Postpancreatectomy Hemorrhage
Postoperative complications represent one of the most debated topics in pancreatic surgery. Indeed, the rate of complications following pancreatectomy is among the highest in abdominal surgery, with morbidity ranging between 30 and 60%. They are often characterized by elevated clinical burden, with a consequent challenging postoperative management. Mortality rates can exceed 5%. The impact on patient recovery and hospital stay eventually leads to massive utilization of resources and increases costs for the health system. The International Study Group of Pancreatic Surgery (ISGPS) provides standardized definitions and clinically based classifications for the most common complications after pancreatectomy, including postoperative pancreatic fistula (POPF), post pancreatectomy hemorrhage (PPH), delayed gastric emptying (DGE), bile leakage, and chyle leak.
Post Pancreatectomy Hemorrhage
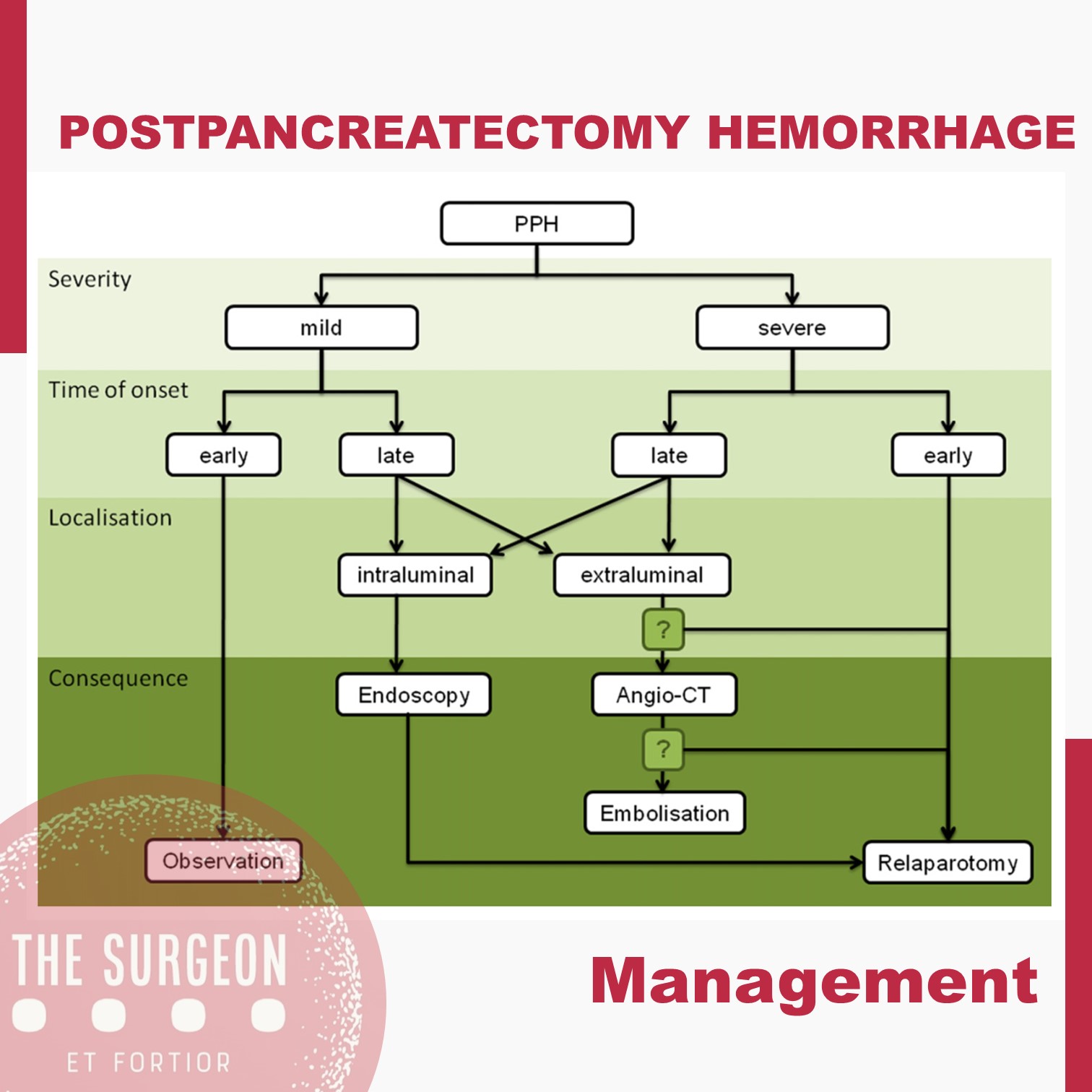
Despite its lower incidence compared with POPF with reported rates of 3–10% after pancreatectomy, PPH remains one of the major of postoperative complications, with mortality rates ranging from 30 to 50%. According to current ISGPS recommendations, PPH is classified in three grades (A, B, and C) based on two main criteria: timing of the hemorrhage and severity of the bleeding. The timing is dichotomized as early, occurring within 24 hours from the index surgery, and late, when it happens afterwards.

Management is tailored according to the clinical picture, the timing of onset, and the presumptive location. Early hemorrhage is generally due to either unsuccessful intraoperative hemostasis or to an underlying coagulopathy. The vast majority of patients are basically asymptomatic, with PPH having no influence on the postoperative course. However, when the bleeding is severe, re-laparotomy is recommended, with the aim of finding and controlling the source of bleeding. This approach usually guarantees an uneventful subsequent course. Late PPH is often challenging and the pathogenesis is diverse. Vascular erosion secondary to POPF or intraabdominal abscess, late failure of intraoperative hemostatic devices, arterial pseudoaneurysm, and intraluminal ulceration are some of the most common causes. In this setting, surgical access to the source of bleeding may be challenging. Angiography (if extraluminal) and endoscopy (if intraluminal) represent the primary approaches to treatment. Surgery is reserved for hemodynamically unstable patients and for those who present with deteriorating condition, multiorgan failure or sepsis. Given these assumptions, except for early mild events, contrast-enhanced abdominal CT is crucial in all cases of PPH, possibly allowing identification of the source and planning the management accordingly. Also, it should be noted that late massive hemorrhages may be preceded by mild self-limiting sentinel bleeds. A prompt abdominal CT scan aimed at excluding vascular lesions is therefore strongly recommended in these cases.
The incidence of complications following pancreatic resection remains high. The ISGPS established standardized definitions and clinical grading systems for POPF, PPH, DGE, and biliary and chyle leak. These classification systems have enabled unbiased comparisons of intraoperative techniques and management decisions. However, the management policies of these complications are most often driven by a patient’s condition and local surgical expertise and is not always based on the available high-level evidence. The development of high-volume specialized units with appropriate resources and multidisciplinary experience in complication management might further improve the evidence and the outcomes.
POPF after Distal Pancreatectomy
Minimally Invasive Versus Open Techniques
Despite advances in laparoscopic and robotic approaches, the vast majority of distal pancreatectomies continue to be performed via an open approach. Recent retrospective data have demonstrated that minimally invasive distal pancreatectomy is associated with decreased blood loss and shorter hospital stays than open pancreatectomy. A large recent study utilizing the Nationwide Inpatient Sample database suggested, first, that the minimally invasive approach is becoming more widely utilized, increasing from 2.4 to 7.3 % over a study period from 1998 to 2009. Second, that study reported that the minimally invasive approach was associated with decreased length of stay as well as decreased incidence of infectious complications, bleeding complications, and blood transfusions. This population-based study echoes conclusions drawn by a large multi-institutional study performed several years previously. Drawing on a combined patient sample of 667 patients, with 24 % initially attempted laparoscopically, the authors were able to demonstrate lower overall complication rate, decreased blood loss, and shorter hospital stays among patients undergoing laparoscopic approach via a multivariate analysis.
Notably, there was no significant difference in the pancreatic leak rate between the open and laparoscopic approaches, although there was a nonsignificant trend favoring the laparoscopic approach. More recently, the robotic approach has generated significant interest as a technique for performing distal pancreatectomy. Retrospective analysis has suggested that the robotic approach is well suited for pancreatectomy. Fistula rates, however, remain a concern. A retrospective review of patients undergoing robotic pancreatic operations included 83 patients who underwent distal pancreatectomy. About 27 % were identified as having a ISPGF type A pancreatic leak; 12 and 4.8 % were identified as having a grade B or C leak, respectively.
Identifying Risk Factors
For pancreaticoduodenectomy (PTD) , a fistula risk score has been recently developed that has been shown to be highly predictive of POPF. This score assigns points based on gland texture, gland pathology, duct diameter, and intraoperative blood loss. In general, high blood loss, soft gland texture, and smaller duct diameter confer increased risk of POPF, whereas pancreatic adenocarcinoma and pancreatitis as the indication for PTD confer protection for the development of pancreatic fistula versus other diagnoses. Also of note, higher fistula risk scores correlated with greater incidence of clinically relevant (ISGPF grade B or C) fistula. The adaptation of this risk score to patients undergoing distal pancreatectomy is yet to be validated; however, at least one published study indicates that this scoring system may have limitations in the setting of distal pancreatectomy. In that study, risk factors for pancreatic fistula after stapled gland transection in patients undergoing distal pancreatectomy were examined, and in a multivariate analysis, only the presence of diabetes and the use of a 4.1-mm staple cartridge were associated with increased risk of pancreatic fistula formation.
Laparoscopic distal PANCREATECTOMY
Laparoscopic distal pancreatectomy has become a relatively standard operation and has been approached by a similar technique by multiple groups since its original description. Generally, four or five trocars are used to gain entrance to the abdominal cavity, but three-trocar LPD has been described. A “clockwise” technique results in an efficient, reliable, and uniform approach for removing the vast majority of lesions that are located to the left of the neck of the pancreas (Asbun & Stauffer, 2011). The technique begins with the positioning of the patient in a modified right lateral decubitus position. The degree of lateral positioning depends on the patient’s body habitus and the location of the lesion, as well as the tilting capabilities of the operative bed. The use of gravity assisted retraction with the patient in a reverse Trendelenburg position with the left flank elevated is a key component to successful exposure of the tail of the pancreas and the spleen. Four mid- to left-sided abdominal trocars are placed in a semicircle around the body and tail of the pancreas, including two 12 mm and two 5 mm trocars, and a five step clockwise method is used.
Step 1: Mobilization of the splenic flexure of the colon
and exposure of the pancreas
The first step is mobilization of the splenic flexure of the colon. The lateral attachments, splenocolic ligament, and gastrocolic ligament are succes-sively transected to allow access to the lesser sac. If the spleen is to be removed, the dissection proceeds cranially, and the short gastric vessels are transected up to the superior pole of the spleen. Sufficient mobilization of the colon allows for gravity-assisted retraction of the colon, and the stomach is completely freed from the anterior aspect of the body and tail of the pancreas. Infrequently, an additional trocar or tacking stitch is required to elevate the stomach to the anterior abdominal wall off the pancreas and out of the operative field.
Step 2: Dissection along the inferior edge of the pancreas
and choosing the site for pancreatic division
The second step is to identify the inferior border of the pancreas and create a window in the fibroadipose tissue plane between the retroperitoneum and the pancreas. This dissection is carried medially toward the lesion of interest. Intraoperative ultrasound is performed to clearly identify the lesion and the planned site of division of the pancreas.
Step 3: Pancreatic parenchymal division and ligation
of the splenic vein and artery
The third step is pancreatic parenchymal division and ligation of the splenic artery and vein. After dissecting around the pancreas in 360 degrees, a Penrose drain or suture is placed around the proposed site of division of the pancreas and is used to elevate the pancreas from the retroperitoneum. A band passer instrument is helpful for this part of the procedure. For distal pancreatectomy, the splenic vessels will often be dissected, ligated, and divided en bloc with the parenchyma. For subtotal resections with division of the pancreas at the neck, the underlying superior mesenteric vein and splenic vein are dissected away from the posterior aspect of the pancreas, and the celiac trunk is identified individually and dissected free from the neck and proximal body of the pancreas. Parenchymal transection is performed with a linear stapling device by using a slow, gradual, and stepwise compression technique. Thick tissue staples (open staple height of approximately 4 mm) with staple line reinforcement is preferred for almost any pancreas consistency, and the stapler is gradually closed in a stepwise manner over the course of several minutes to allow for parenchymal compression. Parenchymal transection and splenic vessel division are done individually for subtotal pancreatectomy for lesions located between the gastroduodenal artery and the celiac trunk.
Step 4: Dissection along the superior edge of the pancreas
The fourth step is to sweep the pancreas inferiorly and anteriorly off the retroperitoneum toward the splenic hilum. A deeper dissection plane that includes Gerota fascia and the left adrenal gland may be chosen for malig-nancies that appear to have posterior invasion from the pancreas.
Step 5: Mobilization of the spleen and specimen removal
The fifth step is the mobilization of the spleen from its diaphragmatic and retroperitoneal attachments and placement of the specimen within a bag for exteriorization. Major complications were seen in less than 10% of patients, and both the conversion rate and the clinically significant pancreatic fistula (grade B/C) rate by using the gradual stepwise compression stapled technique was seen in fewer than 5%. Operative drains were rarely placed.
Outcomes
The minimally invasive approach to resection of the left-sided pancreas by distal or subtotal pancreatectomy has gained acceptance and been used with an increasing frequency worldwide during the past decade. Multiple systematic reviews have demonstrated the safety of LDP and its superiority versus open distal pancreatectomy (ODP) for selected outcomes, such as blood loss, transfusion rates, and hospital stays; it must be remembered, however, that all these studies are retrospective in nature and therefore severely limited by significant selection bias. All studies showed similar reoperation rates and mortality, but most found a lower overall morbidity for the laparoscopic approach. Some studies identified lower rates of specific complications, such as wound infection and even pancreatic fistula. Although oncologic clearance was similar, most studies have shown that ODP is often the surgery of choice for larger tumors.










