Abordagem Tática e Decisão Cirúrgica no Dolicossigmóide
Do Manejo Conservador à Colectomia Subtotal
Autor: Prof. Dr. Ozimo Gama
Categoria: Cirurgia Colorretal / Emergências Cirúrgicas / Anatomia Aplicada
Tempo de Leitura: 14 minutos
Introdução
O dolicocolon e, de forma mais específica, o dolicossigmóide consistem na redundância e alongamento anômalos dos segmentos cólicos. Embora frequentemente interpretados na prática clínica como achados incidentais de exames colonoscópicos ou variantes anatômicas benignas, essas alterações estruturais podem atuar como substrato anatômico para afecções de gravidade expressiva, incluindo a constipação crônica intratável, a distensão abdominal refratária e o vólvulo intestinal. Na rotina da cirurgia do aparelho digestivo, a decisão de intervir requer uma avaliação criteriosa do nexo causal entre a redundância anatômica e o comprometimento funcional do órgão. No Brasil, esse cenário ganha complexidade adicional devido à prevalência histórica do megacólon e dolicocolon de etiologia chagásica em diversas regiões, exigindo diferenciação precisa das formas idiopáticas. Esta revisão analisa as evidências contemporâneas que orientam a estratificação do tratamento do dolicossigmóide, estabelecendo as fronteiras entre a abordagem conservadora e a indicação de ressecções cirúrgicas com base no grau de descompensação morfofuncional da parede colônica.
Fisiopatologia da Descompensação e Estratégias Táticas
A transição de um dolicossigmóide funcionalmente compensado para uma entidade patológica grave e incapacitante é ditada por alterações histopatológicas progressivas na parede intestinal. Estudos morfométricos avançados demonstram que o estágio descompensado do dolicocolon é caracterizado por atrofia da musculatura lisa, esclerose tecidual e uma perda neuronal mioentérica irreversível. Essa degeneração estrutural dos plexos nervosos resulta em atonia colônica e estase fecal persistente, tornando o órgão refratário aos estímulos peristálticos habituais e estabelecendo uma indicação cirúrgica clara.
1. Limites e Indicações do Manejo Conservador
Em pacientes cujos sintomas de constipação são leves a moderados ou estão primariamente associados a distúrbios funcionais isolados, como a disfunção do assoalho pélvico (DAP), a abordagem conservadora deve ser rigorosamente mantida como primeira linha de tratamento. Medidas dietéticas otimizadas e terapia laxativa programada são fundamentais. A realização de ressecções cirúrgicas em indivíduos com DAP concomitante sem atonia colônica estrutural demonstra baixas taxas de sucesso, uma vez que a colectomia não corrige o distúrbio evacuatório de base. Ferramentas de inteligência diagnóstica, como a volumetria colônica por tomografia computadorizada e o estudo do trânsito colônico por marcadores radioopacos ou cintilografia, são essenciais para mapear o tempo de trânsito e quantificar o volume do órgão, diferenciando a redundância simples da verdadeira inércia colônica.
2. O Dilema Cirúrgico: Colectomia Subtotal vs. Sigmoidectomia Isolada
Quando a constipação se torna grave, refratária às medidas clínicas e associada à atonia e dilatação colônica massiva, o tratamento cirúrgico impõe-se como a única conduta resolutiva. A determinação da extensão da ressecção é o ponto crítico do planejamento operacional:
- Colectomia Subtotal: Consolida-se na literatura como a estratégia com os melhores resultados funcionais sustentados a longo prazo. Em estudos comparativos com seguimento de um ano, pacientes com dolicocolon submetidos à colectomia subtotal laparoscópica apresentaram melhora funcional duradoura e taxas de recorrência de colostase praticamente nulas, mesmo em casos de dilatação extrema.
- Sigmoidectomia Isolada ou Hemicolectomia Esquerda: Representa uma armadilha tática comum na urgência ou no planejamento eletivo. Evidências demonstram que a ressecção isolada do segmento redundante apresenta taxas elevadas de falha terapêutica: apenas 55% dos pacientes atingem um desfecho satisfatório, enquanto 45% mantêm colostase pós-operatória severa em decorrência da persistência de atonia nos segmentos colônicos remanescentes.
3. Síndrome da Defecação Obstruída (SDO) e Correções Pélvicas
Nos cenários onde a redundância do dolicocolon atua como fator obstrutivo mecânico intra-abdominal associado a prolapso retal ou intussuscepção, a associação tática de rectopexia ventral com tela laparoscópica (VMR) à sigmoidectomia segmentar demonstra eficácia na redução dos sintomas obstrutivos e melhora dos escores de constipação em curto prazo (6 meses). Contudo, o cirurgião deve estar ciente de que a presença do dolicocolon subjacente constitui um fator de risco independente para a falha funcional tardia da rectopexia, exigindo programas intensivos de reabilitação e fisioterapia pélvica pós-operatória para mitigar a constipação persistente ou de novo.
Aplicação na Cirurgia Digestiva: O Manejo da Urgência no Vólvulo
O dolicossigmóide representa a principal alteração anatômica predisponente para o desenvolvimento de vólvulo de sigmóide, uma emergência cirúrgica de alta fricção que pode acometer desde neonatos e pacientes pediátricos até adultos e idosos. O alongamento do mesocólon com uma base de fixação estreita propicia a torção axial da alça sobre o seu próprio eixo, resultando em obstrução em alça fechada e isquemia intestinal rápida.
O algoritmo de abordagem na urgência pressupõe uma sequência tática rígida:
- Desvolvulação Endoscópica: Em pacientes hemodinamicamente estáveis e sem sinais clínicos ou radiológicos de peritonite, perfuração ou gangrena manifesta, a realização de retossigmoidoscopia ou colonoscopia para derotação mecânica e descompressão gasosa (potencializada por técnicas percutâneas, se necessário) é a conduta inicial de escolha, atuando como ponte para a estabilização e programação eletiva.
- Identificação do Sinal das “Folhas de Outono” (Autumn Leaves): Durante a avaliação endoscópica da mucosa, o cirurgião deve buscar ativamente sinais de sofrimento tecidual. O achado de áreas de descoloração e isquemia mucosa mucosa — denominado sinal das “Folhas de Outono” — indica necrose parietal estabelecida. Diante deste sinal, a desvolvulação endoscópica deve ser imediatamente abortada e o paciente encaminhado em caráter de extrema urgência para laparotomia hemostática e ressecção cirúrgica, devido ao risco iminente de perfuração em cavidade livre.
- Tratamento Definitivo: Em episódios recorrentes de vólvulo ou em quadros neonatais obstrutivos graves com necrose colônica, a colectomia subtotal firma-se como o tratamento definitivo padrão, eliminando o perímetro de redundância colônica e reduzindo a taxa de recidiva do vólvulo a patamares próximos de zero.
Pontos-Chave
- Gravidade Sintomática: O tratamento do dolicossigmóide deve ser guiado pela gravidade da estase fecal, frequência de episódios obstrutivos e complicações isquêmicas, e não apenas pelo achado iconográfico de redundância colônica.
- Indicação Histopatológica: O estágio descompensado do dolicocolon cursa com atrofia muscular e esclerose com perda neuronal irreversível, o que justifica a indicação de ressecção nos casos refratários.
- Superioridade Extensiva: A colectomia subtotal apresenta desfechos funcionais superiores e maior durabilidade quando comparada à sigmoidectomia isolada, a qual apresenta taxas de insucesso de até 45% devido à colostase residual.
- Gatilho de Vólvulo: A redundância estrutural é o principal fator predisponente para torção axial em alça fechada. O sinal endoscópico de “Folhas de Outono” contraindica a derotação endoscópica isolada e impõe laparotomia imediata.
- Manejo na SDO: A associação de sigmoidectomia à rectopexia com tela melhora os escores obstrutivos, mas a redundância colônica de base exige monitoramento devido ao risco elevado de falha funcional tardia.
Conclusões Aplicadas à Prática
O manejo do dolicossigmóide na clínica cirúrgica contemporânea exige o abandono de condutas empíricas em favor de um escalonamento terapêutico preciso, fundamentado na fisiopatologia tecidual e na evidência clínica. Enquanto o suporte conservador e a reabilitação pélvica resguardam os pacientes com distúrbios puramente funcionais ou evacuatórios do compartimento posterior, a cirurgia radical encontra sua indicação precisa diante da falência neuromuscular e estrutural do cólon. O cirurgião do aparelho digestivo deve reconhecer as limitações das ressecções segmentares econômicas no cólon atônico e descompensado. A adoção da colectomia subtotal laparoscópica como o padrão de escolha para casos graves refratários e episódios de vólvulo recorrente reflete a aplicação de uma estratégia cirúrgica focada na segurança e na resolução definitiva. No teatro de operações abdominal, a precisão na indicação cirúrgica e o respeito aos limites biológicos do órgão permanecem como os maiores garantidores do sucesso terapêutico e da qualidade de vida do paciente.
“A cirurgia atinge sua maior nobreza quando compreende os limites da anatomia e submete o bisturi aos ditames da restauração fisiológica.” — Sir Heneage Ogilvie, cujos estudos pioneiros sobre a motilidade e dilatação colônica continuam a inspirar o manejo das colopatias complexas.
Gostou ❔Nos deixe um comentário ✍️ , compartilhe em suas redes sociais e|ou mande sua dúvida pelo 💬 Chat On-line em nossa DM do Instagram.
Specific Competence of Surgical Leadership
Surgeons are uniquely prepared to assume leadership roles because of their position in the operating room (OR). Whether they aspire to the title or not, each and every surgeon is a leader, at least within their surgical team. Their clinical responsibilities offer a rich variety of interpretations that prepare them for a broader role in health care leadership. They deal directly with patients and their families, both in and out of the hospital setting, seeing a perspective that traditional health care administrative leaders rarely experience. They work alongside other direct providers of health care, in varied settings, at night, on weekends, as well as during the typical workday. They understand supply-chain management as something more than lines on a spreadsheet.
The Challenges for a Surgical Leader
Surgeons prefer to lead, not to be led. Surgical training has traditionally emphasized independence, self-reliance, and a well-defined hierarchy as is required in the OR. However, this approach does not work well outside the OR doors. With colleagues, nurses, staff, and patients, they must develop a collaborative approach. Surgeons are entrusted with the responsibility of being the ultimate decision maker in the OR. While great qualities in a surgeon in the OR, it hinders their interactions with others. They have near-absolute authority in the OR, but struggle when switching to a persuasive style while in committees and participating in administrative activities. Most surgeons do not realize they are intimidating to their patients and staff. With patients, a surgeon needs to be empathetic and a good listener. A surgeon needs to slow the pace of the discussion so that the patient can understand and accept the information they are receiving. As perfectionists, surgeons demand a high level of performance of themselves. This sets them up for exhaustion and burnout, becoming actively disengaged, going through the motions, but empty on the inside. Given the many challenges surgeons face, it is difficult for them to understand the leadership role, given its complex demands.
Specific Competencies
Authority
Although teams and all team members provide health care should be allowed input, the team leader makes decisions. The leader must accept the responsibility of making decisions in the presence of all situations. They will have to deal with conflicting opinions and advice from their team, yet they must accept that they will be held accountable for the performance of their team. The surgeon–leader cannot take credit for successes while blaming failures on the team. Good teamwork and excellent communication do not relieve the leader of this responsibility.
Leadership Style
A surgeon often has a position of authority based on their titles or status in an organization that allows them to direct the actions of others. Leadership by this sort of mandate is termed “transactional leadership” and can be successful in accomplishing specific tasks. For example, a surgeon with transactional leadership skills can successfully lead a surgical team through an operation by requesting information and issuing directives. However, a leader will never win the hearts of the team in that manner. The team will not be committed and follow through unless they are empowered and feel they are truly heard. A transformational leader is one who inspires each team member to excel and to take action that supports the entire group. If the leader is successful in creating a genuine atmosphere of cooperation, less time will be spent giving orders and dealing with undercurrents of negativity. This atmosphere can be encouraged by taking the time to listen and understand the history behind its discussion. Blame should be avoided. This will allow the leader to understand the way an individual thinks and the group processes information to facilitate the introduction of change. While leadership style does not guarantee results, the leader’s style sets the stage for a great performance. At the same time, they should be genuine and transparent. This invites the team members to participate, creating an emotional connection. Leaders try to foster an environment where options are sought that meet everyone’s desires.
Conflict Management
Conflict is pervasive, even in healthy, well-run organizations and is not inherently bad. Whether conflict binds an organization together or divides it into factions depends on whether it is constructive or destructive. A good leader needs to know that there are four essential truths about conflict. It is inevitable, it involves costs and risks, the strategies we develop to deal with the conflict can be more damaging than the conflict itself, and conflict can be permanent if not addressed. The leader must recognize the type of conflict that exists and deal with the conflict appropriately. Constructive discussion and debate can result in better decision making by forcing the leader to consider other ideas and perspectives. This dialog is especially helpful when the leader respects the knowledge and opinions of team members with education, experience, and perspective different from the leader’s. Honesty, respect, transparency, communication, and flexibility are all elements that a leader can use to foster cohesion while promoting individual opinion. The leader can create an environment that allows creative thinking, mutual problem solving, and negotiation. These are the hallmarks of a productive conflict. Conflict is viewed as an opportunity, instead of something to be avoided.
Communication Skills
Communication is the primary tool of a successful leader. On important topics, it is incumbent on the leader to be articulate, clear, and compelling. Their influence, power, and credibility come from their ability to communicate. Research has identified the primary skills of an effective communicator. They are set out in the LARSQ model: Listening, Awareness of Emotions, Reframing, Summarizing, and Questions. These are not set in a particular order, but rather should move among each other freely. In a significant or critical conversation, it is important for a leader to listen on multiple levels. The message, body language, and tone of voice all convey meaning. You cannot interrupt or over-talk the other side. They need an opportunity to get their entire message out. Two techniques that enhance listening include pausing and the echo statement. Pausing before speaking allows the other conversant time to process what they have said to make sure the statement is complete and accurate. Echo statements reflect that you have heard what has been said and focuses on a particular aspect needing clarification. Good listening skills assure that the leader can get feedback that is necessary for success.
Vision, Strategy, Tactics, and Goals
One of the major tasks of a leader is to provide a compelling vision, an overarching idea. Vision gives people a sense of belonging. It provides them with a professional identity, attracts commitment, and produces an emotional investment. A leader implements vision by developing strategy that focuses on specific outcomes that move the organization in the direction of the vision. Strategy begins with sorting through the available choices and prioritizing resources. Through clarification, it is possible to set direction. Deficits will become apparent and a leader will want to find new solutions to compensate for those shortfalls. For example, the vision of a hospital is to become a world class health care delivery system. Strategies might include expanding facilities, improving patient satisfaction, giving the highest quality of care, shortening length of hospital stay with minimal readmissions, decreased mortality, and a reduction in the overall costs of health care. Tactics are specific behaviors that support the strategy with the aim to achieve success. Tactics for improving patient satisfaction may include reduced waiting time, spending more time with patients, taking time to communicate in a manner that the patient understands, responding faster to patient calls, etc. These tactics will then allow a leader to develop quantitative goals. Patient satisfaction can be measured. The surgical leader can then construct goals around each tactic, such as increasing satisfaction in specific areas. This information allows a surgical leader to identify barriers and they can take steps to remedy problem areas. This analysis helps a leader find the weakest links in their strategies as they continue toward achieving the vision.
Change Management
The world of health care is in continuous change. The intense rate of political, technical, and administrative change may outpace an individual’s and institution’s ability to adapt. Twenty-first century health care leaders face contradictory demands. They must navigate between competing forces. Leaders must traverse a track record of success with the ability to admit error. They also must maintain visionary ideas with pragmatic results. Individual accountability should be encouraged, while at the same time facilitating teamwork. Most leaders do not understand the change process. There are practical and psychological aspects to change. From an institutional perspective, we know that when 5% of the group begins to change, it affects the entire group. When 20% of a group embraces change, the change is unstoppable.
Succession Planning and Continuous Learning
An often-overlooked area of leadership is planning for human capital movement. As health care professionals retire, take leaves of absences, and move locations, turmoil can erupt in the vacuum. Leaders should regularly be engaging in activities to foster a seamless passing of institutional knowledge to the next generation. They also should seek to maintain continuity to the organization. Ways to accomplish this include senior leaders actively exposing younger colleagues to critical decisions, problem solving, increased authority, and change management. Leaders should identify promising future leaders, give early feedback for areas of improvement, and direct them toward available upward career tracks. Mentoring and coaching help prepare the younger colleagues for the challenges the institution is facing. Teaching success at all levels of leadership helps create sustainable high performance.
ORCID

https://orcid.org/0000-0001-5669-4169
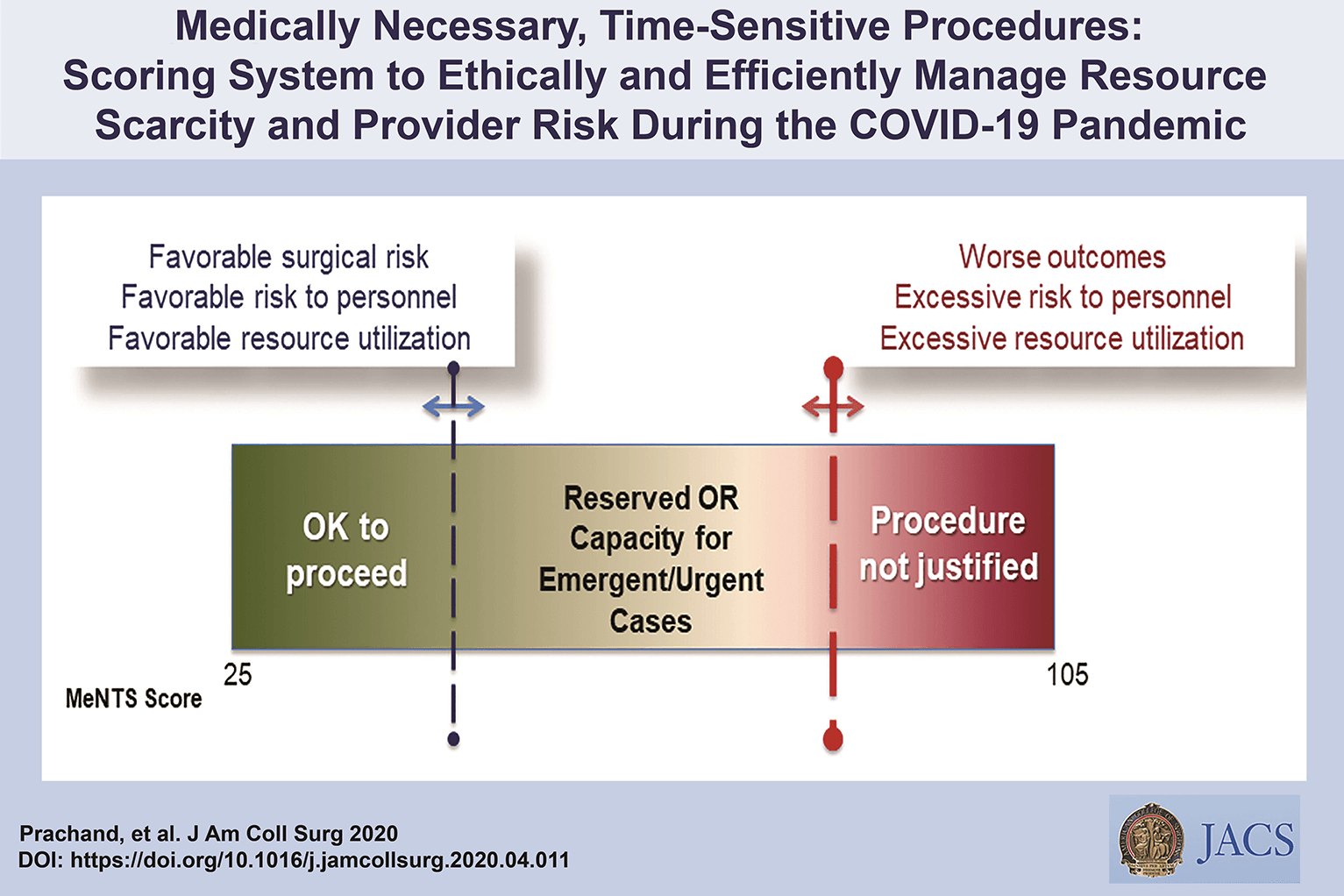
Medically-Necessary, Time Sensitive: (MeNTS) Score
Operating During The COVID-19 Coronavirus Pandemic
“At the University of Chicago, members of the Department of Surgery decided to investigate this issue more precisely. As stay-at-home restrictions in some states are easing, and as non-emergency medical care is being reconsidered, how does one possibly triage the thousands upon thousands of patients whose surgeries were postponed? Instead of the term “elective,” the University of Chicago’s Department of Surgery chose the phrase “Medically-Necessary, Time Sensitive” (MeNTS). This concept can be utilized to better assess the acuity and safety when determining which patients can get to the operating room in as high benefit/low risk manner as possible. And unlike in any recent time in history, risks to healthcare staff as well as risks to the patient from healthcare staff, are now thrown into the equation. The work was published in the April issue of the Journal of the American College of Surgeons.
On March 17, 2020, the American College of Surgeons recommended that all “elective” surgeries be canceled indefinitely. These guidelines were published, stating that only patients with “high acuity” surgical issues, which would include aggressive cancers and severely symptomatic disease, should proceed. Based on the Elective Surgery Acuity Scale (ESAS), most hospitals were strongly encouraged to cancel any surgery that was not high acuity, including slow-growing cancers, orthopedic and spine surgeries, airway surgeries, and any other surgeries for non-cancerous tumors. Heart surgeries for stable cardiac issues were also put on hold. Patients and surgeons waited. Some patients did, indeed undergo non-Covid-19-related surgeries. But most did not. Redeployment is gradually turning to re-entry.
The re-entry process for non-urgent (yet necessary) surgeries is a complicated one. Decisions and timing, based on a given hospital’s number and severity of Covid-19 patients, combined with a given city or state’s current and projected number of Covid-19 cases, how sick those patients will be, and whether or not a second surge may come, involves a fair amount of guesswork. As we have all seen, data manipulation has become a daily sparring match in many arenas. The authors of the study created an objective surgical risk scoring system, in order to help hospitals across this country, as well as others across the world, better identify appropriate timing regarding which surgeries can go ahead sooner rather than later, and why. They factored several variables into their equation, to account for the multiple potential barriers to care, including health and safety of hospital personnel. They created scoring systems based on three factors: Procedure, Disease and Patient Issues.
CALCULATE MeNTS SCORE HERE
The authors of the study created an objective surgical risk scoring system, in order to help hospitals across this country, as well as others across the world, better identify appropriate timing regarding which surgeries can go ahead sooner rather than later, and why. They factored several variables into their equation, to account for the multiple potential barriers to care, including health and safety of hospital personnel. Each patient would receive an overall conglomerate score, based on all of these factors, with the lower risks giving them more favorable scores to proceed with surgery soon, and the higher risks giving patients a higher score, or higher risk regarding proceeding with surgery, meaning it may be safest, for now, to wait.
Dr. Jeffrey Matthews, senior author of the paper, and Department Chair at the University of Chicago, stated that this model is reproducible across hospital systems, in urban, rural, and academic settings. And in the event of potential unpredictable surges of Covid-19 cases, the scoring system “helps prioritize cases not only from the procedure/disease standpoint but also from the pandemic standpoint with respect to available hospital resources such as PPE, blood, ICU beds, and [regular hospital] beds.”
The scoring system is extremely new, and the coming weeks will reveal how patients, surgeons and hospitals are faring as patients without life-and-death emergencies and/or Covid-19 complications gradually begin filling the operating rooms and hospital beds. In addition, and perhaps just as important, the study authors note that creating systems whereby healthcare resources, safety, and impact on outcomes need to be considered more carefully for each patient intervention, the larger impact of each intervention on public health will be better understood: not only for today’s pandemic, but also in future, as yet unknown, global events.”
Source: Nina Shapiro, 2020
Discover our surgical video channel and lectures associated with the surgeon blog.
Share and Join: https://linktr.ee/TheSurgeon
Covid-19 and Digestive Surgery
The current world Covid-19 pandemic has been the most discussed topic in the media and scientific journals. Fear, uncertainty, and lack of knowledge about the disease may be the significant factors that justify such reality. It has been known that the disease presents with a rapidly spreading, it is significantly more severe among the elderly, and it has a substantial global socioeconomic impact. Besides the challenges associated with the unknown, there are other factors, such as the deluge of information. In this regard, the high number of scientific publications, encompassing in vitro, case studies, observational and randomized clinical studies, and even systematic reviews add up to the uncertainty. Such a situation is even worse when considering that most healthcare professionals lack adequate knowledge to critically appraise the scientific method, something that has been previously addressed by some authors. Therefore, it is of utmost importance that expert societies supported by data provided by the World Health Organization and the National Health Department take the lead in spreading trustworthy and reliable information.
Discover our surgical video channel and lectures associated with the surgeon blog.
Share and Join: https://linktr.ee/TheSurgeon
#Medicine #Surgery #GeneralSurgery #DigestiveSurgery
#TheSurgeon #OzimoGama
Abdominal Surgical Anatomy
The abdomen is the lower part of the trunk below the diaphragm. Its walls surround a large cavity called the abdominal cavity. The abdominal cavity is much more extensive than what it appears from the outside. It extends upward deep to the costal margin up to the diaphragm and downward within the bony pelvis. Thus, a considerable part of the abdominal cavity is overlapped by the lower part of the thoracic cage above and by the bony pelvis below. The abdominal cavity is subdivided by the plane of the pelvic inlet into a larger upper part, i.e., the abdominal cavity proper, and a smaller lower part, i.e., the pelvic cavity. Clinically the importance of the abdomen is manifold. To the physician, the physical examination of the patient is never complete until he/she thoroughly examines the abdomen. To the surgeon, the abdomen remains an enigma because in number of cases the cause of abdominal pain and nature of abdominal lump remains inconclusive even after all possible investigations. To summarize, many branches of medicine such as general surgery and gastroenterology are all confined to the abdomen.
Classroom: Abdominal Surgical Anatomy
Perioperative Medicine

Surgery and anesthesia profoundly alter the normal physiologic and metabolic states. Estimating the patient’s ability to respond to these stresses in the postoperative period is the task of the preoperative evaluation. Perioperative complications are often the result of failure, in the preoperative period, to identify underlying medical conditions, maximize the patient’s preoperative health, or accurately assess perioperative risk. Sophisticated laboratory studies and specialized testing are no substitute for a thoughtful and careful history and physical examination. Sophisticated technology has merit primarily in confirming clinical suspicion.
Classroom: Perioperative Medicine
Complications of HEMORROIDH SURGERY

Symptomatic hemorrhoids require a number of therapeutic interventions each of which has its own complications. Office-based therapy such as rubber band ligation carries the risk of pain and bleeding, which are self-limited, but also carries the risk of rare complications such as sepsis, which may be life threatening. Operative treatment of hemorrhoids includes conventional hemorrhoidectomy, stapled hemorrhoidectomy, and the use of energy devices. Complications of pain and bleeding are common but self-limited. Late complications such as stenosis and fecal incontinence are rare. Recurrent disease is related to the initial grade and therapeutic approach. Treatment of recurrent hemorrhoids should be individualized based on previous treatments and the grade of disease. Anesthetic complications, especially urinary retention, are common and related to the anesthetic technique. Practitioners should council their patients as to the risks of the various approaches to treating symptomatic hemorrhoids.
PRINCIPLES OF OSTOMY MANAGEMENT

The creation of a stoma is a technical exercise. Like most undertakings, if done correctly, the stoma will usually function well with minimal complications for the remainder of the ostomate’s life. Conversely, if created poorly, stoma complications are common and can lead to years of misery. Intestinal stomas are in fact enterocutaneous anastomoses and all the principles that apply to creation of any anastomosis (i.e., using healthy intestine, avoiding ischemia and undue tension) are important in stoma creation.
PREVENTION COMPLICATIONS OF COLON SURGERY
COMPLICATIONS OF COLON SURGERY_REVIEW ARTICLE


Colon surgery represents a high number of patients treated at a department of gastrointestinal surgery and is not limited to colon cancer. It includes other non-neoplastic pathologies such as inflammatory bowel disease, diverticular disease or colonic volvulus. As with any major procedure, colon surgery patients may present serious or even fatal complications. The incidence of postoperative complications from colon surgery has been estimated at between 10% and 30% according to selected series. Preventive measures against surgical complications include selection of an appropriate procedure for the patient as well as good preoperative care, appropriate surgical technique and good postoperative management. When diagnosis has been established, risks for patient should be assessed according to patient’s health conditions and type of surgery accomplished. When the patient meets the surgical requirements, an appropriate course of preoperative care should be carried out including colon wash antibiotics and antithrombotic prophylaxis. Postoperative period will be equivalent to any major abdominal surgery. Typically, it was considered appropriate to wait a few days before initiating feeding in order to protect anastomosis; however, some authors agree that an early oral diet hours after intervention is not associated with a higher risk of anastomotic dehiscence and other complications.
Colonoscopia : Quais as principais complicações?
Colonoscopy is a commonly performed procedure for the diagnosis and treatment of a wide range of conditions and symptoms and for the screening and surveillance of colorectal neoplasia. Although up to 33% of patients report at least one minor, transient GI symptom after colonoscopy, serious complications are uncommon. In a 2008 systematic review of 12 studies totaling 57,742 colonoscopies performed for average risk screening, the pooled overall serious adverse event rate was 2.8 per 1000 procedures. The risk of some complications may be higher if the colonoscopy is performed for an indication other than screening. The colorectal cancer miss rate of colonoscopy has been reported to be as high as 6% and the miss rate for adenomas larger than 1 cm is 12% to 17%. Although missed lesions are considered a poor outcome of colonoscopy, they are not a complication of the procedure per se and will not be discussed further in this document. Over 85% of the serious colonoscopy complications are reported in patients undergoing colonoscopy with polypectomy. An analysis of Canadian administrative data, including over 97,000 colonoscopies, found that polypectomy was associated with a 7-fold increase in the risk of bleeding or perforation. However, complication data are often not stratified by whether or not polypectomy was performed. Therefore, complications of polypectomy are discussed with those of diagnostic colonoscopy. A discussion of the diagnosis and management of all complications of colonoscopy is beyond the scope of this document, although general principles are reviewed.
Laparoscopic Colorectal Surgery
With the introduction of laparoscopic colectomy nearly 20 years ago, a relatively slow adoption of laparoscopic colorectal surgery into surgical practice has taken place. It is estimated that 10% to 25% of all colorectal resections are performed utilizing laparoscopy. The persistent steep learning curve, the lack of high-volume colorectal surgery by general surgeons (who perform the bulk of colonic resection in the United States), and the modest advantages reported are but a few of the reasons that the percentage of laparoscopic colorectal procedures has not dramatically risen. With the publication of several large, prospective randomized trials for colon cancer, along with the interest in single-port surgery and natural orifice surgery, there appears to be a renewed interest in minimally invasive procedures for the colon and rectum. This chapter will provide an overview of these issues and offer a current assessment of the common diseases to which minimally invasive techniques have been applied.
Learning Curve
Numerous previous studies have evaluated the learning curve involved in laparoscopic colectomy. It is estimated by conventional laparoscopic techniques that the learning curve for laparoscopic colectomy is at least 20 cases but more likely 50 cases. The need to work in multiple quadrants of the abdomen, the need for a skilled laparoscopic assistant, and the lack of yearly volume has kept the learning curve relatively steep. The surgeon may also need to work in reverse angles to the camera. All of these combined add to the complexity of the procedure and result in the need to perform a number of cases before the surgeon and surgical team become proficient. More recent publications have suggested the learning curve is more than 20 cases. In a prospective randomized study of colorectal cancer in the United Kingdom, the CLASICC trial, surgeons had to perform at least 20 laparoscopic resections before they were allowed to enter the study. The study began in July 1996 and was completed in July 2002. Despite the surgeons’ prior experience, the rate of conversion dropped from 38% to 16% over the course of the study, suggesting that a minimum of 20 cases may not be enough to overcome the learning curve. In the COLOR trial from Europe, another prospective randomized study for colon cancer that required a prerequisite experience in laparoscopic colon resection before surgeons could enter patients in the study, surgeon and hospital volume were directly related to a number of operative and postoperative outcomes. The median operative time for high-volume hospitals (>10 cases/year) was 188 minutes, compared to 241 minutes for low-volume hospitals (<5 cases/year); likewise, conversion rates were 9% versus 24% for the two groups. High-volume groups also had more lymph nodes in the resected specimens, fewer complications, and shortened hospital stays. These two relatively recent multicenter studies suggest that the learning curve is clearly greater than 20 cases and that surgeons need to perform a minimum yearly number of procedures to maintain their skills.
Outcomes
There may not be another area in recent surgical history that has been more heavily scrutinized than laparoscopic colorectal surgery. The plethora of accumulated data allows a careful assessment of all outcome measures for nearly every colorectal disease and procedure. In comparison to conventional colorectal surgery, the benefits of laparoscopy for colorectal procedures compared to open techniques include a reduction in postoperative ileus, postoperative pain, and a concomitant reduction in the need for analgesics; an earlier tolerance of diet; a shortened hospital stay; a quicker resumption of normal activities; improved cosmesis; and possibly preservation of immune function. This is offset by a prolongation in operative time, the cost of laparoscopic equipment, and the learning curve for these technically challenging procedures. When reporting the outcomes of laparoscopic colectomy, a natural selection bias applies when comparing conventional and laparoscopic cases. The most complex cases are generally not suitable for a laparoscopic approach and therefore are performed via an open approach. Also, in many series the results of the successfully completed laparoscopic cases are compared to conventional cases, and the cases converted from a laparoscopic to a conventional procedure may be analyzed separately. Few studies, with the exception of the larger prospective randomized studies, leave the converted cases in the laparoscopic group as part of the “intention to treat” laparoscopic group. This clearly introduces selection bias.
Although the results of prospective randomized trials are available for almost every disease process requiring colorectal resection, the majority of studies of laparoscopic colectomy are retrospective case-control series or noncomparative reports. The conclusions regarding patient outcomes must therefore come from the repetitiveness of the results rather than the superiority of the study design. For any one study, the evidence may be weak; but collectively, because of the reproducibility of results by a large number of institutions, even with different operative techniques and postoperative management parameters, the preponderance of evidence favors a minimally invasive approach with respect to postoperative outcomes.
Operative Time
Nearly all the comparative studies provide information regarding operative times. The definition of the operative time may vary with each series, and there may be different groups of surgeons performing the laparoscopic and conventional procedures. With the exception of a few reports, nearly all studies demonstrated a prolonged operative time associated with laparoscopic procedures. In prospective randomized trials, the procedure was roughly 40 to 60 minutes longer in the laparoscopic groups. As the surgeon and team gain experience with laparoscopic colectomy, the operating times do reliably fall, but rarely do they return to the comparable time for a conventional approach.
Return of Bowel Activity and Resumption of Diet
Reduction in postoperative ileus is one of the proposed major advantages of minimally invasive surgery. Nearly all of the retrospective and prospective studies comparing open and laparoscopic colectomy have shown a statistically significant reduction in the time to passage of flatus and stool. Most series demonstrate a 1- to 2-day advantage for the laparoscopic group. Whether the reduction of ileus relates to less bowel manipulation or less intestinal exposure to air during minimally invasive surgery remains unknown. With the reduction in postoperative ileus, the tolerance by the patient of both liquids and solid foods is quicker following laparoscopic resection. The time to resumption of diet varies from 2 days to 7 days, but in the majority of comparative studies, this is still 1 to 2 days sooner than in patients undergoing conventional surgery. Again, the physician and patient were not blinded in nearly all studies, which may have altered patient expectations. However, the overwhelming reproducible data reported in both retrospective and prospective studies of laparoscopic procedures does likely favor a reduction of postoperative ileus and tolerance of liquid and solid diets.
Postoperative Pain
To measure postoperative pain, a variety of assessments have been performed to demonstrate a significant reduction in pain following minimally invasive surgery; some studies utilize an analog pain scale, and others measure narcotic requirements. Physician bias and psychologic conditioning of patients may interfere with the evaluation of postoperative pain. There are also cultural variations in the response to pain. Three of the early prospective randomized trials have evaluated pain postoperatively, and all three have found a reduction in narcotic requirements in patients undergoing laparoscopic colectomy. In the COST study, the need both for intravenous and oral analgesics was less in patients undergoing successfully completed laparoscopic resections. Numerous other nonrandomized studies have shown a reduction in postoperative pain and narcotic usage.
Length of Stay
The quicker resolution of ileus, earlier resumption of diet, and reduced postoperative pain has resulted in a shortened length of stay for patients after laparoscopic resection when compared to traditional procedures. Recovery after conventional surgery has also been shortened, but in the absence of minimally invasive techniques, it would seem unlikely that the length of stay could be further reduced. In nearly all comparative studies, the length of hospitalization was 1 to 6 days less for the laparoscopic group. Although psychological conditioning of the patient cannot be helped and likely has a desirable effect, the benefits of minimally invasive procedures on the overall length of stay cannot be discounted. The benefit, however, is more likely a 1 to 2 day advantage only. The more recent introduction of clinical pathways, both in conventional and laparoscopic surgery, has also narrowed the gap but appears to be more reliable in patients undergoing a minimally invasive approach.
Hospital Costs
One of the disadvantages of laparoscopy is the higher cost related to longer operative times and increased expenditures in disposable equipment. Whether the total cost of the hospitalization (operative and hospital costs) is higher following laparoscopic colectomy is debatable. A case-control study from the Mayo Clinic looked at total costs following laparoscopic and open ileocolic resection for Crohn’s disease (CD). In this study, 66 patients underwent laparoscopic or conventional ileocolic resection and were well matched. Patients in the laparoscopic group had less postoperative pain, tolerated a regular diet 1 to 2 days sooner, and had a shorter length of stay (4 vs. 7 days). In the cost analysis, despite higher operative costs, the overall mean cost was $3273 less in the laparoscopic group. The procedures were performed by different groups of surgeons at the institution, and although the surgeons may have introduced biases, this study was undertaken during the current era of cost containment, in which all physicians are encouraged to reduce hospital stays. The results are similar for elective sigmoid diverticular resection with a mean cost savings of $700 to $800. Clearly, if operative times and equipment expenditure are minimized, the overall cost of a laparoscopic resection should not exceed a conventional approach.
Tratamento Laparoscópica da DIVERTICULITE AGUDA
O aumento da prevalência de doença diverticular fez o seu adequado manuseio mais um assunto de debate constante. Especialmente para os casos de diverticulite, progresso considerável tem sido feito em termos de diagnóstico e tratamento. Diagnóstico apropriado em TC e técnicas intervencionistas são agora amplamente disponíveis, bem como agentes antimicrobianos eficazes. Finalmente, como a ressecção cirúrgica do cólon envolvido é a única maneira de erradicar definitivamente essa condição, a colectomia eletiva laparoscópica surgiu como uma opção segura e interessante entre as opções de tratamento. Embora tenha sido recentemente contestada sobre a sua progressão, a história natural da diverticulite é assumida como sendo a de recorrência ao longo do tempo, pelo menos, em um terço dos pacientes. O medo das complicações desta doença benigna e prevalente tem motivado sociedades médicas e cirúrgicas para produzir orientações e consensos sobre o assunto. A mortalidade geralmente vem de sepse recorrente e/ou operações de emergência para casos mais complicados. Como resultado, o procedimento cirúrgico mais realizado, a sigmoidectomia eletiva, é normalmente indicada para todos os casos complicados e muitos dos não-complicados. A abordagem laparoscópica para a colectomia esquerda tem evoluído e condições seguras são oferecidas aos pacientes, quando realizado por cirurgiões experientes em laparoscopia.
Transanal Endoscopic Microsurgery for Rectal Tumors

Cancer of the rectum is the fifth most common form of cancer in adults worldwide. In 2012, an estimated 40,300 new rectal cancers will be diagnosed in the US with a median age 69 years. Five-year survival rates for rectal cancer are high for early stage disease (90% for Stage I disease) but drop significantly with worsening stage (7% for metastatic Stage IV disease). Recently, advances in neoadjuvant and adjuvant therapy have decreased the rate of local recurrence and improved long-term survival for some patients. Although the treatment for rectal cancer has become increasingly multimodal, surgical excision of the primary tumor remains essential for eradication of disease.
For a long time there has been a debate about the best surgical approach to early stage rectal cancer, whether treatment should involve radical excision (excision of the rectum) or local excision (tumor alone). Proponents of radical surgery argue that excision of the rectum with its surrounding lymphatic drainage offers the best chance for cure. On the other hand, advocates of local excision feel that a less-aggressive approach can avoid the potential ramifications of major pelvic surgery such as sepsis, poor anorectal function, sexual dysfunction, and difficulty with urination and can eliminate the potential need for a permanent stoma. Although the debate has gone back and forth on the adequacy of local excision, there is a growing body of scientific data that suggests that local excision can be sufficient in patients with early rectal cancer of the mid and distal rectum with good histologic features and preoperative imaging (computed tomography, magnetic resonance imaging, and endorectal ultrasound) that shows no evidence of lymph node involvement.
Traditionally, transanal excision has been performed with the conventional technique using traditional equipment. Although this conventional technique can give surgeons operative access to most distal rectal lesions, it can be difficult to conduct on mid-rectal tumors or in large patients with a deep buttock cleft. The technical difficulties experienced under such circumstances can lead to poor visualization, inadequate margins, or specimen fragmentation. In response to the technical limitations of conventional transanal excision, in the 1980s Professor Gehard Buess from Tubingen, Germany, began to develop the technique of transanal endoscopic microsurgery (TEM).

In collaboration with the Richard Wolf Company in Germany, Dr Buess developed the specialized instruments necessary to perform endoscopic surgery transanally. TEM was introduced into clinical practice in 1983, and was gradually implemented in several European countries and eventually introduced in North America and Asia. The last decade has witnessed international growth in the application of TEM yielding a significant amount of scientific data to support its clinical merits and advantages and also shedding some light on its limitations.
PÓLIPOS COLORRETAIS
Os pólipos colorretais são estruturas que se projetam na superfície da camada mucosa do intestino grosso, podendo ser neoplásicos ou não. Foi Morson, em 1976, quem melhor estabeleceu uma classificação para os diversos tipos de pólipos e a importância da progressão adenoma-câncer. Os pólipos foram divididos em: pólipos neoplásicos, caracterizados pelos adenomas e os carcinomas, e os pólipos não-neoplásicos, que incluem os tipos epiteliais hamartomatosos, inflamatórios, hiperplásicos ou metaplásicos. Os pólipos adenomatosos, que correspondem a cerca de 70% de todos os pólipos, são conhecidamente lesões pré-malignas que antecedem, em 10 a 15 anos, o câncer colorretal. Por conta dessa progressão lenta, a detecção de lesões pré-neoplásicas no intestino grosso é relevante na prevenção do surgimento e complicações do câncer colorretal. Os pólipos podem ser ressecados (polipectomia) antes da sua malignização, diminuindo sobremaneira a taxa de morbimortalidade do câncer colorretal.

A colonoscopia é o padrão-ouro para o diagnóstico do câncer colorretal e para a detecção e ressecção endoscópica das lesões precursoras. A realização de polipectomias e biópsias permite, através da histopatologia, avaliar o tipo histológico, o grau de displasia e as margens de ressecção a fim de quantificar seu potencial de malignização. O câncer colorretal é a quinta neoplasia maligna mais frequente no Brasil, e se estima que 26.990 novos casos tenham sido diagnosticados no ano de 2008, o que evidencia sua alta frequência. Estes valores correspondem a um risco estimado de 13 casos novos a cada 100 mil homens e 15 para cada 100 mil mulheres. Associado a isso, a grande maioria dos tumores malignos se origina dos adenomas, e a detecção e retirada precoces evitam a progressão para o câncer.
SIGMOID DIVERTICULITIS : OPTIONS OF TREATMENT

Sigmoid diverticulitis is a common disease which carries both a significant morbidity and a societal economic burden. Recently published data indicate that sigmoid diverticulitis does not mandate surgical management after the second episode of uncomplicated disease as previously recommended. Rather, a more individualized approach, taking into account frequency, severity of the attacks and their impact on quality of life, should guide the indication for surgery. On the other hand, complicated diverticular disease still requires surgical treatment in patients with acceptable comorbidity risk and remains a life-threatening condition in the case of free peritoneal perforation. Laparoscopic surgery is increasingly accepted as the surgical approach of choice for most presentations of the disease and has also been proposed in the treatment of generalized peritonitis. There is not sufficient evidence supporting any changes in the approach to management in younger patients. Conversely, the available evidence suggests that surgery should be indicated after one attack of uncomplicated disease in immunocompromised individuals.
SIGMOID DIVERTICULITIS_ REVIEW ARTICLE
TRATAMENTO DA TROMBOSE HEMORROIDÁRIA

A trombose hemorroidária é uma condição dolorosa e desconfortável que ocorre quando um coágulo de sangue se forma dentro de uma hemorróida. Essa condição é mais comum em gestantes, pessoas com constipação intestinal crônica, e em situações que aumentam a pressão intra-abdominal, como exercícios físicos intensos e levantamento de peso. Neste artigo, exploraremos as causas, sintomas e opções de tratamento para a trombose hemorroidária, ajudando você a entender melhor essa condição e a buscar a melhor abordagem para o seu caso.
Causas da Trombose Hemorroidária
A trombose hemorroidária geralmente está relacionada a fatores de estilo de vida e hábitos pessoais. Os principais gatilhos incluem:
- Obstipação (prisão de ventre): O esforço excessivo para evacuar aumenta a pressão nas veias do ânus, e as fezes endurecidas podem causar traumatismo no tecido anal.
- Gravidez: A pressão adicional no abdômen durante a gravidez pode contribuir para o desenvolvimento da trombose.
- Esforços prolongados e levantamento de peso: Atividades que aumentam a pressão intra-abdominal são fatores de risco.
- Higiene inadequada: A falta de cuidados apropriados na região anal pode exacerbar a condição.
- Fatores adicionais: Permanecer sentado por longos períodos, consumo excessivo de alimentos picantes e bebidas alcoólicas, e prática de sexo anal.
Sintomas da Trombose Hemorroidária
Os principais sinais de trombose hemorroidária incluem:
- Dor intensa na região anal: A dor é geralmente súbita e pode ser bastante severa.
- Sangramento: Frequentemente observado durante a evacuação.
- Inchaço e aumento de volume: Um nódulo na região anal pode se tornar arroxeado ou preto, indicando a presença de um trombo.
Tratamentos Indicados
O tratamento da trombose hemorroidária varia conforme a gravidade da condição. Entre as abordagens recomendadas estão:
- Uso de analgésicos e pomadas anestésicas: Para alívio da dor e desconforto.
- Banhos de assento: Utilizar água morna para aliviar os sintomas e reduzir o inchaço.
- Correção dos hábitos alimentares: Aumentar a ingestão de fibras e líquidos para prevenir a obstipação.
- Tratamento cirúrgico: Em casos mais graves, pode ser necessário realizar uma cirurgia para remover a hemorróida e o trombo.
Se você apresenta sintomas semelhantes, é crucial consultar um médico para uma avaliação adequada e receber o tratamento adequado.
Gostou ❔ Nos deixe um comentário ✍️, ou mande sua dúvida pelo 💬 Chat On-line.
Lembre-se: A informação aqui fornecida é para orientação geral. Sempre consulte seu médico para aconselhamento específico sobre sua situação.
Não Deixe Sua Saúde Esperar! Entre em Contato Conosco Agora!
☎️ CHAT ONLINE 📞
Entre em contato conosco através da nossa central de atendimento dedicada. Nossos especialistas estão prontos para fornecer orientações personalizadas e responder a todas as suas perguntas. Juntos, podemos trabalhar para garantir o melhor para a sua saúde.
🩺(98)991304454 & (98)988664454📲
ATENDIMENTO REMOTO (TELEMEDICINA)
🤳🏻 Agende com os nossos #especialistas pelo WhatsApp ou Telefone
📲 👩🏽⚕️ Clínico: (98) 9 9130 4454
📲 👨🏻⚕️ Cirúrgico: (98) 9 8866 4454
#TromboseHemorroidária #SaúdeDigestiva #TratamentoHemorroidário #BemEstar #CuidadosComASaúde
VEJA AQUI ONDE FAZER UMA AVALIAÇÃO ESPECIALIZADA E RECEBER UMA SEGUNDA OPINIÃO
GASTROINTESTINAL STROMAL TUMORS (GIST)

INTRODUÇÃO
GIST, da sigla em inglês gastrointestinal stromal tumors, pertence a um grupo de tumores chamados sarcoma de partes moles. Essa neoplasia se diferencia dos outros tipos de tumores por iniciar-se na parede dos órgãos, junto às camadas musculares do trato gastrointestinal, mais especificamente, nas células do plexo mioenterico, chamadas células de Cajal. Tais células são responsáveis pela motilidade intestinal, sendo consideradas o marca-passo do trato gastrointestinal.
O tumor de GIST é relativamente raro, com estudos atuais mostrando uma prevalência anual em torno de 20 a 40 casos por milhão de habitantes. É mais comum entre pessoas de 50 a 60 anos de idade, sendo extremamente raros até os 20 anos. Por representar um tumor raro, recomenda-se que seja tratado por serviços especializados com cirurgiões do aparelho digestivo, que tenham experiência multidisciplinar na condução e no tratamento dos pacientes com este tumor.
O GIST pode se originar em qualquer local do trato gastrointestinal, do esôfago ao ânus. Em relação à distribuição, 50% a 60% das lesões são provenientes do estômago, 20% a 30% do intestino delgado, 10% do intestino grosso, 5% do esôfago e 5% de outros locais da cavidade abdominal.
DIAGNÓSTICO
A apresentação clínica dos pacientes portadores de GIST não é especifica e depende da localização e do tamanho do tumor. O GIST tem uma característica biológica que é uma mutação genética, com ativação do proto-oncogene Kit e a superexpressão do receptor tirosina quinase (c-Kit). Geralmente, o diagnóstico é feito por uma biópsia da lesão, que a depender da localização, pode ser feita por endoscopia, colonoscopia, ou ecoendoscopia. A tomografia computadorizada do abdômen é importante para avaliação da extensão do tumor e também pode ser utilizada em alguns casos para realização de biópsia do tumor. Não apresentam sinais e/ou sintomas específicos. Podem causar náuseas, vômitos, hemorragias intestinais (vômitos com sangue ou evacuações com sangue ou fezes enegrecidas), sensação de plenitude após alimentação, dor e distensão abdominal, ou presença de uma massa ou tumor palpável no abdômen.
TRATAMENTO
O tratamento padrão para pacientes com GIST não metastático, ou seja, não provenientes de outros órgãos, é a ressecção cirúrgica completa da lesão. Muitas vezes é necessária a cirurgia radical e de grande porte, com a retirada de estruturas e órgãos aderidos, oferecendo a maior chance de cura. O tratamento com imatinib, e mais atualmente ao sunitinib, é utilizado para doença metastática ou irressecável, com intuito de diminuir o tamanho da lesão para que a cirurgia possa ser realizada em melhores condições locais. Tais drogas também podem ser utilizadas após a cirurgia. Para o tratamento sistêmico pode ser necessário estudo genético específico para saber qual a mutação presente no tumor, com intuito de guiar a terapia em relação à dose e tipo de medicação utilizada.
FATORES DE RISCO
Não há fatores de risco diretamente relacionados a essa neoplasia. Manter hábitos de vida saudáveis, uma alimentação balanceada e a prática de exercícios físicos ajudam, de maneira geral, na prevenção do câncer.
PARA MAIS INFORMAÇÕES: http://www.gistsupport.org/
Avanços no tratamento cirúrgico das METÁSTASES HEPÁTICAS DE ORIGEM COLORRETAL

O câncer colorretal é o terceiro tumor mais frequente no ocidente. Cerca de 50% dos pacientes desenvolvem metástases hepáticas na evolução da doença, as quais são responsáveis por, no mínimo, dois terços das mortes. O avanço nas técnicas cirúrgicas e a melhora dos esquemas quimioterápicos têm permitido oferecer tratamento com intuito curativo a um número cada vez maior de pacientes. Os avanços recentes do tratamento das metástases hepáticas, incluindo estratégias para aumentar as ressecções (por exemplo: embolização da veia porta, ablação por radiofrequência, hepatectomia em dois tempos, quimioterapia de conversão e estratégia inversa de tratamento) e hepatectomias na presença de doença extra-hepática possibilitam uma melhor sobrevida dos pacientes.
Prevenção e Rastreamento do Câncer Colorretal
O Papel Proativo do Cirurgião na Interrupção da Sequência Adenoma-Carcinoma
Autor: Prof. Dr. Ozimo Gama (Tempo de Leitura: 9 minutos)
Introdução
O Câncer Colorretal (CCR) representa um dos maiores paradoxos da oncologia moderna: é uma das neoplasias mais letais e prevalentes no mundo, e, simultaneamente, uma das mais preveníveis. Para o cirurgião do aparelho digestivo, compreender a biologia tumoral e os protocolos de rastreamento (screening) é tão fundamental quanto dominar a técnica de uma retossigmoidectomia com excisão total do mesorreto (TME). A prevenção do CCR não se restringe a orientações dietéticas; ela é um ato intervencionista. Ao compreender e atuar na fisiopatologia da doença, o médico em formação — seja o estudante de medicina ou o residente de cirurgia — assume o protagonismo na redução da morbimortalidade associada a esta patologia.
O Cenário Brasileiro
A relevância do CCR no Brasil exige atenção redobrada. Segundo as estimativas do Instituto Nacional de Câncer (INCA) para o triênio 2023-2025, são esperados cerca de 45.630 novos casos anuais no país. Atualmente, o CCR ocupa a segunda posição entre os cânceres mais incidentes tanto em homens quanto em mulheres (excluindo os tumores de pele não melanoma). As regiões Sul e Sudeste concentram as maiores taxas, refletindo a íntima relação da doença com a urbanização, sedentarismo e ocidentalização da dieta (alto consumo de carne vermelha processada e baixo teor de fibras).
A Janela de Oportunidade Biológica
A pedra angular da prevenção do CCR é a teoria genética da sequência adenoma-carcinoma, descrita classicamente por Vogelstein. Sabemos que mais de 90% dos carcinomas colorretais esporádicos surgem de lesões benignas precursoras (pólipos adenomatosos ou lesões serrilhadas). Esse processo de acúmulo de mutações genéticas (como APC, KRAS, TP53) é lento. Estima-se que a transição de um adenoma inicial para um adenocarcinoma invasivo leve de 10 a 15 anos. Esta progressão insidiosa cria uma “janela de oportunidade” excepcional para a intervenção médica: a detecção e ressecção das lesões precursoras antes que a malignidade se instale.
Fatores de Risco e Prevenção Primária
A prevenção primária foca em evitar o surgimento dos pólipos. Envolve a mitigação de fatores de risco modificáveis:
- Dietéticos: Redução do consumo de carnes processadas e vermelhas; aumento da ingestão de fibras, cálcio e vitamina D.
- Estilo de vida: Combate ao tabagismo, ao etilismo excessivo e à obesidade (o tecido adiposo visceral é um órgão endócrino ativo que promove um estado pró-inflamatório crônico).
Aplicação na Cirurgia Digestiva: O Rastreamento (Prevenção Secundária)
Para o cirurgião endoscopista, a colonoscopia é a arma definitiva. Diferente de outros métodos de rastreio (como a mamografia ou o PSA, que são puramente diagnósticos), a colonoscopia é diagnóstica e terapêutica.

Protocolos de Rastreamento (Screening)
As diretrizes globais sofreram mudanças recentes devido ao aumento alarmante da incidência de CCR em adultos jovens (abaixo dos 50 anos).
- Risco Habitual (População Geral): A Sociedade Americana de Câncer (ACS) e a Força-Tarefa de Serviços Preventivos dos EUA (USPSTF) passaram a recomendar o início do rastreamento aos 45 anos (e não mais aos 50). No Brasil, sociedades médicas (como o CBCD e a SOBED) já endossam essa antecipação. O rastreio pode ser feito através de Colonoscopia (a cada 10 anos) ou Pesquisa de Sangue Oculto nas Fezes (FIT) anualmente, reservando a colonoscopia para os casos positivos.
- Risco Aumentado (Histórico Familiar): Pacientes com parente de 1º grau com CCR ou adenoma avançado devem iniciar o rastreio aos 40 anos, ou 10 anos antes da idade de diagnóstico do familiar mais jovem (o que ocorrer primeiro).
- Alto Risco (Síndromes Hereditárias e DII):
- PAF (Polipose Adenomatosa Familiar): Rastreio inicia aos 10-12 anos de idade com retossigmoidoscopia. A colectomia profilática é a regra.
- Síndrome de Lynch (HNPCC): Colonoscopia anual ou bienal a partir dos 20-25 anos.
- Doenças Inflamatórias Intestinais (Retocolite Ulcerativa e Crohn): Rastreio intensivo com biópsias seriadas após 8 anos de doença ativa devido ao risco de displasia secundária à inflamação crônica.
Pontos-Chave para a Prática Diária
- Idade de Início: Atualize-se sobre a mudança paradigmática do início do rastreamento para os 45 anos na população de risco habitual.
- Polipectomia é Prevenção: A remoção endoscópica de um adenoma tubular (polipectomia, mucosectomia ou ESD) não é apenas um procedimento diagnóstico; é um ato cirúrgico profilático que salva vidas.
- História Clínica: A anamnese detalhada sobre o histórico oncológico familiar é o teste genético mais barato e eficaz à disposição do médico. Nunca negligencie a construção do heredograma.
Conclusões Aplicadas
A cirurgia oncológica colorretal atingiu patamares de excelência técnica com a laparoscopia e a cirurgia robótica. No entanto, o triunfo definitivo do cirurgião do aparelho digestivo não reside na ressecção de grandes massas tumorais, mas sim na sua prevenção. A atuação ativa do especialista na conscientização dos pacientes, na solicitação rigorosa de exames de rastreio nos prazos adequados e na execução meticulosa de colonoscopias profiláticas é o que verdadeiramente altera a curva epidemiológica desta doença devastadora no Brasil e no mundo.
“As nações ocidentais estão cavando suas próprias sepulturas com os próprios dentes. (…) Se você tem um chão inundado por uma torneira aberta, de nada adianta passar um esfregão sem antes fechar a torneira.” — Denis Parsons Burkitt, renomado cirurgião e pesquisador, sobre a importância da dieta e da prevenção nas doenças do trato gastrointestinal.
Gostou ❔Nos deixe um comentário ✍️ , compartilhe em suas redes sociais e|ou mande sua dúvida pelo 💬 Chat On-line em nossa DM do Instagram.
Apendicectomia Convencional X Laparoscópica : Existe Vantagem?

A apendicite aguda é uma doença freqüente que acomete em sua maioria homens com uma idade média ao redor de 20 anos. O seu tratamento é cirúrgico e está bem estabelecido em sua abordagem convencional. O surgimento e o desenvolvimento da videolaparoscopia abriu uma nova opção para a abordagem cirúrgica dessa patologia, permitindo uma abordagem minimamente invasiva com todas as vantagens dessa técnica.
A primeira apendicectomia videolaparoscópica foi realizada há pouco mais de 20 anos. Nessas duas décadas muito se discutiu, e ainda discute-se, a respeito deste procedimento. Mesmo encontrando com freqüência vários estudos bem realizados na literatura, ainda não há um consenso a respeito das indicações precisas para a realização da apendicectomia laparoscópica; ou mesmo sobre qual método seria superior – o convencional ou o laparoscópico. No entanto, uma revisão atual da literatura nos permite observar que os novos estudos mostram a apendicectomia laparoscópica como um procedimento seguro e eficaz, que pode ser utilizado no tratamento da apendicite complicada em qualquer faixa etária e quando o diagnóstico é duvidoso. Por estes motivos, essa opção cirúrgica está ganhando cada vez mais aceitação sendo que vários trabalhos recentes apontam-na como procedimento de escolha no tratamento da apendicite aguda.
ARTIGO DE METANÁLISE
AVALIAÇÃO PRÉ-OPERATÓRIA
MEDICINA BASEADA EM EVIDÊNCIA_AVALIAÇÃO PRÉ_OPERATÓRIA

O médico CIRURGIÃO realiza a avaliação pré-operatória e define a necessidade de avaliação complementar, considerando a otimização das condições clínicas do paciente e a realização de exames complementares. Pacientes hígidos, com idade inferior a 40 anos, sem fatores de risco detectados na anamnese e no exame físico, a serem submetidos a cirurgias de pequeno porte, após a avaliação clínica básica poderão ser encaminhados à cirurgia após avaliação do Anestesiologista. Porém, nos casos em que o paciente tenha alguma comorbidade, idade maior de 60 anos, estado físico ASA II ou acima, obesidade, dependência funcional ou cirurgia de médio ou grande porte, estará indicado avaliação pré-operatória mais pormenorizada .
Colostomia Temporária: Quando está indicada a cirurgia de reversão?
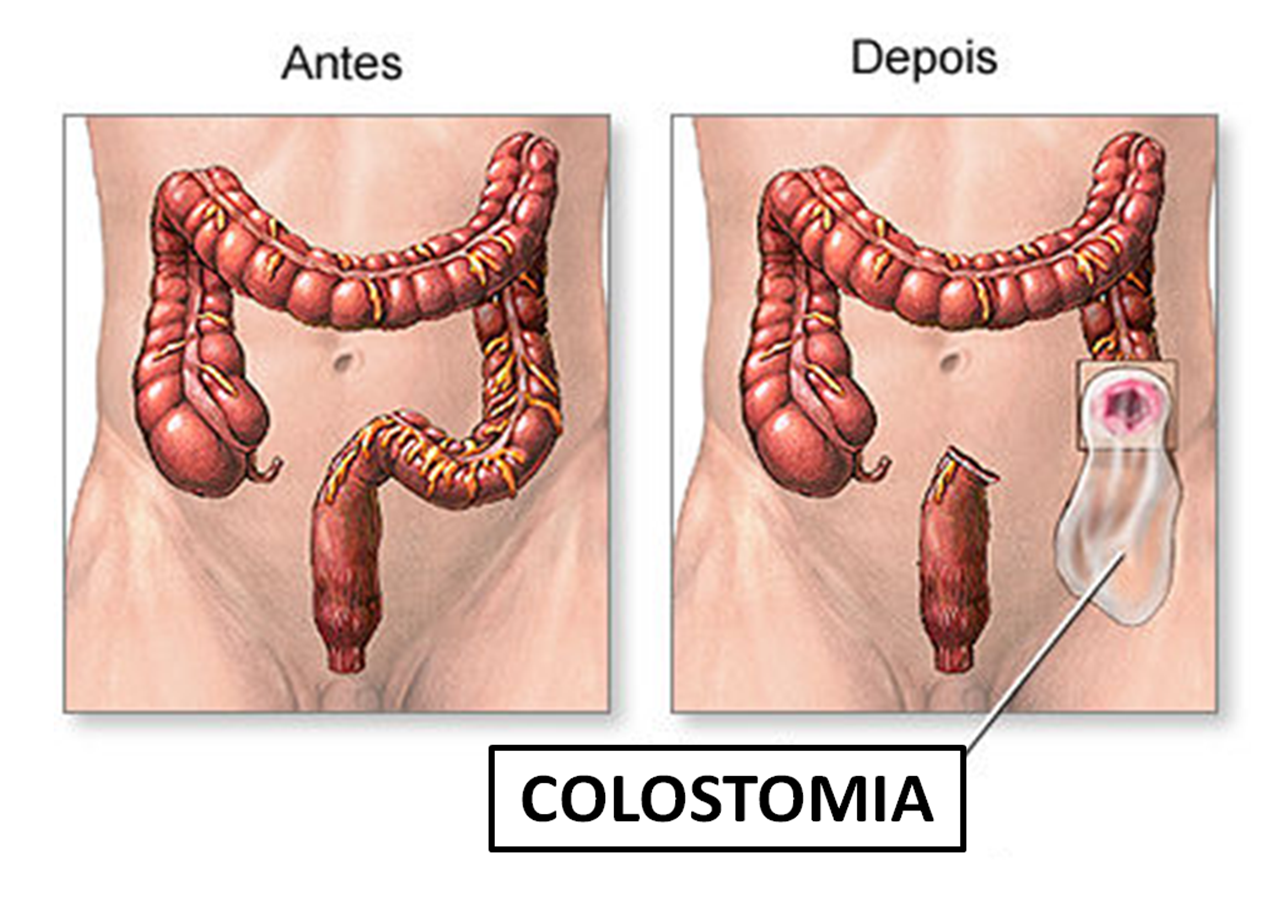
I. INTRODUÇÃO
Apesar de uma diminuição global nas últimas décadas do número de realizações de colostomias temporárias, esta ainda é uma técnica cirúrgica de grande importância no arsenal de opções terapêuticas do CIRURGIÃO DIGESTIVO & COLOPROCTOLOGISTA.
II. EVENTOS ADVERSOS RELACIONADOS
As colostomias, também conhecidas como ostomias, geralmente realizadas em caráter de urgência são desagradáveis para os pacientes e podem trazer uma série de eventos adversos pela sua presença, em especial o risco de infecção de parede abdominal, prolapso (saída) do intestino pela colostomia, oclusão intestinal e as hérnias (enfraquecimento da parede abdominal) para-estomais (ao redor da colostomia), variando a incidência desses eventos adversos em até 60% dos pacientes.
III. RECONSTRUÇÃO DO TRÂNSITO INTESTINAL
Até o momento não se encontra consenso na literatura médica em relação ao tempo ideal de fechamento de uma colostomia temporária. O período clássico de 8 a 12 semanas, encontrado na maioria das publicações, deve ser analisado com grande senso crítico. Os trabalhos científicos especializados identificam taxas de eventos adversos relacionados a cirurgia de fechamento da colostomia ou reconstrução do trânsito intestinal extremamente variadas, com índices que vão de 10% até quase 50% dos casos. O que podemos identificar a partir destes dados é que as cirurgias de decolostomias (cirurgia de reversão de colostomia) são cirurgias complexas e de difícil comparação entre os casos individuais em virtude da especificidade das indicações clínicas. Contudo os fatores inerentes ao próprio paciente, tais como:
1. idade (acima de 60 anos);
2. comorbidades associadas (presença de Diabetes e Hipertensão Arterial);
3. uso crônico de medicações (tais como Corticóides);
4. grau de desnutrição (Albumina sérica menor que 3,0 g/dl); e
5. doença de base que levou a cirurgia de colostomia exercem influência direta no aumento da morbidade (taxa de eventos adversos) dessas operações.
Desta forma, uma diverticulite aguda complicada, um tumor de cólon obstrutivo, uma lesão colônica por projétil de arma de fogo ou arma branca, ou ainda uma perfuração durante um exame endoscópico provocam, dependendo do paciente, respostas metabólicas e endócrinas variáveis, promovendo também efeitos diversos no processo de cicatrização das feridas no pós-operatórios. Portanto quando da programação das cirurgias de restituição do trânsito intestinal uma das avaliações clínicas de grande importância é a total recuperação do trauma cirúrgico anterior que levou a realização da colostomia que é peculiar de paciente para paciente.
IV. AVALIAÇÃO PRÉ-OPERATÓRIA
A programação do fechamento da colostomia através da cirurgia de DECOLOSTOMIA é realizada pela avaliação do estado clínico atual do paciente, assim também como a condição em que se encontram os segmentos intestinais envolvidos, que são apreciados pelos exames radiológicos contrastados (ENEMA OPACO – TRÂNSITO INTESTINAL) e endoscópicos (COLONOSCOPIA) da porção intestinal a ser reconstruída. Outra avaliação importante é que, do ponto de vista técnico, colostomias feitas em caráter de urgência e a presença de aderências intra-abdominais podem resultar na necessidade de ressecções adicionais de segmentos intestinais.
Técnicas de Reconstrução do Trânsito Intestinal
- Anastomose Colorretal
Este procedimento consiste na reconexão do cólon ao reto, permitindo que as fezes sejam eliminadas pelo ânus. Trata-se de uma técnica indicada para determinados pacientes, dependendo das condições específicas e da avaliação do cirurgião. - Rebaixamento do Cólon com Anastomose Coloanal
Essa técnica envolve o rebaixamento de uma parte do cólon e sua conexão direta ao canal anal. É uma alternativa recomendada em casos específicos. A utilização de ferramentas como a manometria anorretal pode auxiliar na indicação dessa abordagem. - Exteriorização do Reto e Anastomose em Segundo Tempo
Em situações em que a cirurgia inicial envolveu a remoção do reto, o cirurgião pode optar por exteriorizar o cólon. Posteriormente, em um segundo procedimento cirúrgico, realiza-se a anastomose entre o canal anal ou reto e o cólon restante, restabelecendo o trânsito intestinal.

Observação Importante
A escolha da técnica mais adequada é altamente individualizada, considerando as condições específicas do paciente, bem como a experiência e o julgamento técnico do cirurgião. Devido à complexidade dessas intervenções, tais procedimentos geralmente são conduzidos por profissionais especializados em CIRURGIA DO APARELHO DIGESTIVO & COLOPROCTOLOGIA.
V. PROGNÓSTICO
A cirurgia de reconstrução do trânsito intestinal após colostomia é um procedimento cirúrgico complexo com expressiva morbimortalidade. Os eventos adversos mais comuns da cirurgia de reversão de colostomia são as INFECÇÕES e os VAZAMENTOS DA ANASTOMOSE (FÍSTULAS). Os resultados da cirurgia de reconstrução intestinal segundo Gomes da Silva (2010) foram: tempo operatório médio de 300 minutos (variando de 180 a 720 minutos); a reconstrução do trânsito intestinal foi alcançado em 93% dos casos; a fístula anastomótica ocorreu em 7% e a infecção de sítio cirúrgico em 22%. A taxa de mortalidade, neste estudo foi de 3,4% ocorrendo principalmente por sepse abdominal ocasionada pela fístula. Dentre os fatores relacionados ao insucesso na reconstrução da colostomia a Hartmann observou-se associação significativa com a tentativa prévia de reconstrução (p = 0,007), a utilização prévia de quimioterapia (p = 0,037) e o longo tempo de permanência da colostomia (p = 0,025).
Referências: Fonseca et al. ABCD, 2017. & Silva et al. ABCD, 2010.
VEJA AQUI ONDE FAZER UMA AVALIAÇÃO ESPECIALIZADA E RECEBER UMA SEGUNDA OPINIÃO
Mais informações: Associação Brasileira de Apoio aos Ostomizados
Eventos Adversos na Clínica Cirúrgica
EVENTOS ADVERSOS # COMPLICAÇÕES

Introdução
O termo “Evento Adverso (EA)” cirúrgico é relativamente novo, mas o conceito de monitoramento dos resultados cirúrgicos, incluindo complicações pós-operatórias, é muito antigo. Desde 1732, existem referências a sistemas de coleta de informações hospitalares. Na Grã-Bretanha, estatísticas vitais datam de 1838, e já em 1850, a associação entre higiene das mãos e a transmissão de infecções foi estabelecida. Em 1854, os riscos de má higiene nos hospitais foram destacados, e em 1910, Ernest Codman defendeu a avaliação rotineira dos resultados negativos em cirurgias para melhorar a qualidade da assistência. Nos anos 1990, o interesse em erros e danos relacionados à saúde cresceu, mudando o foco das pesquisas para estratégias de enfrentamento e uma abordagem sistêmica ou organizacional.
Epidemiologia
Os EAs cirúrgicos contribuem significativamente para a morbidade pós-operatória, e sua avaliação e monitoramento frequentemente são imprecisos. Com a redução do tempo de permanência hospitalar e o aumento do uso de técnicas cirúrgicas inovadoras, especialmente minimamente invasivas e endoscópicas, a eficiência no monitoramento dos eventos adversos torna-se crucial. Revisões recentes identificaram que os EAs são desfavoráveis, indesejáveis, prejudiciais, impactam o paciente e estão associados ao processo de assistência à saúde, mais do que a um processo natural de doenças. A análise dos EAs é complexa devido à variabilidade dos sistemas de registro e às diversas definições na literatura científica para complicações pós-operatórias.
Custo e Efeitos de Medicina Legal
As complicações pós-operatórias resultam da interação de fatores dependentes do paciente, sua enfermidade e a atenção à saúde recebida. O estudo dos EAs cirúrgicos é relevante pela sua frequência, impacto considerável sobre a saúde dos pacientes e repercussão econômica no gasto social e sanitário. Além disso, os EAs servem como instrumento de avaliação da qualidade da assistência. Eventos adversos evitáveis, suscetíveis a intervenções de prevenção, são de maior interesse para a saúde pública. EAs cirúrgicos estão relacionados a acidentes intra-operatórios, complicações pós-operatórias imediatas ou tardias e ao fracasso da intervenção cirúrgica.
Nos Estados Unidos, um estudo em hospitais de Colorado e Utah calculou uma taxa de incidência de 1,9% para pacientes internados, e 3,0% para pacientes submetidos a cirurgia ou parto, com 54% dos EAs considerados evitáveis. Em 5,6% dos casos, os EAs resultaram em óbito. Na Austrália, a prevalência de internações cirúrgicas associadas a um EA foi de 21,9%, com 47,6% dos EAs classificados como altamente evitáveis. Na Espanha, um estudo em cirurgias de parede abdominal encontrou complicações em 16,32% dos pacientes.
Diferença entre Complicação e Evento Adverso
Complicações pós-operatórias surgem da interação entre fatores do paciente, da doença e da atenção recebida. Eventos Adversos, por outro lado, são desfavoráveis, indesejáveis e prejudiciais, resultantes do processo de assistência à saúde. Embora ambos afetem a recuperação, os EAs são frequentemente evitáveis com intervenções preventivas.
Conclusão
A segurança em cirurgia no Brasil é preocupante. Em 2003, 52,5% dos hospitais inspecionados pelo Conselho Regional de Medicina de São Paulo apresentaram condições físicas inadequadas. Hospitais de pequeno porte, que representam 62% dos estabelecimentos, enfrentam desafios significativos em termos de complexidade e densidade tecnológica.
Como Ernest Codman sabiamente afirmou: “A melhoria na assistência médica só pode ser alcançada com a análise sistemática dos resultados”. Esta frase histórica ressoa ainda hoje, destacando a importância da avaliação e monitoramento dos EAs cirúrgicos para a melhoria contínua da qualidade e segurança na assistência à saúde.










