digestivo
Introdução
A endoscopia digestiva flexível transcende a sua definição clássica de método diagnóstico. Na contemporaneidade, ela se consolida como uma extensão essencial da propedêutica e da terapêutica cirúrgica. Historicamente, é imperativo recordar que a endoscopia é um campo desbravado por cirurgiões. Grandes marcos, como a polipectomia colônica (Dr. Hiromi Shinya), a ligadura elástica de varizes (Dr. Goffredo Steigman) e a gastrostomia percutânea (Dr. Jeffrey Ponsky), foram estabelecidos por mentes cirúrgicas que vislumbravam além da incisão convencional. No entanto, observa-se um fenômeno preocupante na formação médica atual: a delegação progressiva dessa competência quase exclusivamente à gastroenterologia clínica e aos Endoscopistas. Este artigo, direcionado a estudantes, residentes e pós-graduandos, visa reafirmar a premissa de que a habilidade endoscópica não é opcional, mas intrínseca à prática do cirurgião do aparelho digestivo de excelência. Discutiremos as bases técnicas, a aplicabilidade clínica e a necessidade premente de retomar o protagonismo nesta área.
Desenvolvimento: O Cirurgião e a Habilidade Endoscópica
A Curva de Aprendizado e a Visão Cirúrgica
A competência em endoscopia flexível depende da fusão entre conhecimento cognitivo e habilidade técnica (psicomotora). O cirurgião, habituado à manipulação tecidual e à anatomia tridimensional (seja por via aberta ou laparoscópica), possui, intrinsecamente, uma coordenação olho-mão refinada. Estudos demonstram que cirurgiões tendem a apresentar uma curva de aprendizado acelerada para procedimentos endoscópicos devido à sua familiaridade com a anatomia topográfica e patológica, permitindo uma transição fluida entre a visão bidimensional da tela e a realidade espacial do órgão.
O Cenário Brasileiro e a Demografia Médica
No contexto do Brasil, um país de dimensões continentais, a distribuição de especialistas é heterogênea. Segundo dados da Demografia Médica no Brasil (CFM/USP, 2023), a concentração de gastroenterologistas clínicos | endoscopistas é significativamente menor e mais centralizada em grandes capitais do que a de cirurgiões gerais. O cirurgião geral, muitas vezes, é o único provedor de saúde especializado em regiões remotas. Portanto, capacitar o cirurgião em endoscopia não é apenas uma questão de reserva de mercado, mas uma estratégia de saúde pública para garantir o rastreamento de neoplasias (como o câncer colorretal) e o atendimento de urgências (Hemorragia Digestiva Alta) em todo o território nacional.
Do “Cirurgião de Resgate” ao “Cirurgião Estrategista”
Tradicionalmente, o cirurgião é chamado apenas quando ocorre uma complicação endoscópica, como perfuração ou sangramento incontrolável. Este paradigma do “cirurgião de resgate” deve evoluir para o de “cirurgião estrategista”. Ao dominar a endoscopia, o profissional torna-se o capitão do navio terapêutico, capaz de indicar, executar e, se necessário, converter procedimentos com total autonomia e continuidade do cuidado (Continuity of Care), otimizando desfechos e minimizando a fragmentação do tratamento.
Aplicação na Cirurgia Digestiva
A integração da endoscopia na rotina cirúrgica pode ser categorizada em três momentos cruciais:
1. Endoscopia Pré-Operatória: O Planejamento
Na cirurgia oncológica gástrica e esofágica, a endoscopia realizada pelo próprio cirurgião permite uma avaliação precisa das margens tumorais, da extensão para a cárdia ou piloro, influenciando diretamente a decisão entre uma gastrectomia total ou subtotal. Na cirurgia bariátrica, a identificação prévia de hérnias hiatais, esofagites severas ou patologias gástricas altera o algoritmo de tratamento, contraindicando, por exemplo, uma gastrectomia vertical (Sleeve) em favor de um bypass gástrico em Y de Roux.
2. Endoscopia Intraoperatória: A Segurança
O uso transoperatório é uma ferramenta de segurança inestimável. Exemplos clássicos incluem:
- Cardiomiotomia de Heller: Confirmação da adequação da miotomia e teste de vazamento (air leak test) para exclusão de perfurações mucosas.
- Exploração de Vias Biliares: O uso do coledocoscópio flexível permite a visualização direta e a certeza da remoção completa de cálculos, superior à colangiografia em casos complexos.
- Localização de Lesões: Em cirurgias colorretais laparoscópicas, a tatuagem prévia pode ser imprecisa; a colonoscopia intraoperatória garante a ressecção do segmento correto.
3. Endoscopia Pós-Operatória e Manejo de Complicações
O cirurgião que realiza a endoscopia está melhor posicionado para tratar as complicações de seus próprios procedimentos ou de seus pares. O arsenal terapêutico inclui:
- Dilatação com balão de estenoses de anastomoses (gástricas ou colorretais).
- Tratamento de fístulas e deiscências pós-Sleeve ou Bypass com uso de próteses autoexpansíveis ou clips endoscópicos.
- Hemostasia de linhas de sutura sangrantes.
A Era da Cirurgia Sem Cicatrizes (NOTES e Endoterapia)
Caminhamos para a era da intervenção minimamente invasiva máxima. Procedimentos como o POEM (Peroral Endoscopic Myotomy) substituem a miotomia laparoscópica; o Endoscopic Sleeve Gastroplasty (ESG) surge como alternativa à cirurgia bariátrica convencional. O cirurgião do futuro deve dominar estas técnicas para oferecer o tratamento “estado da arte” aos seus pacientes.
Pontos-Chave para o Residente e o Cirurgião Jovem
- Necessidade de Treinamento: As sociedades cirúrgicas (como o CBC e a CBCD no Brasil) têm enfatizado a importância de currículos de residência que contemplem carga horária prática em endoscopia.
- Visão Integral: O domínio da luz luminal (endoscopia) e da cavidade peritoneal (laparoscopia/robótica) cria um cirurgião completo.
- Autonomia: A capacidade de diagnosticar, estadiar, tratar e resolver complicações sem depender de terceiros é o ápice da eficiência clínica.

Conclusão
A endoscopia flexível não é uma especialidade à parte, mas uma ferramenta cirúrgica, tal qual o bisturi ou a pinça laparoscópica. Para o cirurgião do aparelho digestivo, delegar essa competência é abdicar de uma parte fundamental da sua herança histórica e do seu futuro profissional. A formação médica deve encorajar a retomada deste espaço, garantindo que as novas gerações de cirurgiões sejam proficientes tanto na ciência da cirurgia quanto na arte da endoscopia. Como mentores e instituições de ensino, nosso dever é prover o acesso e a estrutura para que essa integração seja a norma, e não a exceção.
“Nenhum homem pode ser um grande cirurgião sem ser também um grande médico; e o inverso é igualmente verdadeiro no que tange ao diagnóstico e compreensão da fisiopatologia.” > — Adaptado de Theodor Billroth, pai da cirurgia gástrica moderna, refletindo a necessidade do conhecimento integral.
Gostou ❔Nos deixe um comentário ✍️ , compartilhe em suas redes sociais e|ou mande sua dúvida pelo 💬 Chat On-line em nossa DM do Instagram.
Hashtags: #CirurgiaDigestiva #EndoscopiaTerapeutica #ResidenciaMedica #CirurgiaGeral #EducacaoMedica
Epônimos da Anatomia Abdominal: A Linguagem Clássica da Prática Cirúrgica
Resumo Apesar dos esforços contínuos da Federative International Programme on Anatomical Terminologies (FIPAT) para padronizar a nomenclatura médica através da Terminologia Anatômica, a linguagem operatória permanece, em essência, histórica. Este artigo revisa os epônimos fundamentais da anatomia abdominal, correlacionando a definição topográfica precisa com a aplicação prática na cirurgia do aparelho digestivo, demonstrando que o domínio destes termos é imperativo para a segurança cirúrgica e a comunicação clínica eficaz.
Introdução
A anatomia topográfica é o alicerce da cirurgia. Contudo, existe uma dicotomia persistente entre a taxonomia descritiva moderna e a tradição oral dos centros cirúrgicos. Enquanto a academia privilegia termos locativos e funcionais, a prática diária — da passagem de plantão à descrição operatória — é dominada por epônimos. Estes nomes não são meros vestígios históricos; funcionam como “atalhos cognitivos” que evocam, simultaneamente, uma localização, uma relação anatômica complexa e, frequentemente, uma manobra cirúrgica específica. Este estudo revisa os principais epônimos do abdome, dissecando sua anatomia estrutural e sua relevância crítica na cirurgia geral e digestiva.
1. Parede Abdominal e Região Inguinal
A compreensão da estratigrafia da parede abdominal é o primeiro passo para o acesso seguro à cavidade peritoneal e para o reparo eficaz dos defeitos herniários.
Estratigrafia Subcutânea e Fascial
- Fáscia de Camper
- Anatomia: Camada superficial, de espessura variável e consistência adiposa, do tecido subcutâneo da parede abdominal anterior.
- Relevância Cirúrgica: A sua aproximação é frequentemente negligenciada, mas o manejo adequado do espaço morto nesta camada é vital na prevenção de seromas e infecções de sítio cirúrgico superficiais em laparotomias.
- Fáscia de Scarpa
- Anatomia: Camada membranosa profunda do tecido subcutâneo, contendo fibras elásticas amarelas, que se funde com a fáscia lata da coxa inferiormente e continua como Fáscia de Colles no períneo.
- Relevância Cirúrgica: Estrutura de fixação essencial no fechamento da parede abdominal. A sutura desta camada reduz a tensão sobre a pele e melhora o resultado estético da cicatriz. Devido à sua continuidade perineal, orienta a disseminação de extravasamentos de urina (fraturas de uretra) ou infecções necrotizantes (Síndrome de Fournier).
- Fáscia Inominada de Gallaudet
- Anatomia: A fáscia profunda aderida intimamente à aponeurose do músculo oblíquo externo e bainha do reto.
- Relevância Cirúrgica: Define o plano de dissecção “limpo” sobre a aponeurose durante o reparo de hérnias ou a confecção de retalhos miocutâneos.
Anatomia Inguinal e o Assoalho Pélvico
- Ligamento de Poupart (Ligamento Inguinal)
- Anatomia: A borda inferior espessa e recorvada da aponeurose do oblíquo externo, estendendo-se da Espinha Ilíaca Antero-Superior (EIAS) ao tubérculo púbico.
- Relevância Cirúrgica: O marco anatômico absoluto que diferencia hérnias inguinais (acima) de femorais (abaixo) e serve como âncora inferior para reparos teciduais clássicos (técnica de Bassini) e fixação de telas (técnica de Lichtenstein).
- Ligamento de Gimbernat (Ligamento Lacunar)
- Anatomia: Uma extensão triangular das fibras do ligamento inguinal que se reflete posteriormente e se insere na linha pectínea.
- Relevância Cirúrgica: Forma a borda medial do anel femoral. Em casos de hérnia femoral encarcerada, este ligamento é frequentemente a estrutura constritora que deve ser incisada (com cautela devido à presença eventual da Corona Mortis vascular) para redução do conteúdo.
- Ligamento de Cooper (Ligamento Pectíneo)
- Anatomia: Espessamento do periósteo e fáscia ao longo da crista pectínea (pecten do púbis), posterior ao ligamento inguinal.
- Relevância Cirúrgica: Estrutura de ancoragem robusta utilizada na técnica de McVay e ponto de fixação crítico para telas em reparos laparoscópicos (TAPP/TEP), prevenindo a recidiva direta.
- Triângulo de Hesselbach
- Anatomia: Delimitado inferiormente pelo ligamento inguinal, lateralmente pelos vasos epigástricos inferiores e medialmente pela borda lateral do músculo reto abdominal.
- Relevância Cirúrgica: Local anatômico das hérnias inguinais diretas, resultantes da fraqueza da fáscia transversal, sem passagem pelo anel inguinal profundo.
- Orifício Miopectíneo de Fruchaud
- Anatomia: Área de fraqueza da parede abdominal inferior que engloba tanto a região inguinal quanto a femoral, delimitada pelo músculo oblíquo interno (superior), reto abdominal (medial), iliopsoas (lateral) e osso púbico (inferior).
- Relevância Cirúrgica: Conceito fundamental para a cirurgia moderna de hérnia. Estabelece que o tratamento definitivo deve cobrir toda esta área com material protético (tela) para prevenir todos os tipos de hérnias da virilha, princípio base das abordagens pré-peritoneais (Stoppa, TEP, TAPP).
2. Peritônio e Topografia Gastrointestinal
A semiologia abdominal e o acesso cirúrgico baseiam-se em projeções de superfície e recessos cavitários.
- Linha de Monro-Richter e Ponto de McBurney
- Anatomia: Linha traçada da EIAS à cicatriz umbilical. O Ponto de McBurney localiza-se na união do terço lateral com os dois terços mediais desta linha.
- Relevância Cirúrgica: Projeção clássica da base do apêndice cecal. Guia a incisão oblíqua (McBurney) para apendicectomias abertas e é o ponto de máxima dor à descompressão na apendicite aguda.
- Ponto de Lanz
- Anatomia: Ponto na junção do terço direito com o terço médio da linha bi-ilíaca.
- Relevância Cirúrgica: Representa a projeção variável do ápice de um apêndice pélvico longo, importante no diagnóstico diferencial de patologias anexiais em mulheres.
- Ponto de Murphy
- Anatomia: Ponto situado abaixo do rebordo costal direito, na linha hemiclavicular (borda lateral do reto abdominal).
- Relevância Cirúrgica: Local de palpação do fundo da vesícula biliar. A interrupção súbita da inspiração à palpação profunda (Sinal de Murphy) é altamente sugestiva de colecistite aguda.
- Espaços Peritoneais (Morison, Douglas, Proust, Winslow)
- Bolsa de Morison (Recesso Hepatorrenal): Espaço virtual entre o fígado e o rim direito. É o local mais dependente do abdome superior em decúbito dorsal; local primário de acúmulo de líquido livre (sangue/pus) detectável pelo FAST em trauma.
- Fundo de Saco de Douglas (Retouterino): Ponto mais declive da cavidade peritoneal em mulheres. Local de acúmulo de líquido e de implantes metastáticos palpáveis ao toque retal/vaginal (Prateleira de Blumer).
- Espaço de Proust (Retovesical): Correspondente masculino ao de Douglas, entre o reto e a bexiga/próstata. Relevante na dissecção oncológica do reto baixo.
- Forame de Winslow (Forame Epiploico): Comunicação entre a grande cavidade e a retrocavidade dos epíplons (bolsa omental). Clinicamente, é a via de acesso para a Manobra de Pringle (clampeamento do pedículo hepático para controle de hemorragia) e local potencial para hérnias internas.
3. Trato Digestório e Glândulas Anexas
Nesta região, os epônimos descrevem marcos críticos para ressecções oncológicas e reconstruções.
- Ângulo de His
- Anatomia: Ângulo agudo formado entre o esôfago abdominal e o fundo gástrico.
- Relevância Cirúrgica: Componente anatômico crucial do mecanismo valvular anti-refluxo. A restauração ou acentuação deste ângulo é o objetivo central das fundoplicaturas (Nissen, Toupet) no tratamento da DRGE.
- Espaço de Traube e Triângulo de Labbé
- Anatomia: Áreas de projeção gástrica na parede toracoabdominal.
- Relevância Cirúrgica: O Espaço de Traube (timpânico à percussão) torna-se maciço em casos de esplenomegalia ou derrame pleural. O Triângulo de Labbé é a área de contato do estômago com a parede abdominal anterior, local seguro para gastrostomias percutâneas ou cirúrgicas.
- Ligamento de Treitz
- Anatomia: Músculo suspensor do duodeno, marcando a transição duodeno-jejunal (ângulo de Treitz).
- Relevância Cirúrgica: Divisor anatômico e clínico entre hemorragia digestiva alta e baixa. Marco fundamental para a mobilização do intestino delgado e identificação da primeira alça jejunal em reconstruções (ex: Y de Roux).
- Vias Biliares: Calot, Heister, Vater, Oddi
- Triângulo de Calot (Cisto-Hepático): Delimitado pelo ducto cístico, ducto hepático comum e borda inferior do fígado. Contém a artéria cística e, frequentemente, o linfonodo de Mascagni. Sua dissecção meticulosa para obter a “Visão Crítica de Segurança” (Critical View of Safety) é mandatória para prevenir lesões iatrogênicas da via biliar principal na colecistectomia.
- Válvulas de Heister: Pregas espirais na mucosa do ducto cístico que podem dificultar a cateterização durante a colangiografia intraoperatória.
- Ampola de Vater e Esfíncter de Oddi: A confluência biliopancreática e seu aparelho esfincteriano. Alvo terapêutico nas papilotomias endoscópicas (CPRE) para tratamento de coledocolitíase ou pancreatite biliar.
- Ductos Pancreáticos (Wirsung e Santorini)
- Anatomia: Wirsung é o ducto principal; Santorini é o acessório.
- Relevância Cirúrgica: A variante Pancreas Divisum (falha na fusão dos ductos) drena a maior parte do pâncreas pelo ducto menor (Santorini), sendo causa de pancreatites recorrentes inexplicadas.
- Marcos Hepáticos (Glisson e Cantlie)
- Cápsula de Glisson: Bainha de tecido conjuntivo que envolve o fígado e a tríade portal intra-hepática. Importante na manobra de Pringle e nas hepatectomias.
- Linha de Cantlie: Linha imaginária que divide o fígado funcionalmente em lobos direito e esquerdo, estendendo-se do leito da vesícula biliar à veia cava inferior. Base para hepatectomias anatômicas maiores.
4. Vascularização Abdominal e Colateralização
O conhecimento das arcadas vasculares é determinante para a viabilidade de anastomoses intestinais.
- Tripus Halleri (Tronco Celíaco)
- Anatomia: Trifurcação da aorta abdominal em artéria gástrica esquerda, esplênica e hepática comum.
- Relevância Cirúrgica: O controle vascular proximal em cirurgias de trauma, gastrectomias e pancreatectomias. Variações anatômicas são frequentes e devem ser antecipadas em planejamentos pré-operatórios.
- Arcada de Riolan e Artéria Marginal de Drummond
- Anatomia: Sistemas de anastomose entre a artéria cólica média (ramo da mesentérica superior) e a cólica esquerda (ramo da mesentérica inferior).
- Relevância Cirúrgica: Garantem a irrigação do cólon, especialmente na flexura esplênica (ponto crítico de Griffiths). A preservação ou a integridade funcional destas arcadas é vital para evitar isquemia do coto colônico em retossigmoidectomias e cirurgias de aneurisma de aorta.
- Veias de Sappey e Retzius
- Anatomia: Veias acessórias do sistema porta. As de Sappey correm no ligamento falciforme; as de Retzius são anastomoses retroperitoneais.
- Relevância Cirúrgica: Em pacientes com hipertensão portal, estas veias dilatam-se dramaticamente. As veias de Sappey podem causar hemorragia maciça na incisão supraumbilical. A dissecção do retroperitônio em cirróticos pode encontrar o “sangramento em lençol” das veias de Retzius, de difícil controle.
5. Retroperitônio e Rins
A anatomia dos planos fasciais renais é a chave para a cirurgia oncológica retroperitoneal radical.
- Fáscia de Gerota (e suas lâminas Toldt e Zuckerkandl)
- Anatomia: A fáscia renal envolve o rim e a adrenal em um compartimento fechado. A lâmina anterior é frequentemente associada à Fáscia de Toldt (no contexto da fusão com o mesocólon), e a posterior à Fáscia de Zuckerkandl.
- Relevância Cirúrgica: A “Fáscia de Toldt” (ou linha de Toldt) representa o plano de clivagem avascular embrionário entre o mesocólon e o retroperitônio. A dissecção neste plano permite a mobilização incruenta do cólon direito e esquerdo, essencial em colectomias oncológicas laparoscópicas e abertas. A violação da Fáscia de Gerota propriamente dita é indicativa de invasão tumoral renal ou necessária para nefrectomias radicais.
Conclusão
O domínio dos epônimos da anatomia abdominal transcende o exercício de erudição histórica; constitui uma ferramenta de precisão técnica. Falar em “Triângulo de Calot” ou “Fáscia de Toldt” evoca, instantaneamente, uma estratégia cirúrgica e um plano de segurança. Para o cirurgião do aparelho digestivo, a fluência nesta linguagem clássica é tão fundamental quanto a destreza manual, permitindo a integração segura entre o conhecimento anatômico estático e a dinâmica do ato operatório.
Referência-Base: ten Donkelaar HJ, Quartu M, Kachlík D. An Illustrated Guide to Anatomical Eponyms. Springer, 2025.
Índice Biográfico dos Epônimos Citados
Abaixo listam-se os dados biográficos dos anatomistas e cirurgiões cujos epônimos foram discutidos neste artigo.
- Blumer, George (Reino Unido/EUA, 1858–1940)
- Calot, Jean-François (França, 1861–1944)
- Camper, Pieter (Holanda, 1722–1789)
- Cantlie, James (Escócia, 1851–1926)
- Colles, Abraham (Irlanda, 1773–1843)
- Cooper, Astley Paston (Reino Unido, 1768–1841)
- Douglas, James (Escócia, 1675–1742)
- Drummond, Hamilton (Reino Unido, 1882–1925)
- Fruchaud, Henri (França, 1894–1960)
- Gallaudet, Bern Budd (EUA, 1860–1934)
- Gerota, Dimitrie (Romênia, 1867–1939)
- Gimbernat, Antoni de (Espanha, 1734–1816)
- Glisson, Francis (Reino Unido, 1597–1677)
- Griffiths, Joseph (País de Gales, 1863–1945)
- Haller, Albrecht von (Suíça, 1708–1777)
- Heister, Lorenz (Alemanha, 1683–1758)
- Hesselbach, Franz Kaspar (Alemanha, 1759–1816)
- His, Wilhelm Jr. (Suíça, 1863–1934)
- Labbé, Léon (França, 1832–1916)
- Lanz, Otto (Suíça, 1865–1935)
- Mascagni, Paolo (Itália, 1755–1815)
- McBurney, Charles (EUA, 1845–1913)
- Monro, Alexander III (Escócia, 1773–1859)
- Morison, James Rutherford (Reino Unido, 1853–1939)
- Murphy, John Benjamin (EUA, 1857–1916)
- Oddi, Ruggero (Itália, 1864–1913)
- Poupart, François (França, 1661–1709)
- Pringle, James Hogarth (Escócia, 1863–1941)
- Proust, Robert (França, 1873–1935)
- Retzius, Anders (Suécia, 1796–1860)
- Richter, August Gottlieb (Alemanha, 1742–1812)
- Riolan, Jean (o Jovem) (França, 1580–1657)
- Santorini, Giovanni Domenico (Itália, 1681–1737)
- Sappey, Marie Philibert Constant (França, 1810–1896)
- Scarpa, Antonio (Itália, 1752–1832)
- Toldt, Carl (Áustria, 1840–1920)
- Traube, Ludwig (Alemanha, 1818–1876)
- Treitz, Václav (República Tcheca/Áustria, 1819–1872)
- Vater, Abraham (Alemanha, 1684–1751)
- Winslow, Jacob Benignus (Dinamarca/França, 1669–1760)
- Wirsung, Johann Georg (Alemanha, 1589–1643)
- Zuckerkandl, Emil (Áustria, 1849–1910)
Lifelong Learning na Cirurgia: como a Aprendizagem Autorregulada Define o Cirurgião que Você Vai Ser
Introdução
A cirurgia é uma das áreas da medicina que mais muda ao longo do tempo. Técnicas, tecnologias, diretrizes e condutas são revisadas continuamente. Ninguém termina a residência “pronto para tudo”. O que diferencia o cirurgião que se mantém competente e atualizado ao longo da carreira não é apenas o que aprendeu na formação inicial, mas a capacidade de continuar aprendendo de forma ativa, intencional e estruturada.
Esse é o núcleo do conceito de Lifelong Learning: o compromisso de adquirir, revisar e integrar novos conhecimentos desde o primeiro dia de faculdade até o último dia de atividade profissional. E, na prática, o que sustenta isso é um conjunto de habilidades chamado aprendizagem autorregulada.
O problema: bons alunos, maus aprendizes
Grande parte dos estudantes que chegam à residência é formada por “altos desempenhos acadêmicos”. Mas muitos:
- atribuem sucesso e fracasso quase sempre ao professor, ao serviço ou ao tipo de prova;
- não conseguem descrever com clareza como estudam;
- acreditam que aprender é algo que “acontece com eles”, não algo que podem controlar.
Esse modelo funciona em um ambiente escolar tradicional, com provas previsíveis e conteúdo delimitado. Em cirurgia, não. No centro cirúrgico, na UTI ou no pronto-socorro, o cirurgião depende de outra coisa: da capacidade de identificar o que não sabe, de estudar com foco e de ajustar a própria prática a partir de resultados reais.
É aqui que entra a aprendizagem autorregulada.
O que é aprendizagem autorregulada?
Aprendizagem autorregulada é o conjunto de hábitos, estratégias e atitudes que fazem o aluno assumir o controle do próprio processo de aprendizagem.
Um aprendiz autorregulado:
- pensa sobre como aprende (metacognição);
- acredita que é capaz de melhorar com esforço e estratégia (autoeficácia realista);
- organiza o ambiente, o tempo e os recursos para aprender melhor (comportamento ativo).
Na prática, isso aparece em três dimensões:
1. Metacognitiva
- Define objetivos de aprendizado (“quero entender critérios de indicação de neoadjuvância no pâncreas”, “quero melhorar decisão em vesícula difícil”).
- Planeja como chegar lá (o que ler, que casos observar, que vídeos rever).
- Monitora se está, de fato, avançando.
- Se autoavalia com honestidade ao final.
2. Motivacional
- Liga esforço a desempenho.
- Não se vê como “bom” ou “ruim”, mas como alguém em processo de desenvolvimento.
- Usa erros como feedback, não como sentença.
3. Comportamental
- Seleciona ativamente casos, plantões e oportunidades que trazem aprendizado.
- Busca ajuda, feedback e coaching quando necessário.
- Usa estratégias de estudo estruturadas, não apenas leitura passiva.
O ciclo da aprendizagem autorregulada
Você pode enxergar esse processo como um ciclo contínuo:
- Planejamento (forethought)
- O que quero aprender?
- Por que isso é importante agora?
- Quanto tempo vou dedicar? Com que materiais?
- Execução (performance)
- Implementar o plano (leitura, vídeo, simulação, prática supervisionada).
- Monitorar em tempo real: estou entendendo? estou apenas decorando? estou aplicando?
- Reflexão (self-reflection)
- O que funcionou? O que não funcionou?
- O problema foi falta de esforço, estratégia inadequada, falta de recurso ou algo fora do meu controle?
- O que vou manter, o que vou mudar no próximo ciclo?
Quem atribui tudo a “azar”, “caso difícil”, “erro do serviço” sai mais fraco do caso.
Quem atribui a fatores ajustáveis (estratégia, preparação, decisão) sai mais forte, mesmo depois de um erro.
Ferramentas práticas para residentes e cirurgiões
1. Autoavaliação de como você aprende
Não é apenas “sou bom ou ruim”, mas:
- eu planejo o que estudar ou vou “apagando incêndio”?
- eu mudo de estratégia quando não entendo um tema?
- eu reviso os casos difíceis depois do plantão?
- eu procuro ativamente feedback objetivo sobre minha performance?
Transformar isso em rotina escrita (um caderno, um app, uma planilha) ajuda a tirar a aprendizagem do improviso e colocá-la em modo profissional.
2. Coaching cirúrgico
Coaching não é “mais uma aula”; é uma conversa estruturada para:
- definir objetivos de melhoria claros (ex.: decisão de conversão; planejamento de colecistectomia difícil; comunicação com a equipe);
- identificar pontos cegos (o que você não está vendo sobre a própria prática);
- desenhar um plano concreto de treinamento e estudo.
Ferramentas de vídeo-coaching (assistir a uma operação sua com um colega experiente e revisar decisões, tempos e manobras) têm efeito duplo: refinam a técnica e amplificam a sua metacognição.
3. Leitura inteligente: saindo do “sublinhar tudo”
Um exemplo prático é a estratégia SQ3R para capítulos e diretrizes:
- Survey (percurso) – passar rapidamente pelos subtítulos, tabelas, figuras.
- Question (perguntas) – transformar subtítulos em perguntas (“quando indicar intervalo apendicectomia?”, “como manejar abscesso apendicular?”).
- Read (leitura) – ler com foco em responder suas próprias perguntas.
- Recall (recordar) – fechar o texto e anotar o que lembra de cabeça.
- Review (revisar) – conferir no texto e corrigir lacunas.
É mais trabalhoso do que reler passivamente, mas a retenção é muito maior — e é isso que interessa na prática cirúrgica.
Aplicando isso na formação cirúrgica
Na rotina de um serviço de cirurgia, aprendizagem autorregulada se traduz em ações muito concretas:
- Antes do plantão: definir 1–2 objetivos de aprendizado (por exemplo, “revisar escore de Alvarado e conduta em apendicite complicada”).
- Durante o plantão: escolher conscientemente 1–2 casos para estudar em profundidade depois.
- Após a cirurgia: registrar rapidamente:
- o que foi bem,
- o que não foi,
- o que você precisa estudar para a próxima situação semelhante.
No nível do serviço, vale estimular:
- discussão de M&M com foco em análise de processo, não apenas em “culpa”;
- preceptores que verbalizam seu raciocínio e seus próprios erros;
- metas claras por ano de residência (o que se espera que o R1, R2, R3 saiba de fato).
Pontos-chave para o cirurgião que quer ser lifelong learner
- Assuma o comando do próprio aprendizado – ninguém fará isso por você.
- Planeje o estudo como planeja uma cirurgia – com objetivo, estratégia e checagem.
- Use erro e desconforto como combustível, não como fonte de paralisia.
- Busque feedback específico, não elogios genéricos.
- Padronize suas estratégias de leitura e revisão, fuja do improviso.
Conclusão
Formar um cirurgião tecnicamente competente é obrigatório.
Formar um cirurgião capaz de continuar aprendendo, se adaptando e se avaliando ao longo da vida é o verdadeiro diferencial.
Lifelong learning não é um slogan bonito de documento institucional.
É uma competência prática, treinável, que começa na residência, mas precisa acompanhar cada decisão, cada leitura, cada caso difícil.
Quanto mais cedo você organizar o próprio processo de aprender, mais preparado estará para os desafios que ainda nem existem hoje – mas que certamente farão parte da cirurgia de amanhã.
Hashtags (SEO)
#LifelongLearningEmCirurgia #AprendizagemAutorregulada #FormaçãoDoCirurgião #EducaçãoMédicaContinuada #ResidênciaEmCirurgia
Gostou❔ Deixe seu comentário ✍️, compartilhe com seus colegas e mande sua dúvida pelo 💬 Chat On-line em nossa DM no Instagram.
ASPECTOS MÉDICO-LEGAIS DA LESÃO INADVERTIDA DA VIA BILIAR
- Membro Titular do Colégio Brasileiro de Cirurgiões
- Membro Titular do Colégio Brasileiro de Cirurgia Digestiva
1. Introdução
A lesão inadvertida da via biliar (LVB) é a complicação com maior impacto clínico, emocional e jurídico da colecistectomia. Em muitos países, é uma das principais causas de processos por erro médico em cirurgia geral. Do ponto de vista médico-legal, o ponto central não é a existência da lesão em si, mas a forma como o cirurgião:
- Indicou a cirurgia;
- Conduziu o procedimento (técnica, CVS, bailouts);
- Reconheceu e tratou a lesão;
- Documentou e comunicou o evento ao paciente e à família.
Este texto aborda, em linguagem direta, os principais aspectos médico-legais que o cirurgião geral | cirurgião do aparelho digestivo precisa dominar frente a uma suspeita de lesão iatrogênica da via biliar principal.
2. Lesão de via biliar ≠ erro médico automático
Juridicamente, lesão de via biliar é, em princípio, um evento de risco inerente ao procedimento, sobretudo na colecistectomia laparoscópica, reconhecido em diretrizes nacionais e internacionais.
Em termos de responsabilidade profissional, o que será avaliado é se houve:
- Indicação adequada da cirurgia;
- Técnica compatível com o padrão atual (CVS, uso de bailouts, conversão quando necessário);
- Diligência no reconhecimento precoce da lesão;
- Conduta correta após o dano (referência, reconstrução, suporte);
- Transparência na comunicação.
Ou seja: não é a complicação que gera responsabilidade, e sim a condução inadequada antes, durante ou depois do evento.
3. Consentimento informado
Do ponto de vista pericial, o consentimento é peça-chave:
- A colecistectomia deve ser apresentada como procedimento com:
- Risco de sangramento, infecção, fístula biliar, lesão de via biliar e necessidade de reoperação.
- O termo deve ser:
- Claro, objetivo, datado, assinado pelo paciente (ou responsável) e pela equipe.
- Ideal:
- Anotação no prontuário reforçando que os riscos foram explicados verbalmente.
Em muitos litígios, a ausência de menção à possibilidade de lesão de via biliar no consentimento é usada como argumento de falha na informação, mesmo quando a técnica foi correta.
4. Padrão técnico esperado (CVS, bailouts e conversão)
Peritos costumam avaliar:
- Se houve tentativa documentada de obter o Critical View of Safety;
- Se o cirurgião reconheceu a “vesícula difícil” e utilizou manobras de bailout (subtotal, fundo–primeiro, conversão, abandono);
- Se a insistência em dissecar um triângulo de Calot obliterado foi temerária.
Alguns pontos práticos com peso médico-legal:
- Não obter CVS e mesmo assim clipar e seccionar estruturas é quase sempre visto como conduta imprudente.
- Não converter ou não chamar ajuda em cirurgias claramente difíceis pode ser interpretado como negligência.
- O uso de colangiografia intraoperatória em caso de dúvida anatômica é bem visto pericialmente, mesmo que não obrigatório.
5. Reconhecimento e manejo da lesão intraoperatória
Do ponto de vista jurídico, lesão reconhecida e tratada intraoperatória gera cenário muito mais favorável ao cirurgião do que lesão ignorada e diagnosticada tardiamente com peritonite biliar ou sepse.
Boas práticas com impacto médico-legal:
- Se houver suspeita de lesão maior:
- Registrar no ato operatório que houve dificuldade anatômica e suspeita de dano.
- Se a equipe não tiver expertise em reconstrução, não improvisar; encaminhar para centro de referência.
- Drenos adequados e exames de imagem precoces (TC, colangioRM, CPRE) em pós-operatório duvidoso demonstram diligência.
A omissão em investigar icterícia, febre ou saída de bile por dreno no pós-operatório é frequentemente qualificada como negligência em perícias.
6. Documentação operatória
O relatório cirúrgico é uma das peças centrais em processos médico-legais. Deve conter:
- Indicação da cirurgia (cólica biliar, colecistite aguda, etc.);
- Achados intraoperatórios (inflamação, fibrose, “vesícula difícil”);
- Descrição da técnica:
- Tentativa de obter CVS;
- Uso de colangiografia intraoperatória, quando feita;
- Manobras de bailout, conversão, subtotal, etc.;
- Quaisquer intercorrências (sangramento, suspeita de lesão, necessidade de sutura em via biliar, etc.).
A ausência de descrição detalhada geralmente é interpretada contra o cirurgião, pois abre espaço para a presunção de que padrões técnicos não foram seguidos.
7. Comunicação com o paciente e a família
A forma como o cirurgião comunica a complicação é relevante:
- Negar ou minimizar o evento, ou culpar exclusivamente “o organismo do paciente”, costuma agravar o conflito.
- O recomendado é:
- Explicar com clareza o que ocorreu;
- Deixar claro que a complicação está sendo manejada com todos os recursos disponíveis;
- Documentar o conteúdo da conversa no prontuário.
Transparência e empatia costumam reduzir a judicialização. O oposto também é verdadeiro.
8. Encaminhamento a centros de referência
Outra questão avaliada em perícia é quando e para onde o paciente foi encaminhado:
- Lesões complexas (Strasberg E, perda de segmento biliar, comprometimento vascular) não devem ser reparadas por equipes sem experiência em reconstrução biliodigestiva.
- Reconstruções malsucedidas em série, feitas em hospitais sem expertise, frequentemente são interpretadas como imprudência e imperícia.
O encaminhamento precoce para centro com cirurgião HPB experiente demonstra boa prática e costuma ter peso favorável em eventual demanda judicial.
9. Papel das diretrizes e literatura
Em perícia, é comum a comparação da conduta com:
- Diretrizes societárias (CBCD, WSES, SAGES, EAES etc.);
- Protocolos hospitalares;
- “Estado da arte” à época do procedimento (por exemplo, reconhecimento do CVS como padrão-ouro).
Se o cirurgião seguiu recomendações amplamente aceitas, é difícil sustentar que houve erro grosseiro, mesmo diante de complicação grave.
10. Dano, nexo causal e responsabilidade
Em termos médico-legais, três elementos precisam estar presentes para configurar responsabilidade civil:
- Ato ou omissão culposa (técnica inadequada, falta de diligência, ausência de informação).
- Dano (lesão de via biliar, perda de parte do fígado, invalidez, óbito).
- Nexo causal entre a conduta e o dano.
Exemplo:
– Lesão biliar reconhecida, adequadamente reparada em centro de referência, com boa evolução → pode ser entendida como complicação aceitável.
– Lesão ignorada, sem investigação, evoluindo para sepse e transplante → há forte argumento de falha na assistência.
11. Estratégias de prevenção médico-legal
Em linhas simples:
- Indique bem (indicação precisa e registrada).
- Faça CVS sempre que possível e saiba abandonar a dissecção perigosa.
- Use bailouts (subtotal, fundo–primeiro, conversão) quando necessário; não insista em anatomia impossível.
- Documente tudo (relatório detalhado, fotos/vídeos, evolução diária).
- Investigue sinais de complicação sem demora.
- Encaminhe cedo lesões complexas a centros de referência.
- Comunique com clareza e registre a conversa.
Essas medidas não apenas reduzem o risco de processo, mas principalmente melhoram o cuidado ao paciente, que é o objetivo central.
“O objetivo técnico principal na Colecistectomia, não é a retirada da vesícula biliar, mas proteger a via biliar principal.” Prof. Dr. Ozimo Gama
Hashtags (SEO)
#LesãoDeViaBiliar #ResponsabilidadeMédica #CirurgiaDigestiva #MedicinaLegal #CriticalViewOfSafety
Ambroise Paré (1510–1590): o Cirurgião que Não Sabia Latim
Introdução
Ambroise Paré é reconhecido como um dos pais da cirurgia moderna. Nascido em 1510, na pequena vila de Bourg-Hersent, próximo a Laval, na França, viveu em uma época de intensas transformações políticas, religiosas e científicas. Sem formação médica formal e sem domínio do latim — idioma obrigatório da ciência de seu tempo —, Paré rompeu barreiras sociais e acadêmicas para revolucionar a cirurgia com base em observação empírica, técnica precisa e humanidade.

Formação e Primeiros Anos no Hôtel-Dieu
Paré iniciou sua trajetória como aprendiz de cirurgião-barbeiro, profissão considerada de segunda classe em relação aos médicos da época. Em Paris, conseguiu, aos dezenove anos, ingressar no Hôtel-Dieu, o mais antigo hospital da cidade, onde se destacou pela habilidade manual e pela curiosidade científica. Nessa instituição, conviveu com feridos, queimados e amputados de guerra, experiências que moldaram sua prática futura. Posteriormente, serviu como cirurgião militar do exército francês nas campanhas da Itália entre 1536 e 1545, período em que faria suas descobertas mais marcantes.
A Descoberta do Tratamento das Feridas por Arma de Fogo
Até o século XVI, acreditava-se que as feridas por projéteis de pólvora eram envenenadas e deviam ser cauterizadas com ferro em brasa ou óleo fervente, conforme ensinava o cirurgião italiano Giovanni da Vigo. Durante uma campanha militar em 1536, Paré ficou sem óleo fervente e improvisou um curativo com gema de ovo, óleo de rosas e terebintina. Na manhã seguinte, observou que os pacientes tratados com essa mistura estavam tranquilos e com feridas limpas, enquanto os cauterizados sofriam febre e dor intensa. Esse acaso deu origem à primeira grande inovação de Paré: o abandono do cautério e do óleo fervente, substituídos por curativos mais suaves e fisiológicos — um avanço que reduziu a mortalidade e o sofrimento dos soldados.
A Ligadura das Artérias e a Hemostasia Moderna
Outro marco histórico atribuído a Paré é a introdução da ligadura de vasos sanguíneos nas amputações.
Até então, a hemostasia era obtida cauterizando os cotos com ferro em brasa — prática cruel e ineficaz. Em 1552, Paré começou a usar pinças e fios de seda para ligar os vasos, técnica descrita em seu livro Traité de la Chirurgie (1564). Ele também projetou instrumentos como o “Bec de Corbin” (“bico de corvo”), precursor dos hemostatos modernos. Esse método, apesar de rudimentar, representou a fundação da cirurgia vascular moderna e foi adotado em toda a Europa.
Reconhecimento Real e Ascensão Profissional
Graças à sua habilidade e serenidade, Paré ganhou prestígio na corte francesa. Serviu como cirurgião de quatro reis:
Henrique II, Francisco II, Carlos IX e Henrique III.
Após a morte trágica de Henrique II em 1559 — em consequência de um ferimento craniano durante um torneio, atendido por Paré e Vesalius —, ele foi nomeado primeiro cirurgião do rei por Carlos IX e posteriormente cirurgião real de Henrique III, o posto mais alto que um cirurgião poderia ocupar na França renascentista. Mesmo sem formação universitária e alvo de críticas por “não saber latim”, Paré foi admitido na Confraria de São Cosme, onde obteve o título de mestre em cirurgia, superando o preconceito dos médicos letrados.
Obras, Invenções e Contribuições
Em 1564, publicou Dix Livres de la Chirurgie, e em 1575 reuniu todos os seus trabalhos em 27 volumes sob o título Les Œuvres de M. Ambroise Paré.
Entre suas contribuições destacam-se:
- Introdução da ligadura arterial;
- Uso de curativos terapêuticos não cáusticos;
- Desenvolvimento de membros artificiais e próteses oculares de metal e porcelana;
- Observação pioneira do fenômeno do “membro fantasma” em amputados;
- Correlação entre sífilis e aneurisma da aorta;
- Reintrodução de técnicas obstétricas antigas (como a versão podálica);
- Abordagem crítica ao uso de “pó de múmia” como medicamento, prática supersticiosa comum na época.
Fé, Humanismo e Legado
Ambroise Paré viveu em meio às Guerras Religiosas da França e sobreviveu ao Massacre da Noite de São Bartolomeu (1572), protegido pelo rei Carlos IX. Embora simpatizante dos huguenotes (protestantes calvinistas), manteve-se oficialmente católico para evitar perseguições. Seu lema, inscrito em sua cadeira na Confraria de São Cosme, resumia sua filosofia médica:
“Je le pansai, Dieu le guérit.”
(Eu o tratei, mas Deus o curou.)
Faleceu em 1590, aos 80 anos, em Paris. Foi sepultado com honras, e um monumento em sua memória foi erguido em Laval, sua cidade natal.

Conclusão
Ambroise Paré foi mais do que um cirurgião: foi um símbolo da medicina humanista, que uniu técnica e compaixão em uma era de brutalidade. Seu trabalho elevou a cirurgia de ofício manual a disciplina científica, lançando as bases da prática moderna e do ensino cirúrgico. De aprendiz barbeiro a cirurgião real, Paré encarnou o ideal atemporal do médico-cientista movido por propósito, disciplina e fé.
“Há cinco deveres da cirurgia: remover o que é supérfluo, restaurar o que foi deslocado, separar o que cresceu junto, reunir o que foi dividido e corrigir as imperfeições da natureza.” — Ambroise Paré
#HistóriaDaCirurgia #AmbroisePare #CirurgiaModerna #EducaçãoMédicaContinuada #HumanismoMédico
Evolução da Cirurgia Abdominal: das Incisões à Robótica
Introdução
A cirurgia abdominal representa um dos campos mais transformadores da medicina moderna. Desde os primeiros relatos de intervenções rudimentares no Egito Antigo até os procedimentos laparoscópicos e robóticos do século XXI, essa especialidade foi moldada por uma combinação de coragem, ciência e inovação. Entender a evolução da cirurgia abdominal é compreender a trajetória do próprio raciocínio cirúrgico — da exploração empírica à precisão tecnológica.
Origens Antigas e Pré-Anestésicas
Os primeiros registros datam de cerca de 1500 a.C., com relatos de drenagens de abscessos e tentativas de reparo de ferimentos abdominais em papiros egípcios. Na Grécia Clássica, Hipócrates e Galeno descreveram técnicas rudimentares de incisão e sutura, mas a ausência de anestesia e controle infeccioso limitava qualquer intervenção intra-abdominal. Durante séculos, abrir o abdome equivalia a uma sentença de morte. A verdadeira revolução só viria com três marcos fundamentais: anestesia, antissepsia e hemóstase.
O Século XIX: O Nascimento da Cirurgia Moderna
Em 1846, William T. G. Morton realizou a primeira anestesia com éter no Massachusetts General Hospital, permitindo intervenções prolongadas sem sofrimento. Pouco depois, Joseph Lister introduziu o conceito de antissepsia (1867), reduzindo drasticamente a mortalidade pós-operatória. Esses avanços abriram caminho para a “era heroica” da cirurgia abdominal. Em 1881, Theodor Billroth executou a primeira gastrectomia parcial com sucesso, e Carl Langenbuch realizou a primeira colecistectomia (1882), marco fundador da cirurgia hepatobiliar moderna.
A partir daí, o abdome deixou de ser território proibido e tornou-se o novo campo de batalha da ciência médica.
O Século XX: Consolidação e Aperfeiçoamento Técnico
O século XX testemunhou a consolidação das grandes operações digestivas: Whipple descreveu sua pancreatoduodenectomia em 1935; Halsted refinou a técnica de sutura e as bases da cirurgia oncológica; e os avanços na anestesia inalatória e transfusão sanguínea tornaram procedimentos cada vez mais complexos possíveis. Após as guerras mundiais, o desenvolvimento da cirurgia vascular, hepática e de trauma foi impulsionado pelo atendimento de feridos, transferindo o aprendizado militar para os hospitais civis.
A Revolução Laparoscópica
Em 1987, o francês Philippe Mouret realizou a primeira colecistectomia laparoscópica, inaugurando a era da cirurgia minimamente invasiva. A visão endoscópica e o controle de pequenos instrumentos trouxeram redução de dor, tempo de internação e morbidade. A laparoscopia transformou não apenas a técnica, mas também a mentalidade cirúrgica — substituindo força por precisão, e exposição por visualização.
O Século XXI: A Era Robótica e da Inteligência Artificial
A introdução da cirurgia robótica no início dos anos 2000 levou o conceito de precisão a um novo patamar. O sistema da Vinci®, com movimentos articulados e visão tridimensional, ampliou a capacidade de dissecção em espaços confinados e redefiniu o ensino cirúrgico. Hoje, a inteligência artificial generativa começa a ser usada no planejamento operatório, simulação de complicações e análise de prognóstico, inaugurando uma nova fase da medicina baseada em dados e aprendizado automatizado.
Conclusão
A história da cirurgia abdominal é uma narrativa de disciplina e superação: de um ato de desespero tornou-se um gesto de ciência e compaixão. Cada avanço — da antissepsia à robótica — ampliou a margem de segurança e reduziu o sofrimento humano. Mais do que uma linha do tempo, é uma linha de coragem. E o futuro, inevitavelmente, será moldado pela integração entre o bisturi humano e a inteligência das máquinas.
“A cirurgia é o encontro entre a precisão da técnica e a grandeza do propósito humano.” — Adaptado de Harvey Cushing
#CirurgiaAbdominal #HistóriaDaMedicina #CirurgiaMinimamenteInvasiva #RobóticaCirúrgica #EducaçãoMédicaContinuada
Tríade Cirúrgica
Introdução
A cirurgia é, antes de tudo, uma escola de caráter. O domínio técnico é apenas uma das faces da formação do cirurgião; o verdadeiro diferencial está na capacidade de manter disciplina, cultivar resiliência e agir com propósito. Esses três pilares sustentam a excelência médica em um ambiente de pressão constante, decisões imediatas e responsabilidade sobre vidas humanas.
“O cirurgião é um soldado em tempo de paz: luta sem armas, vence sem glória e serve sem descanso.”
A Disciplina: A Arte da Constância
A disciplina é a virtude silenciosa que transforma talento em competência. Ela se manifesta nas pequenas rotinas diárias: revisar casos antes do plantão, estudar o que foi operado, cuidar dos detalhes do pós-operatório e seguir protocolos com rigor. Para o cirurgião, disciplina não é rigidez, mas constância inteligente. É o hábito de fazer o certo mesmo quando ninguém observa, o compromisso de preparar-se continuamente para o imprevisto. A disciplina cria confiança — no bisturi, na equipe e no paciente.
Sem disciplina, não há precisão; sem precisão, não há vitória. A disciplina do cirurgião é o equivalente à prontidão de combate: preparação constante, execução impecável e obediência rigorosa aos princípios da técnica e da ética.
A Resiliência: A Força que se Refaz
O caminho cirúrgico é inevitavelmente marcado por falhas, complicações e perdas. O cirurgião que não aprende a lidar com o insucesso corre o risco de se quebrar por dentro. A resiliência é a capacidade de aprender com o erro sem se paralisar, de suportar a frustração sem perder a ética, e de recomeçar com humildade e vigor. Mais do que resistir, o cirurgião resiliente se transforma. Ele reconhece a dor como instrumento de amadurecimento profissional e humano, e compreende que nenhuma cicatriz — seja no paciente, seja nele próprio — é em vão.
Toda missão tem perdas. Toda operação tem falhas. O cirurgião que não suporta a frustração é como o soldado que abandona o posto na primeira ofensiva. A resiliência é a blindagem emocional que permite ao médico enfrentar a adversidade, aprender com o erro e voltar mais forte. O cirurgião resiliente não nega a dor — ele a transforma em disciplina moral. Sabe que cada complicação é uma batalha perdida, mas não a guerra. Sabe que a autocrítica é o campo de treinamento da sabedoria.
O Propósito: O Norte que Sustenta a Jornada
Sem propósito, a técnica torna-se mecânica. O propósito é o eixo moral que dá sentido às longas horas de centro cirúrgico, às privações e às renúncias pessoais. Ele nasce do reconhecimento do valor da vida humana e da consciência de que cada ato cirúrgico é um gesto de confiança depositado pelo paciente. Trabalhar com propósito é lembrar-se diariamente de por que se escolheu operar — e não apenas de como se opera. É compreender que cada decisão impacta uma biografia, não apenas um prontuário.
O propósito é a bússola que guia o soldado e o cirurgião no caos. Sem ele, a técnica vira rotina, o bisturi vira arma e o ofício perde o sentido. O propósito é servir: servir à vida, à verdade e ao dever. É ele que dá coragem para entrar no centro cirúrgico às 3h da manhã, que sustenta o comando em meio à fadiga e que transforma o ato cirúrgico em missão.
Conclusão
Disciplina mantém o foco; resiliência sustenta o espírito; propósito dá direção.
Juntos, formam o tripé que sustenta o cirurgião diante da complexidade da vida moderna e da impermanência dos resultados.
Em um mundo que valoriza a pressa, o cirurgião deve cultivar o tempo — o tempo de estudar, de refletir, de cuidar e de evoluir. A grandeza profissional não se mede pelo número de cirurgias realizadas, mas pela qualidade humana com que cada uma é conduzida.
“A mão que opera deve ser firme; o coração que conduz, compassivo; e a mente que decide, disciplinada.”
#CirurgiaComPropósito #ResiliênciaMédica #DisciplinaCirúrgica #FormaçãoMédica #LiderançaNaSaúde
Neoadjuvância no Adenocarcinoma de Pâncreas: Evidências e Aplicações Clínicas
Introdução
O adenocarcinoma de pâncreas é uma das neoplasias mais agressivas do trato gastrointestinal, caracterizada por diagnóstico tardio, baixa ressecabilidade e alta taxa de recorrência. Apesar dos avanços técnicos e terapêuticos, a sobrevida global em 5 anos permanece inferior a 10%. A terapia neoadjuvante (quimioterapia com ou sem radioterapia antes da cirurgia) vem ganhando papel central, especialmente em tumores localmente avançados, borderline ressecáveis e, em casos selecionados, em tumores ressecáveis. Seu objetivo é tratar micrometástases precoces, aumentar taxas de ressecção R0 e selecionar pacientes com melhor biologia tumoral para cirurgia.
Racional da Neoadjuvância
- Controle sistêmico precoce: trata micrometástases antes da cirurgia.
- Seleção de pacientes: evita cirurgias em pacientes com progressão rápida da doença.
- Maior chance de completar quimioterapia: até 50% dos pacientes não recebem adjuvância após pancreatectomia devido à morbidade.
- Aumento da taxa de R0: margens negativas são fator prognóstico chave.
Evidências Recentes
- Borderline ressecável: ensaios mostram benefício claro. Regimes como FOLFIRINOX ou gemcitabina/nab-paclitaxel aumentam ressecabilidade e sobrevida global.
- Ressecáveis: ainda em estudo, mas meta-análises sugerem equivalência ou até superioridade em pacientes com alto risco prognóstico (ex.: CA 19-9 elevado).
- Radioterapia: pode melhorar controle local, mas seu papel isolado ainda é controverso.
O estudo PREOPANC (fase III, multicêntrico) demonstrou que quimiorradioterapia neoadjuvante não aumentou complicações maiores, fístula pancreática ou mortalidade pós-operatória, reforçando a segurança da estratégia.
Critérios para Indicar Neoadjuvância em Tumores Ressecáveis
- Marcadores de alto risco:
- CA 19-9 >150–250 U/mL
- Tumor ≥35 mm
- Albumina ≤3,5 g/dL
- Relação neutrófilo-linfócito ≥3,5
- Dupan-2 ≥750 U/mL
- Achados clínicos e radiológicos:
- Linfonodomegalia suspeita
- Invasão vascular incipiente
- Sinais sistêmicos de agressividade
- Preocupação com adesão ao adjuvante:
- Pacientes frágeis ou comorbidades que dificultem completar quimioterapia após cirurgia.
Taxa de Abandono da Neoadjuvância
- Varia entre 15–30% nos principais estudos.
- Motivos: toxicidade da quimioterapia, progressão tumoral, deterioração clínica ou recusa do paciente.
- Estratégia exige acompanhamento multidisciplinar próximo e suporte intensivo para reduzir perdas.
Segurança Cirúrgica
Estudos randomizados e coortes demonstram que a neoadjuvância não aumenta o risco de complicações pós-operatórias, incluindo fístula pancreática, infecção intra-abdominal e mortalidade hospitalar. Em alguns trabalhos, observou-se até redução da incidência de fístula pancreática clinicamente relevante.
Pontos-Chave para a Prática
- Padrão atual: recomendado em borderline ressecáveis.
- Ressecáveis: indicado em casos com fatores de alto risco.
- Regimes preferenciais: FOLFIRINOX (pacientes com bom performance status); gemcitabina/nab-paclitaxel em casos selecionados.
- Multidisciplinaridade é essencial: decisão deve envolver oncologia, cirurgia, radiologia e gastroenterologia.
Conclusão
A terapia neoadjuvante no adenocarcinoma de pâncreas representa um avanço significativo, transformando a abordagem tradicional baseada em cirurgia seguida de adjuvância. Atualmente, é padrão para tumores borderline ressecáveis, considerada em tumores ressecáveis com alto risco prognóstico, e investigada em ensaios clínicos como alternativa ao tratamento clássico. O futuro caminha para uma estratificação mais refinada baseada em biomarcadores, imagem funcional e resposta precoce ao tratamento, permitindo individualizar a neoadjuvância e maximizar o benefício oncológico.
“O futuro da cirurgia oncológica não é apenas retirar o tumor, mas entender a biologia da doença e intervir no momento certo.” — Veronesi
Gostou ❔ Nos deixe um comentário ✍️, compartilhe em suas redes sociais e|ou mande sua dúvida pelo 💬 Chat On-line em nossa DM do Instagram.
#PancreaticCancer #Neoadjuvância #OncologiaCirúrgica #CirurgiaDigestiva #EducaçãoMédicaContinuada
Inteligência Artificial & Apendicite Aguda
Uso da Inteligência Artificial Generativa no Diagnóstico, Tratamento Cirúrgico e Avaliação de Prognóstico da Apendicite Aguda
Introdução
A apendicite aguda continua sendo a causa mais comum de abdome agudo cirúrgico no mundo, com incidência estimada de 100 a 150 casos por 100.000 habitantes ao ano. No Brasil, representa uma das principais causas de internação cirúrgica no SUS. Apesar de amplamente estudada e com tratamento bem estabelecido, a apendicite aguda ainda apresenta desafios clínicos, como o diagnóstico precoce, a decisão operatória e a estratificação de risco de complicações. Nesse contexto, a Inteligência Artificial Generativa (IAG) emerge como uma tecnologia disruptiva com potencial transformador na abordagem cirúrgica dessa condição.
Diagnóstico com Apoio de IA Generativa
O diagnóstico precoce da apendicite aguda depende da correlação de dados clínicos, laboratoriais e de imagem. A IAG, treinada com grandes volumes de dados de prontuários eletrônicos, imagens de tomografia e ultrassonografias, pode sintetizar essas informações em tempo real para gerar hipóteses diagnósticas com acurácia comparável — e, em alguns casos, superior — à avaliação humana isolada. Modelos generativos baseados em deep learning, como os transformers, são capazes de identificar padrões sutis de apresentação clínica atípica, sobretudo em populações vulneráveis, como crianças pequenas, idosos e gestantes. Um exemplo prático é o uso de sistemas que combinam texto livre do prontuário com imagens de abdome para gerar relatórios diagnósticos automatizados e sugerir scores clínicos (como Alvarado ou AIR score) com ajuste probabilístico personalizado, auxiliando o cirurgião na tomada de decisão.
Tratamento Cirúrgico Guiado por IA
A cirurgia laparoscópica é o padrão ouro no tratamento da apendicite aguda, mas a escolha do momento cirúrgico e a abordagem ideal ainda são decisões dependentes da experiência do cirurgião e das condições clínicas do paciente. A IAG pode ser integrada a sistemas de suporte intraoperatório, auxiliando em navegação cirúrgica assistida por imagem, sugestão de condutas intraoperatórias com base em bancos de dados operatórios, e até mesmo em treinamento em simulações realistas de apendicectomia via realidade aumentada e modelos generativos de anatomia personalizada.
Em cenários de medicina robótica, já há estudos utilizando IA generativa para gerar “scripts” de procedimentos otimizados e oferecer feedback em tempo real com base em dados históricos de performance técnica — promovendo cirurgias mais seguras, rápidas e com menor taxa de complicações.
Avaliação Prognóstica com IA Generativa
A estratificação de risco no pós-operatório é outro campo onde a IAG pode oferecer avanços concretos. A partir de redes neurais treinadas em desfechos de milhares de pacientes com apendicite, esses modelos podem prever probabilidades de complicações como abscesso residual, íleo paralítico ou necessidade de reabordagem, considerando variáveis clínicas, laboratoriais, intraoperatórias e demográficas. Além disso, ferramentas baseadas em IA podem gerar relatórios individualizados de prognóstico funcional, tempo estimado de retorno às atividades e risco de reinternação, permitindo ao cirurgião personalizar o plano de alta, acompanhamento ambulatorial e orientações ao paciente com maior precisão.
Pontos-Chave
- A IA generativa tem capacidade de analisar simultaneamente dados clínicos, laboratoriais e de imagem para melhorar o diagnóstico precoce da apendicite aguda.
- Pode ser integrada à decisão cirúrgica, tanto no pré quanto no intraoperatório, por meio de simulação, navegação assistida e análise de performance técnica.
- Modelos preditivos baseados em IA oferecem ferramentas objetivas para prognóstico pós-operatório personalizado, otimizando o seguimento do paciente.
- O uso de IAG deve ser encarado como ferramenta complementar ao raciocínio clínico do cirurgião, jamais como substituto da experiência e do julgamento médico.
- O avanço dessas tecnologias requer formação crítica e ética dos futuros cirurgiões, capacitando-os para liderar a incorporação segura e eficaz dessas ferramentas na prática assistencial.
Conclusão
A incorporação da Inteligência Artificial Generativa na cirurgia do aparelho digestivo representa um novo paradigma na medicina personalizada, baseada em dados e centrada no paciente. No caso da apendicite aguda — uma das mais frequentes emergências cirúrgicas —, o uso responsável e crítico da IAG pode aprimorar significativamente os pilares do cuidado: diagnóstico, decisão operatória e prognóstico. O cirurgião do futuro será, acima de tudo, um líder clínico capaz de integrar inteligência humana e artificial com sabedoria e discernimento ético.
“A tecnologia não substitui o cirurgião. Ela amplia sua visão, mas é o julgamento humano que decide a incisão.” — Sir John Black, ex-presidente do Royal College of Surgeons
Gostou ❔ Nos deixe um comentário ✍️, compartilhe em suas redes sociais e|ou mande sua dúvida pelo 💬 Chat On-line em nossa DM do Instagram.
#InteligenciaArtificialNaMedicina #CirurgiaDoAparelhoDigestivo #ApendiciteAguda #DiagnósticoComIA #CirurgiaGuiadaPorDados
O Bisturi
Ele é longo e pontudo.
Não precisa ser afiado —
em sua forma reside
a perfeição. Um instrumento
para penetrar de um modo
limpo e preciso.
Seja em um corte
no flanco, nas costas
ou atravessando
tecidos delicados,
seu efeito é vital.
Na mão do cirurgião,
não traz a morte,
mas a cura:
ferida que sara,
toque que liberta,
anatomia exata
entre a mão e a vida.
Fundamentos Filosóficos da Prática Cirúrgica Contemporânea
Reflexões para Cirurgiões do Aparelho Digestivo

Introdução
A conexão entre cirurgia e filosofia vai além da prática técnica, envolvendo uma reflexão profunda sobre os impactos éticos e humanos da profissão. Inspirado pela obra de Yves Chapuis e por grandes pensadores como Sócrates e Heidegger, este artigo examina como fundamentos filosóficos moldam a prática cirúrgica contemporânea, especialmente na cirurgia do aparelho digestivo, propondo um diálogo entre técnica, ética e humanização. A prática cirúrgica exige mais do que habilidade técnica. Ela demanda do cirurgião um compromisso ético, psicológico e social. Exploramos aqui 10 tópicos que integram esses fundamentos, demonstrando sua relevância na cirurgia digestiva:
Aplicação na Cirurgia Digestiva: 10 Tópicos Fundamentais
- Cirurgia e Filosofia
A filosofia aplicada à cirurgia busca compreender as causas primeiras e os valores humanos. A prática cirúrgica, enquanto combate às doenças, exige reflexão sobre o impacto dos atos no paciente e na sociedade, alinhando técnica e moralidade. - Indignação como Ponto de Partida
Chapuis, ecoando Sócrates e Heidegger, destaca a indignação diante do sofrimento humano como o motor da filosofia e, por extensão, da cirurgia. O cirurgião não apenas observa, mas age para transformar a realidade, aliviando a dor e restaurando a dignidade. - Aspecto Moral da Cirurgia
O avanço técnico amplia as possibilidades terapêuticas, mas exige maior responsabilidade ética. Como afirmou Ollier: “Quanto mais poderosa a cirurgia se torna, mais moral ela deve ser.” No Brasil, isso é crucial para lidar com as disparidades no acesso a procedimentos como transplantes hepáticos. - Perigos da Supremacia Técnica
A dependência excessiva da tecnologia pode desumanizar a prática. Como alertou Jean-François Mattei: “Se o médico dedica mais tempo ao seu computador do que ao seu paciente, algo está errado.” O foco deve permanecer no paciente, não apenas na doença. - Desafios Psicológicos do Cirurgião
O desgaste emocional, a monotonia e a pressão social afetam a saúde mental dos cirurgiões. Reflexões regulares sobre os desafios enfrentados podem ajudar a equilibrar a prática com o bem-estar pessoal. - Necessidade de Adaptação e Aprendizado Contínuo
A resistência às mudanças limita o progresso. Para enfrentar as inovações como a laparoscopia ou a robótica, é necessário um aprendizado constante e uma mente aberta, valorizando o impacto positivo dessas técnicas no tratamento de doenças como câncer gástrico. - Dimensão Coletiva e Social
A prática cirúrgica não é isolada, mas afeta diretamente o acesso aos cuidados de saúde. No Brasil, regiões periféricas sofrem com a falta de infraestrutura e profissionais qualificados, destacando a necessidade de políticas públicas mais inclusivas. - Responsabilidade com o Corpo e o Tempo
A íntima relação do cirurgião com o corpo humano é única. Como reflete Saint Augustin: “Se você não me pergunta o que é o tempo, eu sei o que ele é; mas, assim que você me pergunta, eu já não sei mais.” O tempo dedicado ao paciente, muitas vezes negligenciado, é um reflexo do compromisso ético e técnico do cirurgião. - Confronto com a Morte
A cirurgia é uma batalha constante contra a morte. Valéry define-a como “Combater o mal com as próprias mãos armadas.”, enquanto Bichat a vê como “Destruir as forças que se opõem à vida” Este enfrentamento exige equilíbrio entre ousadia terapêutica e limites éticos. - Desafios Futuros com a Genética
Avanços na genética trazem novos dilemas, como intervenções preventivas em indivíduos predispostos a doenças digestivas. A antecipação ética e a relação de confiança com o paciente tornam-se ainda mais importantes.
Pontos-Chave
- Humanização: A cirurgia é uma prática que conecta técnica e cuidado humano.
- Ética e Progresso: Avanços devem ser acompanhados de responsabilidade moral.
- Educação e Reflexão: Cirurgiões precisam de constante aprendizado e autocrítica.
- Desafios Brasileiros: A desigualdade regional exige ações concretas para ampliar o acesso.
- Sustentabilidade e Futuro: A integração de novas tecnologias deve considerar a realidade socioeconômica.
Conclusões
A prática cirúrgica contemporânea requer dos profissionais uma abordagem que mescle técnica, ética e reflexão filosófica. Inspirados por Chapuis, podemos construir um modelo que priorize o paciente, enfrente desigualdades e avance de forma responsável. A cirurgia do aparelho digestivo, com seus desafios únicos, é um campo que exemplifica essa necessidade de equilíbrio.
Como disse René Leriche:
“Todo cirurgião carrega consigo um cemitério, ao qual ele deve voltar de tempos em tempos para meditar.”
Gostou ❔Nos deixe um comentário ✍️, compartilhe em suas redes sociais e|ou mande sua dúvida pelo 💬 Chat On-line em nossa DM do Instagram.
#CirurgiaDigestiva #FilosofiaNaMedicina #HumanizaçãoNaSaúde #InovaçãoCirúrgica #EducaçãoMédica

Colecistectomia Robótica
A colecistectomia, procedimento cirúrgico para remoção da vesícula biliar, pode ser realizada por diferentes abordagens, sendo as mais comuns a via laparoscópica (1985), a assistida por robô (1987) e a cirurgia convencional ou aberta (1882). Cada uma dessas técnicas tem vantagens e desvantagens em termos de custo, eficácia clínica e complexidade, o que torna a análise de custo-efetividade crucial para a escolha da abordagem mais adequada em cada caso.
Colecistectomia Laparoscópica (CVL)
A colecistectomia laparoscópica (CVL) é amplamente reconhecida como a técnica de escolha devido à sua eficácia, recuperação rápida e menor custo comparado a outras abordagens. Diversos estudos confirmam que a laparoscopia é a opção mais custo-efetiva para a maioria dos pacientes com doenças benignas da vesícula biliar, como a colelitíase, devido ao menor custo direto das etapas cirúrgicas.
Estudos de Custo-efetividade indicam que o custo variável direto para o cirurgião na execução de uma colecistectomia laparoscópica foi significativamente inferior ao de técnicas mais complexas. A via laparoscópica custou, em média, $929, enquanto a colecistectomia assistida por robô (ROBOSILS) alcançou o custo de $2,608. Isso demonstra que a laparoscopia tem uma vantagem substancial em termos de custo sem comprometer a qualidade do procedimento.
Colecistectomia Robótica
Por outro lado, a colecistectomia assistida por robô tem ganhado popularidade devido à promessa de maior precisão, visualização e controle durante a cirurgia. No entanto, sua viabilidade econômica tem sido amplamente discutida na literatura, com estudos demonstrando que, embora seja uma técnica segura, os custos hospitalares associados a ela são consideravelmente mais altos. Em um estudo de caso-controle, os custos totais hospitalares para a cirurgia robótica foram de $7,985.4, em comparação com $6,255.3 para a laparoscopia. A maior parte desses custos adicionais vem dos gastos com a amortização e os consumíveis do sistema robótico, que são significativamente mais caros. Outra análise revelou uma razão de custo-efetividade da cirurgia robótica de $1,795,735.21 por ano de vida ajustado pela qualidade, um valor muito acima dos limiares aceitáveis para a maioria dos sistemas de saúde. Além disso, um banco de dados nacional demonstrou que, enquanto a colecistectomia robótica pode oferecer benefícios como redução do tempo de internação, os custos globais continuam elevados devido aos custos variáveis e consumíveis associados ao uso da tecnologia robótica, fazendo com que essa técnica não seja necessariamente mais custo-efetiva, mesmo em contextos que poderiam sugerir vantagens clínicas.
Colecistectomia Convencional ou Abertia (Via Laparotômica)
A colecistectomia convencional, ou aberta, apresenta indicações específicas, sendo geralmente reservada para situações onde a abordagem laparoscópica não oferece segurança ou viabilidade adequada. Esta modalidade cirúrgica encontra suas principais indicações em casos de inflamação severa, particularmente na colecistite aguda complicada, onde o risco de complicações durante a laparoscopia se mostra elevado, bem como em pacientes com histórico de múltiplas intervenções abdominais prévias que resultaram em aderências extensas. A suspeita de malignidade da vesícula biliar também constitui indicação relevante para a abordagem aberta, dada a necessidade de acesso mais amplo para ressecção e avaliação adequada. Ademais, pacientes com condições médicas que contraindicam anestesia geral prolongada ou que apresentam comorbidades significativas com elevado risco cirúrgico podem ser considerados candidatos à abordagem convencional, especialmente quando se antecipa a possibilidade de conversão do procedimento laparoscópico. Em determinados grupos, como idosos ou portadores de hepatopatias avançadas, a escolha entre as abordagens laparoscópica e aberta demanda análise criteriosa, ponderando-se riscos e benefícios específicos de cada caso. Desta forma, a colecistectomia convencional mantém-se como opção cirúrgica fundamental para casos complexos ou de alto risco, nos quais a segurança do paciente constitui o principal determinante da escolha terapêutica.
Indicando a Melhor Abordagem para o Paciente
A escolha da abordagem cirúrgica para a colecistectomia pode ser influenciada por uma série de fatores, incluindo a condição clínica do paciente, as características da doença e os custos. A colecistectomia laparoscópica continua sendo a técnica de escolha para a maioria dos pacientes com doenças benignas da vesícula biliar devido à sua eficácia comprovada e menor custo. Além disso, estudos sugerem que a colecistectomia robótica pode ser considerada em casos específicos, como:
- Pacientes com doença hepática avançada, onde a probabilidade de conversão para cirurgia aberta é menor e o tempo de internação é reduzido.
- Contextos de treinamento cirúrgico, onde a precisão e a visualização aprimorada podem ser cruciais.
No entanto, mesmo nesses casos, é importante ponderar os custos adicionais envolvidos e os benefícios clínicos específicos que a cirurgia robótica pode oferecer, considerando que, em geral, as vantagens não são suficientes para justificar o alto custo.
Considerações Finais sobre a Abordagem Convencional e Robótica
Embora a colecistectomia robótica tenha algumas vantagens técnicas, ela não é superior em termos de desfechos clínicos quando comparada à laparoscopia, o que faz com que a escolha por esta última, em termos de custo-benefício, seja preferível na grande maioria dos casos. A colecistectomia laparoscópica oferece uma recuperação mais rápida, menor dor pós-operatória, menos complicações e melhores resultados estéticos, com menor tempo de internação. Além disso, a técnica laparoscópica convencional tem uma mortalidade operatória baixa e um risco de lesão do ducto biliar de aproximadamente 0,5%, valor que é três vezes maior que o encontrado na cirurgia aberta. Por outro lado, a colecistectomia robótica tem se mostrado vantajosa apenas em contextos específicos, como na redução da taxa de conversão para cirurgia aberta em colecistite aguda. Contudo, o risco aumentado de lesões do ducto biliar com a abordagem robótica é uma preocupação adicional que deve ser considerada.
Conclusão
Em resumo, enquanto a colecistectomia laparoscópica continua sendo a técnica de escolha padrão devido ao seu custo-benefício superior e resultados clínicos satisfatórios, a colecistectomia assistida por robô pode ser útil em casos específicos, como doença hepática avançada ou treinamento cirúrgico. No entanto, os custos elevados da técnica robótica não são amplamente justificados por melhorias nos desfechos clínicos, o que reforça a técnica laparoscópica como a abordagem mais custo-efetiva para a maioria dos pacientes.
Pontos-Chave
- Colecistectomia Convencional : Esta técnica é indicada em casos onde a abordagem minimamente invasiva não é viável, como em colecistite aguda complicada com fistulizações ou em pacientes com histórico de múltiplas cirurgias abdominais por laparotomia. No Brasil, cerca de 10% das colecistectomias ainda são realizadas de maneira convencional, de acordo com dados do DATASUS. O procedimento por via convencional apresenta uma taxa de complicações como lesão do ducto biliar em torno de 0.15%, porém, vem com um período de recuperação mais prolongado e uma maior dor pós-operatória.
- Colecistectomia Laparoscópica: Tornou-se o padrão-ouro para a maioria dos casos devido à sua menor invasividade, resultando em menor tempo de hospitalização e recuperação mais rápida. Estudos indicam que no Brasil, aproximadamente 90% das colecistectomias são laparoscópicas. No entanto, a laparoscopia ainda carrega um risco de lesão do ducto biliar que, embora baixo (cerca de 0.5%), é três vezes maior do que na técnica aberta.
- Colecistectomia Robótica: Oferece precisão e visualização 3D, mas com um custo significativamente mais alto. Dados recentes no Brasil mostram que a prática da cirurgia robótica está crescendo, embora ainda seja limitada devido ao custo e disponibilidade de equipamentos. A técnica robótica pode reduzir a necessidade de conversão para cirurgia aberta em pacientes com condições hepáticas complicadas, mas a incidência de lesão do ducto biliar é potencialmente maior, chegando a ser até 5 vezes mais alta do que na laparoscopia, segundo alguns estudos.
Aplicação na Cirurgia Digestiva
A escolha da técnica deve ser baseada na condição do paciente, na expertise do cirurgião e na disponibilidade de recursos. No contexto brasileiro, onde o acesso a tecnologia de ponta pode ser desigual, a laparoscopia tem sido a escolha preferencial por equilibrar custo e eficácia. Entretanto, a cirurgia robótica pode ser considerada em cenários específicos, como em pacientes com doença hepática avançada ou em instituições com investimento em tecnologia robótica.
- Custo: Laparoscópica < Convencional < Robótica.
- Segurança: Convencional e Laparoscópica com taxas comparáveis de complicações, embora com diferentes perfis de risco.
- Eficácia: Todas as técnicas são eficazes, mas a laparoscópica é a mais custo-efetiva para a maioria dos casos.
- Recuperação: Laparoscópica e Robótica oferecem recuperação mais rápida.
“Nós cirurgiões devemos compreender que a tecnologia é meramente um instrumento, não uma solução milagrosa, e sua aplicação deve ser ponderada com cautela, levando em conta o equilíbrio entre segurança, desfechos clínicos e custos assistenciais.”
Gostou ❔ Nos deixe um comentário ✍️, compartilhe em suas redes sociais e|ou mande sua dúvida pelo 💬 Chat On-line em nossa DM do Instagram.
Hashtags:
#Colecistectomia #Laparoscopia #CirurgiaRobótica #CustoEfetividade #SaúdeDigestiva
Qual a função do Apêndice Vermiforme?
Da Teoria Vestigial ao Protagonismo Imunológico e Microbiológico
Autor: Prof. Dr. Ozimo Gama (Tempo de Leitura: 12 minutos)

Introdução
Durante mais de um século, o apêndice vermiforme foi relegado ao status de um mero resquício evolutivo — um órgão vestigial, desprovido de função e célebre apenas pela sua capacidade de inflamar e exigir intervenção cirúrgica de urgência. No entanto, a medicina baseada em evidências e a compreensão profunda do trato gastrointestinal reescreveram esta narrativa. Longe de ser uma “sobra” anatômica, o apêndice é hoje reconhecido como uma estrutura morfofuncional de extrema relevância, atuando ativamente na imunidade mucosal e na regulação do microbioma intestinal. Para o estudante de medicina, o residente e o cirurgião do aparelho digestivo, compreender a anatomia, a fisiologia e o impacto a longo prazo da ressecção deste pequeno órgão tubular é fundamental para aprimorar o raciocínio clínico e refinar as indicações terapêuticas perante a suspeita de um abdome agudo inflamatório.
A Anatomia Cirúrgica do Apêndice
O conhecimento anatômico do apêndice é o mapa que guia o bisturi (ou o trocarte) na sala de operações.
1. Morfologia e Topografia
O apêndice vermiforme é uma projeção tubular cega que se origina na confluência das tênias colônicas, no ceco. Seu comprimento varia de 5 a 25 cm (média de 10 cm). Sua localização típica é na fossa ilíaca direita, topografada na superfície abdominal pelo ponto de McBurney (terço externo da linha imaginária entre a espinha ilíaca anterossuperior direita e a cicatriz umbilical). Contudo, a ponta do apêndice é como o ponteiro de um relógio, assumindo diversas posições:
- Retrocecal (mais comum – aprox. 65%): Oculto atrás do ceco, frequentemente simulando afecções renais ou dificultando o diagnóstico de peritonite precoce.
- Pélvico (aprox. 30%): Pode irritar a bexiga ou anexos uterinos.
- Subcecal, Pré ou Pós-ileal.
- Nota Cirúrgica: Em casos raros de má rotação intestinal ou situs inversus, o apêndice pode estar localizado no quadrante inferior esquerdo.
2. Vascularização e Inervação
A irrigação provém da artéria apendicular, um ramo terminal da artéria ileocólica (ramo da mesentérica superior), que transita na borda livre do mesoapêndice. Por ser uma artéria terminal, a oclusão da luz apendicular (por um fecalito) gera rápido ingurgitamento, trombose, isquemia e, subsequentemente, necrose e perfuração. A inervação, oriunda do plexo mesentérico superior (T10), explica a evolução clássica da dor na apendicite aguda: inicialmente dor visceral, difusa e periumbilical; que, com a progressão da inflamação para o peritônio parietal (inervação somática), migra e se localiza na fossa ilíaca direita.
A Mudança de Paradigma: Funções Funcionais (Microbioma e Imunidade)
A verdadeira revolução na compreensão do apêndice ocorreu no campo da imunologia e da microbiologia.
O “Refúgio Seguríssimo” (Safe House) do Microbioma
A mucosa apendicular é rica em biofilmes e serve como um autêntico “cofre” para as bactérias comensais (benéficas) do intestino. Durante infecções gastrointestinais severas, que resultam em diarreia profusa e “lavagem” da flora cólica, o apêndice mantém um reservatório seguro destas bactérias. Uma vez cessado o quadro agudo, este reservatório é utilizado para repovoar o cólon, restaurando a homeostase do microbioma de forma acelerada.
O Campo de Treinamento Imunológico
O apêndice é um componente vital do GALT (Gut-Associated Lymphoid Tissue). Ele contém uma densa rede de folículos linfoides e células M especializadas. Estas células capturam antígenos luminais e os apresentam aos linfócitos (Células T e B), orquestrando a resposta imune local (produção de IgA) e sistêmica. O apêndice atua como um órgão linfoide primário no desenvolvimento inicial e como um sentinela imune na vida adulta.
Aplicação na Cirurgia Digestiva e Implicações Clínicas
A apendicectomia continua sendo o procedimento cirúrgico de urgência mais realizado no mundo. Contudo, a ablação deste órgão carrega repercussões que a cirurgia moderna não pode mais ignorar.
1. Implicações da Apendicectomia a Longo Prazo
A remoção da “base de treinamento” imune e do reservatório microbiano altera a fisiologia intestinal. Estudos epidemiológicos recentes sugerem que a apendicectomia pode estar associada a um risco aumentado de desenvolvimento de:
- Síndrome do Intestino Irritável (SII): Devido à disbiose crônica (redução de bactérias protetoras, como o Butyricicoccus).
- Doenças Metabólicas e Autoimunes: Modulações na tolerância imunológica têm sido correlacionadas com maior incidência de Diabetes Mellitus tipo 2 e Lúpus.
- Risco Oncológico: Embora ainda exija mais robustez estatística, algumas coortes sugerem que a perda da vigilância imunológica (redução de células T CD3+ e CD8+ induzidas pelo apêndice) possa ter um papel na carcinogênese colorretal.
2. O Debate Contemporâneo: Cirurgia vs. Antibioticoterapia
Dado o seu papel funcional, extirpar o apêndice profilaticamente ou ao menor sinal de dor já não é consenso absoluto. A literatura recente, notavelmente o estudo CODA publicado no New England Journal of Medicine (NEJM, 2020), demonstrou que a antibioticoterapia exclusiva pode ser uma alternativa segura e eficaz em casos selecionados de apendicite aguda não complicada, evitando a cirurgia e preservando o órgão em uma parcela significativa dos pacientes. Cabe ao cirurgião avaliar criteriosamente a presença de fecalitos (que predizem falha do tratamento clínico) e o risco de ruptura.
Pontos-Chave para a Prática Diária
- Não é Vestigial: O apêndice é um órgão linfoide ativo e um modulador essencial do microbioma e da imunidade mucosal.
- A Anatomia Dita a Clínica: A variação na posição da ponta do apêndice (retrocecal, pélvica) é a principal causa de apresentações clínicas atípicas que atrasam o diagnóstico cirúrgico.
- A Isquemia é Precoce: Por ser irrigado por uma artéria terminal (a. apendicular), a obstrução luminal rapidamente evolui para gangrena e perfuração se não diagnosticada.
- Reservatório Protetor: O apêndice atua como um “safe house” bacteriano, acelerando a recuperação do cólon após infecções entéricas severas.
- Apendicectomia tem Preço Fisiológico: A remoção não é isenta de consequências a longo prazo, predispondo a disbiose, SII e possíveis disfunções imunológicas.
- Tratamento Conservador: O manejo não operatório com antibióticos da apendicite não complicada é uma realidade baseada em evidências que deve constar no arsenal terapêutico do cirurgião moderno.
Conclusões Aplicadas à Prática do Cirurgião Digestivo
A apendicectomia — preferencialmente por via laparoscópica — permanecerá como o esteio do tratamento da apendicite aguda, salvando inúmeras vidas de peritonites letais. No entanto, o cirurgião do aparelho digestivo do século XXI deve abandonar a visão mecanicista e adotar uma perspectiva fisiológica. Considerar o tratamento antimicrobiano exclusivo em casos iniciais e não complicados não é uma heresia cirúrgica, mas sim o reconhecimento do valor morfofuncional do apêndice. Além disso, a vigilância clínica a longo prazo dos pacientes apendicectomizados, monitorando o desenvolvimento de disbiose ou patologias colorretais, deve ser encorajada. Conhecer a fundo a biologia daquilo que operamos é o que separa o mero “operador” do verdadeiro médico cirurgião.
A Anatomia Cirúrgica do Apêndice
O conhecimento anatômico do apêndice é o mapa que guia o bisturi (ou o trocarte) na sala de operações.
1. Morfologia e Topografia
O apêndice vermiforme é uma projeção tubular cega que se origina na confluência das tênias colônicas, no ceco. Seu comprimento varia de 5 a 25 cm (média de 10 cm). Sua localização típica é na fossa ilíaca direita, topografada na superfície abdominal pelo ponto de McBurney (terço externo da linha imaginária entre a espinha ilíaca anterossuperior direita e a cicatriz umbilical). Contudo, a ponta do apêndice é como o ponteiro de um relógio, assumindo diversas posições:
- Retrocecal (mais comum – aprox. 65%): Oculto atrás do ceco, frequentemente simulando afecções renais ou dificultando o diagnóstico de peritonite precoce.
- Pélvico (aprox. 30%): Pode irritar a bexiga ou anexos uterinos.
- Subcecal, Pré ou Pós-ileal.
- Nota Cirúrgica: Em casos raros de má rotação intestinal ou situs inversus, o apêndice pode estar localizado no quadrante inferior esquerdo.
2. Vascularização e Inervação
A irrigação provém da artéria apendicular, um ramo terminal da artéria ileocólica (ramo da mesentérica superior), que transita na borda livre do mesoapêndice. Por ser uma artéria terminal, a oclusão da luz apendicular (por um fecalito) gera rápido ingurgitamento, trombose, isquemia e, subsequentemente, necrose e perfuração. A inervação, oriunda do plexo mesentérico superior (T10), explica a evolução clássica da dor na apendicite aguda: inicialmente dor visceral, difusa e periumbilical; que, com a progressão da inflamação para o peritônio parietal (inervação somática), migra e se localiza na fossa ilíaca direita.
3. Resumo Prático da Anatomia Apendicular
Para uma consulta rápida e direcionada à prática cirúrgica, eis a síntese estrutural do apêndice:
- Forma e Dimensões: Estrutura tubular cega, medindo em média 10 cm de comprimento.
- Base Anatômica: Origina-se invariavelmente na confluência das três tênias colônicas no ceco.
- Posição da Ponta: Mais frequentemente retrocecal (65%) ou pélvica (30%).
- Referência de Superfície: Ponto de McBurney (fossa ilíaca direita).
- Irrigação Sanguínea: Artéria apendicular (artéria terminal; o que favorece isquemia precoce em casos de obstrução).
- Inervação Autonômica: Segmento T10, justificando a dor periumbilical referida na fase inicial da inflamação.
“A medicina é uma arte, não uma ciência exata.” — William Osler. A compreensão contínua das funções do apêndice e a evolução das abordagens terapêuticas refletem a natureza dinâmica da prática médica, onde novas evidências moldam as decisões clínicas e cirúrgicas.
Gostou ❔Nos deixe um comentário ✍️, compartilhe em suas redes sociais e|ou mande sua dúvida pelo 💬 Chat On-line em nossa DM do Instagram.
A Medicina que Salva
Ética, Ciência e Humanismo no Tratamento Cirúrgico das Doenças do Aparelho Digestivo.
Introdução
A prática médica moderna, especialmente no campo da cirurgia do aparelho digestivo, está ancorada no progresso científico e na inovação tecnológica. Contudo, a essência da medicina não reside apenas nos avanços técnicos, mas na aplicação ética e humanística do conhecimento para aliviar o sofrimento humano. C.S. Lewis, conhecido por sua contribuição literária e teológica, trouxe à luz princípios que, mesmo fora do contexto médico, iluminam os fundamentos éticos e morais que sustentam a arte de curar. Este artigo analisa como esses princípios podem ser aplicados à prática cirúrgica, destacando a importância de integrar ciência e humanidade na busca pela cura.
Desenvolvimento
A Importância da Imaginação na Medicina
A imaginação é uma ponte essencial para alcançar verdades profundas. Na cirurgia digestiva, a imaginação é fundamental para visualizar soluções complexas, como planejar abordagens minimamente invasivas ou interpretar imagens radiológicas de maneira criativa para encontrar o melhor caminho terapêutico. A capacidade de “ver além” permite ao cirurgião inovar e adaptar-se às necessidades do paciente.
Moralidade Objetiva e Decisões Médicas
O tratamento cirúrgico é uma terapêutica universal, aplicável a todos quando indicada. Na medicina, isso se traduz através da ética profissional, que guia decisões difíceis, como quando ponderar entre tratamentos curativos e paliativos. O respeito pela dignidade humana é um pilar que sustenta essas escolhas, especialmente na oncologia digestiva.
Sacrifício e Redenção no Cuidado com o Paciente
O sacrifício de Aslan em O Leão, a Feiticeira e o Guarda-Roupa reflete o compromisso cirúrgico com a entrega pessoal. A medicina exige sacrifícios diários, desde longas horas de trabalho até decisões que podem impactar emocionalmente. A redenção ocorre quando o esforço resulta em salvar vidas ou proporcionar conforto a quem sofre.
O Conflito Entre Bem e Mal nas Escolhas Terapêuticas
A luta entre bem e mal se manifesta diariamente na medicina, onde o cirurgião enfrenta dilemas éticos, como a aplicação de tecnologias avançadas em contextos que podem beneficiar ou prejudicar pacientes. O nosso compromisso com o bem-estar do paciente deve ser o norteador.
A Alegria como Reflexo da Cura
A alegria é um vislumbre do divino. Na cirurgia digestiva, a alegria está presente em momentos simples, como ver um paciente se recuperar após uma colectomia ou uma gastrectomia bem-sucedida. Esses momentos dão sentido ao trabalho árduo e reforçam a missão do cirurgião.
Humildade e Aprendizado Contínuo
A humildade, um valor essencial para Lewis, é igualmente crucial para o cirurgião. Reconhecer limitações, buscar aprendizado contínuo e valorizar o trabalho em equipe são atitudes que fortalecem a prática médica.
A Eternidade e o Impacto das Escolhas Médicas
Cada escolha cirúrgica tem um impacto que transcende o momento imediato, pois todos os seres humanos têm um valor eterno. O respeito a essa visão confere à medicina um caráter sagrado, onde cada paciente é tratado como único.
Fé e Razão na Tomada de Decisão
A fé e a razão não são antagônicas. Na medicina, a razão científica é enriquecida pela fé no potencial humano e no desejo de servir ao próximo, formando uma abordagem holística no cuidado.
Pequenos Gestos, Grandes Impactos
A clínica cirúrgica é enriquecida por atos simples de bondade. Para o cirurgião digestivo, isso pode significar ouvir atentamente as preocupações de um paciente ou explicar detalhadamente um procedimento. Pequenos gestos constroem confiança e humanizam a prática médica.
Livre-Arbítrio e Responsabilidade
Assim como o livre-arbítrio é central para o Cristianismo, a responsabilidade é uma constante na medicina. Cada decisão do cirurgião, desde indicar uma laparotomia exploratória até manejar complicações, deve ser guiada pela prudência e pela ética.
Aplicação na Cirurgia Digestiva Contemporânea
No contexto atual, a prática cirúrgica do aparelho digestivo enfrenta desafios complexos, como o tratamento de doenças oncológicas, o avanço da cirurgia robótica e a integração de abordagens multidisciplinares. Os princípios de C.S. Lewis reforçam a necessidade de alinhar o progresso científico com a compaixão, criando uma medicina que salva não apenas corpos, mas também pode ajudar a restaurar as almas – dos profissionais e dos pacientes.
Exemplos práticos incluem:
- A Ética na Cirurgia Bariátrica: Equilibrar a necessidade de ajudar o paciente com obesidade mórbida e o respeito à autonomia.
- A Inovação no Tratamento de Tumores Digestivos: Usar avanços como a ablação por radiofrequência com responsabilidade, priorizando o benefício do paciente.
- Humanização no Pós-Operatório: Incorporar cuidados centrados no paciente, promovendo recuperação emocional além da física.
Pontos-Chave
- A imaginação e a criatividade são indispensáveis para solucionar problemas médicos.
- Decisões éticas devem ser baseadas em uma moralidade universal que respeite a dignidade humana.
- A prática médica exige sacrifício pessoal e uma visão humanística do cuidado.
- A integração de fé e razão fortalece a abordagem holística no tratamento.
- Pequenos gestos de bondade humanizam a relação médico-paciente.
Conclusões Aplicadas à Prática do Cirurgião Digestivo
A prática da cirurgia do aparelho digestivo deve transcender a técnica, fundamentando-se nos princípios éticos e humanísticos que fizeram da medicina uma vocação sagrada. Inspirados pelos ensinamentos de C.S. Lewis, os cirurgiões podem abraçar uma abordagem que une ciência e compaixão, transformando a cirurgia em uma “medicina que salva” na mais ampla acepção.
“Você nunca encontrará um ser humano comum. Nunca conversou com um mero mortal.” — C.S. Lewis
Gostou❔ Nos deixe um comentário ✍️, compartilhe em suas redes sociais e/ou mande sua dúvida pelo 💬 Chat On-line em nossa DM do Instagram.
Hashtags
#MedicinaHumanista #CirurgiaDigestiva #EducaçãoMédica #ÉticaNaMedicina #MedicinaQueSalva
História da Anatomia Humana
A palestra “Fundamentos Históricos da Anatomia Humana” traça a evolução do estudo da anatomia desde a pré-história até a era moderna. A apresentação destaca a importância de figuras como Cláudio Galeno e Andreas Vesalius, enfatizando a transição de métodos não científicos para a observação direta e a metodologia científica. A influência da anatomia em outras áreas, como arte e filosofia, também é abordada, assim como a evolução das práticas éticas e regulamentações na aquisição de corpos para estudo. A palestra conclui sublinhando a importância inabalável do conhecimento anatômico para profissionais de saúde.
Highlights
- 🏛️ Da Pré-história ao Renascimento: A apresentação percorre a longa história do estudo anatômico, desde as primeiras representações artísticas pré-históricas até os trabalhos detalhados de Leonardo da Vinci e Michelangelo, mostrando como a compreensão do corpo humano evoluiu ao longo dos séculos.
- 🔬 Galeno vs. Vesalius: A palestra destaca a transição paradigmática na anatomia, contrastando o trabalho de Cláudio Galeno, baseado em dissecção animal e que perdurou por séculos, com a abordagem revolucionária de Andreas Vesalius, que enfatizou a observação direta do corpo humano.
- 🎨 A Arte e a Anatomia: A profunda interligação entre a anatomia e a arte renascentista é explorada, mostrando como a compreensão precisa do corpo humano influenciou a representação artística em esculturas e pinturas de grandes mestres.
- 📜 Evolução Ética e Regulamentação: A apresentação aborda as mudanças éticas e regulatórias no acesso a corpos para estudo, destacando o Ato de Anatomia de 1832 na Inglaterra como marco importante na normatização dessas práticas.
- 🧑⚕️ Importância Indispensável: A palestra conclui enfatizando a importância inabalável do conhecimento anatômico para a prática médica, desde o diagnóstico até os procedimentos cirúrgicos, salientando sua relevância em todas as fases da formação e da carreira de um profissional de saúde.
Andreas Vesalius
O Cirurgião Anatomista e Seu Legado no Conhecimento Médico
Introdução
Andreas Vesalius (1514–1564), frequentemente chamado de “pai da anatomia moderna”, é uma figura central na história da medicina. Sua abordagem inovadora ao estudo do corpo humano, fundamentada na dissecação e observação direta, transformou o conhecimento médico, especialmente no campo da cirurgia. Neste artigo, exploraremos como Vesalius, ao articular a importância da anatomia para a prática cirúrgica, moldou a base científica do tratamento das doenças do aparelho digestivo.

A Revolução de Vesalius: Do Teatro ao Livro
No Renascimento, a cirurgia era amplamente relegada a uma posição inferior em relação à medicina teórica. Cirurgiões eram vistos como “trabalhadores manuais”, enquanto os médicos universitários, alinhados aos ensinamentos de Galeno, raramente praticavam a dissecação. Vesalius desafiou esse paradigma. Em sua obra-prima, De humani corporis fabrica (1543), ele não apenas corrigiu erros galênicos, mas também destacou a relação intrínseca entre o conhecimento anatômico e a prática cirúrgica. A anatomia para Vesalius não era apenas um exercício acadêmico; era uma ferramenta essencial para o manejo cirúrgico. Ele mostrou que o entendimento detalhado da anatomia era vital para intervenções seguras, como a sutura de feridas intestinais ou a drenagem de abscessos abdominais. Embora a Fabrica não fosse destinada como um manual de cirurgia, sua ênfase no conhecimento anatômico estabeleceu os alicerces para técnicas cirúrgicas mais precisas no trato digestivo e além.
O Papel da Anatomia na Cirurgia do Aparelho Digestivo
Vesalius defendia que um cirurgião habilidoso devia conhecer profundamente a organização dos órgãos internos. Para ele, compreender a estrutura e a função do trato digestivo era crucial para evitar complicações iatrogênicas. Um exemplo prático disso está na importância da anatomia na sutura intestinal, onde a direção das fibras musculares influencia diretamente a recuperação pós-operatória e a funcionalidade do tecido. Além disso, Vesalius abordava a necessidade de ferramentas apropriadas para a prática anatômica e cirúrgica. Em sua Fabrica, ele ilustrou instrumentos que poderiam ser adaptados para dissecação e procedimentos cirúrgicos, desde lâminas para cortes delicados até agulhas curvas para suturas. Ele enfatizava que, embora os instrumentos fossem importantes, era a habilidade do cirurgião – adquirida por meio do estudo e prática – que determinava o sucesso do procedimento.
Desafios e Contribuições à Educação Médica
Vesalius enfrentou críticas intensas de seus contemporâneos, particularmente dos seguidores de Galeno, que viam sua abordagem como uma afronta às tradições estabelecidas. No entanto, ele persistiu, integrando a dissecção ao ensino médico e instigando seus alunos a examinarem corpos humanos reais, ao invés de dependerem exclusivamente de textos antigos. Esse método transformador, baseado na dissecção – o exame direto do corpo – permanece até hoje como pilar fundamental da formação em cirurgia. No tratamento das doenças do aparelho digestivo, a aplicação prática desse aprendizado reflete-se na precisão em procedimentos como gastrectomias, colecistectomias e ressecções intestinais, que requerem um conhecimento detalhado das relações anatômicas entre órgãos como estômago, fígado e intestinos.
Legado para a Cirurgia Moderna
Embora Vesalius tenha se distanciado da prática cirúrgica em seus escritos, ele elevou o status da anatomia ao patamar de ciência central à medicina, garantindo que futuros cirurgiões tivessem uma base sólida para o desenvolvimento de técnicas mais avançadas. Seu trabalho abriu caminho para o desenvolvimento da cirurgia, permitindo avanços que hoje salvam incontáveis vidas.
Conclusão
O legado de Andreas Vesalius não se limita à anatomia; ele inspirou gerações de médicos e cirurgiões a desafiar paradigmas, questionar autoridades e buscar a verdade diretamente no corpo humano. Suas contribuições à medicina moderna são um lembrete da importância de integrar o conhecimento científico ao cuidado do paciente.
“Eu quem sempre fui tão devotado aos escritos de Galeno, admito minha própria estupidez por confiar tanto em seus textos sem examinar a realidade com meus próprios olhos.” – Andreas Vesalius
Gostou❔Nos deixe um comentário ✍️, compartilhe em suas redes sociais e|ou mande sua dúvida pelo 💬 Chat On-line em nossa DM do Instagram.
Hashtags
#AnatomiaModerna #AndreasVesalius #EducaçãoMédica #CirurgiaDigestiva #HistóriaDaMedicina
Cronologia
1514 – Nasce filho de Isabel Crabbe e Andries van Wesel.
1530 – Matricula-se na Universidade de Louvain.
1533 – Inicia seus estudos de medicina na Universidade de Paris.
1536–1538 – Guerra entre Francisco I e Carlos V.
1536–1537 – Continua seus estudos médicos na Universidade de Louvain.
1537
- Fevereiro: Publicação de A Paráfrase do Nono Livro de Rhazes . . . por Andreas Vesalius de Bruxelas, Candidato em Medicina, em Louvain, por Rutgerus Rescius.
- Março: Publicação de A Paráfrase do Nono Livro de Rhazes por Andreas Vesalius, o Autor, em Basileia, por Robert Winter.
- 5 de dezembro: Recebe o título de doutor em medicina no palácio do Bispo de Pádua.
- 6 de dezembro: Nomeado para as cátedras de cirurgia na Universidade de Pádua.
- 6–24 de dezembro: Realiza dissecação pública em Pádua.
1538
- Publicação de Seis Tabelas Anatômicas em Veneza por Bernardino Vitali.
- Princípios de Anatomia Segundo a Opinião de Galeno por Johann Guinter, Ampliado e Corrigido por Andreas Vesalius de Bruxelas publicado em Veneza por Melchior Sessa.
1539
- Publicação de Uma Carta Ensinando que em Casos de Dor no Lado, Deve-se Cortar a Veia Axilar no Cotovelo Direito em Basileia por Robert Winter.
1540
- 15–24 de janeiro: Realiza dissecação pública na Universidade de Bolonha.
1540–1542
- Contribuições para as traduções latinas das Obras Completas de Galeno (1541–1542), publicadas em Veneza pela firma de Lucantonio Giunta.
1542
- Agosto: Envia os blocos de madeira e o texto da Fabrica para Johannes Oporinus em Basileia.
1543
- Janeiro: Chega a Basileia.
- Maio: Disseca e monta um esqueleto articulado de Jakob Karrer.
- Julho: Publicação de Sete Livros sobre a Estrutura do Corpo Humano e Epitome da Estrutura do Corpo Humano (Fabrica) em Basileia por Johannes Oporinus.
- Agosto: Edição alemã da Fabrica, traduzida por Albanus Torinus, publicada em Basileia por Oporinus.
- Agosto: Apresentação de cópias da Fabrica e Epitome a Carlos V, sendo nomeado médico imperial.
1544
- Realiza demonstrações anatômicas em Pisa a convite de Cosme de Médici.
- Casa-se com Anne van Hamme.
1545 – Nasce sua filha, Anne.
1546 – Publicação da Epístola Explicando o Método e Técnica de Administração da Raiz da China Fervida que o Invencível Carlos Recentemente Empregou em Basileia por Oporinus.
1555 – Segunda edição de Sete Livros sobre a Estrutura do Corpo Humano publicada em Basileia por Oporinus.
1556
- Recebe o título de Conde Palatino por Carlos V.
- Abdicação de Carlos V, que cede seus territórios espanhóis ao filho, Filipe II.
1559
- Enviado por Filipe II para atender ao ferimento de Henrique II, Rei da França, após um torneio.
- Muda-se para a corte de Filipe II em Madri.
1561 – Recebe uma cópia de Observações Anatômicas de Gabriel Falloppio.
1562 – Trata um ferimento de Don Carlos, filho de Filipe II.
1564
- Publicação de Uma Consideração sobre as Observações Anatômicas de Falloppio em Veneza por Francesco Franceschi.
- Março: Parte em peregrinação à Terra Santa e entrega um presente de Filipe para apoiar católicos em Jerusalém.
- 15 de outubro: Morre em seu retorno à Europa, na Ilha de Zakynthos.
Fundamentos do Transplante Hepático
O transplante hepático é uma das intervenções mais complexas e, ao mesmo tempo, revolucionárias no tratamento de doenças hepáticas terminais. Este procedimento, que substitui o fígado doente por um fígado saudável, é crucial para muitos pacientes que sofrem de doenças hepáticas graves e progressivas, além de algumas condições metabólicas e neoplásicas. Para os estudantes de medicina, residentes em cirurgia geral e pós-graduandos em cirurgia do aparelho digestivo, compreender os fundamentos do transplante hepático é essencial para atuar na linha de frente do tratamento avançado de doenças hepáticas. Neste artigo, abordaremos as principais indicações, critérios de seleção, técnicas cirúrgicas, imunologia, complicações, prognóstico e perspectivas futuras do transplante hepático.

Introdução
O transplante hepático tornou-se a única opção viável para pacientes com falência hepática irreversível, proporcionando uma sobrevida significativamente prolongada e melhor qualidade de vida. Desde a sua primeira realização em humanos, ele se consolidou como o tratamento padrão para diversas doenças hepáticas. No entanto, as limitações relacionadas à disponibilidade de doadores e as complexidades inerentes ao procedimento tornam-no um desafio tanto para médicos quanto para a sociedade.
Evolução Histórica
A história do transplante hepático iniciou-se nos anos 1960, quando o Dr. Thomas Starzl realizou o primeiro transplante bem-sucedido de fígado. Desde então, avanços significativos na imunossupressão e na técnica cirúrgica melhoraram dramaticamente os resultados. O desenvolvimento de drogas imunossupressoras, como a ciclosporina, foi crucial para reduzir a rejeição e aumentar a sobrevida dos pacientes. Hoje, o transplante hepático é realizado globalmente com taxas de sucesso que eram inimagináveis no início da prática.
Indicações de Transplante Hepático
O transplante de fígado é indicado principalmente para pacientes com falência hepática crônica ou aguda que apresentam risco de morte em curto prazo. As principais indicações incluem:
- Cirrose hepática avançada, incluindo cirrose hepática por hepatite viral crônica, cirrose biliar primária e doença hepática alcoólica;
- Hepatocarcinoma em fase inicial, que pode ter cura através do transplante em pacientes selecionados;
- Doenças metabólicas hereditárias, como a doença de Wilson e deficiência de alfa-1 antitripsina;
- Insuficiência hepática aguda, geralmente causada por hepatite fulminante.
Critérios de Seleção dos Receptores
A seleção de candidatos é orientada principalmente pelo MELD (Model for End-Stage Liver Disease) para adultos e o PELD (Pediatric End-Stage Liver Disease) para crianças, ambos sistemas de pontuação que avaliam a gravidade da doença hepática. Pacientes com MELD ≥ 15 geralmente são considerados elegíveis, enquanto aqueles com hepatocarcinoma devem atender aos critérios de Milão para serem listados. Além dos critérios médicos, os candidatos são avaliados em relação ao apoio familiar, aderência ao tratamento e estabilidade psicológica, pois esses fatores influenciam significativamente o sucesso pós-transplante.
Critérios de Seleção dos Doadores
Os doadores de fígado podem ser falecidos ou vivos. Os critérios para doadores falecidos incluem idade adequada, ausência de doença hepática e compatibilidade sanguínea com o receptor. Nos doadores vivos, além desses critérios, a saúde física e mental do doador é minuciosamente avaliada. A utilização de doadores vivos tornou-se comum em alguns países, sendo especialmente importante em regiões com baixa disponibilidade de doadores falecidos.
Contraindicações Relativas e Absolutas
Certas condições médicas são consideradas contraindicativas para o transplante hepático. Contraindicações absolutas incluem:
- Neoplasias extra-hepáticas não controladas;
- Insuficiência cardíaca ou pulmonar grave;
- Uso ativo de substâncias ilícitas. As contraindicações relativas, por outro lado, são avaliadas caso a caso, incluindo infecções controladas pelo HIV, cânceres tratados e comorbidades cardiovasculares que podem ser manejadas clinicamente.
Tipos de Transplante Hepático e Fundamentos Técnicos
Os transplantes hepáticos podem ser classificados como transplante de fígado total, reduzido, split-liver (dividido entre dois receptores), ou de doadores vivos. Nos transplantes de doadores vivos, segmentos específicos do fígado, geralmente o lobo esquerdo para crianças e o lobo direito para adultos, são removidos do doador e transplantados para o receptor. Cada tipo requer preparo técnico especializado e apresenta desafios próprios, especialmente em relação à preservação do fluxo sanguíneo e à minimização de complicações vasculares.
Principais Complicações
As complicações podem ocorrer tanto no pós-operatório imediato quanto no longo prazo. As principais incluem:
- Rejeição aguda e crônica do enxerto;
- Complicações vasculares, como trombose da artéria hepática e obstrução da veia porta;
- Complicações biliares, incluindo estenoses e fístulas;
- Infecções devido à imunossupressão prolongada.
Imunologia dos Transplantes: Tipos de Rejeição e Imunossupressão
A rejeição é um dos maiores desafios no transplante hepático e pode ser classificada em rejeição celular aguda, geralmente controlada por imunossupressão, e rejeição crônica, que leva à perda do enxerto. Os principais medicamentos imunossupressores incluem ciclosporina, tacrolimus e micofenolato de mofetila. A terapia é cuidadosamente ajustada para minimizar a rejeição e evitar efeitos adversos, como infecções oportunistas e cânceres secundários.
Prognóstico do Transplante: Sobrevida Global e do Enxerto
A sobrevida após o transplante hepático continua a melhorar, com taxas de 1 ano superiores a 90% e sobrevida média de 20 anos para pacientes transplantados na década de 1990. O prognóstico depende de múltiplos fatores, incluindo a gravidade da doença original, a idade do receptor e as complicações pós-operatórias. O acompanhamento vitalício é necessário para monitorar a função do enxerto e ajustar a imunossupressão.
Perspectivas Futuras
As inovações no transplante hepático incluem avanços na perfusão de órgãos, que permite avaliar e condicionar o fígado doado antes do transplante, e o potencial uso de xenotransplantes e engenharia de tecidos. Esses avanços visam aumentar a disponibilidade de órgãos e melhorar a longevidade dos enxertos. O desenvolvimento de técnicas para induzir tolerância imunológica também promete reduzir a necessidade de imunossupressão a longo prazo, melhorando a qualidade de vida dos transplantados.
Conclusão
O transplante hepático é um procedimento altamente complexo, mas fundamental para pacientes com doenças hepáticas terminais. Para estudantes e residentes, entender os critérios de seleção, o manejo das complicações e os fundamentos técnicos é essencial para a prática em gastroenterologia e cirurgia hepática. À medida que a medicina avança, a capacidade de tratar pacientes com insuficiência hepática melhora continuamente, levando a novos horizontes na área de transplantes.
“Liver transplantation provides an opportunity for these patients to reclaim a healthy life, free from the shadow of chronic liver disease.” – Thomas Starzl
Gostou? Nos deixe um comentário ✍️, compartilhe em suas redes sociais e/ou mande sua dúvida pelo 💬 Chat On-line em nossa DM do Instagram.
#TransplanteHepático #Medicina #CirurgiaDigestiva #SaúdeHepática #Imunossupressão
A Filosofia da Cirurgia
No contexto do tratamento cirúrgico das doenças do aparelho digestivo, a formação de um cirurgião vai além do domínio técnico. Inspirados nos ensinamentos de Galeno, renomado médico e filósofo da antiguidade, reconhecemos que o cirurgião ideal deve incorporar uma combinação de habilidades práticas e virtudes filosóficas que guiam sua conduta ética e profissional. Neste artigo, direcionado a estudantes de medicina, residentes de cirurgia geral e pós-graduandos em cirurgia do aparelho digestivo, exploraremos as cinco virtudes fundamentais que definem o “cirurgião filósofo”. Essas virtudes não apenas aprimoram a prática clínica, mas também integram os princípios éticos da medicina na vida do cirurgião, como enfatizado por Galeno.
1. Proeficiência Técnica e Conhecimento Filosófico
O bom cirurgião não é apenas aquele que domina as técnicas cirúrgicas com excelência, mas também aquele que entende a importância de uma formação filosófica sólida. Para Galeno, a medicina e a filosofia caminham lado a lado, pois o cirurgião deve ser capaz de fazer julgamentos críticos baseados em raciocínios demonstrativos, além de possuir uma visão clara das causas e consequências de suas ações.
“O médico que pratica sua arte visando apenas ganhos pessoais é um charlatão; somente o conhecimento profundo do corpo e da alma o torna um verdadeiro mestre de sua prática.” – Galeno.
2. Ética e Humanidade
A prática cirúrgica, quando orientada pela ética e pelo respeito à vida humana, transforma-se em uma verdadeira arte de cura. Galeno reforça que o cirurgião não deve estar motivado por ambições financeiras ou status social, mas pela filantropia – o desejo genuíno de aliviar o sofrimento humano. Ao tratar doenças do aparelho digestivo, essa virtude é especialmente relevante, pois muitas intervenções são decisivas para a qualidade de vida do paciente.
“A medicina existe para o benefício da humanidade; aquele que visa o lucro ao invés de curar não é digno do título de médico.” – Galeno.
3. Disciplina e Dedicação Inabalável
A vida de um cirurgião é marcada por noites de estudo e jornadas exaustivas no centro cirúrgico. Para Galeno, a dedicação é a chave para o sucesso na prática médica. Ele descreve o verdadeiro cirurgião como alguém que sacrifica o próprio conforto pela excelência no cuidado dos pacientes, não permitindo que o cansaço ou a rotina afete sua atenção e precisão cirúrgica.
“Passei noites sem dormir por meus pacientes, pois, como um escravo do meu ofício, minha dedicação não conhecia limites.” – Galeno.
4. Humildade e Rejeição ao Luxo
A humildade, segundo Galeno, é uma virtude essencial para um cirurgião. Ele critica fortemente aqueles que se entregam ao luxo e à bajulação, comportamentos que desviam o foco do verdadeiro propósito da medicina. O cirurgião deve evitar a busca por reconhecimento superficial, concentrando-se na melhoria contínua de suas habilidades e na obtenção de resultados clínicos favoráveis para seus pacientes.
“O verdadeiro médico deve evitar o luxo e a bajulação; sua maior honra é a saúde de seus pacientes.” – Galeno.
5. Responsabilidade Social e Participação Comunitária
Para Galeno, a medicina vai além das portas dos hospitais. O cirurgião filósofo deve estar envolvido em sua comunidade, utilizando seu conhecimento e habilidades para o benefício da sociedade como um todo. Isso inclui atuar em programas de saúde pública, educação médica e prevenção de doenças. Um cirurgião deve ser um líder que promove a saúde e o bem-estar, não apenas em seus pacientes, mas na população em geral.
“A medicina, em sua essência, é uma arte pública, destinada a servir todos os membros da sociedade, do mais nobre ao mais humilde.” – Galeno.

Conclusão
As virtudes mencionadas por Galeno são mais do que um código moral; elas são uma diretriz prática para os cirurgiões que desejam integrar a filosofia em sua prática médica. Essas virtudes formam o alicerce de uma carreira dedicada não apenas à técnica cirúrgica, mas à verdadeira arte de cuidar da vida humana. Como futuros cirurgiões do aparelho digestivo, é fundamental adotar essas virtudes para uma prática cirúrgica que vá além da cura física, abraçando a responsabilidade ética e social que acompanha a medicina.
“Um médico que cura corpos, mas não cultiva o bem em sua alma, jamais será verdadeiramente completo.” – Galeno.
Gostou ❔ Nos deixe um comentário ✍️, compartilhe em suas redes sociais e|ou mande sua dúvida pelo 💬 Chat On-line em nossa DM do Instagram.
#cirurgiageral #aparelhodigestivo #éticaemmedicina #galeno #cirurgiafilosófica
Como Eu Trato Colelitíase e Suas Complicações
Um Guia Prático para Estudantes de Medicina e Residentes de Cirurgia
A colelitíase, ou a formação de cálculos biliares na vesícula, é uma condição amplamente prevalente, especialmente no contexto do aumento da síndrome metabólica e do envelhecimento populacional. Cerca de 10% a 20% da população adulta pode desenvolver cálculos biliares, embora apenas 20% dessa população apresente sintomas ou complicações. Com mais de 1,2 milhões de colecistectomias realizadas anualmente nos Estados Unidos, a cirurgia continua sendo o tratamento padrão para colelitíase sintomática, com complicações potencialmente graves como a colecistite aguda, colangite e pancreatite biliar. No Brasil, estudos epidemiológicos indicam que a colelitíase afeta cerca de 15% da população adulta.
Introdução
A colelitíase se refere à formação de cálculos biliares no trato biliar, com maior prevalência na vesícula biliar. Esta condição pode ser assintomática ou associada a dor abdominal, chamada cólica biliar. A maioria dos pacientes permanece assintomática, mas, em alguns casos, podem surgir complicações graves, como colecistite aguda, colangite ou pancreatite. A escolha do tratamento depende da presença ou ausência de sintomas e complicações.
Diagnóstico e Classificação
O diagnóstico de colelitíase frequentemente é feito incidentalmente por ultrassonografia abdominal. Para pacientes com sintomas, a ultrassonografia tem uma acurácia de cerca de 95% na detecção de cálculos. Além disso, em casos mais complicados, exames como a colangiopancreatografia por ressonância magnética (CPRM) e a colangiopancreatografia retrógrada endoscópica (CPRE) podem ser usados para detectar cálculos no ducto biliar comum.
A classificação das complicações da colelitíase inclui:
- Colecistite aguda: Inflamação da vesícula biliar, geralmente causada por obstrução do ducto cístico por cálculos.
- Colangite: Infecção bacteriana da via biliar, associada à obstrução biliar.
- Pancreatite biliar: Inflamação do pâncreas causada por cálculos impactados no ducto biliar.
- Coledocolitíase: Presença de cálculos no ducto biliar comum.
Aplicação na prática da Cirurgia Digestiva
O manejo cirúrgico da colelitíase varia de acordo com a apresentação clínica do paciente. Para pacientes assintomáticos, a colecistectomia profilática não é indicada, exceto em casos de risco elevado, como na presença de vesícula em porcelana (associada ao câncer de vesícula biliar).
- Colelitíase sintomática: A abordagem cirúrgica padrão é a colecistectomia laparoscópica, preferencialmente realizada nas primeiras 72 horas após o início dos sintomas em casos de colecistite aguda. A colecistectomia tem uma taxa de mortalidade inferior a 1%, sendo extremamente eficaz na resolução dos sintomas.
- Coledocolitíase: Pacientes com coledocolitíase podem requerer uma abordagem multimodal, combinando a CPRE para remoção de cálculos no ducto biliar e colecistectomia subsequente. A laparoscopia também pode ser utilizada para explorar o ducto biliar comum, permitindo a retirada dos cálculos.
- Pancreatite biliar: A pancreatite causada por cálculos biliares requer estabilização inicial do paciente, com reposição volêmica e analgesia. A colecistectomia deve ser realizada na mesma internação para prevenir recorrências, exceto em casos de pancreatite grave com necrose pancreática, onde o cirurgião deve aguardar até a resolução do quadro inflamatório.
- Tratamento de emergência: Casos de colangite e pancreatite biliar requerem intervenção imediata, com drenagem biliar emergente via CPRE ou drenagem percutânea seguida de colecistectomia, dependendo do estado clínico do paciente.
Em casos mais raros, como a síndrome de Mirizzi ou o íleo biliar, intervenções complexas são necessárias. A síndrome de Mirizzi, caracterizada pela obstrução do ducto biliar comum por compressão extrínseca de um cálculo, pode requerer remoção cirúrgica e, às vezes, reconstrução da via biliar.
Pontos-Chave
- A ultrassonografia abdominal é o exame inicial mais adequado para o diagnóstico de colelitíase.
- A colecistectomia laparoscópica continua sendo o tratamento padrão para colelitíase sintomática e colecistite aguda.
- Pacientes com coledocolitíase e pancreatite biliar requerem uma abordagem multimodal, incluindo CPRE e colecistectomia.
- A colangite aguda é uma emergência médica e deve ser tratada com descompressão biliar urgente.
- No Brasil, estima-se que cerca de 15% dos adultos tenham colelitíase, com uma incidência crescente devido a fatores de risco como obesidade e diabetes.
Conclusão
O tratamento cirúrgico da colelitíase e suas complicações é bem estabelecido, com a colecistectomia laparoscópica sendo o padrão de tratamento para a maioria dos pacientes sintomáticos. Entretanto, é importante que os profissionais de saúde identifiquem as complicações precocemente e adaptem o tratamento à condição clínica do paciente. O uso da CPRE e da colecistectomia precoce reduzem significativamente as taxas de complicações graves, como pancreatite e colangite. Além disso, o manejo adequado da dor e o reconhecimento rápido das emergências, como a colangite, são essenciais para melhorar os desfechos clínicos.
Como o Dr. Steven Strasberg observou:
“A decisão cirúrgica em pacientes com doença do trato biliar deve ser orientada não apenas pelos achados de imagem, mas pela fisiopatologia subjacente e pelo quadro clínico individualizado.”
Gostou ❔ Nos deixe um comentário ✍️, compartilhe em suas redes sociais e|ou mande sua dúvida pelo 💬 Chat On-line em nossa DM do Instagram.
Hashtags:
CirurgiaDigestiva #Colelitíase #TratamentoCirúrgico #PancreatiteBiliar #EducaçãoMédicaContinuada
Cirurgião Digestivo Contemporâneo
Introdução
A cirurgia do aparelho digestivo é uma especialidade em constante evolução, que exige do cirurgião não apenas habilidades técnicas, mas também uma forte capacidade de liderança e visão estratégica. O cirurgião digestivo contemporâneo deve ser um arquiteto de sua prática, capaz de transformar desafios em oportunidades e de inspirar sua equipe a buscar a excelência. Este artigo é direcionado a estudantes de medicina, residentes de cirurgia geral e pós-graduandos em cirurgia do aparelho digestivo, abordando as características essenciais que definem um cirurgião digestivo contemporâneo.
1. Liderança
A liderança eficaz é fundamental para o sucesso em qualquer especialidade médica. Um cirurgião deve ser um multiplicador de talentos, capaz de inspirar e motivar sua equipe. Para isso:
- Sinceridade e Empatia: Acredite genuinamente na visão que você está promovendo. Inspire confiança ao demonstrar vulnerabilidade e autenticidade.
- Decisões Rápidas e Informadas: Em um ambiente cirúrgico, a indecisão pode ser prejudicial. Desenvolva a habilidade de tomar decisões rápidas, baseadas em dados e experiências anteriores.
- Comunicação Clara: Certifique-se de que sua equipe compreenda a visão e os objetivos do procedimento. Uma comunicação eficaz evita mal-entendidos e promove um ambiente colaborativo.
2. Visão
A definição de uma visão clara é crucial para guiar as operações diárias e as decisões estratégicas. O cirurgião deve:
- Estabelecer Metas Claras: Definir objetivos específicos para a equipe cirúrgica ajuda a manter o foco e a motivação.
- Inspirar Sua Equipe: Compartilhe essa visão com todos os membros da equipe, fazendo com que se sintam parte do processo. Uma equipe engajada é mais propensa a trabalhar em conjunto para alcançar objetivos comuns.
3. Estratégia
Uma vez que a visão está definida, é crucial desenvolver uma estratégia robusta:
- Planejamento Estratégico: Elabore um plano detalhado que inclua as melhores práticas cirúrgicas, protocolos de segurança e estratégias de recuperação para os pacientes.
- Avaliação Contínua: Monitore os resultados das intervenções cirúrgicas e ajuste suas estratégias conforme necessário. Use dados para embasar suas decisões.
4. Inovação
A inovação deve ser uma parte central da sua prática:
- Estimule Criatividade: Crie um ambiente onde a equipe se sinta à vontade para sugerir novas ideias e abordagens. A inovação pode surgir de qualquer lugar.
- Adote Novas Tecnologias: Esteja aberto às inovações tecnológicas, como técnicas minimamente invasivas e endoscópicas, que podem melhorar os resultados dos pacientes.
5. Excelência Tática
Finalmente, a excelência tática é essencial para traduzir sua visão em ações concretas:
- Desenvolva Protocolos Eficazes: Estabeleça diretrizes claras para cada procedimento cirúrgico, garantindo consistência e segurança.
- Treinamento Contínuo: Invista no treinamento da equipe para garantir que todos estejam atualizados sobre as melhores práticas e novas técnicas.
Pontos-Chave
- Integração da Tecnologia: A adoção de tecnologias avançadas é essencial para melhorar os resultados cirúrgicos.
- Foco no Paciente: O cirurgião deve considerar não apenas os aspectos técnicos da cirurgia, mas também o impacto emocional e psicológico nos pacientes.
- Colaboração Multidisciplinar: Trabalhar em equipe com outros profissionais da saúde é fundamental para garantir um tratamento abrangente e eficaz.
Conclusões Aplicadas à Prática do Cirurgião Digestivo
O cirurgião digestivo contemporâneo deve ser um líder eficaz, capaz de inspirar sua equipe enquanto navega pelas complexidades da prática clínica. A combinação de uma liderança sólida, uma visão clara, inovação constante e excelência tática não só melhora os resultados dos pacientes, mas também contribui para a construção de uma carreira duradoura e respeitada na cirurgia digestiva.
William Stewart Halsted: “A única via para a maestria cirúrgica é através do treinamento constante, da prática rigorosa e da dedicação incansável à arte e ciência da cirurgia.”
Essa citação reflete a importância da ciência no avanço da medicina e da cirurgia, enfatizando que o conhecimento deve ser utilizado para melhorar a vida dos pacientes.
Gostou ❔ Nos deixe um comentário ✍️ , compartilhe em suas redes sociais e|ou mande sua dúvida pelo 💬 Chat On-line em nossa DM do Instagram.
#Hashtags #CirurgiaDigestiva #LiderançaNaSaúde #InovaçãoCirúrgica #ExcelênciaTática #EducaçãoMédica
Evolução e Avanços na Prática Cirúrgica Gastrointestinal
A cirurgia digestiva, uma das especialidades mais antigas e complexas da medicina, tem suas raízes fincadas em descobertas, inovações e aprimoramentos técnicos que revolucionaram o cuidado com as doenças do aparelho digestivo. Desde os primeiros relatos de intervenções rudimentares até os procedimentos minimamente invasivos da atualidade, essa área continua a avançar e moldar o tratamento cirúrgico de doenças que acometem o esôfago, estômago, intestinos, fígado e pâncreas. Neste artigo, abordaremos a história e os principais marcos da cirurgia digestiva, enfatizando a relevância dos avanços para a prática clínica moderna, com foco no aprendizado de estudantes de medicina, residentes e pós-graduandos em cirurgia do aparelho digestivo.
Introdução
A história da cirurgia digestiva é marcada pela evolução contínua de técnicas cirúrgicas, desenvolvimento de novos instrumentos e a colaboração multidisciplinar que hoje envolve anestesiologia, radiologia e farmacologia. Ao longo dos séculos, as descobertas em anatomia, fisiologia e patologia proporcionaram uma compreensão mais profunda das doenças do trato gastrointestinal, permitindo que as intervenções cirúrgicas se tornassem mais seguras e eficazes.
No Brasil, segundo o Colégio Brasileiro de Cirurgia Digestiva, as cirurgias digestivas correspondem a uma significativa parcela dos procedimentos realizados em hospitais, com alta prevalência de cirurgias de vesícula biliar, câncer de intestino e tratamentos para doenças hepáticas. Este cenário ressalta a importância de conhecer a evolução histórica dessa especialidade, pois, como veremos, muitos dos avanços que hoje tomamos como garantidos foram frutos de pioneirismo e ousadia de cirurgiões ao longo da história.
Primeiros Avanços e Procedimentos Pioneiros
Os primeiros registros de intervenções no sistema digestivo datam de 400 a.C., quando Hipócrates e outros médicos da Grécia antiga descreviam tratamentos rudimentares para abscessos hepáticos e hérnias. No entanto, a verdadeira transformação da cirurgia digestiva começou no final do século XIX, com a descoberta da anestesia e os primeiros relatos de ressecções gástricas bem-sucedidas.
Theodor Billroth (1829–1894), amplamente considerado o “pai da cirurgia digestiva moderna”, realizou a primeira gastrectomia parcial para câncer gástrico em 1881, uma operação que ficou conhecida como procedimento Billroth I. Sua abordagem inovadora marcou o início de uma nova era, onde a cirurgia para tratamento de doenças malignas do estômago e intestinos se tornou uma realidade, salvando milhares de vidas.
Cirurgia Esofágica
A cirurgia do esôfago foi tradicionalmente uma área desafiadora devido à sua anatomia complexa e aos riscos de complicações. O tratamento cirúrgico da doença do refluxo gastroesofágico (DRGE) e hérnias de hiato evoluiu a partir da compreensão do mecanismo do esfíncter esofágico inferior e do uso de técnicas de manometria esofágica. A técnica de fundoplicatura de Nissen, desenvolvida por Rudolf Nissen em 1955, permanece até hoje um dos principais procedimentos para corrigir o refluxo grave.
Cirurgia do Estômago e Úlceras Pépticas
No século XX, as cirurgias para úlceras pépticas eram bastante comuns até a descoberta dos antibióticos e dos inibidores de bomba de prótons, que revolucionaram o tratamento não-cirúrgico dessas condições. No entanto, antes disso, procedimentos como a vagotomia e gastrojejunostomia eram amplamente utilizados. Um dos marcos importantes foi a descoberta, em 1983, de que a bactéria Helicobacter pylori estava associada à maioria das úlceras gástricas e duodenais, o que reduziu drasticamente a necessidade de cirurgias eletivas para essa condição.
Cirurgia do Fígado e Vias Biliares
A cirurgia hepática tem uma rica história que começou com intervenções em abscessos hepáticos na antiguidade. No final do século XIX, Carl Langenbuch realizou a primeira colecistectomia (remoção da vesícula biliar), revolucionando o tratamento da litíase biliar. No Brasil, estima-se que cerca de 500 mil colecistectomias sejam realizadas anualmente, muitas delas agora por via laparoscópica, método introduzido na década de 1990, que reduziu complicações e o tempo de recuperação dos pacientes.
Além disso, a cirurgia do fígado foi significativamente impactada pela evolução da segmentação hepática, que permitiu ressecções mais precisas e seguras de tumores hepáticos.
Cirurgia Pancreática
O tratamento cirúrgico de doenças pancreáticas, como o câncer de pâncreas e a pancreatite crônica, foi um dos mais desafiadores devido à alta complexidade do órgão e suas relações anatômicas. O procedimento de pancreaticoduodenectomia, popularizado por Allen Whipple em 1935, é um dos grandes marcos da cirurgia pancreática. Essa técnica, conhecida como procedimento de Whipple, ainda é considerada o padrão para o tratamento de tumores periampulares e tem sido aprimorada com a abordagem minimamente invasiva.
Impacto das Tecnologias Minimamente Invasivas
Nas últimas décadas, o avanço das tecnologias minimamente invasivas, como a laparoscopia e, mais recentemente, a cirurgia robótica, transformou a prática cirúrgica. Procedimentos que antes exigiam grandes incisões e longos períodos de recuperação agora podem ser realizados com pequenas incisões e internações mais curtas. A laparoscopia, inicialmente utilizada para colecistectomia, é hoje amplamente aplicada em ressecções colorretais, bariátricas e hepáticas.
Avanços no Diagnóstico e Imagem
O desenvolvimento de técnicas de imagem, como ultrassonografia, tomografia computadorizada e ressonância magnética, mudou drasticamente o planejamento cirúrgico, permitindo diagnósticos mais precisos e a avaliação detalhada de tumores e outras lesões abdominais. O surgimento de tecnologias como a colangiopancreatografia por ressonância magnética (MRCP) e a endoscopia terapêutica também possibilitou intervenções menos invasivas para tratar patologias biliares e pancreáticas.
Pontos-chave
- Técnicas de cirurgia digestiva foram amplamente impactadas por avanços em anestesia, esterilização e antibióticos, além de melhorias no diagnóstico por imagem e métodos minimamente invasivos.
- A cirurgia gástrica para úlceras foi substituída em grande parte por tratamentos clínicos devido à descoberta da Helicobacter pylori e inibidores de ácido.
- No Brasil, cirurgias digestivas, como colecistectomias, são realizadas em larga escala, com aproximadamente 500 mil procedimentos por ano.
- A laparoscopia e a robótica representam o futuro da cirurgia digestiva, reduzindo o tempo de internação e complicações pós-operatórias.
Conclusão
A história da cirurgia digestiva é uma jornada contínua de aprendizado e aprimoramento. Para o cirurgião digestivo contemporâneo, compreender essa evolução é crucial para aplicar as melhores práticas no atendimento aos pacientes. Os avanços tecnológicos e o desenvolvimento de técnicas minimamente invasivas não apenas transformaram a maneira como abordamos as doenças do aparelho digestivo, mas também melhoraram significativamente os desfechos cirúrgicos, proporcionando maior segurança e eficiência no tratamento.
Estar familiarizado com esses marcos históricos é essencial para o profissional que deseja se destacar na prática cirúrgica moderna, utilizando o passado como base para inovações futuras.
Como disse Theodor Billroth, “Só quem conhece o passado pode compreender o presente e planejar o futuro”.
Gostou ❔ Nos deixe um comentário ✍️, compartilhe em suas redes sociais e|ou mande sua dúvida pelo 💬 Chat On-line em nossa DM do Instagram.
#CirurgiaDigestiva #HistoriaDaMedicina #TecnologiaCirurgica #CirurgiaMinimamenteInvasiva #EducaçãoMédicaContinuada
Respeito à Liberdade Religiosa
Considerando as teses de repercussão geral fixadas pelo Supremo Tribunal Federal (STF), é essencial que os cirurgiões digestivos estejam cientes das diretrizes que visam respeitar a liberdade religiosa dos pacientes, especialmente no atendimento a Testemunhas de Jeová. De acordo com o ministro Luís Roberto Barroso, essa decisão fortalece a compatibilidade entre a liberdade religiosa e os direitos à vida e à saúde. As teses aprovadas têm repercussão geral, sendo aplicáveis a todos os casos similares.
🔹 Pontos-chave:
1️⃣ Recusa de Transfusões: Testemunhas de Jeová adultas podem recusar transfusões de sangue com base na sua liberdade religiosa.
2️⃣ Procedimentos Alternativos: O SUS deve garantir alternativas viáveis, incluindo tratamento fora do domicílio do paciente, quando necessário.
3️⃣ Casos de Crianças e Adolescentes: Em situações que envolvem menores de idade, o princípio do melhor interesse da saúde e da vida da criança prevalece sobre a liberdade religiosa dos pais.
Essa decisão representa um avanço na proteção das crenças individuais, sem deixar de lado o compromisso do Estado com a saúde e a vida de seus cidadãos. A recente decisão do STF estabelece que Testemunhas de Jeová, adultas e capazes, têm o direito de recusar procedimentos médicos que envolvam transfusão de sangue, em conformidade com sua liberdade religiosa. O Sistema Único de Saúde (SUS) deve garantir o acesso a procedimentos alternativos, quando disponíveis, e, caso necessário, encaminhar o paciente para tratamento em outras localidades.
🔹 Diretrizes para Cirurgiões Digestivos:
1️⃣ Respeito à Liberdade Religiosa: A recusa de transfusões por pacientes adultos e capazes deve ser livre, informada e com plena consciência dos riscos e alternativas.
2️⃣ Oferecimento de Procedimentos Alternativos: O SUS tem a responsabilidade de fornecer tratamentos alternativos que respeitem a decisão do paciente de não receber transfusões de sangue.
3️⃣ Diretivas Antecipadas de Vontade: Pacientes podem registrar previamente sua recusa por meio de diretivas antecipadas, que devem ser consideradas pela equipe médica durante o planejamento cirúrgico.
4️⃣ Viabilidade Técnico-Científica: Os procedimentos alternativos devem ser viáveis e seguros, com o apoio da equipe médica para garantir o sucesso do tratamento.
5️⃣ Processo de Consentimento: O consentimento do paciente deve ser esclarecido e sem coação, com total entendimento dos riscos e benefícios.
Essa decisão do STF reforça a importância de equilibrar a autonomia individual com a segurança médica, respeitando as crenças dos pacientes sem comprometer a qualidade do atendimento. Cirurgiões digestivos devem estar preparados para oferecer soluções seguras e alternativas compatíveis com as preferências religiosas dos pacientes, contribuindo para um atendimento ético e humanizado.
#CirurgiaDigestiva #LiberdadeReligiosa #STF #AutonomiaDoPaciente #AlternativasSemSangue #SUS
Aprendizado pelo Contraste
Ressignificando os Eventos Adversos na Cirurgia Digestiva
Introdução
No campo da medicina, especialmente na cirurgia digestiva, lidar com eventos adversos é uma parte inevitável da prática clínica. Dado o grau de complexidade dos procedimentos e a vulnerabilidade dos órgãos envolvidos, complicações como fístulas, hemorragias ou infecções podem ocorrer, desafiando a habilidade do cirurgião. Embora esses momentos tragam desconforto e pressão, também oferecem oportunidades valiosas de aprendizado. Ressignificar os eventos adversos é uma abordagem que transforma desafios em crescimento técnico e emocional, resultando em uma prática mais segura e eficaz. Este artigo, voltado para estudantes de medicina, residentes em cirurgia geral e pós-graduandos em cirurgia digestiva, explora o conceito de aprendizado pelo contraste e a importância de ressignificar as adversidades cirúrgicas. Discutiremos como essa mentalidade pode ser aplicada na prática, visando a melhoria contínua e a prevenção de complicações futuras.
Desenvolvimento
Eventos adversos, como complicações intraoperatórias ou pós-operatórias, são uma realidade que o cirurgião deve aprender a enfrentar. No Brasil, estima-se que cerca de 7% das internações hospitalares resultem em algum tipo de evento adverso. Na área cirúrgica, especialmente no aparelho digestivo, complicações como fístulas anastomóticas, infecções intra-abdominais e perfurações têm incidência significativa. Tais eventos, no entanto, não devem ser vistos exclusivamente como fracassos, mas como catalisadores para o aprimoramento técnico.
A ressignificação desses eventos é baseada no conceito de reframe (mudar a perspectiva). Adler, em seus estudos sobre psicologia individual, destacou que as dificuldades podem se transformar em oportunidades de desenvolvimento. Para o cirurgião digestivo, esse aprendizado pelo contraste, ou seja, aprender com os erros ou complicações, é essencial para aperfeiçoar suas habilidades técnicas e fortalecer a confiança no atendimento ao paciente.
Aplicação na Cirurgia Digestiva
Em procedimentos de alta complexidade, como ressecções intestinais, gastrectomias ou cirurgias hepáticas, os eventos adversos, apesar de serem inevitáveis em alguns casos, podem ser fontes de aprendizado profundo. A seguir, apresentamos cinco dicas práticas para ressignificar e aprender com esses eventos, transformando-os em oportunidades de aprimoramento:
- Analisar detalhadamente o evento adverso: Logo após a ocorrência de uma complicação, é fundamental revisitar o caso por completo. Analise cada etapa do procedimento, desde o pré-operatório até o intraoperatório. Identificar fatores como condições do paciente, técnica cirúrgica empregada e possíveis fatores de risco não previstos pode fornecer insights preciosos. Por exemplo, em uma cirurgia com fístula anastomótica (complicação que ocorre entre 2% e 12% dos casos de anastomose intestinal), revisar a técnica de sutura e as condições do paciente pode evitar futuras ocorrências.
- Debriefing com a equipe cirúrgica: O aprendizado não deve ser individual. Discuta abertamente o evento adverso com a equipe. Essa prática colaborativa permite que todos os membros aprendam com a experiência, reforçando práticas seguras e permitindo o ajuste de protocolos internos. Estudos mostram que equipes que realizam debriefings após complicações melhoram significativamente a coesão e a prevenção de novos erros.
- Aplicação de protocolos e checklists: Reforçar o uso de protocolos estabelecidos, como o ERAS (Enhanced Recovery After Surgery), tem se mostrado eficaz na redução de complicações cirúrgicas. Ao ressignificar um evento adverso, o cirurgião pode revisar quais protocolos foram seguidos e quais etapas foram negligenciadas. A introdução de checklists específicos para cada tipo de procedimento cirúrgico também pode ser uma ferramenta poderosa de prevenção.
- Investir em simulações e treinamentos específicos: Após um evento adverso, a prática deliberada em simulações cirúrgicas pode ajudar a melhorar as habilidades técnicas. Participar de treinamentos simulados, como em cursos de laparoscopia avançada, oferece a oportunidade de refinar técnicas em um ambiente seguro, aumentando a confiança e reduzindo a probabilidade de complicações futuras em cenários reais.
- Monitorar o impacto emocional: Além das questões técnicas, o impacto emocional de uma complicação deve ser considerado. Estudos brasileiros indicam que o burnout entre cirurgiões pode ser exacerbado por complicações cirúrgicas. Para prevenir a exaustão emocional, é essencial que o cirurgião reconheça a importância da saúde mental. Práticas como meditação, terapia e suporte emocional entre colegas podem ajudar a lidar com a pressão associada a eventos adversos.
Pontos-chave
- Revisão crítica e colaborativa: A análise sistemática e a troca aberta de informações sobre o evento adverso são fundamentais para garantir que os mesmos erros não se repitam.
- Prevenção com protocolos: O uso consistente de protocolos e checklists aumenta significativamente a segurança dos pacientes.
- Educação contínua: A participação em treinamentos e simulações reforça a habilidade técnica e a confiança, especialmente após um evento adverso.
- Saúde mental do cirurgião: É fundamental gerenciar o estresse e o impacto emocional das complicações, garantindo que o cirurgião mantenha o equilíbrio mental ao longo da carreira.
Conclusão
A ressignificação dos eventos adversos na prática cirúrgica não é apenas uma ferramenta de aprendizagem, mas uma atitude essencial para o crescimento contínuo. O sucesso de um cirurgião digestivo depende não apenas de sua habilidade técnica, mas de sua capacidade de aprender com os desafios, adaptando-se a cada nova experiência. Ao transformar dificuldades em oportunidades de melhoria, o cirurgião evolui não só em sua prática, mas também em sua resiliência emocional. Como afirmou Alfred Adler: “A maior força não vem de evitar os fracassos, mas de aprender com eles e seguir em frente“. Ressignificar eventos adversos é parte integrante do caminho de evolução para um cirurgião mais completo e resiliente.
Gostou❔ Nos deixe um comentário ✍️, compartilhe em suas redes sociais ou mande sua dúvida pelo 💬 Chat On-line em nossa DM do Instagram.
Hashtags
#cirurgiadigestiva #eventosadversos #ressignificação #aprendizadocirurgico #educacaomedica
Aprendendo com a Cirurgia de Guerra
Cada grande guerra tem sido um catalisador para avanços rápidos no atendimento ao trauma. À medida que os sistemas médicos lidam com os desafios de cuidar de muitas pessoas feridas (militares e civis), muitas vezes em ambientes muito adversos, eles evoluem, se adaptam e improvisam rapidamente. As guerras também provocam investimentos financeiros significativos dos governos em pesquisa e desenvolvimento e atraem algumas das melhores mentes para o campo.
Muitos dos recursos (várias intervenções operatórias, medicamentos, fluidos, curativos, sistemas de transporte rápido, equipes de trauma, atendimento no campo e muito mais) que são considerados garantidos hoje nos centros de trauma civis podem ser rastreados até as guerras do passado. Porém, curiosamente, à medida que a medicina de guerra melhora e evolui para cuidar de lesões piores, a indústria bélica responde desenvolvendo armamentos mais letais.
Assim, a porcentagem de feridos que morrem no campo de batalha (taxa de mortos em ação ou KIA) permaneceu relativamente estática durante o século XX, ficando em torno de 25%. No entanto, o atual conflito é a primeira vez na guerra moderna que a taxa de KIA caiu para 10%. Essa queda dramática é claramente multifatorial em etiologia e reflete o foco em estratégias de prevenção com uso generalizado de armaduras corporais superiores e implantação de veículos militares de melhor design.
Além disso, os atuais conflitos em andamento alteraram fundamentalmente a forma como cuidamos dos feridos, o que resultou não apenas em taxas de sobrevivência melhores, mas também em desfechos funcionais marcadamente superiores. A cirurgia de guerra tem sido um campo fértil para o desenvolvimento de técnicas e estratégias inovadoras no tratamento de lesões traumáticas. Muitas dessas lições aprendidas no campo de batalha podem ser aplicadas com sucesso no cenário da cirurgia do trauma, melhorando os desfechos dos pacientes.
Prevenção e Controle de Hemorragia
Avanços como bandagens hemostáticas e torniquetes, amplamente utilizados por socorristas militares, têm sido adotados pela medicina civil para o controle temporário de hemorragia compressível ou de extremidade. No Brasil, o curso “Pare o Sangramento”, inspirado no programa militar “Stop the Bleed”, já treinou mais de 100 mil socorristas civis na aplicação dessas técnicas.
Ressuscitação e Prevenção da Coagulopatia Associada ao Trauma
Protocolos de Transfusão Maciça (MTPs) baseados em dados militares priorizam o uso precoce de hemoderivados, evitando cristaloides. Esses protocolos, agora padrão de atendimento em centros de trauma civis, têm demonstrado redução significativa da mortalidade em pacientes com hemorragia grave.
Evacuação Rápida e Transporte de Longa Distância
As lições aprendidas sobre a segurança e o benefício de sobrevida do transporte de longa distância para pacientes gravemente feridos têm aplicações importantes para civis feridos em áreas rurais, onde podem estar distantes dos centros de trauma de referência.
Reabilitação
O atendimento de lesões complexas em sistemas de trauma civis aprendeu muito com a experiência militar mais recente em relação ao manejo inicial da lesão e às necessidades da recuperação funcional de longo prazo. Estratégias de reabilitação abrangentes e tecnologias de ponta em próteses têm sido fundamentais para a reintegração dos pacientes à sociedade.
Pontos-Chave
- A colaboração entre medicina militar e civil é essencial para a troca de conhecimentos e aprimoramento do atendimento ao trauma
- Técnicas como bandagens hemostáticas e torniquetes, desenvolvidas em cenários de guerra, têm sido amplamente adotadas pela medicina civil
- Protocolos de ressuscitação e transfusão baseados em evidências militares têm melhorado significativamente os desfechos em pacientes com hemorragia grave
- O transporte rápido e seguro de pacientes gravemente feridos, mesmo a longas distâncias, é fundamental para a sobrevivência
- A reabilitação abrangente, com foco na recuperação funcional, é essencial para a reintegração dos pacientes à sociedade
Conclusão
A cirurgia de guerra tem sido um catalisador para o desenvolvimento de técnicas e estratégias inovadoras no tratamento de lesões traumáticas. Ao aplicar essas lições aprendidas no campo de batalha ao cenário da cirurgia de urgência no trauma cívil, podemos melhorar significativamente os desfechos dos pacientes e promover uma recuperação mais rápida e completa.
“A cirurgia de guerra é a mãe de todas as cirurgias.” – John Kirkpatrick
Gostou? Nos deixe um comentário, compartilhe em suas redes sociais e/ou mande sua dúvida pelo Chat On-line em nossa DM do Instagram.
#CirurgiaDeGuerra #CirurgiaDigestivaComplexa #TraumaAbdominal #ReabilitaçãoFuncional #MedicinaDeGuerra
Desafiando a Decadência
O Código de Conduta de Julius Evola e Sua Aplicação na Cirurgia Digestiva Contemporânea
A medicina, especialmente a cirurgia digestiva, exige não apenas habilidades técnicas, mas também uma profunda reflexão ética e filosófica. Em tempos de crescente complexidade e desafios na prática médica, o pensamento de Julius Evola, particularmente seu “código de conduta” expresso em “Cavalgar o Tigre”, oferece uma perspectiva intrigante para cirurgiões digestivos contemporâneos. Este artigo explora como os princípios de Evola podem ser aplicados à prática cirúrgica, promovendo uma abordagem que transcende a mera técnica e se aprofunda na ética e na filosofia do cuidado.
Introdução
A cirurgia digestiva é uma especialidade que lida com condições complexas que afetam o trato gastrointestinal. Os cirurgiões enfrentam não apenas desafios técnicos, mas também dilemas éticos que exigem uma reflexão profunda sobre o papel do médico na sociedade. Evola, em sua análise da condição humana na era moderna, propõe um “código de conduta” que pode ser interpretado como uma orientação para aqueles que buscam não apenas a excelência técnica, mas também uma vida de significado e propósito.
“ego sum qui sum” Ex 3:14
Evola define um “tipo diferenciado” de homem, que se destaca por sua capacidade de transcender as limitações do mundo moderno. Esse conceito é particularmente relevante para cirurgiões digestivos, que muitas vezes se encontram em situações de alta pressão e estresse. A ideia de “transcendência” que Evola propõe pode ser vista como um convite para que os cirurgiões desenvolvam uma consciência mais profunda de si mesmos e do impacto de suas ações.
A Dimensão da Transcendência
A “dimensão da transcendência” de Evola enfatiza a importância de se manter à parte das influências corrosivas da sociedade contemporânea. Para o cirurgião digestivo, isso significa cultivar uma prática que não se limite a resultados cirúrgicos, mas que também considere a experiência do paciente, a ética do cuidado e a responsabilidade social. A prática cirúrgica deve ser uma expressão de um compromisso mais profundo com a vida e a saúde, em vez de uma mera execução de técnicas.
Ascetismo e Autodomínio
Evola fala sobre um “ascetismo natural” que envolve testar a própria força e resiliência. Para o cirurgião, isso pode se traduzir na busca constante pela excelência, enfrentando desafios e aprendendo com as dificuldades. A capacidade de transformar a dor e a resistência em aprendizado é crucial para o desenvolvimento profissional e pessoal. Essa abordagem não apenas melhora as habilidades técnicas, mas também fortalece a ética profissional.
Aplicação na Cirurgia Digestiva
Os princípios de Evola podem ser aplicados de várias maneiras na prática da cirurgia digestiva:
- Autonomia e Responsabilidade: O cirurgião deve assumir a responsabilidade por suas decisões, cultivando uma autonomia que permite a reflexão crítica sobre cada caso.
- Busca pela Excelência: A prática cirúrgica deve ser vista como uma arte, onde a busca pela perfeição é contínua. Isso implica em aceitar desafios e aprender com os erros.
- Ética do Cuidado: A abordagem cirúrgica deve ser centrada no paciente, considerando não apenas a doença, mas a pessoa como um todo. Isso implica em um compromisso com a dignidade e a qualidade de vida do paciente.
- Resiliência Emocional: A capacidade de enfrentar a pressão e o estresse do ambiente cirúrgico é fundamental. O cirurgião deve desenvolver uma mentalidade que permita lidar com a infelicidade e os desafios de forma construtiva.
- Transcendência do Ego: A prática cirúrgica deve ser uma expressão de serviço, onde o ego é colocado de lado em favor do bem-estar do paciente.
Pontos-Chave
- Transcendência: A prática cirúrgica deve ir além da técnica, incorporando uma dimensão ética e filosófica.
- Autodomínio: O desenvolvimento contínuo das habilidades e a resiliência emocional são essenciais para o sucesso.
- Ética do Cuidado: O cirurgião deve ver o paciente como um ser humano integral, não apenas como um caso clínico.
Conclusões Aplicadas à Prática do Cirurgião Digestivo
A aplicação do “código de conduta” de Julius Evola na cirurgia digestiva contemporânea oferece uma abordagem que valoriza a ética, a transcendência e o compromisso com a excelência. Em um mundo onde a medicina muitas vezes se torna mecanicista e desumanizada, a filosofia de Evola pode servir como um guia para cirurgiões que buscam não apenas operar, mas também curar de forma holística. A prática da cirurgia digestiva, quando alinhada a esses princípios, não apenas melhora os resultados clínicos, mas também enriquece a experiência do cirurgião e do paciente, promovendo uma medicina mais humana e significativa.
#CirurgiaDigestiva #JuliusEvola #ÉticaMédica #Transcendência #Autodomínio
“A grandeza de caráter não consiste em não ter paixões, mas em tê-las sob controle.”
Gostou ❔ Nos deixe um comentário ✍️, compartilhe em suas redes sociais e|ou mande sua dúvida pelo 💬 Chat On-line em nossa DM do Instagram.
Relação Médico-Paciente
Como a Conexão Humana Influencia o Sucesso Operatório.
Introdução
A relação médico-paciente é um dos pilares centrais da medicina, especialmente em áreas complexas como a cirurgia do aparelho digestivo. Embora o foco principal de um cirurgião seja a resolução técnica das patologias, a qualidade da interação com o paciente pode influenciar diretamente os resultados clínicos e a satisfação geral do tratamento. Este artigo examina como a construção de um vínculo eficaz e empático entre médico e paciente pode impactar positivamente o sucesso cirúrgico, com base em modelos consagrados de interação médica e evidências contemporâneas da prática cirúrgica.
Desenvolvimento
Desde os tempos antigos, a medicina tem sido guiada por princípios éticos e humanísticos que transcendem o mero conhecimento técnico. Hipócrates, considerado o pai da medicina, já afirmava a importância de cuidar do paciente como um todo, e não apenas da doença. No contexto atual, essa visão se mantém viva, especialmente na cirurgia digestiva, onde procedimentos muitas vezes invasivos e com risco elevado demandam uma abordagem que considere o bem-estar físico e emocional do paciente.
Estudos indicam que uma comunicação aberta e empática pode reduzir a ansiedade pré-operatória em até 30%, melhorar a adesão ao tratamento e diminuir o tempo de recuperação. No Brasil, onde o número de cirurgias digestivas cresce a cada ano, com mais de 150.000 procedimentos realizados anualmente, a habilidade do cirurgião em estabelecer uma relação de confiança com o paciente se torna ainda mais crucial. A adoção de modelos de interação, como a participação mútua descrita por Szasz e Hollender, onde o paciente é encorajado a participar ativamente das decisões médicas, tem se mostrado eficaz em promover melhores resultados.
Modelo de Consulta do Cirurgião Digestivo
O modelo de consulta ideal para o cirurgião digestivo deve ser estruturado de forma a estabelecer uma comunicação clara e empática desde o primeiro contato. Isso inclui:
- Identificação e Apresentação: O cirurgião deve se apresentar claramente, informando seu nome e função, criando um ambiente de confiança desde o início.
- Cumprimento e Ligação Inicial: Cumprimentar o paciente adequadamente e estabelecer uma boa ligação, indo além das questões médicas.
- Questionamento e Exploração: Perguntar sobre os motivos da consulta e explorar tanto os fatores físicos quanto psicossociais que influenciam a condição do paciente.
- Explanação e Orientação: Explicar as razões para os procedimentos diagnósticos e terapêuticos, garantindo que o paciente compreenda todas as etapas do tratamento.
- Encerramento e Reavaliação: Ao final da consulta, verificar se há algo mais que o paciente deseja discutir e revisar os próximos passos.
Valores e Princípios da Relação Médico-Paciente
Na relação médico-paciente, especialmente no contexto cirúrgico, certos valores e princípios são fundamentais:
- Sigilo e Privacidade: A confidencialidade das informações deve ser mantida em todas as circunstâncias, salvo em casos que envolvam um bem maior.
- Respeito ao Pudor: Durante exames e procedimentos, o respeito ao paciente deve ser rigorosamente observado, assegurando conforto e dignidade.
- Justiça e Equidade: O tratamento deve ser justo e equitativo, sem discriminação, com base em normas que garantam uma distribuição apropriada de recursos e atenção.
- Beneficência e Não Maleficência: A conduta do médico deve sempre visar o benefício do paciente, evitando causar danos intencionais.
- Autonomia: Respeitar a autonomia do paciente é crucial, promovendo um diálogo aberto onde o paciente se sinta capaz de tomar decisões informadas sobre seu tratamento.
Componentes da Qualidade na Relação Médico-Paciente
A qualidade da relação médico-paciente é composta por diversos elementos que podem melhorar a interação e os resultados clínicos:
- Empatia: Reduzir a distância entre médico e paciente, tratando-o pelo nome e reconhecendo suas necessidades e desafios.
- Interesse Genuíno: Mostrar interesse genuíno pela condição e bem-estar do paciente, investindo tempo suficiente para ouvi-lo e orientá-lo.
- Tempo de Qualidade: Dedicar o tempo necessário ao paciente, sem apressar a consulta, e proporcionando informações claras e detalhadas.
- Escuta Ativa: Permitir que o paciente fale livremente nos primeiros minutos de consulta, demonstrando que suas preocupações são valorizadas e compreendidas.
- Orientação e Esclarecimento: Garantir que o paciente entenda todos os aspectos de sua condição e tratamento, oferecendo uma visão clara e um plano de ação definido.
Conclusão
A prática da cirurgia digestiva não se limita à sala de operação; ela começa muito antes, na construção de uma relação de confiança entre médico e paciente. Ao adotar uma abordagem centrada no paciente, o cirurgião não apenas melhora os resultados clínicos, mas também fortalece o vínculo humano que é a base da medicina. Assim, a habilidade técnica deve ser sempre acompanhada pela capacidade de escuta e empatia, elementos que, juntos, podem transformar o processo cirúrgico em uma experiência mais positiva para ambos os lados.
Como afirmou Sir William Osler, um dos fundadores da medicina moderna: “O bom médico trata a doença; o grande médico trata o paciente que tem a doença.”
Gostou ❔ Nos deixe um comentário ✍️, compartilhe em suas redes sociais e|ou mande sua dúvida pelo 💬 Chat On-line em nossa DM do Instagram.
#MedicinaCirúrgica #RelaçãoMédicoPaciente #CirurgiaDigestiva #EducaçãoMédica #SaúdeeBemEstar
Cuidados Paliativos em Tumores Biliares
Como Integrar Práticas Cirúrgicas com Abordagens Humanizadas para Melhorar a Qualidade de Vida do Paciente
Introdução
Os tumores biliares, compreendendo o câncer de vesícula biliar e o colangiocarcinoma, apresentam-se como desafios significativos no campo da cirurgia do aparelho digestivo. Essas malignidades raras são frequentemente diagnosticadas em estágios avançados, quando a ressecção curativa não é mais uma opção viável para a maioria dos pacientes. Neste contexto, a integração precoce dos cuidados paliativos torna-se crucial para melhorar a qualidade de vida dos pacientes, abordando tanto os sintomas físicos quanto as necessidades emocionais e espirituais.
Desenvolvimento
A palavra “paliativo” deriva do latim palliare, que significa cobrir com um manto, uma metáfora que reflete a proteção e o alívio oferecidos ao paciente diante de uma doença incurável. No caso dos tumores biliares, onde apenas 20% a 30% dos pacientes com câncer de ducto biliar e 15% a 47% daqueles com câncer de vesícula biliar são candidatos à ressecção cirúrgica, os cuidados paliativos assumem um papel central.
O prognóstico desses pacientes é frequentemente desolador, com taxas de sobrevida de 5 anos inferiores a 5% para o câncer de vesícula biliar e de 2% a 17% para o colangiocarcinoma. Essas estatísticas evidenciam a necessidade urgente de abordagens paliativas que não apenas prolonguem a vida, mas que, acima de tudo, melhorem sua qualidade.

As intervenções paliativas em tumores biliares incluem uma variedade de técnicas, como a colocação de stents biliares, tanto endoscópicos quanto percutâneos, para aliviar a obstrução biliar, radiofrequência para ablação tumoral, terapia fotodinâmica e braquiterapia intraluminal. Cada uma dessas opções é escolhida com base no quadro clínico específico do paciente, buscando-se sempre um equilíbrio entre eficácia e minimização dos riscos.
Aplicação na Cirurgia Digestiva
No cenário da cirurgia digestiva, o papel do cirurgião vai além da remoção tumoral. Em muitos casos, os cirurgiões são os principais responsáveis pela implementação de medidas paliativas que podem incluir desde procedimentos de derivação biliar até a colocação de stents para aliviar sintomas obstrutivos. Além disso, a abordagem multidisciplinar é fundamental para assegurar que o paciente receba um cuidado integral, que envolva não apenas o controle dos sintomas, mas também suporte psicológico e espiritual.
Por exemplo, a inserção de um stent metálico endoscópico, que oferece maior patência a longo prazo em comparação aos stents plásticos, pode ser preferível em casos de obstrução biliar maligna. Outro exemplo é o bloqueio do plexo celíaco, que pode ser realizado para o controle da dor em pacientes com tumores avançados que envolvem o plexo celíaco. Essas intervenções cirúrgicas e endoscópicas são cruciais para manter a qualidade de vida, mesmo quando a cura não é mais possível.
Pontos-Chave
- Diagnóstico Tardio: A maioria dos tumores biliares é diagnosticada em estágio avançado, quando as opções curativas são limitadas.
- Importância dos Cuidados Paliativos: A introdução precoce dos cuidados paliativos é essencial para melhorar a qualidade de vida dos pacientes com tumores biliares.
- Intervenções Paliativas: Técnicas como a colocação de stents, ablação por radiofrequência, e terapia fotodinâmica são opções importantes no manejo paliativo.
- Abordagem Multidisciplinar: O cuidado paliativo eficaz em tumores biliares requer uma abordagem que envolva cirurgiões, oncologistas, endoscopistas, radiologistas e especialistas em cuidados paliativos.
Conclusões Aplicadas à Prática do Cirurgião Digestivo
Para o cirurgião digestivo, é imperativo compreender que a eficácia do tratamento paliativo não se mede apenas em termos de sobrevivência, mas na capacidade de aliviar sintomas e melhorar o bem-estar do paciente. O papel do cirurgião evolui para incluir a gestão de técnicas paliativas, que devem ser integradas precocemente no curso da doença. A educação contínua sobre essas técnicas e o desenvolvimento de habilidades de comunicação para discutir prognóstico e expectativas com os pacientes e suas famílias são igualmente cruciais. Assim, ao ampliar o foco para além da intervenção curativa, o cirurgião digestivo pode fornecer um cuidado mais compassivo e centrado no paciente, alinhado com as melhores práticas em cuidados paliativos.
“Curar quando possível, aliviar frequentemente, consolar sempre.” – Edward Livingston Trudeau
Gostou ❔Nos deixe um comentário ✍️, compartilhe em suas redes sociais e|ou mande sua dúvida pelo 💬 Chat On-line em nossa DM do Instagram.
Hashtags: #CuidadosPaliativos #TumoresBiliares #CirurgiaDigestiva #Oncologia #QualidadedeVida
Cuidados Paliativos na Cirurgia do Aparelho Digestivo
Integração Essencial para a Prática Cirúrgica Contemporânea
Introdução
Os cuidados paliativos (CP) desempenham um papel vital na medicina contemporânea, particularmente em pacientes com doenças graves do aparelho digestivo. Tradicionalmente associados ao cuidado de pacientes em fase terminal, os CP evoluíram para uma abordagem mais ampla e integrada, voltada para o alívio do sofrimento e a melhoria da qualidade de vida, independentemente do estágio da doença. Este artigo tem como objetivo esclarecer a importância dos CP na cirurgia digestiva, explorando como essa prática pode ser incorporada ao manejo clínico de forma eficaz e humanizada.
Desenvolvimento
Até o início do século XXI, os CP eram erroneamente percebidos como sinônimo de cuidados exclusivamente para pacientes em fase terminal. Essa visão dicotômica, em que o paciente “virava” um caso de CP apenas ao se aproximar da morte, tem sido progressivamente superada. Em 2002, a Organização Mundial da Saúde (OMS) redefiniu os CP como uma abordagem para o alívio do sofrimento em pacientes e suas famílias diante de doenças que ameaçam a vida, independentemente do estágio da doença. Essa mudança de paradigma promoveu uma integração entre tratamentos curativos e paliativos, destacando que os CP são uma competência essencial para todos os profissionais de saúde.
No contexto da cirurgia do aparelho digestivo, essa integração se torna ainda mais crucial. Pacientes com câncer gastrointestinal, por exemplo, frequentemente enfrentam desafios físicos e emocionais que vão além do tratamento cirúrgico. A aplicação dos princípios dos CP permite aos cirurgiões digestivos oferecer um cuidado mais holístico, abordando não apenas a doença, mas também o impacto dela na vida do paciente e de sua família.
Aplicação na Cirurgia Digestiva
A aplicação dos cuidados paliativos na cirurgia digestiva envolve várias etapas críticas. Desde o diagnóstico inicial, o cirurgião deve incorporar uma abordagem paliativa que englobe o controle eficaz dos sintomas, a comunicação clara sobre prognóstico e a definição conjunta dos objetivos de cuidado.
- Controle de Sintomas: Dor, náuseas, fadiga e outros sintomas comuns em pacientes com doenças digestivas avançadas devem ser avaliados e tratados de forma proativa. Técnicas como analgesia com opioides, tratamentos adjuvantes para dores neuropáticas e intervenções específicas, como a radioterapia para metástases ósseas, são essenciais para o manejo adequado desses pacientes.
- Prognóstico: A incerteza no prognóstico é um desafio, especialmente em pacientes graves. No entanto, essa incerteza pode ser abordada de maneira estruturada, usando escalas padronizadas e estimativas probabilísticas, que ajudam a guiar as decisões de tratamento.
- Comunicação de Objetivos de Cuidado: Discutir e definir os objetivos de cuidado é uma etapa fundamental. Para muitos pacientes com doenças do aparelho digestivo, as decisões sobre intervenções cirúrgicas ou a limitação de tratamentos invasivos devem ser alinhadas com seus valores e preferências pessoais.

Pontos-Chave para o Cirurgião Digestivo
- Integração Precoce dos CP: Iniciar os cuidados paliativos desde o diagnóstico de uma doença grave melhora a qualidade de vida do paciente e facilita a tomada de decisões.
- Controle Adequado da Dor: Avaliar sistematicamente a dor e utilizar uma combinação de analgesia preemptiva e de resgate é crucial para o conforto do paciente.
- Comunicação Clara e Empática: Explicar o prognóstico e as opções de tratamento de forma clara, respeitando as emoções e expectativas dos pacientes e suas famílias.
- Planejamento de Cuidados: Definir objetivos de cuidado com base nas preferências do paciente, seja priorizando o conforto ou optando por tratamentos agressivos.
- Uso Adequado de Opioides: Conhecimento sobre a meia-vida, equipotência e efeitos colaterais dos opioides é essencial para evitar complicações.
- Abordagem Multidisciplinar: Trabalhar em conjunto com outros especialistas, como oncologistas e anestesiologistas, para oferecer um cuidado integrado.
- Avaliação Funcional: Monitorar continuamente a funcionalidade do paciente para ajustar as intervenções conforme necessário.
- Gestão de Sintomas Não-Dolorosos: Controle de náuseas, fadiga e dispneia são tão importantes quanto o controle da dor.
- Evitar Tratamentos Fúteis: Identificar quando as intervenções cirúrgicas ou outras medidas invasivas não trarão benefícios significativos ao paciente.
- Educação Continuada: Manter-se atualizado sobre as melhores práticas em cuidados paliativos para garantir que os pacientes recebam o melhor cuidado possível.
Conclusão
A integração dos cuidados paliativos na prática cirúrgica digestiva não apenas melhora a qualidade de vida dos pacientes, mas também promove uma prática médica mais ética, centrada no paciente e em sua dignidade. O cirurgião digestivo que domina essas competências está melhor equipado para enfrentar os desafios clínicos e emocionais de seus pacientes, contribuindo para um cuidado mais humano e eficaz. Como disse William Osler, um dos pais da medicina moderna:
“A boa medicina é a que cuida do paciente como um todo, e não apenas da doença.”
Gostou? Nos deixe um comentário ✍️ , compartilhe em suas redes sociais e|ou mande sua dúvida pelo 💬 Chat On-line em nossa DM do Instagram.
Hashtags: #CuidadosPaliativos #CirurgiaDigestiva #MedicinaPaliativa #EducaçãoMédica #QualidadeDeVida
Cicatrização de Feridas
A cicatrização de feridas operatórias é um processo fundamental para o sucesso de qualquer intervenção cirúrgica, especialmente nas complexas cirurgias do aparelho digestivo. Este post visa explorar detalhadamente o processo de cicatrização, destacando os mecanismos biológicos envolvidos e sua aplicação prática na cirurgia digestiva, com enfoque em fornecer uma visão compreensiva para estudantes de medicina, residentes em cirurgia geral e pós-graduandos em cirurgia do aparelho digestivo.
A Complexidade da Cicatrização em Cirurgias Digestivas
A cicatrização de uma ferida operatória é um fenômeno biológico essencial que visa restaurar a integridade tecidual após uma intervenção cirúrgica. Em cirurgias do aparelho digestivo, onde o risco de complicações infecciosas é elevado, entender as fases e os fatores que influenciam a cicatrização é crucial para otimizar os resultados e prevenir complicações como deiscências, infecções e formação de fístulas.
Fisiologia e Fases da Cicatrização Operatória
Hemostasia e Fase Inflamatória
Imediatamente após o trauma cirúrgico, ocorre a fase de hemostasia, na qual a vasoconstrição e a ativação da cascata de coagulação interrompem o sangramento. Esse processo não só previne a hemorragia como também forma uma matriz de fibrina, que serve como um arcabouço inicial para a cicatrização. A fase inflamatória segue imediatamente, durando entre 1 a 4 dias. Durante esse período, células inflamatórias como neutrófilos e macrófagos migram para o local da ferida, desempenhando um papel vital na fagocitose de detritos celulares e na liberação de citocinas que promovem a reparação tecidual.
Fase Proliferativa e Angiogênese
A fase proliferativa, que inicia após o terceiro ou quarto dia, envolve a migração e proliferação de fibroblastos, células mesenquimais e a formação de novos vasos sanguíneos—a angiogênese. Esses processos são críticos para a formação do tecido de granulação, que preenche a ferida e estabelece uma nova matriz extracelular rica em colágeno.
Remodelamento e Maturação
Finalmente, a fase de remodelamento, que pode se estender por meses, é caracterizada pela deposição de colágeno e reorganização da matriz extracelular. Nesta fase, o tecido cicatricial se fortalece, atingindo cerca de 80% da resistência do tecido original após seis meses.

Aplicação na Cirurgia Digestiva: Desafios e Abordagens
Na cirurgia do aparelho digestivo, as feridas operatórias apresentam desafios específicos devido ao alto risco de contaminação e infecção, especialmente em anastomoses intestinais. Segundo estatísticas do Ministério da Saúde, as infecções de sítio cirúrgico (ISC) estão entre as principais complicações pós-operatórias no Brasil, com uma incidência de aproximadamente 11,7% em cirurgias abdominais.
Fechamento Primário e Secundário: Escolhas Estratégicas
O fechamento primário, onde as margens da ferida são aproximadas diretamente, é ideal em cirurgias limpas, com baixo risco de infecção. No entanto, em situações onde há contaminação, como em ressecções intestinais com peritonite, o fechamento secundário, onde a ferida é deixada aberta para cicatrizar por segunda intenção, pode ser mais seguro.
Uso de Tecnologias Avançadas
O uso de produtos como hidrocolóides, hidrofibras e até mesmo fatores de crescimento recombinantes tem sido explorado para melhorar a cicatrização de feridas complexas em cirurgias digestivas. Estudos recentes indicam que esses tratamentos podem acelerar a formação de tecido de granulação e reduzir a taxa de complicações infecciosas, especialmente em pacientes com comorbidades como diabetes.
Pontos-Chave
- A cicatrização de feridas operatórias segue um processo ordenado de hemostasia, inflamação, proliferação e remodelamento.
- Nas cirurgias digestivas, o manejo adequado da cicatrização é crucial para prevenir complicações como infecções e deiscências.
- O fechamento primário é preferível em condições limpas, enquanto o fechamento secundário é recomendado em casos de alta contaminação.
- Avanços tecnológicos, como o uso de fatores de crescimento e novos materiais de curativos, oferecem promissoras abordagens para melhorar a cicatrização de feridas em cirurgias digestivas.
Aplicações na Prática Cirúrgica
A compreensão detalhada dos processos de cicatrização e a aplicação adequada das técnicas de fechamento e tratamento de feridas são essenciais para o sucesso em cirurgias do aparelho digestivo. Cirurgiões devem estar atentos às novas tecnologias e abordagens para otimizar os resultados pós-operatórios e reduzir as taxas de complicações, garantindo, assim, uma recuperação mais rápida e eficaz para seus pacientes.
Como bem disse o cirurgião pioneiro Joseph Lister: “A cicatrização das feridas é o teste do cirurgião.” A excelência no cuidado pós-operatório é tão vital quanto a habilidade na sala de cirurgia.
Gostou ❔ Nos deixe um comentário ✍️, compartilhe em suas redes sociais e|ou mande sua dúvida pelo 💬 Chat On-line em nossa DM do Instagram.
#CicatrizaçãoCirúrgica #CirurgiaDigestiva #CuidadosPósOperatórios #CicatrizaçãoDeFeridas #MedicinaCirúrgica
Formação Acadêmica na Cirurgia do Aparelho Digestivo
“Não somente Cirurgiões…”
A formação acadêmica na cirurgia do aparelho digestivo é um tema de grande relevância para estudantes de medicina e residentes em cirurgia geral. Neste contexto, a importância do Mestrado e Doutorado profissionais se destaca como um pilar fundamental para o desenvolvimento de habilidades e competências necessárias para a prática cirúrgica de excelência. Este artigo busca explorar a formação acadêmica na cirurgia digestiva, abordando a importância da pesquisa, a aplicação prática dos conhecimentos adquiridos e as conclusões que podem ser aplicadas na prática clínica.
Introdução
A cirurgia do aparelho digestivo é uma especialidade que exige não apenas habilidades técnicas, mas também um profundo entendimento dos avanços científicos e tecnológicos. A formação acadêmica, especialmente por meio de programas de Mestrado e Doutorado profissionais, é essencial para preparar cirurgiões que possam enfrentar os desafios contemporâneos da medicina. Segundo dados da Coordenação de Aperfeiçoamento de Pessoal de Nível Superior (Capes), o Brasil tem visto um aumento significativo no número de programas de pós-graduação na área da saúde, refletindo a crescente demanda por profissionais qualificados.

Desenvolvimento
Mestrado e Doutorado Profissionais
Os programas de Mestrado e Doutorado profissionais foram criados para atender a uma demanda crescente por profissionais que possam aplicar o conhecimento científico em contextos práticos. O Mestrado profissional, regulamentado pela Lei n. 9.394 de 1996 e com diretrizes estabelecidas em 2009, visa a formação de profissionais com uma abordagem focada na aplicação prática do conhecimento. Este tipo de formação é particularmente relevante para cirurgiões, que frequentemente se deparam com desafios que exigem soluções inovadoras e práticas. O Doutorado profissional, por sua vez, tem ganhado espaço nas últimas décadas, refletindo uma tendência global. Em muitos países, essa modalidade já é uma realidade consolidada, com instituições de ensino superior oferecendo programas que integram pesquisa e prática. No Brasil, a criação de programas de Doutorado profissional é uma resposta à necessidade de aprofundar a formação de cirurgiões, permitindo que eles se tornem líderes em suas áreas de atuação.
Pesquisa Científica
A pesquisa é um componente crucial na formação do cirurgião, pois permite o desenvolvimento do raciocínio crítico e a atualização constante dos conhecimentos. Estudantes e residentes que se envolvem em projetos de pesquisa têm a oportunidade de aplicar o método científico à prática clínica, contribuindo para a melhoria dos cuidados de saúde. A produção científica brasileira na área da saúde tem avançado, mas ainda existem desafios a serem superados, como a aplicação prática dos novos conhecimentos em problemas relevantes da população. Estudos mostram que a pesquisa não apenas aprimora as habilidades técnicas dos cirurgiões, mas também os capacita a identificar e resolver problemas complexos no ambiente clínico. A incorporação de metodologias de pesquisa, como análise crítica e design thinking, pode levar a melhorias significativas na eficiência dos serviços de saúde.
Publicações
A publicação dos resultados de pesquisa é um aspecto crucial para o avanço da ciência e da medicina. Publicar em periódicos de alto impacto é uma forma de disseminar o conhecimento e contribuir para o progresso da área. O processo de revisão por pares garante a qualidade e a integridade dos estudos publicados, permitindo que os cirurgiões compartilhem suas descobertas com a comunidade científica. Além disso, a publicação de artigos científicos é uma maneira de os cirurgiões se estabelecerem como especialistas em suas áreas. A produção de conhecimento não se limita a artigos, mas pode incluir patentes, projetos técnicos e inovações que impactem diretamente a prática clínica. A diversidade de formatos para a apresentação de resultados de pesquisa é um reflexo da necessidade de adaptação às demandas do mercado e da sociedade.
Aplicação na Cirurgia Digestiva
Os conhecimentos adquiridos durante a formação acadêmica são diretamente aplicáveis na prática da cirurgia digestiva. O Mestrado e Doutorado profissionais capacitam os cirurgiões a desenvolver novas técnicas e processos, além de promover a inovação no atendimento ao paciente. A formação não se limita à teoria, mas inclui a aplicação prática em ambientes clínicos, onde os cirurgiões podem identificar e solucionar problemas reais. Por exemplo, a utilização de metodologias como design thinking e análise crítica de processos pode levar a melhorias significativas na eficiência dos serviços de saúde.
Pontos-chave
- Integração entre teoria e prática: A formação acadêmica deve equilibrar o conhecimento teórico com a experiência prática, permitindo que os cirurgiões se tornem profissionais completos.
- Desenvolvimento contínuo: A educação médica não termina com a graduação; a participação em programas de pós-graduação é vital para a atualização e o aprimoramento das habilidades.
- Contribuição para a saúde pública: Cirurgiões bem formados têm o potencial de impactar positivamente a saúde da população, desenvolvendo soluções inovadoras para problemas de saúde.
- Importância da pesquisa e publicação: A pesquisa e a publicação científica são fundamentais para o avanço da medicina e a melhoria da prática cirúrgica.
Conclusões Aplicadas à Prática do Cirurgião Digestivo
A formação acadêmica na cirurgia do aparelho digestivo, através de Mestrados e Doutorados profissionais, é essencial para o desenvolvimento de cirurgiões competentes e inovadores. A pesquisa e a aplicação prática dos conhecimentos adquiridos são fundamentais para enfrentar os desafios da medicina moderna. Com uma formação sólida, os cirurgiões não apenas melhoram suas habilidades técnicas, mas também se tornam agentes de mudança no sistema de saúde, contribuindo para a melhoria da qualidade de vida dos pacientes. A frase de J. Robert Oppenheimer, um dos grandes nomes da ciência, resume bem essa busca por excelência.
“A ciência não é apenas uma disciplina, mas uma forma de pensar, uma maneira de questionar o mundo ao nosso redor.”
ACESSE AQUI NOSSAS PUBLICAÇÕES
Gostou ❔ Nos deixe um comentário ✍️, compartilhe em suas redes sociais e|ou mande sua dúvida pelo 💬 Chat On-line em nossa DM do Instagram.#FormaçãoCirurgiã #CirurgiaDigestiva #EducaçãoMédica #MestradoProfissional #InovaçãoEmSaúde
Mindset Cirúrgico Aprimorado
Por que alguns médicos alcançam a excelência em assistência médica enquanto outros permanecem na mediana? Este é um questionamento essencial para qualquer profissional de saúde, especialmente para aqueles que aspiram à maestria na cirurgia do aparelho digestivo. Inspirado nos princípios de Napoleon Hill em “Pense e Enriqueça,” este artigo explora como essas leis podem ser aplicadas para transformar a prática cirúrgica e melhorar a assistência médica prestada aos pacientes.
Introdução
A medicina é uma arte e uma ciência, e a excelência na prática clínica vai além do conhecimento técnico. Envolve a aplicação de princípios que impulsionam o sucesso, tanto no tratamento dos pacientes quanto na evolução profissional. Napoleon Hill, em seu clássico “Pense e Enriqueça,” descreveu 12+1 leis que, quando aplicadas, podem levar ao sucesso em qualquer campo. Adaptamos essas leis ao contexto da assistência médica, mostrando como elas podem guiar um cirurgião do aparelho digestivo para um patamar elevado de prática.
Desenvolvimento
- Desejo Ardente e Fé na Prática Médica: Assim como o desejo ardente é o ponto de partida para qualquer conquista, na medicina, é o desejo de proporcionar o melhor cuidado que impulsiona o médico a superar obstáculos. A fé na própria capacidade de melhorar constantemente e alcançar a excelência é fundamental para um cirurgião do aparelho digestivo. Esta crença deve estar enraizada, motivando o médico a buscar o conhecimento especializado e aplicar técnicas inovadoras.
- Autossugestão e Conhecimento Especializado: A autossugestão, ou a prática de repetição de ideias positivas, pode ser vista na preparação mental antes de procedimentos cirúrgicos. Reforçar mentalmente as habilidades e a confiança contribui para uma performance cirúrgica superior. Aliado a isso, o conhecimento especializado é vital. Cirurgiões que se dedicam ao aprendizado contínuo, especializando-se em técnicas avançadas e tratamentos inovadores, são aqueles que se destacam no campo.
- Imaginação e Planejamento Organizado: A imaginação, no contexto médico, pode ser traduzida como a capacidade de visualizar soluções criativas para desafios clínicos complexos. Por exemplo, adaptar técnicas cirúrgicas para pacientes com condições anatômicas únicas requer uma imaginação prática e clínica. Entretanto, sem planejamento organizado, a imaginação se perde. Portanto, a elaboração de planos cirúrgicos detalhados e a organização dos recursos necessários são indispensáveis para a execução bem-sucedida das operações.
- Persistência e Decisão: A persistência é uma característica crítica para os profissionais de saúde. Diante de complicações cirúrgicas, é a persistência que permite ao cirurgião manter o foco e buscar soluções eficazes. A decisão rápida e assertiva também é essencial, especialmente em emergências, onde o tempo é um fator crucial. Estatísticas brasileiras mostram que a rápida decisão em cirurgias de emergência pode reduzir a mortalidade em até 25%, destacando a importância desse princípio.
- O Poder da Mente Mestra na Cirurgia: Trabalhar em equipe é a essência da cirurgia moderna. A colaboração com outros especialistas, desde anestesiologistas e enfermeiros, forma uma ‘Mente Mestra’ que eleva o nível de cuidado prestado. Cirurgiões que cultivam relações profissionais positivas e trabalham bem em equipe tendem a ter melhores resultados cirúrgicos.
Aplicação na Cirurgia Digestiva
No contexto da cirurgia do aparelho digestivo, aplicar esses princípios pode fazer a diferença entre uma prática comum e uma extraordinária. Um cirurgião que deseja aprimorar sua assistência médica deve, primeiramente, cultivar um desejo intenso de excelência. Esse desejo deve ser apoiado pela fé em sua capacidade de melhorar, pela constante busca por conhecimento especializado e pela prática de autossugestão positiva. O planejamento organizado de cada procedimento, aliado à capacidade de decisão rápida e à persistência em face dos desafios, são fundamentais para o sucesso na sala de cirurgia. Além disso, formar e manter uma equipe coesa e colaborativa é essencial para proporcionar uma assistência médica de alta qualidade.
Pontos-chave
- Desejo Ardente e Fé: A motivação e a crença na capacidade de evolução são a base para o sucesso na medicina.
- Autossugestão e Conhecimento Especializado: A preparação mental e o aprendizado contínuo são vitais para a excelência cirúrgica.
- Imaginação e Planejamento Organizado: Soluções criativas e um planejamento cuidadoso são essenciais para o sucesso cirúrgico.
- Persistência e Decisão: Manter o foco e tomar decisões rápidas são habilidades críticas em situações de emergência.
- Poder da Mente Mestra: A colaboração eficaz em equipe é indispensável para a prática cirúrgica de alta qualidade.
Conclusões Aplicadas à Prática do Cirurgião Digestivo
Aplicar os princípios de Napoleon Hill no contexto da cirurgia digestiva pode transformar a prática médica, elevando a qualidade da assistência prestada e contribuindo para melhores desfechos clínicos. Ao incorporar esses conceitos, o cirurgião não só melhora sua técnica, mas também enriquece sua prática com um sentido mais profundo de propósito e realização.
Como disse William Osler, um dos grandes nomes da medicina: “A prática da medicina é uma arte, não um comércio; uma vocação, não um negócio; e, do mesmo modo que outras artes liberais, exige uma dedicação completa, pois trata-se de uma arte de vida ou morte.”
Gostou ❔ Nos deixe um comentário ✍️, compartilhe em suas redes sociais e|ou mande sua dúvida pelo 💬 Chat On-line em nossa DM do Instagram.
Hashtags:
CirurgiaDigestiva #ExcelenciaMedica #DesenvolvimentoProfissional #AssistenciaMedica #MedicinaEArte
Falência Hepática Terminal: Aspectos Clínicos e Implicações Cirúrgicas
Introdução
A falência hepática terminal é uma síndrome clínica grave, comumente associada a doenças hepáticas crônicas, particularmente a cirrose. Ela abrange tanto formas agudas, como a hepatite fulminante, quanto a falência hepática aguda sobre crônica, levando a altas taxas de mortalidade. Essa condição se apresenta com uma constelação de sintomas e sinais indicativos de insuficiência hepática, destacando-se pela sua importância epidemiológica devido à sua frequência, impacto na morbidade e mortalidade, e ao consumo substancial de recursos de saúde.
No Brasil, a carga de cirrose causada pelo vírus da hepatite C ocupava a 22ª posição em 1990 em termos de Anos de Vida Perdidos (AVP). Em 2010, subiu para a 15ª posição, enquanto a cirrose induzida pelo álcool subiu da 32ª para a 25ª posição, destacando a crescente prevalência das principais causas de falência hepática crônica. As principais etiologias da cirrose incluem abuso crônico de álcool, infecção pelo vírus da hepatite C e esteato-hepatite não alcoólica (NASH). A falência hepática aguda, por sua vez, é desencadeada principalmente por infecção pelo vírus da hepatite A e hepatite medicamentosa.
Desenvolvimento
A cirrose representa o estágio patológico final de uma variedade de agressões hepáticas crônicas. Histologicamente, é caracterizada por fibrose extensa, acompanhada pela formação de nódulos regenerativos, levando à hipertensão portal e à falência hepática. O fígado é central para diversas funções vitais, incluindo a síntese de proteínas (albumina e fatores de coagulação), produção de glicose durante o jejum (gliconeogênese hepática), síntese de lipídios e lipoproteínas, e a biotransformação de substâncias endógenas (amônia, hormônios esteroides, bilirrubinas) e exógenas (drogas e toxinas).
O diagnóstico clínico da insuficiência hepática baseia-se principalmente na presença de fatores de risco para doença hepática crônica, sintomas gerais e neuropsiquiátricos, e achados de exame físico sugestivos de falência hepática. Ao contrário da insuficiência renal, onde marcadores quantificáveis como ureia e creatinina estão disponíveis, a insuficiência hepática é avaliada por meio de sintomas, achados físicos e marcadores indiretos de disfunção hepática, como hipoalbuminemia e tempo de protrombina prolongado.
Pacientes com cirrose podem se apresentar clinicamente com cirrose compensada ou descompensada. A cirrose compensada é frequentemente diagnosticada incidentalmente ou durante a investigação de sintomas inespecíficos como mal-estar geral, anorexia, perda de peso, fraqueza ou dispepsia. Em contraste, a cirrose descompensada se manifesta com icterícia, ascite, encefalopatia hepática ou hemorragia varicosa.
Aplicação na Cirurgia Digestiva
A falência hepática terminal impõe desafios significativos no manejo cirúrgico de pacientes com doenças digestivas. Os cirurgiões devem avaliar cuidadosamente o grau de disfunção hepática e seu impacto potencial nos resultados cirúrgicos. O transplante hepático continua sendo o tratamento definitivo para pacientes com falência hepática terminal; no entanto, o momento da cirurgia, a otimização pré-operatória e o manejo de complicações como hipertensão portal e coagulopatia são fundamentais. Os cirurgiões devem estar atentos a sinais clínicos como eritema palmar, telangiectasias, ginecomastia e atrofia testicular, que, embora não exclusivos da doença hepática, são altamente sugestivos de cirrose. Asterixis, ou “tremor das asas,” frequentemente indica doença hepática avançada e encefalopatia hepática, servindo como um marcador de mau prognóstico.

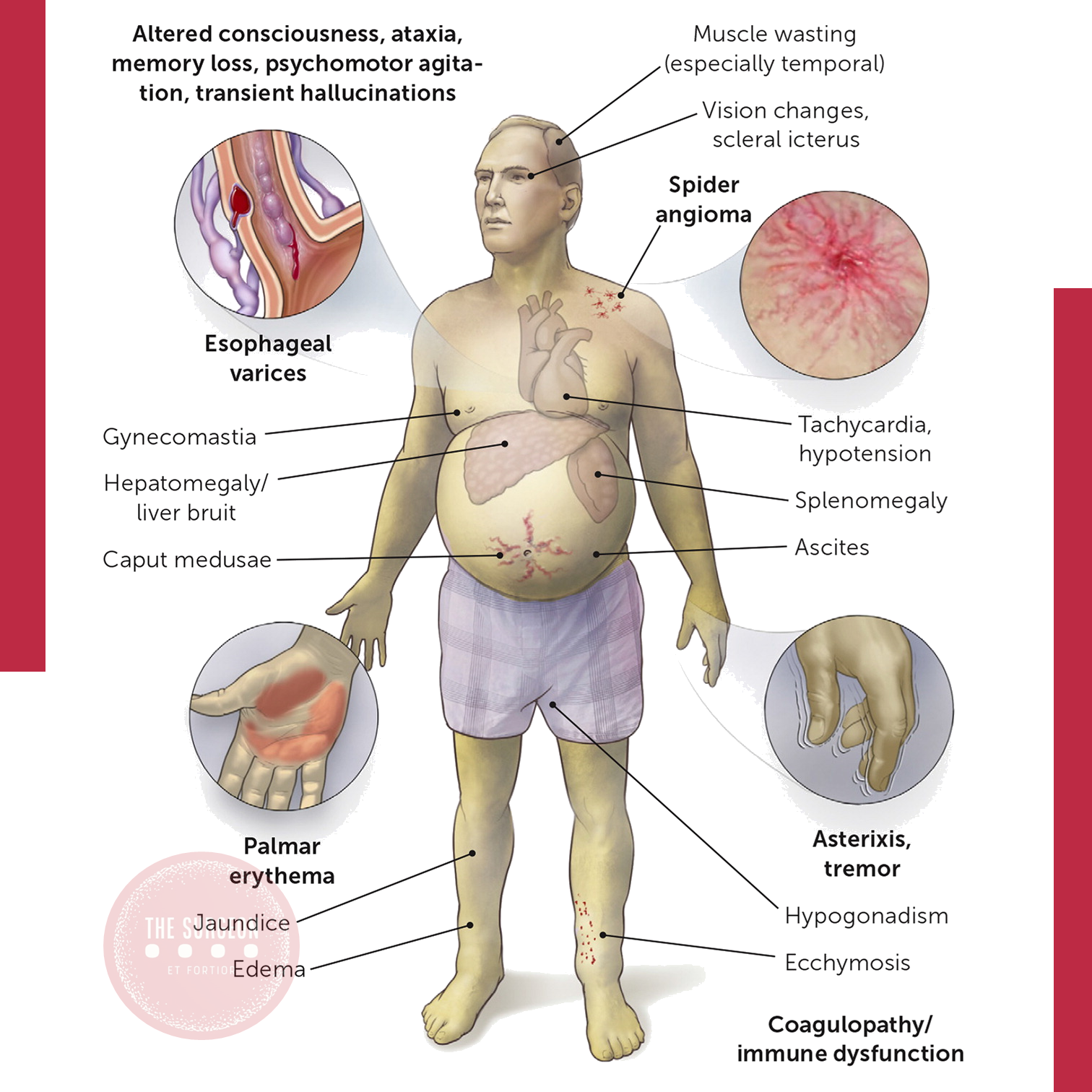
Pontos-Chave
- A falência hepática terminal, frequentemente resultante de doença hepática crônica, é uma condição crítica com alta morbidade e mortalidade.
- A cirrose é o resultado patológico comum de diversas agressões crônicas ao fígado, caracterizada por fibrose e nódulos regenerativos.
- O diagnóstico de insuficiência hepática é complexo, baseando-se em sinais clínicos, sintomas e marcadores indiretos da função hepática.
- Na prática cirúrgica, a falência hepática requer avaliação pré-operatória cuidadosa e manejo adequado, especialmente no contexto do transplante hepático.
- Sinais clínicos importantes incluem eritema palmar, telangiectasias, ginecomastia e asterixis, que ajudam no diagnóstico e prognóstico da doença hepática.
Conclusões Aplicadas à Prática Cirúrgica Digestiva
O manejo de pacientes com falência hepática terminal na cirurgia digestiva exige uma abordagem multidisciplinar, equilibrando os riscos e benefícios da intervenção cirúrgica. O transplante hepático, embora ofereça uma cura potencial, requer planejamento meticuloso e consideração de fatores específicos do paciente, como a gravidade da disfunção hepática e a presença de comorbidades. Os cirurgiões devem estar atentos às sutis manifestações clínicas da falência hepática e adaptar sua abordagem para otimizar os resultados dos pacientes.
Como disse Hipócrates: “Curar é uma questão de tempo, mas às vezes também é uma questão de oportunidade.” O mesmo se aplica ao manejo cirúrgico da falência hepática terminal — tempo e oportunidade são fundamentais.
Gostou ❔ Nos deixe um comentário ✍️, compartilhe em suas redes sociais e|ou mande sua dúvida pelo 💬 Chat On-line em nossa DM do Instagram.
#FalenciaHepatica #Cirrose #CirurgiaDigestiva #InsuficienciaHepatica #EducacaoMedica
Estilos de Mentoria na Cirurgia
Explorando as Diferenças e Aplicações
No campo da cirurgia, a mentoria desempenha um papel crucial no desenvolvimento profissional dos cirurgiões. Entretanto, entender as nuances entre os diferentes estilos e tipos de mentoria é fundamental para maximizar o impacto dessa relação. Kashiwagi descreve uma série de estilos de mentoria que podem ser aplicados de acordo com as necessidades específicas do mentor e do mentee. Este artigo explora esses estilos e discute como eles podem ser aplicados eficazmente na prática cirúrgica.
Introdução
A mentoria não é uma abordagem única. Diferentes estilos de interação entre mentor e mentee podem ser adotados dependendo dos objetivos da mentoria e das características individuais dos envolvidos. É importante diferenciar entre “tipos” e “estilos” de mentoria: enquanto os tipos referem-se ao escopo e à organização do programa de mentoria, os estilos referem-se ao processo real de interação entre mentor e mentee. Vamos nos concentrar nos principais estilos de mentoria descritos por Kashiwagi e suas implicações para a cirurgia.
Estilos de Mentoria
Dyad
O estilo mais tradicional de mentoria, a “Dyad”, envolve uma relação direta entre um mentor e um mentee. Neste modelo, geralmente é o mentee quem seleciona o mentor, permitindo um maior controle sobre o processo de mentoria. Este estilo é comum em ambientes onde há um número suficiente de mentores disponíveis e onde o mentee tem clareza sobre suas necessidades de orientação.
Peer
No estilo “Peer”, a mentoria ocorre entre indivíduos de idades, experiências e níveis hierárquicos semelhantes. Esse modelo é particularmente útil em contextos em que a mentoria hierárquica tradicional não é ideal ou em ambientes onde há uma escassez de mentores seniores eficazes e comprometidos. Na cirurgia, este estilo pode ser valioso para residentes que estão em fases semelhantes de treinamento, permitindo uma troca de experiências e apoio mútuo.
Facilitated Peer
Uma variação do modelo “Peer” é o “Facilitated Peer”, no qual um mentor sênior supervisiona o grupo de mentoria entre pares. Este estilo combina a abordagem colaborativa do peer mentoring com a orientação e supervisão de um mentor mais experiente, criando um equilíbrio entre autonomia e suporte.
Speed
O estilo “Speed” refere-se a uma interação única e breve entre mentor e mentee, geralmente com duração de 10 a 15 minutos, para determinar se uma relação de mentoria seria benéfica para ambas as partes. Esse estilo pode ser útil em conferências ou eventos profissionais, onde há oportunidade de realizar várias dessas interações rápidas, permitindo ao mentee explorar múltiplas possibilidades de mentoria.
Functional
No estilo “Functional”, o mentor é emparelhado com o mentee para fornecer orientação em um projeto específico. Este estilo é altamente focado e orientado para resultados, ideal para situações onde o mentee precisa de assistência em um aspecto particular de seu trabalho, como a condução de uma pesquisa ou o desenvolvimento de uma nova técnica cirúrgica.
Group
O estilo “Group” envolve a mentoria de um grupo de mentees por vários mentores seniores, possivelmente de diferentes áreas de especialização. Este modelo pode ser particularmente eficaz na cirurgia, onde diferentes aspectos de uma condição clínica complexa podem ser abordados por especialistas em áreas complementares, proporcionando uma formação mais holística para o mentee.
Distance
No estilo “Distance”, o mentor é recrutado de uma instituição geograficamente separada da do mentee. Com o avanço da tecnologia, este estilo de mentoria tem se tornado cada vez mais viável, permitindo que mentees acessem orientação de especialistas de renome mundial, independentemente da localização física. Na cirurgia, isso pode significar acesso a técnicas ou conhecimentos especializados que não estão disponíveis localmente.
Aplicação na Cirurgia
Na prática da cirurgia, a escolha do estilo de mentoria deve ser cuidadosamente considerada em função das necessidades do mentee e dos recursos disponíveis. Por exemplo, um residente em início de carreira pode se beneficiar mais de uma abordagem “Dyad”, enquanto um cirurgião mais experiente, procurando desenvolver uma nova área de especialização, pode preferir um estilo “Functional” ou “Group”. É igualmente importante reconhecer que, em muitos casos, diferentes estilos de mentoria podem ser combinados ao longo da carreira de um cirurgião. Por exemplo, um cirurgião pode começar com uma mentoria “Dyad” e, conforme progride, envolver-se em “Peer” mentoring ou até mesmo em uma mentoria “Distance” para ampliar seu conhecimento em áreas específicas.
Conclusão
Os estilos de mentoria descritos por Kashiwagi oferecem uma estrutura valiosa para cirurgiões que buscam orientação em diferentes fases de suas carreiras. Compreender essas opções e aplicá-las de forma estratégica pode ser a chave para o sucesso profissional e o desenvolvimento contínuo na cirurgia.
“O verdadeiro mentor não apenas transmite conhecimento, mas também inspira a busca constante pelo aprimoramento.” – William Osler.
Gostou? Deixe um comentário ✍️, compartilhe em suas redes sociais e/ou mande suas dúvidas pelo 💬 Chat On-line em nossa DM do Instagram.
Hashtags: #EstilosDeMentoria #Cirurgia #MentoriaMedica #DesenvolvimentoProfissional #EducaçãoContinuada
Desafios da Mentoria Cirúrgica
Como Escolher o Mentor Ideal?
A mentoria é um pilar fundamental na formação dos cirurgiões. Contudo, encontrar o mentor ideal que não só compreenda as nuances da cirurgia, mas que também esteja alinhado com os valores e expectativas do mentee, é um desafio que não pode ser subestimado. Neste artigo, abordaremos os principais fatores que podem impactar a relação entre mentor e mentee, explorando como esses desafios se manifestam na prática da cirurgia digestiva.
Introdução
A relação de mentoria na cirurgia é complexa e multifacetada, influenciada por diversas variáveis como a geração, gênero, raça, cultura, especialização, e o equilíbrio entre vida profissional e pessoal. Estes fatores podem afetar significativamente a eficácia da mentoria e, em última análise, o sucesso profissional do mentee. No Brasil, onde a diversidade cultural e a crescente inclusão de mulheres na medicina são realidades cada vez mais presentes, entender esses desafios é essencial para uma formação cirúrgica de excelência.
Desenvolvimento
Impacto das Gerações na Mentoria Cirúrgica
Cada geração traz consigo valores e expectativas diferentes, que podem influenciar a dinâmica da mentoria. Cirurgiões da geração Baby Boomer (nascidos entre 1944 e 1959) tendem a valorizar uma hierarquia rígida, com um foco forte no trabalho e no sucesso profissional. Em contraste, cirurgiões da Geração X (nascidos entre 1960 e 1980) valorizam a independência e o equilíbrio entre vida pessoal e profissional, enquanto os Millennials (nascidos entre 1981 e 2000) buscam mentores que sejam acessíveis e que os tratem como iguais, com um foco no feedback contínuo e na flexibilidade.
Gênero e Mentoria na Cirurgia Digestiva
A composição de gênero na medicina está mudando rapidamente. Em 2010, aproximadamente 50% dos estudantes de medicina no Brasil eram mulheres. Apesar disso, a ascensão das mulheres na cirurgia acadêmica ainda enfrenta barreiras significativas, como a falta de modelos femininos de sucesso e as dificuldades em equilibrar a carreira com a vida pessoal. Dados brasileiros mostram que, em 2022, apenas 15% das cirurgiãs ocupavam posições de destaque em hospitais universitários, indicando que o “teto de vidro” ainda é uma realidade a ser superada.
Diversidade Cultural e Raça na Mentoria
No Brasil, a diversidade cultural é uma característica marcante, refletida também na formação cirúrgica. No entanto, as minorias raciais ainda estão sub-representadas entre os cirurgiões acadêmicos. Estudos mostram que apenas 7% dos cirurgiões formados em programas de residência entre 2010 e 2020 pertenciam a minorias étnicas. Esta realidade destaca a importância de um mentor que compreenda e respeite as diferenças culturais e raciais, promovendo um ambiente inclusivo e de apoio.
Especialização e seus Desafios
A especialização em cirurgia digestiva trouxe consigo novos desafios na relação de mentoria. Enquanto no passado o cirurgião geral era responsável por uma ampla gama de procedimentos, hoje a tendência é a superespecialização. Isso pode gerar conflitos quando o mentor, possivelmente de uma geração anterior, possui uma visão mais generalista, enquanto o mentee busca uma formação mais especializada.
Equilíbrio entre Vida Profissional e Pessoal
A busca por um equilíbrio entre vida profissional e pessoal é um tema recorrente entre os cirurgiões mais jovens. A geração Millennial, em particular, valoriza o tempo de qualidade fora do trabalho tanto quanto o sucesso profissional. Essa mudança de paradigma pode ser um desafio na relação mentor-mentee, especialmente quando o mentor provém de uma geração que priorizava o trabalho em detrimento da vida pessoal.
Aplicação na Cirurgia Digestiva
Para o mentee em cirurgia digestiva, escolher um mentor ideal envolve mais do que buscar alguém com conhecimento técnico. É crucial considerar como os valores e as expectativas do mentor podem influenciar o desenvolvimento de sua carreira. A escolha deve ser estratégica, buscando não apenas orientação técnica, mas também apoio em aspectos como desenvolvimento profissional, equilíbrio entre vida pessoal e profissional, e compreensão das particularidades culturais e sociais do Brasil.
Pontos-Chave
- Entender as diferenças geracionais é fundamental para alinhar expectativas entre mentor e mentee.
- A igualdade de gênero na cirurgia ainda enfrenta desafios, sendo crucial que os mentores estejam conscientes dessas barreiras.
- A diversidade cultural e racial deve ser respeitada e promovida na mentoria, especialmente em um país como o Brasil.
- A superespecialização em cirurgia digestiva pode gerar conflitos, que devem ser abordados com clareza e abertura.
- O equilíbrio entre vida profissional e pessoal é cada vez mais valorizado, sendo importante que o mentor apoie essa busca.
Conclusões Aplicadas à Prática do Cirurgião Digestivo
A mentoria na cirurgia digestiva é um desafio que exige uma abordagem holística. O mentor ideal deve ser capaz de oferecer orientação técnica de alto nível, ao mesmo tempo em que respeita e apoia as necessidades individuais do mentee. No contexto brasileiro, onde a diversidade e a inclusão são realidades cada vez mais presentes, essa sensibilidade torna-se ainda mais crucial.
“Ensinar é aprender duas vezes.” – Joseph Joubert.
Gostou? Nos deixe um comentário ✍️, compartilhe em suas redes sociais e/ou mande sua dúvida pelo 💬 Chat On-line em nossa DM do Instagram.
Hashtags: #MentoriaCirurgica #CirurgiaDigestiva #EducaçãoMedica #CarreiraCirurgica #EquilibrioProfissional
Existe o mentor ideal?
O Mentor Ideal em Cirurgia Digestiva: Um Guia para Aspirantes a Cirurgiões
Na complexa jornada para se tornar um cirurgião habilidoso, a mentoria desempenha um papel fundamental. Para estudantes de medicina, residentes de cirurgia e pós-graduandos especializados em cirurgia digestiva, a escolha de um mentor pode impactar significativamente seu desenvolvimento profissional. Compreender as características de um mentor ideal é essencial nesse contexto.
Introdução
A mentoria na cirurgia, especialmente em áreas especializadas como a cirurgia digestiva, não se trata apenas de guiar um mentorado durante sua formação médica. É uma relação que molda o futuro tanto do mentorado quanto do mentor, promovendo um legado de excelência e inovação. Mas o que exatamente faz de um mentor alguém ideal neste campo exigente e em rápida evolução?
Desenvolvimento: Características Principais do Mentor Ideal
- Reconhecimento Profissional: O mentor deve ser um especialista reconhecido, respeitado tanto dentro quanto fora de sua instituição. Esse reconhecimento não apenas inspira o mentorado, mas também abre portas para redes e oportunidades valiosas. No Brasil, onde a demanda por cirurgiões digestivos qualificados é alta, a reputação profissional de um mentor pode proporcionar uma vantagem significativa na trajetória de carreira de um mentorado.
- Generosidade com Tempo, Conhecimento e Reconhecimento: O mentor ideal é generoso com seu tempo, compartilhando habilidades clínicas e técnicas enquanto oferece orientação em pesquisa e desenvolvimento profissional. Em um país onde o equilíbrio entre trabalho e vida pessoal é cada vez mais valorizado, especialmente entre as gerações mais jovens, um mentor que consiga gerenciar seu tempo de forma eficaz, dedicando-se ao sucesso do mentorado, é inestimável.
- Integridade e Liderança Ética: Um mentor deve ser honesto e ético, guiando o mentorado pelas complexidades da pesquisa clínica, do cuidado ao paciente e dos desafios profissionais. Isso inclui ajudar o mentorado a enfrentar os inevitáveis reveses, como propostas de pesquisa rejeitadas ou resultados clínicos inesperados, com resiliência e compromisso com a verdade e a prática ética.
- Disponibilidade e Acessibilidade: Interações regulares e significativas são essenciais. O mentor deve estar acessível tanto para reuniões agendadas quanto para discussões informais. Essa disponibilidade é particularmente crítica no ambiente de alta pressão do treinamento cirúrgico, onde conselhos rápidos e bem-pensados podem fazer uma diferença significativa.
- Consciência Social e Empatia: O ambiente cirúrgico moderno exige mentores que compreendam a importância de equilibrar uma carreira de sucesso com a vida pessoal. Isso é especialmente relevante no Brasil, onde as dinâmicas culturais e sociais podem influenciar as decisões de carreira e o equilíbrio entre vida profissional e pessoal.

Pontos-chave para Mentores na Cirurgia Digestiva
Equilíbrio entre Crescimento Profissional e Pessoal: Selecione mentores que compreendam e apoiem seus objetivos pessoais e seu equilíbrio entre vida profissional e pessoal.
Procure Mentores com Histórico de Sucesso: Busque mentores que tenham um histórico de mentorados bem-sucedidos e uma forte reputação profissional.
Valorize a Liderança Ética: A integridade de um mentor é tão importante quanto sua expertise. Escolha mentores que priorizem práticas éticas e o cuidado centrado no paciente.
Garanta Comunicação Regular: Estabeleça uma rotina de reuniões regulares e seja proativo ao buscar orientação.
Aplicação na Cirurgia Digestiva
No campo da cirurgia digestiva, a relação mentor-mentorado tem implicações únicas. A complexidade dessa especialidade exige mentores que não apenas possuam expertise técnica, mas também compreendam o cenário em constante evolução das técnicas cirúrgicas e do cuidado ao paciente. No Brasil, onde as doenças digestivas representam um grande problema de saúde pública, os mentores desempenham um papel crucial na formação de cirurgiões que possam enfrentar esses desafios com abordagens inovadoras e culturalmente sensíveis.
Mentoria como Catalisador de Excelência em Cirurgia Digestiva
A jornada para se tornar um cirurgião digestivo habilidoso é desafiadora e complexa. O mentor ideal é aquele que não apenas guia você pelos aspectos técnicos da cirurgia, mas também ajuda a enfrentar os desafios profissionais e pessoais que acompanham essa carreira. Como disse o Dr. William Osler: “A prática da medicina é uma arte, não um comércio; uma vocação, não um negócio; uma vocação na qual seu coração será exercido tanto quanto sua cabeça.” Essa sabedoria aplica-se igualmente à relação mentor-mentorado, onde o coração e a mente devem trabalhar juntos para cultivar a próxima geração de líderes cirúrgicos.
Gostou? Nos deixe um comentário ✍️, compartilhe em suas redes sociais e|ou mande sua dúvida pelo 💬 Chat On-line em nossa DM do Instagram.










