Tumor Markers in HPB Cancers

The “ideal” tumor marker is economical, easy to estimate in easily accessible body fluids like blood or urine, has high sensitivity and specificity, can be used to screen for a cancer, has prognostic and predictive value at diagnosis, and is reliable during treatment and follow-up. It does not exist as of now. Commonly used tumor markers in gastrointestinal, liver, biliary tract, and pancreatic cancers are alpha fetoprotein (AFP), CA19.9, carcinoembryonic antigen (CEA), and chromogranin A (CgA).
Alpha Fetoprotein (AFP)
Alpha fetoprotein (AFP) is a glycoprotein that is produced in the yolk sac and the fetal liver. It is the most commonly used tumor marker for hepatocellular carcinoma (HCC). AFP may be raised in gonadal tumors, gastric cancer, and benign states like pregnancy, viral hepatitis, and cirrhosis caused by hepatitis C. The normal range is 10–20 ng/ml. Values above 400 ng/ml or a steady rise in serial estimation (even if lower than 400 ng/ml) is highly suggestive of HCC in a patient at risk of developing HCC. Persistent elevation of AFP is more significant than fluctuating levels. AFP levels are usually normal in the fibrolamellar variety of HCC. AFP is a heterogeneous molecule with respect to the carbohydrate moiety. Different AFP glycoforms can be separated and characterized by their affinity for lectins. Lectins are carbohydrate-binding proteins.

AFP level >500 ng/ml predicts high recurrence rate after transplantation, and such patients are not listed in the USA. Rise of AFP while on the wait list is also a poor prognostic factor. AFP >1000 ng/ml appears to be related to poor prognostic factors like microvascular invasion, portal vein invasion, bile duct invasion, and intrahepatic metastasis. In 2012 a French paper reported a model that added AFP to Milan criteria which improved prediction of recurrence and survival after liver transplantation for HCC.
CA 19-9
CA 19-9 is the abbreviation for carbohydrate antigen or cancer antigen 19-9. This tumor marker belongs to the family of mucinous markers. These have a transmembrane protein skeleton and an extracellular side that has glycosylated oligosaccharides. It is a sialylated Lewis blood group antigen. Mucus glands in the pancreas, biliary tree, salivary glands, stomach, colon, and endometrium physiologically secrete CA 19-9, and this is present in small quantities in serum. Higher levels are observed in inflammatory conditions of the pancreas and biliary tree like acute pancreatitis, biliary obstruction, and cholangitis. Overall mean sensitivity and specificity of serum CA 19-9 for diagnosis of pancreatic cancer are 81% and 90% according to one recent review. This study reported these results using 37 KU/l as cutoff of CA 19-9. Serum CA 19-9 seems to fare very poorly and is unsuitable as a screening modality for pancreatic cancer.
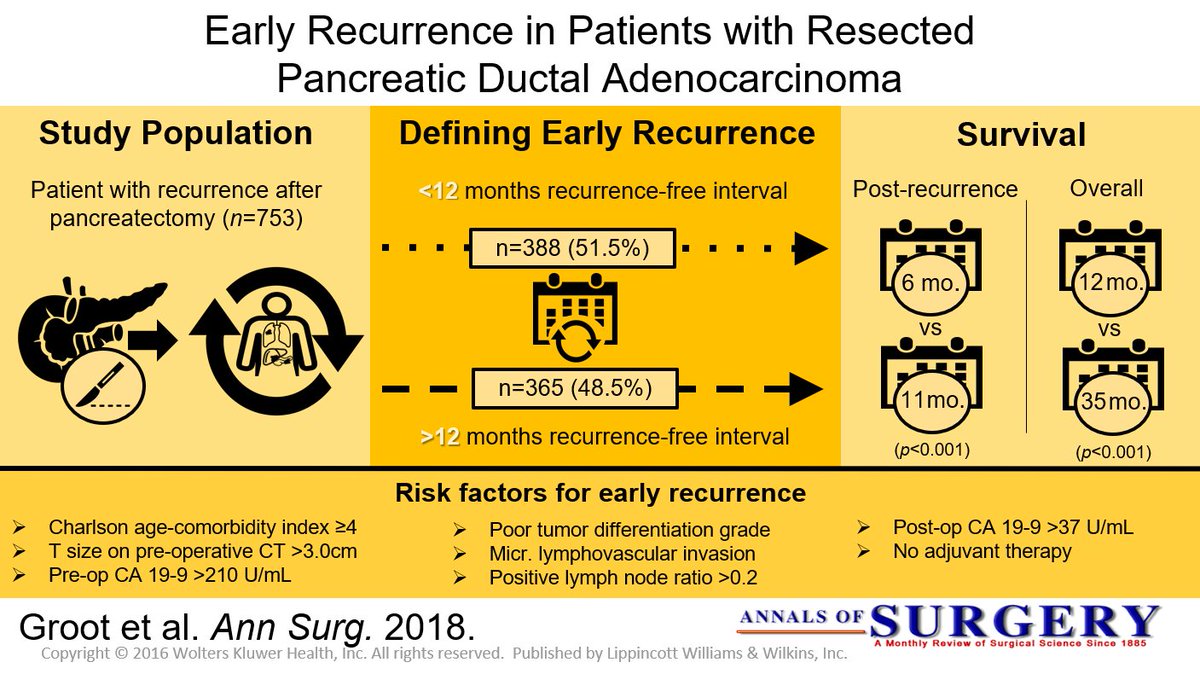
In one of the largest reviews of data, positive predictive value for diagnosis of pancreatic cancer was only 0.9%. Another study from Mumbai used CA 19-9 to predict operability in 49 patients with pancreatic cancer. When CA 19-9 was more than twice the normal (37 U/l), 88% were unresectable. Out of the 29 patients considered resectable after contrast-enhanced CT scan of abdomen, 5 patients were found unresectable at operation due to subcentimeter liver or peritoneal metastasis. All these five patients had CA 19-9 level more than three times the normal limit. These investigators suggest that diagnostic/ staging laparoscopy should be used to avoid a non-therapeutic laparotomy if CA 19-9 is more than thrice the normal limit.
Chromogranin A (CgA)
CgA is an acidic glycoprotein that is ubiquitously present in almost all endocrine and neuroendocrine cells of the human body. They are synthesized in these cells, stored along with other hormones /neurotransmitters in vesicles and released from the cells by exocytosis along with other hormones. The granin family consists of eight different substances of which chromogranin A is the best known and the one in clinical use for several decades now. CgA is thus a universal marker for neuroendocrine cell differentiation and activity. Testing its serum level is a marker of neuroendocrine secretory activity in the body. There are numerous limitations for the use of serum chromogranin A for diagnosis or follow-up of gastroenteropancreatic neuroendocrine tumors (GEP-NETs). However, it still remains the preferred tumor marker in these conditions, as it is widely available and less cumbersome to perform and retains a reasonable sensitivity and specificity provided the clinician applies all necessary recommended precautions in performance of the test and interpretation of the results.

Highest levels of CgA in GEP-NETs are obtained in midgut neuroendocrine tumors, previously termed as “carcinoid tumors.” In ileal carcinoids with liver metastasis, level as high as 200 times upper normal limit is reported. GEP-NETs in MEN-1 syndrome could result in chromogranin A values of about 150 times the upper normal limit. CgA levels in pancreatic NETs are about 60–80 times upper normal limit. CgA is elevated in 100% of gastrinomas and 70% of pancreatic NETs. In gastrinoma, very high levels are reported even in the absence of liver metastasis. CgA level of more than 5000 μg/l was found to be an independent prognostic factor for midgut NETs. Median survival was 33 and 57 months below and above the 5000 μg/l cutoff, respectively. This interpretation of CgA level cannot be generalized to all GEP-NETs. Typical exception of high level without any metastatic disease is gastrinoma as mentioned earlier. CgA level does not correlate with the degree of differentiation of GEP-NETs. Diagnostic accuracy of CgA was 73% in well-differentiated NETs and 50% in poorly differentiated NETs. This is probably related to loss of secretory function of poorly differentiated NETs, where this tumor marker is less reliable. CgA level has been reported to fall after all forms of therapy for GEP-NETs. This could be resection of the tumor, liver transplantation for metastatic disease, radionuclide therapy, or treatment with receptor blockade like everolimus.










