In the epoch of minimally invasive management of biliary and pancreatic disorders, endoscopic retrograde cholangiopancreatography (ERCP) combined with endoscopic sphincterotomy (ES) has become a prevalent procedure all over the world. Even though ES is a safe procedure, it carries a small but significant number of serious complications which include pancreatitis, bleeding, cholangitis and perforation. As per old literature, ERCP-related perforations were reported in 0.5–2.1% of sphincterotomies with a mortality rate of 16–18%. However, the improvement in the experience and skill of the endoscopy specialists combined with advancements in technology have reduced the incidence of perforation to <0.5% over the years. Sphincterotomy (56%) and guidewire manipulation (23%) are widespread causes of perforations related to endoscopic retrograde cholangiopancreatography (ERCP). There is a dearth of evidence-based strategies with respect to the proper management of ERCP perforations. While one set of investigators promote on-demand conservative and surgical management, based on a clinical course, the others support operative repair in all cases on account of the complications associated with the delayed operative intervention.
INDICATIONS OF SURGICAL MANAGEMENT
1. Large extravasation of contrast at the time of ERCP defined as incomplete dissipation of contrast after 1 min on follow-up plain film.
2. If there is only a small amount of contrast extravasation, where there is complete dissipation after 1 min of ERCP, on follow-up plain film, then a UGI with contrast injection on fluoroscopy is performed in 2–8 h. If this shows extravasation, we recommend surgical exploration.
3. Follow-up CT scan showing a collection due to perforation in the retroperitoneum or intraperitoneum.
4. Retained hardware unable to be removed by endoscopy along with perforation.
5. Massive subcutaneous emphysema.
6. Failure of conservative management.
A delay in diagnosis or in surgery will lead to death. The reason is that there is a massive autodigestion of body tissues which is due to a constant release of enzymes, and this eventually leads to sepsis. The principle of treatment by surgery is the same as endoscopic treatment. Any case that is suspected to have ERCP-induced perforation is kept nil by mouth, and the gastric contents are decompressed by Ryles tube and intravenous antibiotics.
This is done by diverting bile, enteric and pancreatic juices away from the site of perforation. However simple drainage will also cause the juices to flow through the perforation site and body cavities before draining out of the tubes. This could be avoided by diverting the juices through well-controlled different paths which could be done by the following procedures:
1. T-tube in CBD;
2. Placement of duodenostomy tube—lateral/end duodenostomy;
3. Duodenal diverticulization;
4. Pyloric exclusion;
5. Roux-en-Y duodenojejunostomy.
The disadvantage of using Roux-en-Y duodenojejunostomy is that if the edges are inflamed, then the sutures will not hold properly. However other procedures can be used even when the edges are inflamed. Even though duodenostomy appears to be simple, a part of gastric and duodenal contents pass across the perforation site.
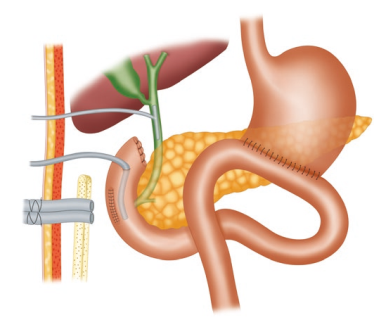
Duodenal diverticulization involves three things: (1) tube to divert duodenal and pancreatic juice, (2) T-tube in CBD to divert bile and (3) distal
gastrectomy and Billroth II anastomosis to provide an alternate pathway for food and gastric juice, thereby preventing these from passing through the site of perforation. Although this procedure has been proved to be successful, it is less widely used due to its complex nature. Pyloric exclusion is a simpler form in which the pylorus is closed by purse string by long-standing absorbing sutures like PDS 2.0 instead of distal gastrectomy. Similar to duodenal diverticulization, T-tube drainage of the CBD and loop gastrojejunostomy are done. The duodenal perforation is closed over a duodenostomy tube.
Whenever there is collection which is localized to the retroperitoneum, retroperitoneal surgical approach can be carried out. Advantages of this procedure are (1) it permits gravitational drainage, (2) avoids septic complication of the peritoneal cavity, (3) directs retroperitoneal necrosectomy with post-operative washes and (4) avoids complex intra-abdominal surgeries. However the disadvantage of this procedure is that it can be used only for retroperitoneal-contained perforations.











[…] system in patients with resectable periampullary malignancies, given widespread availability of endoscopic retrograde cholangiopancreatography and its perceived safety profile. On the other hand, the purported benefits of routine preoperative […]