O Fio da Navalha na Prevenção da Isquemia e Estenose
Autor: Prof. Dr. Ozimo Gama (Tempo de Leitura: 11 minutos)
Introdução
No campo minado que é a cirurgia hepatobiliar, existe um princípio fisiológico que não admite margem para erro: enquanto o parênquima hepático é um órgão privilegiado, nutrido por um duplo suprimento sanguíneo (arterial e venoso portal), a árvore biliar é alimentada exclusivamente pelo sistema arterial. Para o estudante de medicina e o residente de cirurgia, a compreensão desta premissa muda drasticamente a forma como o bisturi e o cautério são manuseados em torno do hilo hepático. A esqueletização excessiva de um ducto biliar não é um sinal de dissecção meticulosa, mas sim a antessala anatómica de uma complicação catastrófica: a isquemia, seguida de necrose e estenose biliar. Neste artigo, dissecaremos a anatomia vascular da árvore biliar, as armadilhas do ducto cístico e os fundamentos anatómicos da cirurgia oncológica da vesícula.
1. A Vesícula Biliar: Topografia e Peculiaridades Histológicas
A vesícula biliar repousa no equador que divide o fígado direito do esquerdo — uma linha imaginária conhecida como Linha de Cantlie (ou linha de Rex-Cantlie), que cursa entre os segmentos IVb e V em direção à veia cava inferior posteriormente.
A vesícula é maioritariamente peritonizada, exceto na sua face posterior, que assenta diretamente na placa cística. No entanto, o seu verdadeiro “Calcanhar de Aquiles” reside na sua histologia: a vesícula biliar não possui muscularis mucosae, não possui submucosa e apresenta uma camada muscular descontínua.
- Implicação Cirúrgica Oncológica: Estas especificidades anatómicas removem as barreiras naturais contra a progressão tumoral, facilitando a invasão direta do cancro da vesícula biliar para o parênquima hepático. É por este motivo que o tratamento cirúrgico curativo exige uma Colecistectomia Radical (que inclui a ressecção em cunha dos segmentos hepáticos IVb e V) sempre que o estadiamento tumoral (T) for superior ou igual a T1b.

2. O Labirinto Anatómico do Ducto Cístico e da Via Biliar Principal
A partir do infundíbulo cónico da vesícula, o ducto cístico estende-se como o limite inferior do triângulo hepatocístico em direção ao hilo, unindo-se ao ducto hepático comum (DHC) para formar o ducto colédoco (VBP). Contudo, na via biliar, a variação anatómica é a regra, não a exceção. O ducto cístico pode correr paralelamente ao DHC, espiralar posteriormente a este e inserir-se na sua face medial. Mais perigoso ainda é quando o cístico se insere no Ducto Setorial Posterior Direito (RPD), uma variação que ocorre em cerca de 4% dos fígados. Esta configuração é notoriamente perigosa, expondo o RPD a um risco altíssimo de secção inadvertida durante uma colecistectomia de rotina. Distalmente, o colédoco entra na cabeça do pâncreas e une-se ao ducto pancreático (Wirsung) para formar a ampola hepatopancreática, controlada pelo Esfíncter de Oddi.
- O Canal Comum Longo: Quando a junção entre o colédoco e o ducto pancreático ocorre de forma anómala (antes do complexo esfincteriano), ocorre o refluxo de enzimas pancreáticas ativadas para a árvore biliar. Este trauma químico crónico é o principal fator de risco para a formação de cistoss do colédoco e para o desenvolvimento de Colangiocarcinoma.
3. O “Tendão de Aquiles”: A Vascularização Arterial da Via Biliar
Como mencionado, a árvore biliar depende de um fluxo arterial ininterrupto. O suprimento segue um padrão de perfusão que ascende e descende ao longo dos ductos:
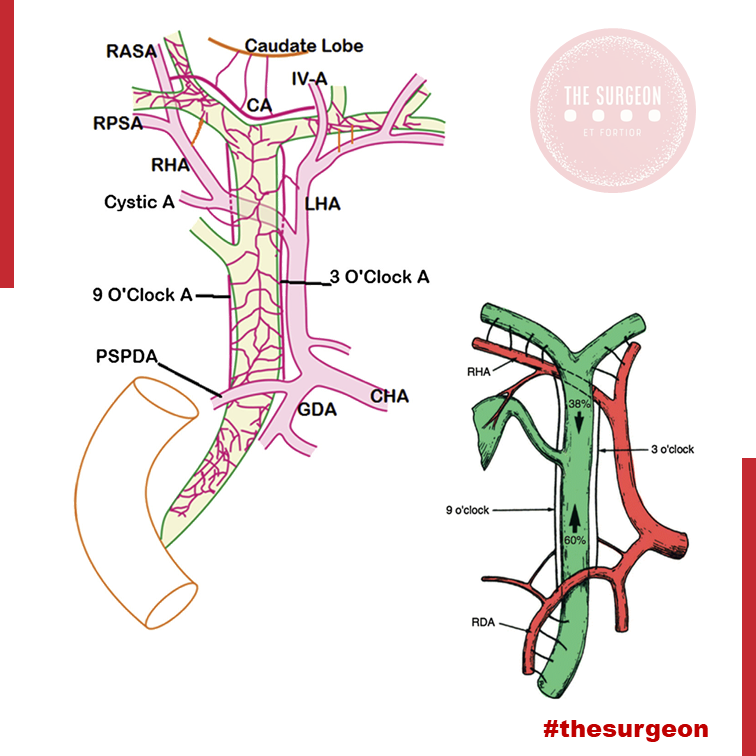
- O Suprimento Distal (Ascendente): O ducto colédoco recebe a sua irrigação inferior a partir de arteríolas emparelhadas provenientes da Artéria Gastroduodenal (GDA) e da Artéria Pancreatoduodenal Superior Posterior (PSPDA). Esta última representa o suprimento arterial mais importante e constante para o colédoco distal.
- O Suprimento Proximal (Descendente): Proximamente, o colédoco é alimentado por arteríolas originadas da artéria hepática direita (AHD).
- As Artérias Marginais: Estes vasos superiores e inferiores anastomosam-se para formar as artérias marginais, que correm paralelamente ao longo do ducto colédoco, situando-se tipicamente nas posições das 3 e 9 horas (lateral e medialmente). Desnudar (esqueletizar) o colédoco deste suprimento arterial para criar uma anastomose ou durante uma linfadenectomia não regrada acarreta um risco altíssimo de isquemia e estenose cicatricial a longo prazo.
4. O Plexo Epicoledociano Hilar e as Variações Arteriais
No interior do hilo hepático, uma rica rede de capilares liga as artérias hepáticas direita e esquerda. Este leito vascular, denominado Plexo Epicoledociano Hilar, fornece uma circulação colateral crítica que pode manter o suprimento arterial para um lado do fígado caso o vaso ipsilateral seja lesado. A preservação deste plexo e do suprimento sanguíneo arterial para o fígado remanescente é absolutamente crucial na criação de uma anastomose biliodigestiva (hepaticojejunostomia). A isquemia hilar resulta na temível colangiopatia isquémica e no desenvolvimento de abcessos hepáticos intratáveis.
O Papel das Variações Arteriais no Colangiocarcinoma Hilar
Na cirurgia do colangiocarcinoma hilar (Tumor de Klatskin), a complexidade aumenta devido às variações arteriais. A artéria hepática direita cruza posteriormente ao ducto hepático na maioria dos casos, mas em 25% cruza anteriormente. Mais relevante ainda é a presença de uma Artéria Hepática Direita Substituída (ou Acessória), com origem na Artéria Mesentérica Superior (AMS). Ao contrário da anatomia clássica, este vaso cursa lateralmente ao ducto colédoco (e não medialmente), estando extremamente vulnerável à iatrogenia se o cirurgião não o identificar durante a dissecção do ligamento hepatoduodenal. Combinações destas variações com a localização exata do tumor ditarão se uma lesão hilar é ressecável ou irresecável.
Pontos-Chave para a Prática Diária
- A Regra das 3 e 9 Horas: Lembre-se sempre de que o suprimento axial do colédoco viaja nos seus flancos laterais. Evite dissecções circunferenciais extensas da via biliar principal.
- Histologia e Neoplasias: A ausência de submucosa na vesícula biliar dita a necessidade de cirurgia hepática radical (ressecção em cunha do leito) em tumores T1b ou superiores.
- Inserções Anómalas do Cístico: A inserção num ducto setorial direito (RPD) é uma armadilha clássica. A Visão Crítica de Segurança (CVS) e a colangiografia são as únicas formas de evitar a transecção de um ducto principal aberrante.
- O Perigo do Canal Comum: A junção biliopancreática anómala exige vigilância ou tratamento cirúrgico devido ao elevado risco de colangiocarcinoma derivado da inflamação enzimática crónica.
Conclusões Aplicadas à Prática do Cirurgião Digestivo
O respeito pela árvore biliar transcende a mera identificação do tubo que transporta a bílis; exige uma veneração profunda pela sua microvascularização. O cirurgião que descasca a via biliar como se tratasse de um cabo elétrico condena o seu doente a um futuro de estenoses isquémicas, colangites de repetição e reintervenções de extrema complexidade. O domínio da variabilidade anatómica vascular (como as artérias substituídas da AMS) e o conhecimento tático do plexo epicoledociano não são meros detalhes de rodapé dos livros de anatomia; são a linha que separa o triunfo cirúrgico oncológico da catástrofe iatrogénica irreparável.
“A anatomia biliar não segue regras absolutas, apenas tendências. Operar no hilo hepático assumindo a normalidade é o primeiro passo para o desastre. O cirurgião deve dissecar com a expectativa constante da variação.” — Aforismo clássico da cirurgia hepatobiliar.
Gostou ❔Deixe-nos um comentário ✍️, partilhe nas suas redes sociais e|ou envie a sua dúvida pelo 💬 Chat On-line na nossa DM do Instagram.











[…] The gold standard for the surgical treatment of symptomatic cholelithiasis is conventional laparosco… The “difficult gallbladder” is a scenario in which a cholecystectomy turns into an increased surgical risk compared with standard cholecystectomy. The procedure may be difficult due to processes that either obscure normal biliary anatomy (such as acute or chronic inflammation) or operative exposure (obesity or adhesions caused by prior upper abdominal surgery). So, when confronted with a difficult cholecystectomy, the surgeon has a must: to turn the operation into a safe cholecystectomy, which can mean conversion (to an open procedure), cholecystostomy, or partial/ subtotal cholecystectomy. The surgeon should understand that needs to rely on damage control, to prevent more serious complications if choosing to advance and progress to a complete cholecystectomy. […]