Surgical Management of Cholangiocarcinoma
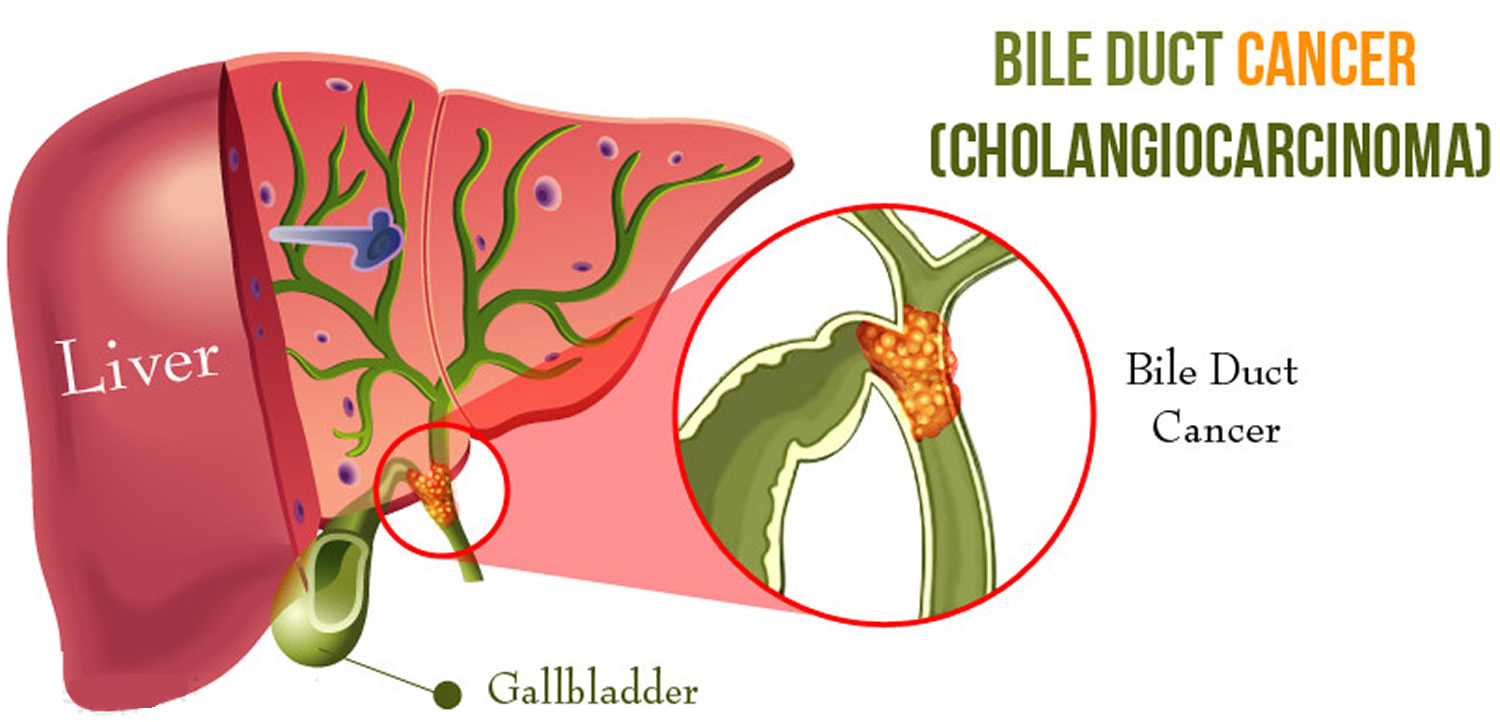
Cholangiocarcinoma (CCA) is a rare but lethal cancer arising from the bile duct epithelium. As a whole, CCA accounts for approximately 3 % of all gastrointestinal cancers. It is an aggressive disease with a high mortality rate. Unfortunately, a significant proportion of patients with CCA present with either unresectable or metastatic disease. In a retrospective review of 225 patients with hilar cholangiocarcinoma, Jarnagin et al. reported that 29 % of patients had either unresectable disease were unfit for surgery. Curative resection offers the best chance for longterm survival. Whereas palliation with surgical bypass was once the preferred surgical procedure even for resectable disease, aggressive surgical resection is now the standard.
Classroom: Surgical Management of Cholangiocarcinoma
Strangulation in GROIN HERNIAS
Importance
Declining Mortality Rates
In both the UK and the USA, the annual death rate due to inguinal and femoral hernias has significantly decreased over the past two to three decades. In the UK, deaths from these hernias declined by 22% to 55% between 1975 and 1990. Similarly, in the USA, the annual deaths per 100,000 population for patients with hernia and intestinal obstruction decreased from 5.1 in 1968 to 3.0 in 1988. For patients with obstructed inguinal hernias, 88% underwent surgery, with a remarkably low mortality rate of 0.05%. These improvements suggest that elective groin hernia surgery has played a crucial role in reducing overall mortality rates.
Elective Surgery and Strangulation Rates
Supporting this observation, the USA has lower rates of strangulation compared to the UK, possibly due to the threefold higher rate of elective hernia surgeries in the USA. Nevertheless, statistics indicate that the rate of elective hernia surgeries in the USA per 100,000 population decreased from 358 to 220 between 1975 and 1990, although this may be an artifact of data collection rather than a genuine decline.
Mortality Analysis from UK and Denmark Studies
During 1991–1992, the UK National Confidential Enquiry Into Perioperative Deaths investigated 210 deaths following inguinal hernia repair and 120 deaths following femoral hernia repair. This inquiry, which focuses on the quality of surgery, anesthesia, and perioperative care, found that many patients were elderly (45 were aged 80–89 years) and significantly infirm; 24 were ASA grade III and 21 ASA grade IV. The majority of postoperative mortality was attributed to preexisting cardiorespiratory issues.
A nationwide study in Denmark of 158 patients who died after acute groin hernia repair by Kjaergaard et al. also found that these patients were old (median age 83 years) and frail (>80% with significant comorbidity), with frequent delays in diagnosis and treatment. These findings highlight the need for high-quality care by experienced surgeons and anesthetists, especially for patients with high ASA grades.
Postoperative Care Recommendations
Postoperative care for these patients should occur in a high-dependency unit or intensive therapy unit. This might necessitate transferring selected patients to appropriate hospitals and facilities. Decisions about interventional surgery should be made in consultation with the relatives of extremely elderly, frail, or moribund patients, adopting a humane approach that may rule out surgery.
Emergency Admissions and Prioritization
Forty percent of patients with femoral hernias are admitted as emergency cases with strangulation or incarceration, while only 3% of patients with direct inguinal hernias present with strangulation. This disparity has implications for prioritizing patients on waiting lists when these hernias present electively in outpatient clinics.
Risk of Strangulation
A groin hernia is at its greatest risk of strangulation within three months of onset. For inguinal hernias, the cumulative probability of strangulation is 2.8% at three months after presentation, rising to 4.5% after two years. The risk is much higher for femoral hernias, with a 22% probability of strangulation at three months, rising to 45% at 21 months. Right-sided hernias have a higher strangulation rate than left-sided hernias, potentially due to anatomical differences in mesenteric attachment. The decline in hernia-related mortality in both the UK and USA underscores the importance of elective hernia surgery. Ensuring timely surgery, especially for high-risk femoral hernias, and providing high-quality perioperative care for elderly and frail patients are crucial steps in further reducing mortality and improving patient outcomes.
Evidence-Based Medicine
In a randomized trial, evaluating an expectative approach to minimally symptomatic inguinal hernias, Fitzgibbons et al. in the group of patients randomized to watchful waiting found a risk of an acute hernia episode of 1.8 in 1,000 patient years. In another trial, O’Dwyer and colleagues, randomizing patients with painless inguinal hernias to observation or operation, found two acute episodes in 80 patients randomized to observation. In both studies, a large percentage of patients randomized to nonoperative care were eventually operated due to symptoms. Neuhauser, who studied a population in Columbia where elective herniorrhaphy was virtually unobtainable, found an annual rate of strangulation of 0.29% for inguinal hernias.
Management of Strangulation
The diagnosis of hernias is primarily based on clinical symptoms and signs, supplemented by imaging studies when necessary. Pain at the hernia site is a constant symptom. In cases of obstruction with intestinal strangulation, patients may present with colicky abdominal pain, distension, vomiting, and constipation. Physical examination may reveal signs of dehydration, with or without central nervous system depression, especially in elderly patients with uremia, along with abdominal signs of intestinal obstruction.
Femoral hernias can be easily missed, particularly in obese women, making a thorough physical examination essential for an accurate diagnosis. However, physical examination alone is often insufficient to confirm the presence of a strangulated femoral hernia versus lymphadenopathy or a lymph node abscess. In such cases, urgent radiographic studies, such as ultrasound or CT scan, may be necessary.
The choice of incision depends on the type of hernia if the diagnosis is clear. When there is doubt, a half Pfannenstiel incision, 2 cm above the pubic ramus extending laterally, provides adequate access to all types of femoral or inguinal hernias. The fundus of the hernia sac is exposed, and an incision is made to assess the viability of its contents. If nonviability is detected, the transverse incision should be converted into a laparotomy incision, followed by the release of the constricting hernia ring, reduction of the sac’s contents, resection, and reanastomosis. Precautions must be taken to avoid contamination of the general peritoneal cavity by gangrenous bowel or intestinal contents.
In most cases, once the constriction of the hernia ring is released, circulation to the intestine is restored, and viability returns. The intestine that initially appears dusky or non-peristaltic may regain color with a short period of warming with damp packs. If viability is doubtful, resection should be performed. Resection rates are highest for femoral or recurrent inguinal hernias and lowest for simple inguinal hernias. Other organs, such as the bladder or omentum, should be resected as needed.
After peritoneal lavage and formal closure of the laparotomy incision, specific repair of the hernia should be performed. Prosthetic mesh should not be used in a contaminated operative field due to the high risk of wound infection. Hernia repair should follow the general principles of elective hernia repair. It is important to remember that in this predominantly frail and elderly patient group with a high postoperative mortality risk, the primary objective of the operation is to stop the vicious cycle of strangulation, with hernia repair being a secondary objective.
Key Point
The risk of an acute groin hernia episode is of particular relevance, when discussing indication for operation of painless or minimally symptomatic hernias. A sensible approach in groin hernias would be, in accordance with the guidelines from the European Hernia Society to advise a male patient, that the risk of an acute operation, with an easily reducible (“disappears when lying down”) inguinal hernia with little or no symptoms, is low and that the indication for operation in this instance is not absolute, but also inform, that usually the hernia after some time will cause symptoms, eventually leading to an operation. In contrast, female patients with a groin hernia, due to the high frequency of femoral hernias and a relatively high risk of acute hernia episodes, should usually be recommended an operation.
Wound Healing
There are many local and systemic factors that affect wound healing. The physician should be actively working to correct any abnormality that can prevent or slow wound healing.
Local Factors
A health care provider can improve wound healing by controlling local factors. He or she must clean the wound, debride it, and close it appropriately. Avulsion or crush wounds below under general management of wounds) need to be debrided until all nonviable tissue is removed. Grossly contaminated wounds should be cleaned as completely as possible to remove particulate matter (foreign bodies) and should be irrigated copiously. Bleeding must be controlled to prevent hematoma formation, which is an excellent medium for bacterial growth. Hematoma also separates wound edges, preventing the proper contact of tissues that is necessary for healing.
Radiation affects local wound healing by causing vasculitis, which leads to local hypoxia and ischemia. Hypoxia and ischemia impede healing by reducing the amount of nutrients and oxygen that are available at the wound site. Infection decreases the rate of wound healing and detrimentally affects proper granulation tissue formation, decreases oxygen delivery, and depletes the wound of needed nutrients. Care must be taken to clean the wound adequately. All wounds have some degree of contamination, if the body is able to control bacterial proliferation in a wound, that wound will heal. The use of cleansing agents (the simplest is soap and water) can help reduce contamination. A wound that contains the highly virulent streptococci species should not be closed. Physicians should keep in mind the potential for Clostridium tetani in wounds with devitalized tissue and use the proper prophylaxis.
Systemic Factors
In addition to controlling local factors, the physician must address systemic issues that can affect wound healing. Nutrition is an extremely important factor in wound healing. Patients need adequate nutrition to support protein synthesis, collagen formation, and metabolic energy for wound healing. Patients need adequate vitamins and nutrients to facilitate healing; folic acid is critical to the proper formation of collagen. Adequate fat intake is required for the absorption of vitamins D, A, K, and E. Vitamin K is essential for the
carboxylation of glutamate in the synthesis of clotting factors II, VII, IX, and X. Decreasing clotting factors can lead to hematoma formation and altered wound healing. Vitamin A increases the inflammatory response, increases collagen synthesis, and increases the influx of macrophages into a wound. Magnesium is required for protein synthesis, and zinc is a cofactor for RNA and DNA polymerase. Lack of any one of these vitamins or trace elements will adversely affect wound healing. Uncontrolled diabetes mellitus results in uncontrolled hyperglycemia, impairs wound healing, and alters collagen
formation. Hyperglycemia also inhibits fibroblast and endothelial cell proliferation within the wound. Medications will also affect wound healing. For example, steroids blunt the inflammatory response, decrease the available vitamin A in the wound, and alter the deposition and remodeling of collagen. Chronic illness (immune deficiency, cancer, uremia, liver disease, and jaundice) will predispose to infection, protein deficiency, and malnutrition, which, as noted previously, can affect wound healing. Smoking has a systemic effect by decreasing the oxygencarrying capacity of hemoglobin. Smoking may also decrease collagen formation within a wound. Hypoxia results in a decrease in oxygen delivery to a wound and retards healing.
Abdominal Surgical Anatomy
The abdomen is the lower part of the trunk below the diaphragm. Its walls surround a large cavity called the abdominal cavity. The abdominal cavity is much more extensive than what it appears from the outside. It extends upward deep to the costal margin up to the diaphragm and downward within the bony pelvis. Thus, a considerable part of the abdominal cavity is overlapped by the lower part of the thoracic cage above and by the bony pelvis below. The abdominal cavity is subdivided by the plane of the pelvic inlet into a larger upper part, i.e., the abdominal cavity proper, and a smaller lower part, i.e., the pelvic cavity. Clinically the importance of the abdomen is manifold. To the physician, the physical examination of the patient is never complete until he/she thoroughly examines the abdomen. To the surgeon, the abdomen remains an enigma because in number of cases the cause of abdominal pain and nature of abdominal lump remains inconclusive even after all possible investigations. To summarize, many branches of medicine such as general surgery and gastroenterology are all confined to the abdomen.
Classroom: Abdominal Surgical Anatomy
Minimally Invasive Approach to Choledocholithiasis
Introduction
The incidence of choledocholithiasis in patients undergoing cholecystectomy is estimated to be 10 %. The presence of common bile duct stones is associated with several known complications including cholangitis, gallstone pancreatitis, obstructive jaundice, and hepatic abscess. Making the diagnosis early and prompt management is crucial. Traditionally, when choledocholithiasis is identified with intraoperative cholangiography during the cholecystectomy, it has been managed surgically by open choledochotomy and place- ment of a T-tube. This open surgical approach has a morbidity rate of 10–15 %, mortality rate of <1 %, with a <6 % incidence of retained stones. Patients who fail endoscopic retrieval of CBD stones, as well as cases in which an endoscopic approach is not appropriate, should be explored surgically.
Clinical Manifestation
Acute obstruction of the bile duct by a stone causes a rapid distension of the biliary tree and activation of local pain fibers. Pain is the most common presenting symptom for choledocholithiasis and is localized to either the right upper quadrant or to the epigastrium. The obstruction will also cause bile stasis which is a risk factor for bacterial over- growth. The bacteria may originate from the duodenum or the stone itself. The combination of biliary obstruction and colo- nization of the biliary tree will lead to the development of fevers, the second most common presenting symptom of cho- ledocholithiasis. Biliary obstruction, if unrelieved, will lead to jaundice. When these three symptoms (pain, fever, and jaundice) are found simultaneously, it is known as Charcot’s triad. This triad suggests the diagnosis of acute ascending cholangitis, a potentially life-threatening condition. If not treated promptly, this can lead to hypotension and decreased metal status, both signs of severe sepsis. When combined with Charcot’s triad, this constellation of symptoms is commonly referred to as Reynolds pentad.
Laparoscopic common bile duct exploration
Laparoscopic common bile duct exploration (LCBDE) allows for single stage treatment of gallstone disease, reducing overall hospital stay, improving safety and cost-effectiveness when compared to the two-stage approach of ERCP and laparoscopic cholecystectomy. Bile duct clearance can be confirmed by direct visualization with a choledochoscope. But, before the advent of choledochoscope, bile duct clearance was uncertain, and blind instrumentation of the duct resulted in accentuated edema and inflammation. Due to advancement in instruments, optical magnification, and direct visualization, laparoscopic exploration of the CBD results in fewer traumas to the bile duct. This has led to an increasing tendency to close the duct primarily, reducing the need for placement of T-tubes. Still, laparoscopic bile duct exploration is being done in only a few centers. Apart from the need for special instruments, there is also a significant learning curve to acquire expertise to be able to perform a laparoscopic bile duct surgery.
Morbidity and mortality rates of laparoscopic exploration are comparable to ERCP (2–17 and 1–5 %), and there is no clear difference in primary success rates between the two approaches. However, the endoscopic approach may be preferable for elderly and frail patients, who are at higher risk with surgery. Patients older than 70–80 years of age have a 4–10 % mortality rate with open duct exploration. It may be as high as 20 % in elderly patients undergoing urgent procedures. In comparison, advanced age and comor- bidities do not have a significant impact on overall complication rates for ERCP. A success rate of over 90 % has been reported with laparoscopic CBD exploration. Availability of surgical expertise and appropriate equipment affect the success rate of laparoscopic exploration, as does the size, number of the CBD stones, as well as biliary anatomy. Over the years, laparoscopic exploration has become efficient, safe, and cost effective. Complications include CBD laceration, stricture formation, bile leak, abscess, pancreatitis, and retained stones.
In cases of failure of laparoscopic CBD exploration, a guidewire or stent can be passed through the cystic duct, common bile duct, and through the ampulla into the duodenum followed by cholecystectomy. This makes the identification and cannulation of the ampulla easier during the post- operative ERCP. Laparoscopic common bile duct exploration is traditionally performed through a transcystic or transductal approach. The transcystic approach is appropriate under certain circumstances. These include a small stone (<10 mm) located in the CBD, presence of small common bile duct (<6 mm), or if there is poor access to the common duct. The transductal approach is preferable in cases of large stones, stones in proximal ducts (hepatic ducts), large occluding stones in a large duct, presence of multiple stones, or if the cystic duct is small (<4 mm) or tortuous. Contraindications for laparoscopic approach include lack of training, and severe inflammation in the porta hepatis making the exploration difficult and risky.
Key Points
With advancement in imaging technology, laparoscopic and endoscopic techniques, management of common bile duct stone has changed drasti- cally in recent years. This has made the treatment of this condition safe and more efficient. Many options are now available to manage this condition, and any particular modality for treatment should be chosen carefully based on the patient related factors, institutional protocol, available expertise, resources, and cost-effectiveness.
Classroom: M.I.A. of Choledocholithiasis
Management of Complicated Appendicitis: Open or Laparoscopic Surgery?
Patients with acute appendicitis can present at different stages of the disease process, ranging from mild mucosal inflammation to frank perforation with abscess formation. The reported overall incidence of acute appendicitis varies with age, gender, and geographical differences. Interestingly, while the incidence of non-perforated appendicitis in the United States decreased between 1970 and 2004, no significant decline in the rate of perforated appendicitis was observed despite the increasng use of computed tomography (CT) and fewer negative appendectomies.
Of 32,683 appendectomies sampled from the American College of Surgeons National Surgical Quality Improvement Program (ACS-NSQIP) hospitals between 2005 and 2008, 5,405 patients (16.5%) had a preoperative diagnosis of acute appendicitis with peritonitis/abscess.
The definition of complicated appendicitis varies slightly in the literature. Clinicopathological diagnoses (gangrenous, perforated, appendiceal abscess/phlegmon) of acute appendicitis are commonly used for its definition. Classically, patients at the extremes of age are more likely to present with complicated appendicitis. Similarly, pre-morbid conditions including diabetes and type of medical insurance are significantly associated with the risk of perforation.
The importance of early appendectomy has also been emphasized to prevent perforation of the appendix and the sub- sequent negative impact on patient outcomes. However, more recent meta-analysis data supports the safety of a relatively short (12–24 h) delay before appendectomy, which was not significantly associated with increased rate of complicated appendicitis. Teixeira et al. also showed that the time to appendectomy was not a significant risk factor for perforated appendicitis but did result in a significantly increased risk of surgical site infection.
The outcome of patients with complicated appendicitis is significantly worse than patients with uncomplicated appendicitis. A population-based study from Sweden showed that, in a risk-adjusted model, patients with perforated appendicitis were 2.34 times more likely to die after appendectomy than non- perforated appendicitis patients. Because of its higher mortality and morbidity in patients with complicated appendicitis, the management of complicated appendicitis has evolved significantly over the last few decades.
Open or Laparoscopic Surgery
Since the first laparoscopic appendectomy was described by Semm in 1983, multiple studies have compared operative time, complication rates, length of hospital stay, hospital cost, and other outcomes between open and laparoscopic appendectomy for acute appendicitis. The most recent Cochrane review included 67 studies showing that laparoscopic appendectomy was associated with a lower incidence of wound infection, reduced postoperative pain, shorter postoperative length of hospital stay, and faster recovery to daily activity. In contrast, reduced risk of intra-abdominal abscesses and shorter operative time were found as the advantages of open appendectomy.
Due to increased surgeon experience in uncomplicated appendicitis, laparoscopic appendectomy is more frequently attempted even in complicated appendicitis cases as an alternative approach to open appendectomy. Although the general surgical steps for complicated appendicitis are similar to those for uncomplicated appendicitis, the laparoscopic procedure can be more technically demanding. Therefore, conversion from laparoscopic appendectomy to open appendectomy can be expected.
Despite these concerns, the laparoscopic approach in patients with com- plicated appendicitis has been proven to be safe and comparable to open appendectomy. Retrospective studies using a large database in the United States uniformly showed more favorable clinical outcomes (mortality, morbidity, length of hospital stay, readmission rate) and hospital costs in patients who underwent laparoscopic appendectomy when compared to open appendectomy. The real risk of developing an intra- abdominal abscess after laparoscopic appendectomy remains unclear. A meta-analysis by Markides et al. found no significant difference in the intra-abdominal abscess rate between laparoscopic and open appendectomy for complicated appendicitis, whereas Ingraham et al. showed a higher likelihood of developing an organ-space surgical site infection in patients undergoing laparoscopic appendectomy.
Non Operative Management of SPLENIC TRAUMA

The spleen, an important component of the reticuloendothelial system in normal adults, is a highly vascular solid organ that arises as a mass of differentiated mesenchymal tissue during early embryonic development. The normal adult spleen weighs between 75 and 100 g and receives an average blood flow of 300 mL/min. It functions as the primary filter of the reticuloendothelial system by sequestering and removing antigens, bacteria, and senescent or damaged cellular elements from the circulation. In addition, the spleen has an important role in humoral immunity because it produces immunoglobulin M and opsonins for the complement activation system.
The increased availability of high-resolution CT scan and advances in arterial angiography and embolization techniques have contributed to the success of nonoperative management of splenic injuries.
The hemodynamically stable patient with blunt splenic trauma can be adequately managed with bed rest, serial abdominal exams, and hemoglobin and hematocrit monitoring. This approach, in combination with occasional angiography, especially for grade III and IV injuries, confers a splenic salvage rate of up to 95%.
In the setting of expectant management, indications for angiography have been delineated by several studies and include the following CT scan features: contrast extravasation, the presence of a pseudoaneurysm, significant hemoperitoneum, high-grade injury, and evidence of a vascular injury. The goal of angiography is to localize bleeding and embolize the source with coils or a gelatin foam product. Embolization can occur either at the main splenic artery just distal to the dorsal pancreatic portion of the vessel—known as proximal embolization—or selectively at the distal branch of the injured vessel. The goal behind the former technique is to decrease the perfusion pressure to the spleen to encourage hemostasis. The disadvantage to this technique is global splenic ischemia, and many have questioned the spleen’s immunocompetence following proximal embolization.
Malhotra et al. examined the effects of angioembolization on splenic function by examining serum levels of a particular T-cell line. T-cell proportions between patients who had undergone splenic embolization with asplenic patients and healthy controls were similar suggesting some degree of splenic immunocompetency was maintained. A Norwegian study comparing blood samples from patients who had undergone angioembolization with healthy controls demonstrated that the study samples had similar levels of pneumococcal immunoglobulins and no Howell-Jolly bodies, suggesting normal splenic function. Although these preliminary studies remain encouraging, there is no definitive evidence that splenic immunocompetency is fully maintained following angio-embolization.
There is no question that advancements in interventional techniques have contributed to the successful nonoperative management of splenic injuries. This has certainly changed the strategy, but it has not completely replaced operative intervention. The challenge now remains predicting those patients who will ultimately require splenectomy.
Many groups have studied potential predictors of nonoperative failure. Earlier studies found that a higher injury grade, increased transfusion requirement, and hypotension on initial presentation consistently predicted failure of nonoperative management. More recent literature reflects the use of advanced imaging techniques for predicting which patients will ultimately require splenectomy. Haan looked at the overall outcomes of patients admitted with blunt splenic trauma and reported several radiographic findings that were prevalent among patients requiring splenectomy after angioembolization:
- contrast extravasation,
- pseudoaneurysm,
- significant hemoperitoneum,
- and arteriovenous fistula.
Among these characteristics, an arteriovenous fistula had the highest rate of nonoperative failure at 40%. Nonradiographic features associated with significant risk of nonoperative failure include age greater than 40, injury severity score of 25 or greater, or presence of large-volume hemoperitoneum.
Aside from radiographic findings, some groups have also examined the mechanism of injury and its association with nonoperative failure. Plurad et al. conducted a retrospective review over a 15-year period and found that patients who were victims of blunt assault were more likely to fail nonoperative management: 36% of these patients required splenectomy versus 11.5% of patients from all other mechanisms combined. These findings suggest that regardless of overall injury severity, individuals who sustain a direct transfer of injury to the left torso are more likely to require splenectomy.
Currently, the accepted standard of care for most splenic trauma is expectant management with close observation. Operative intervention is reserved for the hemodynamically labile patient who shows signs of active hemorrhage and who does not respond appropriately to fluid resuscitation. Although these clinical scenarios seem straightforward, it is often the condition of the patient who falls in between the two ends of the spectrum that can be the most challenging to manage. In the setting of advanced imaging techniques and interventional radiology, the trauma surgeon has more diagnostic information and more treatment options for the patient with splenic trauma.
IPMN Surgical Management

INTRODUCTION
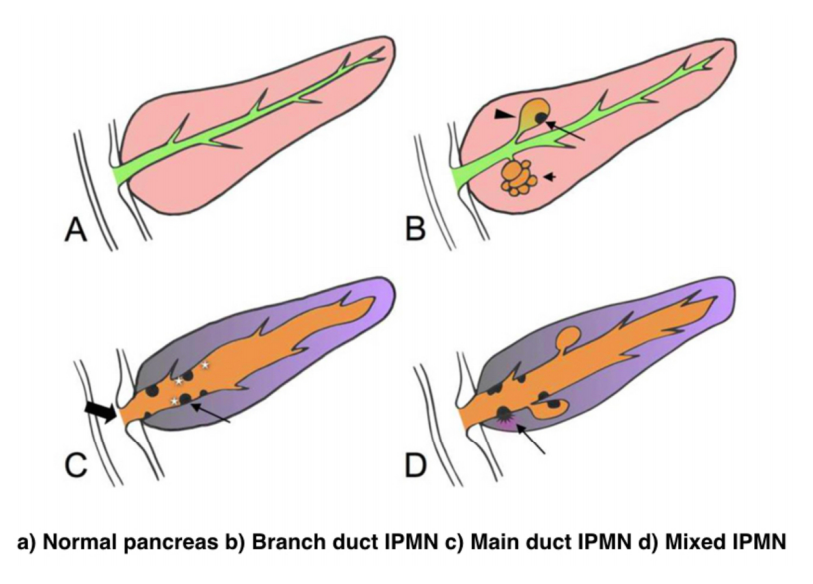
IPMNs were first recognized in 1982 by Ohashi, but the term IPMN was not officially used until 1993. IPMNs are defined in the WHO Classification of Tumors of the Digestive System as an intraductal, grossly visible epithelial neoplasm of mucin-producing cells. Using imaging and histology, IPMNs can be classified into three types based on duct involvement:
1. Main-duct IPMN (approximately 25% of IPMNs): Segmental or diffuse dilation of the main pancreatic duct (>5 mm) in the absence of other causes of ductal obstruction.
2. Branch-duct IPMN (approximately 57% of IPMNs): Pancreatic cysts (>5 mm) that communicate with the main pancreatic duct.
3. Mixed type IPMN (approximately 18% of IPMNs): Meets criteria for both main and branch duct.
Due to the asymptomatic nature of the disease, the overall incidence of IPMNs is difficult to define but is thought to account for approximately 3% to 5% of all pancreatic tumors. Most IPMNs are discovered as incidental lesions from the workup of an unrelated process by imaging or endoscopy. IPMNs are slightly more prevalent in males than in females, with a peak incidence of 60 to 70 years of age. Branch-duct IPMNs tend to occur in a slightly younger population and are less associated with malignancy compared with main-duct or mixed variants.
Because a majority of IPMNs are discovered incidentally, most are asymptomatic. When symptoms do occur, they tend to be nonspecific and include unexplained weight loss, anorexia, abdominal pain, and back pain. Jaundice can occur with mucin obstructing the ampulla or with an underlying invasive carcinoma. The obstruction of the pancreatic duct can also lead to pancreatitis. IPMNs may represent genomic instability of the entire pancreas. This concept, known as a “field defect,” has been described as a theoretical risk of developing a recurrent IPMN or pancreatic adenocarcinoma at a site remote from the original IPMN. The three different types of IPMNs, main duct, branch duct, and mixed duct, dictate different treatment algorithms.
MAIN DUCT IPMNs
Main-duct IPMNs should be resected in all patients unless the risks of existing comorbidities outweigh the benefits of resection. The goal of operative management of IPMNs is to remove all adenomatous or potentially malignant epithelium to minimize recurrence in the pancreas remnant. There are two theories on the pathophysiologic basis of IPMNs. The first groups IPMNs into a similar category as an adenocarcinoma, a localized process involving only a particular segment of the pancreas. The thought is that removal of the IPMN is the only treatment necessary. In contrast, some believe IPMNs to represent a field defect of the pancreas. All of the ductal epithelium remains at risk of malignant degeneration despite removal of the cyst. Ideally, a total pancreatectomy would eliminate all risk, but this is a radical procedure that is associated with metabolic derangements and exocrine insufficiency. Total pancreatectomy should be limited to the most fit patients, with a thorough preoperative assessment and proper risk stratification prior to undertaking this surgery.
There is less uncertainty with treatment of main-duct IPMNs. The high incidence of underlying malignancy associated with the IPMNs warrants surgical resection. IPMNs localized to the body and tail (approximately 33%) can undergo a distal pancreatectomy with splenectomy. At the time of surgery, a frozen section of the proximal margin should be interpreted by a pathologist to rule out high-grade dysplasia. A prospective study identified a concordance rate of 94% between frozen section and final pathologic examination. If the margin is positive (high-grade dysplasia, invasion) additional margins may be resected from the pancreas until no evidence of disease is present. However, most surgeons will proceed to a total pancreatectomy after two subsequent margins demonstrate malignant changes. This more extensive procedure should be discussed with the patient prior to surgery, and the patient should be properly consented regarding the risks of a total pancreatectomy.
IPMNs localized to the head or uncinate process of the pancreas should undergo a pancreaticoduodenectomy. A frozen section of the distal margin should be analyzed by pathology for evidence of disease. As mentioned before, after two additional margins reveal malignant changes, a total pancreatectomy is usually indicated (approximately 5%). The absence of abnormal changes in frozen sections does not equate to negative disease throughout the pancreas remnant. Rather, skip lesions involving the remainder of the pancreas can exist and thus patients ultimately still require imaging surveillance after successful resection. A prophylactic total pancreatectomy is rarely performed because the subsequent pancreatic endocrine (diabetes mellitus) and exocrine deficits (malnutrition) carry an increased morbidity.
BRANCH DUCT IPMNs
Localized branch-duct IPMN can be treated with a formal anatomic pancreatectomy, pancreaticoduodenectomy, or distal pancreatectomy, depending on the location of the lesion. However, guidelines were established that allow for nonoperative management with certain branch- type IPMN characteristics.
These include asymptomatic patients with a cyst size less than 3 cm and lack of mural nodules. The data to support this demonstrate a very low incidence of malignancy (approximately 2%) in this patient group. Which nearly matches the anticipated mortality of undergoing a formal anatomic resection. In approximately 20% to 30% of patients with branch- duct IPMNs, there is evidence of multifocality. The additional IPMNs can be visualized on high-resolution CT or MRI imaging. Ideally, patients with multifocal branch-duct IPMNs should undergo a total pancreatectomy. However, as previously mentioned, the increased morbidity and lifestyle alterations associated with a total pancreatectomy allows for a more conservative approach. This would include removing the most suspicious or dominant of the lesions in an anatomic resection and follow-up imaging surveillance of the remaining pancreas remnant. If subsequent imaging demonstrates malignant charac- teristics, a completion pancreatectomy is usually indicated.
RECURRENCE RATES
Recurrence rates with IPMNs are variable. An anatomic resection of a branch-duct IPMN with negative margins has been shown to be curative. The recurrence of a main- duct IPMN in the remnant gland is anywhere from 0% to 10% if the margins are negative and there is no evidence of invasion. Most case series cite a 5-year survival rate of at least 70% after resection of noninvasive IPMNs. In contrast, evidence of invasive disease, despite negative margins, decreases 5-year survival to 30% to 50%. The recurrence rate in either the pancreatic remnant or distant sites approaches 50% to 90% in these patients. Histopathologic subtype of the IPMN is correlated with survival. The aggressive tubular subtype has a 5-year survival ranging from 37% to 55% following surgical resection, whereas the colloid subtype has 5-year survival ranging from 61% to 87% post resection. Factors associated with decreased survival include tubular subtype, lymph node metastases, vascular invasion, and positive margins. IPMNs with evidence of invasion should be treated similar to pancreatic adenocarcinomas. Studies show that IPMNs tend to have better survival than pancreatic adenocarcinoma. This survival benefit may be secondary to the less aggressive tumor biology or the earlier diagnosis of IPMNs.
SURVEILLANCE
All patients who have a resected IPMN should undergo imaging surveillance. There is continual survival benefit with further resection if an IPMN does recur. International Consensus Guidelines published in 2017 offer recom- mendations for the frequency and modality of imaging surveillance after resection. Routine serum measurement of CEA and CA 19-9 has a limited role for detection of an IPMN recurrence. Of note, a new pancreatic lesion discovered on imaging after resection could represent a postoperative pseudocyst, a recurrence of the IPMN from inadequate resection, a new IPMN, or an unrelated new neoplastic process. IPMNs may also be associated with extrapancreatic neoplasms (stomach, colon, rectum, lung, breast) and pancreatic ductal adenocarcinoma. It is unclear if this represents a true genetic syndrome. However, patients with IPMNs should have a discussion about the implications of their disease with their physician and are encouraged to undergo colonoscopy to exclude a synchronous neoplastic process.
The incidence of PANCREATIC CYSTIC LESIONS will continue to increase as imaging technology improves. EUS, cytology, and molecular panels have made differentiating the type of PCN less problematic. The importance of an accurate preoperative diagnosis ensures that operative management is selectively offered to those with high-risk lesions. Management beyond surgery, including adjuvant therapy and surveillance, continue to be active areas of research.
Perioperative Medicine

Surgery and anesthesia profoundly alter the normal physiologic and metabolic states. Estimating the patient’s ability to respond to these stresses in the postoperative period is the task of the preoperative evaluation. Perioperative complications are often the result of failure, in the preoperative period, to identify underlying medical conditions, maximize the patient’s preoperative health, or accurately assess perioperative risk. Sophisticated laboratory studies and specialized testing are no substitute for a thoughtful and careful history and physical examination. Sophisticated technology has merit primarily in confirming clinical suspicion.
Classroom: Perioperative Medicine
Hepatocellular Carcinoma: Resection Versus Transplantation

Hepatocellular carcinoma is the second most common cause of cancer mortality worldwide and its incidence is rising in North America, with an estimated 35,000 cases in the U.S. in 2014. The best chance for cure is surgical resection in the form of either segmental removal or whole organ transplantation although recent survival data on radiofrequency ablation approximates surgical resection and could be placed under the new moniker of “thermal resection”. The debate between surgical resection and transplantation focuses on patients with “within Milan criteria” tumors, single tumors, and well compensated cirrhosis who can safely undergo either procedure. Although transplantation historically has had better survival outcomes, early diagnosis, reversal of liver disease, and innovations in patient selection and neo-adjuvant therapies have led to similar 5-year survival. Transplantation clearly has less risk of tumor recurrence but exposes recipients to long term immunosuppression and its side effects. Liver transplantation is also limited by the severe global limit on the supply of organ donors whereas resection is readily available. The current data does not favor one treatment over the other for patients with minimal or no portal hypertension and normal synthetic function. Instead, the decision to resect or transplant for HCC relies on multiple factors including tumor characteristics, biology, geography, co-morbidities, location, organ availability, social support and practice preference.
Resection Versus Transplantation
The debate between resection and transplantation revolves around patients who have well compensated cirrhosis with Milan criteria resectable tumors. Patients within these criteria represent a very small proportion of those who initially present with HCC. This is especially true in western countries where hepatitis C is the most common cause of liver failure and HCC is a result of the progressive and in most cases advanced cirrhosis.
Given the need for a large number of patients to show statistical significance, it would be difficult to perform a high-quality prospective randomized controlled trial comparing resection and transplantation. In fact the literature revealed that no randomized controlled trials addressing this issue exist. Instead, outcomes of surgical treatment for HCC stem from retrospective analyses that have inherent detection, selection and attrition biases.
Given the numerous articles available on this subject, several meta-analyses have been published to delineate the role of transplantation and resection for treatment of HCC. However, there is reason to be wary of these meta-analyses because they pool data from heterogeneous populations with variable selection criteria and treatment protocols. One such meta-analysis by Dhir et al. focused their choice of articles to strict criteria which excluded studies with non-cirrhotic patients, fibrolamellar HCC and hepato-cholangiocarcinomas but included those with HCC within Milan criteria and computation of 5-year survival; between 1990 and 2011 they identified ten articles that fit within these criteria, of which six were ITT analyses, six included only well-compensated cirrhotics (Child-Pugh Class A without liver dysfunction) and three were ITT analyses of well-compensated cirrhotics.
Analysis of the six ITT studies that included all cirrhotics (n = 1118) (Child-Pugh Class A through C) showed no significant difference in survival at 5 years (OR = 0.600, 95 % CI 0.291– 1.237 l; p=0.166) but ITT analysis of only well-compensated cirrhotics (Child- Pugh Class A) revealed that patients undergoing transplant had a significantly higher 5-year survival as compared to those with resection (OR=0.521, 95 % CI 0.298–0.911; p=0.022).
A more recent ITT retrospective analysis from Spain assessed long-term survival and tumor recurrence following resection or transplant for tumors <5 cm in 217 cirrhotics (Child-Pugh Class A, B and C) over the span of 16 years. Recurrence at 5 years was significantly higher in the resection group (71.6 % vs. 16 % p<0.001) but survival at 4 years was similar (60 % vs. 62 %) which is likely explained by the evolving role of adjuvant therapies to treat post-resection recurrence.
Conclusions
- Patients with anatomically resectable single tumors and no cirrhosis or Child-Pugh Class A cirrhosis with normal bilirubin, HVPG (<10 mmHg), albumin and INR can be offered resection (evidence quality moderate; strong recommendation).
- Patients with Milan criteria tumors in the setting of Child- Pugh Class A with low platelets and either low albumin or high bilirubin or Child-Pugh Class B and C cirrhosis, especially those with more than one tumor, should be offered liver transplantation over resection (evidence quality moderate; strong recommendation).
- Those with Milan criteria tumors and Child-Pugh Class A cirrhosis without liver dysfunction should be considered for transplantation over resection (evidence quality low; weak recommendation).
- No recommendation can be made in regard to transplanting tumors beyond Milan criteria (evidence quality low) except to follow regional review board criteria.
- Pre-transplant therapies such as embolic or thermal ablation are safe and by expert opinion considered to be effective in decreasing transplant waitlist dropout and bridging patients to transplant (evidence quality low, weak recommendation). These interventions should be considered for those waiting longer than 6 months (evi- dence quality low, moderate recommendation).
- Living donor liver transplantation is a safe and effective option for treatment of HCC that are within and exceed Milan criteria (evidence quality moderate, weak recommendation).
The century of THE SURGEONS
Surgery is a profession defined by its authority to cure by means of bodily invasion. The brutality and risks of opening a living person’s body have long been apparent, the benefits only slowly and haltingly worked out. Nonetheless, over the past two centuries, surgery has become radically more effective, and its violence substantially reduced — changes that have proved central to the development of mankind’s abilities to heal the sick.
Consider, for instance, amputation of the leg.
The procedure had long been recognized as lifesaving, in particular for compound fractures and other wounds prone to sepsis, and at the same time horrific. Before the discovery of anesthesia, orderlies pinned the patient down while an assistant exerted pressure on the femoral artery or applied a tourniquet on the upper thigh.
Surgeons using the circular method proceeded through the limb in layers, taking a long curved knife in a circle through the skin first, then, a few inches higher up, through the muscle, and finally, with the assistant retracting the muscle to expose the bone a few inches higher still, taking an amputation saw smoothly through the bone so as not to leave splintered protrusions. Surgeons using the flap method, popularized by the British surgeon Robert Liston, stabbed through the skin and muscle close to the bone and cut swiftly through at an oblique angle on one side so as to leave a flap covering the stump.
The limits of patients’ tolerance for pain forced surgeons to choose slashing speed over precision. With either the flap method or the circular method, amputation could be accomplished in less than a minute, though the subsequent ligation of the severed blood vessels and suturing of the muscle and skin over the stump sometimes required 20 or 30 minutes when performed by less experienced surgeons.
No matter how swiftly the amputation was performed, however, the suffering that patients experienced was terrible. Few were able to put it into words. Among those who did was Professor George Wilson. In 1843, he underwent a Syme amputation — ankle disarticulation — performed by the great surgeon James Syme himself. Four years later, when opponents of anesthetic agents attempted to dismiss them as “needless luxuries,” Wilson felt obliged to pen a description of his experience:
“The horror of great darkness, and the sense of desertion by God and man, bordering close on despair, which swept through my mind and overwhelmed my heart, I can never forget, however gladly I would do so. During the operation, in spite of the pain it occasioned, my senses were preternaturally acute, as I have been told they generally are in patients in such circumstances. I still recall with unwelcome vividness the spreading out of the instruments: the twisting of the tourniquet: the first incision: the fingering of the sawed bone: the sponge pressed on the flap: the tying of the blood-vessels: the stitching of the skin: the bloody dismembered limb lying on the floor.”
It would take a little while for surgeons to discover that the use of anesthesia allowed them time to be meticulous. Despite the advantages of anesthesia, Liston, like many other surgeons, proceeded in his usual lightning-quick and bloody way. Spectators in the operating-theater gallery would still get out their pocket watches to time him. The butler’s operation, for instance, took an astonishing 25 seconds from incision to wound closure. (Liston operated so fast that he once accidentally amputated an assistant’s fingers along with a patient’s leg, according to Hollingham. The patient and the assistant both died of sepsis, and a spectator reportedly died of shock, resulting in the only known procedure with a 300% mortality.)
How to Choose a Mesh in Hernia Repair

Since the introduction of polypropylene (PP) mesh for hernia repair, surgeons continue to discuss the use of mesh in a variety of settings for one of the most common operations performed by general surgeons—hernia repair. This discussion has involved raw materials, cost, and outcomes and for many years referred to only a few products, as manufacturing was limited. Nowadays, with multiple permanent, absorbable, biologic, and hybrid products on the market, the choice of mesh for a hernia repair can be daunting. Increasing clinical complexity further emphasizes the need for individualizing care, but more frequently, hospital supply chain personnel institute product procurement procedures for cost control, limiting mesh choice for surgeons. This can force surgeons into a “one-size-fits-all” practice regarding mesh choice, which may not be ideal for some patients. Conversely, current literature lacks definitive evidence supporting the use of one mesh over another, a fact that has not escaped the radar screen of the hospital supply chain and mesh industry, both of which attempt to limit vendor and mesh choice for financial gain. It is unlikely that this type of “proof” will ever come to fruition. This leaves us with choosing a mesh based on an algorithm that is centered on the patient and the patient’s unique clinical scenario.
Article: Mesh in Hernia Repair
The Surgical Personality

Surgical stereotypes are remnants of the days of pre-anaesthesia surgery and include impulsivity, narcissism, authoritativeness, decisiveness, and thinking hierarchically. Medical students hold these stereotypes of surgeons early in their medical training. As Pearl Katz says in the The Scalpel’s Edge: ‘Each generation perpetuates the culture and passes it on by recruiting surgical residents who appear to resemble them and training these residents to emulate their thinking and behaviour.’ The culture of surgery has evolved, and certain behaviours are rightly no longer seen as acceptable, Non-technical skills such as leadership and communication have become incorporated into surgical training. Wen Shen, Associate Professor of Clinical Surgery at University of California San Francisco, argues that this has gone too far: ‘Putting likeability before surgical outcomes is like judging a restaurant by the waiters and ignoring the food,’ I would argue that operative and communication skills are indivisible, An aggressive surgeon is a threat to patient safety if colleagues are frightened to speak up for fear of a colleague shouting or, worse, throwing instruments. Conversely, a flattened hierarchy promotes patient safety.
Read More
Article: The Surgical Personality
The “GOOD” Surgeon
Surgery is an extremely enjoyable, intellectually demanding and satisfying career, and many more people apply to become surgeons each year than there are available places.
Those who are successful have to be ready not just to learn a great deal, but have the right kind of personality for the job.
Is a surgical career right for you?
Read the link…
THE GOOD SURGEON
Modern Concepts of Pancreatic Surgery
 Operations on the gallbladder and bile ducts are among the surgical procedures most commonly performed by general surgeons. In most hospitals, cholecystectomy is the most frequently performed operation within the abdomen. Pancreatic surgery is less frequent , but because of the close relation between the biliary system and the pancreas, knowledge of pancreatic problems is equally essential to the surgeon. Acute and chronic pancreatitis and cancer of the pancreas are often encountered by surgeons, with apparently increasing frequency; their treatment remains difficult and perplexing. This review demonstrates the modern aspects of pancreatic surgery. Good study.
Operations on the gallbladder and bile ducts are among the surgical procedures most commonly performed by general surgeons. In most hospitals, cholecystectomy is the most frequently performed operation within the abdomen. Pancreatic surgery is less frequent , but because of the close relation between the biliary system and the pancreas, knowledge of pancreatic problems is equally essential to the surgeon. Acute and chronic pancreatitis and cancer of the pancreas are often encountered by surgeons, with apparently increasing frequency; their treatment remains difficult and perplexing. This review demonstrates the modern aspects of pancreatic surgery. Good study.
AULA: PRÍNCIPIOS MODERNOS DA CIRURGIA PANCREÁTICA
Palestras e Vídeoaulas
Vejam nos links a seguir algumas de nossas palestras disponíveis para download no Canal do SlideShare e Videoaulas presentes no You Tube.
Postoperative Delirium

Postoperative delirium is recognized as the most common surgical complication in older adults,occurring in 5% to 50% of older patients after an operation. With more than one-third of all inpatient operations in the United States being performed on patients 65 years or older, it is imperative that clinicians caring for surgical patients understand optimal delirium care. Delirium is a serious complication for older adults because an episode of delirium can initiate a cascade of deleterious clinical events, including other major postoperative complications, prolonged hospitalization, loss of functional independence, reduced cognitive function, and death. The annual cost of delirium in the United States is estimated to be $150 billion. Delirium is particularly compelling as a quality improvement target, because it is preventable in up to 40% of patients; therefore, it is an ideal candidate for preventive interventions targeted to improve the outcomes of older adults in the perioperative setting. Delirium diagnosis and treatment are essential components of optimal surgical care of older adults, yet the topic of delirium is under-represented in surgical teaching.
Postoperative Delirium in Older Adults
Surgical treatment of ACUTE PANCREATITIS
Acute pancreatitis is more of a range of diseases than it is a single pathologic entity. Its clinical manifestations range from mild, perhaps even subclinical, symptoms to a life-threatening or life-ending process. The classification of acute pancreatitis and its forms are discussed in fuller detail by Sarr and colleagues elsewhere in this issue. For the purposes of this discussion, the focus is on the operative interventions for acute pancreatitis and its attendant disorders. The most important thing to consider when contemplating operative management for acute pancreatitis is that we do not operate as much for the acute inflammatory process as for the complications that may arise from inflammation of the pancreas. In brieSurgical treatment of acute pancreatitisf, the complications are related to: necrosis of the parenchyma, infection of the pancreas or surrounding tissue, failure of pancreatic juice to safely find its way to the lumen of the alimentary tract, erosion into vascular or other structures, and a persistent systemic inflammatory state. The operations may be divided into three major categories: those designed to ameliorate the emergent problems associated with the ongoing inflammatory state, those designed to ameliorate chronic sequelae of an inflammatory event, and those designed to prevent a subsequent episode of acute pancreatitis. This article provides a review of the above.
SURGICAL TREATMENT OF ACUTE PANCREATITIS
O TEMPLO DO CIRURGIÃO.

BLOCO CIRÚRGICO: O TEMPLO DO CIRURGIÃO.
Templo (do latim templum, “local sagrado”) é uma estrutura arquitetônica dedicada ao serviço religioso. O termo também pode ser usado em sentido figurado. Neste sentido, é o reflexo do mundo divino, a habitação de Deus sobre a terra, o lugar da Presença Real. É o resumo do macrocosmo e também a imagem do microcosmo: ‘o corpo é o templo do Espírito Santo’ (I, Coríntios, 6, 19).
Dos locais especiais, O corpo humano (morada da alma), a Cavidade Peritoneal e o Bloco Cirúrgico, se bem analisados, são muito semelhantes e merecem atitudes e comportamentos respeitáveis. O Templo, em todos os credos, induz à meditação, absoluto silêncio tentando ouvir o Ser Supremo. A cavidade peritoneal | abdominal , espaço imaculado da homeostase, quando injuriada, reage gritando em dor, implorando uma precoce e efetiva ação terapêutica.
O Bloco Cirúrgico, abrigo momentâneo do indivíduo solitário, que mudo e quase morto de medo, recorre à prece implorando a troca do acidente, da complicação, da recorrência, da seqüela, da mutilação, da iatrogenia e do risco de óbito pela agressiva e controlada intervenção que lhe restaure a saúde, patrimônio magno de todo ser vivo.
O Bloco Cirúrgico clama por respeito ao paciente cirúrgico, antes mesmo de ser tomado por local banal, misturando condutas vulgares, atitudes menores, desvio de comportamento e propósitos secundários. Trabalhar no Bloco Cirúrgico significa buscar a perfeição técnica, revivendo os ensinamentos de William Stewart Halsted , precursor da arte de operar, dissecando para facilitar, pinçando e ligando um vaso sangüíneo, removendo tecido macerado, evitando corpos estranhos e reduzindo espaço vazio, numa síntese feita com a ansiedade e vontade da primeira e a necessidade e experiência da última.
Mas, se a cirurgia e o cirurgião vêm sofrendo grande evolução, técnica a primeira e científica o segundo, desde o início do século, a imagem que todo doente faz persiste numa simbiose entre mitos e verdades. A cirurgia significa enfrentar ambiente desconhecido chamado “sala de cirurgia” onde a fobia ganha espaço rumo ao infinito. O medo ainda prepondera em muitos.
A confiança neste momento além de um reconhecimento é um troféu que o cirurgião recebe dos pacientes e seus familiares. Tanto a CONFIANÇA quanto a SEGURANÇA têm que ser preservadas a qualquer custo. Não podem correr o risco de serem corroídas por palavras e atitudes de qualquer membro da equipe cirúrgica. Não foi tarefa fácil transformar, para a população, o ato cirúrgico numa atividade científica, indispensável, útil e por demais segura. Da conquista da cirurgia, como excelente arma terapêutica para a manutenção de um alto padrão de qualidade técnica, resta a responsabilidade dos cirurgiões, os herdeiros do suor e sangue, que se iniciou com o trabalho desenvolvido por Billroth, Lister, Halsted, Moyniham, Kocher e uma legião de figuras humanas dignas do maior respeito, admiração e gratidão universal.
No ato operatório os pacientes SÃO TODOS SEMELHANTES EM SUAS DIFERENÇAS, desde a afecção, ao prognóstico, ao caráter da cirurgia e especialmente sua relação com o ato operatório. Logo, o cirurgião tem por dever de ofício entrar no bloco cirúrgico com esperança e não deve sair com dúvida. Nosso trabalho é de equipe, cada um contribui com uma parcela, maior ou menor, para a concretização do todo, do ato cirúrgico por completo, com muita dedicação, profissionalismo e sabedoria. Toda tarefa, da limpeza do chão ao ato de operar, num crescendo, se faz em função de cada um e em benefício da maioria, o mais perfeito possível e de uma só vez, quase sempre sem oportunidade de repetição e previsão de término.
O trabalho do CIRURGIÃO é feito com carinho, muita dignidade, humildade e executado em função da alegria do resultado obtido aliado a dimensão ética do dever cumprido que transcende a sua existência. A vida do cirurgião se materializa no ato operatório e o bloco cirúrgico, palco do nosso trabalho não tolera e jamais permite atitudes menores, inferiores, ambas prejudiciais a todos os pacientes e a cada cirurgião. Como ambiente de trabalho de uma equipe diversificada, precisamos manter, a todo custo, o controle de qualidade, eficiência, eficácia e efetividade técnina associados aos mais altos valores ético, pois lidamos com o que há de mais precioso da criação divina na Terra: O SER HUMANO.
“Tem presença de Deus, como já a tens. Ontem estive com um doente, um doente a quem quero com todo o meu coração de Pai, e compreendo o grande trabalho sacerdotal que os médicos levam a cabo. Mas não se ponham orgulhosos, porque todas as almas são sacerdotais. Devem pôr em prática esse sacerdócio! Ao lavares as mãos, ao vestires a bata, ao calçares as luvas, pensa em Deus, e pensa nesse sacerdócio real de que fala São Pedro, e então não se te meterá a rotina: farás bem aos corpos e às almas” São Josemaria Escriva
Bariatric Complications

Over the past decade, following the publication of several long-term outcome studies that showed a significant improvement in cardiovascular risk and mortality after bariatric surgery, the number of bariatric procedures being carried out annually in the UK has grown exponentially. Surgery remains the only way to produce significant, sustainable weight loss and resolution of comorbidities. Nevertheless, relatively few surgeons have developed an interest in this field. Most bariatric surgery is now performed in centres staffed by surgeons with a bariatric interest, usually as part of a multidisciplinary team.
The commonest weight loss procedures performed around the world at present are the gastric band, the gastric bypass and the sleeve gastrectomy. In very obese patients, an alternative operation is the duodenal switch, while the new ileal transposition procedure represents one of the few purely metabolic operations designed specifically for the treatment of type II diabetes. Older operations such as vertical banded gastroplasty and jejuno-ileal bypass are now obsolete, although patients who have undergone such procedures in the distant past may still present to hospital with complications. The main endoscopic option at present is insertion of a gastric balloon, with newer procedures like the endoscopic duodenojejunal barrier and gastric plication on the horizon. Implantable neuroregulatory devices (gastric ‘pacemakers’) represent a new direction for surgical weight control by harnessing neural feedback signals to help control eating.
It should be within the capability of any abdominal surgeon to manage the general complications of bariatric surgery, which include pulmonary atelectasis/pneumonia, intra-abdominal bleeding, anastomotic or staple-line leak with or without abscess formation, deep vein thrombosis (DVT)/pulmonary embolus and superficial wound infections. Patients may be expected to present with malaise, pallor, features of sepsis or obvious wound problems. However, clinical features may be difficult to recognise owing to body habitus. Abdominal distension, tenderness and guarding may be impossible to determine clinically due to the patient’s obesity. Pallor is non-specific. Fever and leucocytosis may be absent. Wound collections may be very deep. These complications in a bariatric patient should be actively sought with appropriate investigations. In particular, it is vital for life-threatening complications such as bleeding, sepsis and bowel obstruction to be recognised promptly and treated appropriately. A persistent tachycardia may be the only sign heralding significant complications and should always be taken seriously. It is useful to classify complications as ‘early’, ‘medium’ and ‘late’ because, from the receiving clinician’s point of view, the differential diagnosis will differ accordingly.
Complications of bariatric surgery presenting to the GENERAL SURGEON
A “PROFISSÃO” CIRÚRGICA
 “A arte de curar vem do coração e da mente mais do que das mãos.” – Hipócrates
“A arte de curar vem do coração e da mente mais do que das mãos.” – Hipócrates

Na complexa tapeçaria da sociedade moderna, as profissões desempenham papéis fundamentais na organização dos serviços necessários ao bem-estar coletivo. Definida pelo American College of Surgeons, uma profissão é um campo onde a maestria de um corpo complexo de conhecimento e habilidades é essencial. É uma vocação em que o conhecimento científico ou a prática de uma arte, fundamentada nesse conhecimento, é empregada em benefício dos outros. O compromisso com a competência, a integridade e a moralidade forma a base de um contrato social entre a profissão e a sociedade, que concede à profissão um monopólio sobre o uso de seu conhecimento, considerável autonomia na prática e o privilégio da auto-regulação. Em troca, a profissão deve prestar contas a quem serve e à sociedade como um todo.
Os Elementos Essenciais da Profissão
No cerne de toda profissão estão quatro elementos fundamentais:
- Monopólio do Conhecimento Especializado: Profissionais detêm o direito exclusivo de utilizar conhecimentos e habilidades especializados, o que lhes confere uma posição única na sociedade.
- Autonomia e Auto-Regulação: Em troca deste monopólio, profissionais desfrutam de uma relativa autonomia na prática e são responsáveis pela sua própria regulação.
- Serviço Altruísta: A profissão deve servir tanto indivíduos quanto a sociedade de forma altruísta, colocando o bem-estar do paciente acima de outros interesses.
- Responsabilidade pela Manutenção e Expansão do Conhecimento: Profissionais são responsáveis por atualizar e expandir continuamente seu conhecimento e habilidades.
O Que é Profissionalismo?
Profissionalismo descreve as qualidades cognitivas, morais e colegiais de um profissional. É o conjunto de razões pelas quais um pai se orgulha de dizer que seu filho é um médico e cirurgião. Profissionalismo é mais do que apenas conhecimento técnico; é uma combinação de ética, respeito e dedicação ao ofício e ao paciente.
Por Que Precisamos de um Código de Conduta Profissional?
A confiança é o alicerce da prática cirúrgica. O Código de Conduta Profissional esclarece a relação entre a profissão cirúrgica e a sociedade que serve, frequentemente referido como contrato social. Para os pacientes, o código cristaliza o compromisso da comunidade cirúrgica em relação aos indivíduos e suas comunidades. A confiança é construída, tijolo por tijolo.
O Código de Conduta Profissional
O Código de Conduta Profissional aplica os princípios gerais do profissionalismo à prática cirúrgica e serve como a fundação sobre a qual os privilégios profissionais e a confiança dos pacientes e do público são conquistados. Durante o cuidado pré-operatório, intraoperatório e pós-operatório, os cirurgiões têm a responsabilidade de:
- Advogar Eficazmente pelos interesses dos pacientes.
- Divulgar Opções Terapêuticas incluindo seus riscos e benefícios.
- Divulgar e Resolver Conflitos de Interesse que possam influenciar as decisões de cuidado.
- Ser Sensível e Respeitoso com os pacientes, compreendendo sua vulnerabilidade durante o período perioperatório.
- Divulgar Completamente Eventos Adversos e Erros Médicos.
- Reconhecer Necessidades Psicológicas, Sociais, Culturais e Espirituais dos pacientes.
- Incorporar Cuidados Especiais para Pacientes Terminais.
- Reconhecer e Apoiar as Necessidades das Famílias dos Pacientes.
- Respeitar o Conhecimento, Dignidade e Perspectiva de outros profissionais de saúde.
A Necessidade do Código de Profissionalismo para Cirurgiões
Procedimentos cirúrgicos são experiências extremas que impactam os pacientes fisiológica, psicológica e socialmente. Quando os pacientes se submetem a uma experiência cirúrgica, devem confiar que o cirurgião colocará seu bem-estar acima de todas as outras considerações. O código escrito ajuda a reforçar esses valores, garantindo que a confiança e o compromisso sejam mantidos.
Princípios Fundamentais do Código de Conduta Profissional
- Primazia do Bem-Estar do Paciente: Os interesses do paciente sempre devem vir em primeiro lugar. O altruísmo é central para esse conceito, e é o altruísmo do cirurgião que fomenta a confiança na relação médico-paciente.
- Autonomia do Paciente: Pacientes devem entender e tomar suas próprias decisões informadas sobre o tratamento. Os médicos devem ser honestos para que os pacientes façam escolhas educadas, garantindo que essas decisões estejam alinhadas com práticas éticas.
- Justiça Social: Como médicos, devemos advogar pelos pacientes individuais enquanto promovemos a saúde do sistema de saúde como um todo. Precisamos equilibrar as necessidades dos pacientes (autonomia) sem desviar recursos escassos que beneficiariam a sociedade (justiça social).
“Não há maior coisa a ser conquistada do que a confiança dos pacientes e da sociedade, pois ela é a base sobre a qual construímos nossas práticas e nossa profissão.” – William Osler
Metabolismo Perioperatório

A melhor forma de se conhecer as necessidades energéticas é através de sua medida por calorimetria indireta, cada vez mais disponível em nosso ambiente hospitalar. Quando não se dispõe de calorimetria indireta, é possível estimar o gasto energético por meio de fórmulas estimativas que levam em conta, entre outros fatores, o peso e altura corpóreos, idade e sexo. Das diferentes fórmulas disponíveis, a equação de Harris-Benedict tem sido muito usada. Para homens a formula é 66,5 + (13.8 x peso [kg])+(5,0 x altura [cm]) – (6,8 x idade [anos]). Para mulheres a formula é diferente: 655 + (9,6 x peso [kg]) + (1,7 x altura [cm]) – (4,7 x idade [anos]). A regra de bolso (30-35 kcal/kg/dia) é mais prática e também é muito utilizada. No período pré-operatório a oferta de proteína deve ser em torno de 1,0-1,5 g/Kg/dia e, após trauma ou intervenção cirúrgica aumenta, podendo chegar até 2,0 g/Kg/dia. Em pacientes com SIRS moderado, a oferta calórica deve ser menor (25-30 kcal/kg/dia). Pacientes em estresse importante (SIRS grave, sepse) devem receber 20-25 kal/kg/dia e 1,5 a 2,0 g de proteínas/kg/dia. Deve-se evitar em pacientes gravemente desnutridos aporte rápido de calorias e proteínas (síndrome da realimentação). Nesses pacientes a oferta deve ser cautelosa com controle diário de fósforo, magnésio e potássio.
Aula: Suporte Nutricional Perioperatório
Tratamento Cirúrgico da Hemorragia digestiva alta por varizes esofágicas | Hipertensão Porta
Introdução
A hipertensão portal é uma das principais complicações das doenças hepáticas crônicas e representa um dos maiores desafios da cirurgia do aparelho digestivo. Define-se classicamente como um aumento do gradiente de pressão portossistêmico acima de 5 mmHg, sendo clinicamente significativo quando ultrapassa 10–12 mmHg, nível a partir do qual surgem varizes gastroesofágicas e risco de hemorragia digestiva alta.
A cirrose hepática responde por cerca de 90% dos casos de hipertensão portal no mundo, sendo também a principal etiologia no Brasil. Estima-se que aproximadamente 50–60% dos pacientes cirróticos desenvolvem varizes esofágicas, e cerca de 30% destes apresentarão episódio de sangramento varicoso ao longo da vida.
Apesar dos avanços na terapia endoscópica e farmacológica, o tratamento cirúrgico da hipertensão portal permanece uma ferramenta essencial em casos selecionados, particularmente quando ocorre falha terapêutica ou quando há indicações específicas relacionadas à etiologia e à função hepática do paciente.
Neste artigo de educação médica continuada revisaremos os principais aspectos do tratamento cirúrgico da hipertensão portal, com foco em indicações, resultados comparativos entre técnicas e implicações na prática atual da cirurgia digestiva.
ARTIGO DE REVISÃO – HIPERTENSÃO PORTAL
Fisiopatologia da Hipertensão Portal
A hipertensão portal resulta do aumento da resistência ao fluxo portal associado ou não ao aumento do fluxo sanguíneo esplâncnico. Os mecanismos principais incluem:
- Aumento da resistência intra-hepática
- fibrose e distorção arquitetural na cirrose
- compressão sinusoidal
- disfunção endotelial hepática
- Aumento do fluxo portal
- vasodilatação esplâncnica mediada por óxido nítrico
- Formação de circulação colateral portossistêmica
- desenvolvimento de varizes esofagogástricas
- shunts espontâneos
As principais manifestações clínicas incluem:
- hemorragia digestiva alta por varizes
- ascite
- encefalopatia hepática
- hiperesplenismo
O tratamento cirúrgico visa reduzir a pressão portal ou interromper o fluxo varicoso, prevenindo novos episódios hemorrágicos.
Indicações do Tratamento Cirúrgico
Com o advento da ligadura elástica endoscópica, da terapia farmacológica vasoativa e do TIPS, as indicações cirúrgicas tornaram-se mais restritas. Atualmente, as principais indicações incluem:
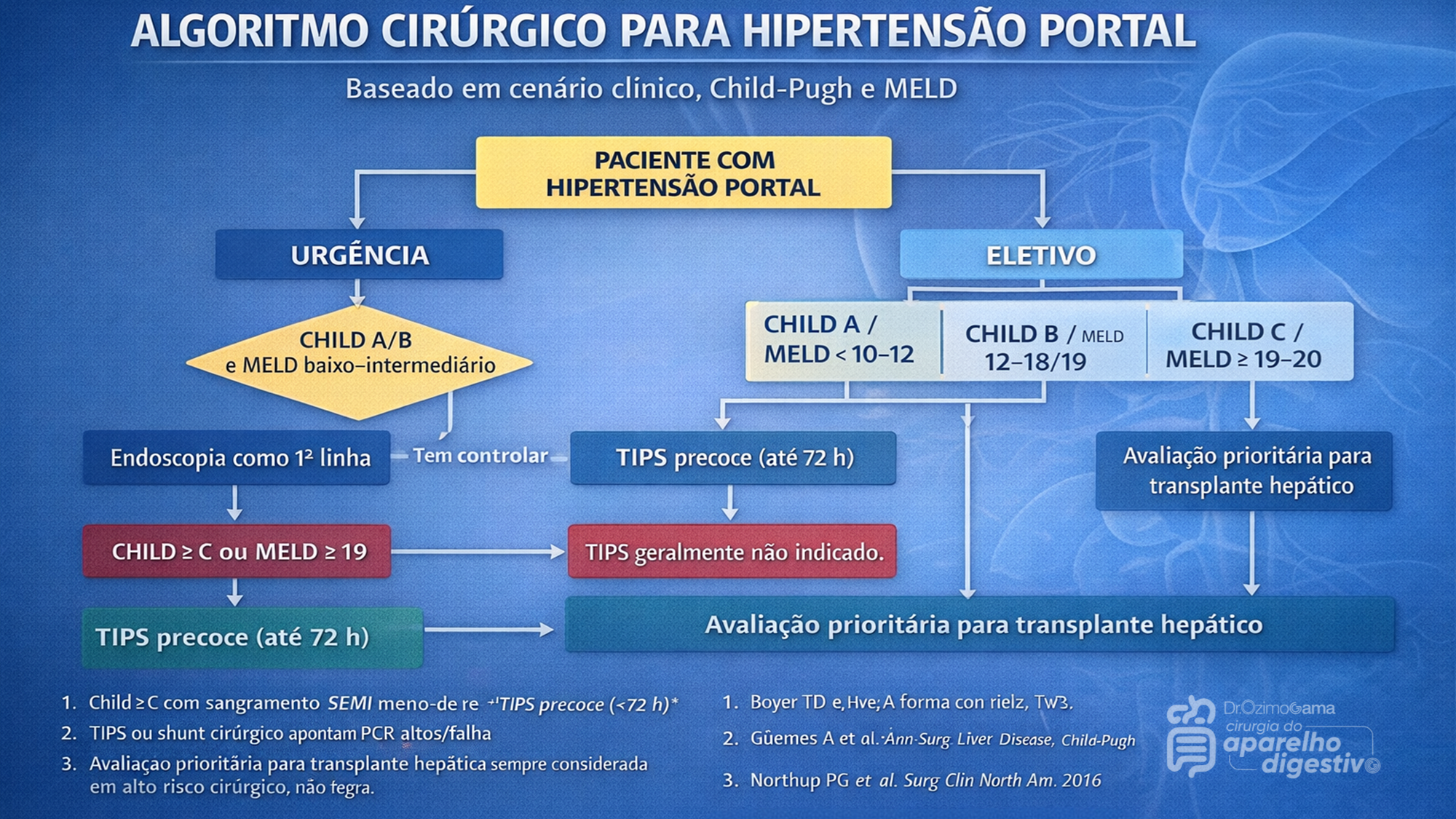
A indicação cirúrgica atual exige a aplicação rigorosa de escores prognósticos, notadamente o Child-Pugh e o MELD. Pacientes Child-Pugh A (MELD < 10 a 15) possuem baixo risco cirúrgico, sendo candidatos ideais para cirurgias eletivas, incluindo shunts e desvascularização. Por outro lado, pacientes descompensados (Child-Pugh C ou MELD > 19-20) apresentam alto risco de mortalidade pós-operatória, inclusive pós-TIPS, sendo o transplante hepático a via mandatória. O grande desafio recai sobre os pacientes limítrofes (Child-Pugh B ou MELD 15-19). Neste estrato de risco intermediário, shunts cirúrgicos tendem a oferecer maior sobrevida a longo prazo para aqueles com função hepática estável, enquanto o TIPS demonstra maior benefício na sobrevida de pacientes com ascite refratária ou sangramento agudo.
AULA: TRATAMENTO CIRÚRGICO DA HIPERTENSÃO PORTAL
Na prática contemporânea da cirurgia hepatobiliar, o manejo da hipertensão portal é multidisciplinar, envolvendo:
- hepatologistas
- endoscopistas
- radiologistas intervencionistas
- cirurgiões digestivos
O algoritmo terapêutico atual pode ser resumido da seguinte forma:
- Primeira linha
- terapia farmacológica
- ligadura elástica endoscópica
- Falha terapêutica
- TIPS
- Pacientes selecionados
- shunt cirúrgico
- desvascularização
- Doença hepática avançada
- transplante hepático
O cirurgião digestivo continua desempenhando papel fundamental, sobretudo em centros terciários e unidades de referência hepatobiliar.
Pontos-chave para o Cirurgião Digestivo
- A hipertensão portal clinicamente significativa ocorre com gradiente >10–12 mmHg
- O sangramento varicoso continua sendo a complicação mais grave
- TIPS é hoje a principal estratégia de resgate após falha endoscópica
- Shunts cirúrgicos permanecem relevantes em pacientes selecionados
- A desvascularização gastroesofágica ainda possui papel importante na esquistossomose
- Transplante hepático é o único tratamento curativo da hipertensão portal associada à cirrose
Conclusão
Embora os avanços na radiologia intervencionista e na endoscopia tenham modificado profundamente o manejo da hipertensão portal, o tratamento cirúrgico permanece indispensável em situações específicas. A seleção adequada do paciente, baseada em função hepática, etiologia da hipertensão portal e recursos disponíveis, continua sendo o fator mais importante para bons resultados. Para o cirurgião digestivo moderno, compreender as diferentes estratégias — desde shunts portossistêmicos até o transplante hepático — é essencial para oferecer um tratamento individualizado e seguro.
PROF. DR. OZIMO GAMA
Gastroenterologia Cirúrgica
“O transplante de fígado e as complexas derivações portais nos ensinaram que não há limites absolutos na cirurgia, apenas fronteiras do conhecimento que aguardam para ser ultrapassadas com dedicação e ciência.” — Thomas Starzl
Gostou ❔Nos deixe um comentário ✍️ , compartilhe em suas redes sociais e|ou mande sua dúvida pelo 💬 Chat On-line em nossa DM do Instagram.
FERIDA PÓS-OPERATÓRIA

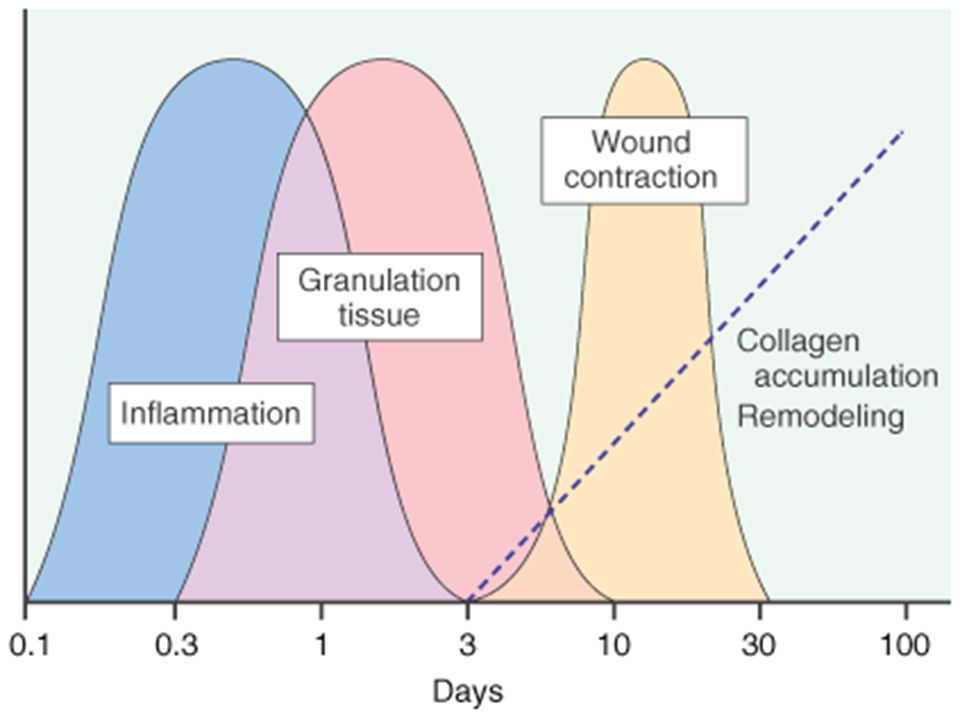
A avaliação e os cuidados de feridas pós-operatórias deve ser do domínio de todos os profissionais que atuam na clínica cirúrgica. O conhecimento a cerca dos processos relacionados a cicatrização tecidual é importante tanto nos cuidados como na prevenção de complicações, tais como: infecções e deiscência. Como tal, todos os profissionais médicos, sendo eles cirurgiões ou de outras especialidades, que participam do manejo clínico dos pacientes no período perioperatório devem apreciar a fisiologia da cicatrização de feridas e os princípios de tratamento de feridas pós-operatório. O objetivo deste artigo é atualizar os profissionais médicos de outras especialidades sobre os aspectos importantes do tratamento de feridas pós-operatório através de uma revisão da fisiologia da cicatrização de feridas, os métodos de limpeza e curativo, bem como um guia sobre complicações de feridas pós-operatórias mais prevalentes e como devem ser manejados nesta situação.
Esophagectomy: Anastomotic Complications (Leakage and Stricture)

Esophagectomy can be used to treat several esophageal diseases; it is most commonly used for treatment of esophageal cancer. Esophagectomy is a major procedure that may result in various complications. This article reviews only the important complications resulting from esophageal resection, which are anastomotic complications after esophageal reconstruction (leakage and stricture), delayed emptying or dumping syndrome, reflux, and chylothorax.
Causas de conversão da VIDEOCOLECISTECTOMIA
Atualmente, a colecistectomia laparoscópica é a abordagem preferida para o tratamento da litíase biliar, representando cerca de 90% dos procedimentos realizados, uma marca alcançada nos Estados Unidos em 1992. A popularidade dessa técnica se deve a suas vantagens evidentes: menos dor no pós-operatório, recuperação mais rápida, redução dos dias de trabalho perdidos e menor tempo de hospitalização. Apesar de ser considerada o padrão-ouro na cirurgia biliar, a colecistectomia laparoscópica não está isenta de desafios. Entre 2% e 15% dos casos podem exigir a conversão para cirurgia convencional. Os motivos mais comuns para essa conversão incluem dificuldades na identificação da anatomia, suspeita de lesão da árvore biliar e controle de sangramentos. Identificar os fatores que contribuem para uma maior taxa de conversão é essencial para a equipe cirúrgica. Isso não apenas permite uma avaliação mais precisa da complexidade do procedimento, mas também ajuda na preparação do paciente para possíveis riscos e na mobilização de cirurgiões mais experientes quando necessário. Em um cenário onde a precisão e a segurança são cruciais, a compreensão dos desafios e a preparação adequada podem fazer toda a diferença no resultado da cirurgia.
Relacionados ao Paciente: 1. Obesidade (IMC > 35), 2. Sexo Masculino, 3. Idade > 65 anos, 4. Diabetes Mellitus e 5. ASA > 2.
Relacionadas a Doença: 1. Colecistite Aguda, 2. Líquido Pericolecístico, 3. Pós – CPRE, 4. Síndrome de Mirizzi e 5. Edema da parede da vesícula > 5 mm.
Relacionadas a Cirurgia: 1. Hemorragia, 2. Aderências firmes, 3. Anatomia obscura, 4. Fístulas internas e 5. Cirurgia abdominal prévia.
POST-HEPATECTOMY ADVERSE EVENTS

Hepatectomia Esquerda – Metástase CR
Hepatic resection had an impressive growth over time. It has been widely performed for the treatment of various liver diseases, such as malignant tumors, benign tumors, calculi in the intrahepatic ducts, hydatid disease, and abscesses. Management of hepatic resection is challenging. Despite technical advances and high experience of liver resection of specialized centers, it is still burdened by relatively high rates of postoperative morbidity and mortality. Especially, complex resections are being increasingly performed in high risk and older patient population. Operation on the liver is especially challenging because of its unique anatomic architecture and because of its vital functions. Common post-hepatectomy complications include venous catheter-related infection, pleural effusion, incisional infection, pulmonary atelectasis or infection, ascites, subphrenic infection, urinary tract infection, intraperitoneal hemorrhage, gastrointestinal tract bleeding, biliary tract hemorrhage, coagulation disorders, bile leakage, and liver failure. These problems are closely related to surgical manipulations, anesthesia, preoperative evaluation and preparation, and postoperative observation and management. The safety profile of hepatectomy probably can be improved if the surgeons and medical staff involved have comprehensive knowledge of the expected complications and expertise in their management.
Classroom: Hepatic Resections
The era of hepatic surgery began with a left lateral hepatic lobectomy performed successfully by Langenbuch in Germany in 1887. Since then, hepatectomy has been widely performed for the treatment of various liver diseases, such as malignant tumors, benign tumors, calculi in the intrahepatic ducts, hydatid disease, and abscesses. Operation on the liver is especially challenging because of its unique anatomic architecture and because of its vital functions. Despite technical advances and high experience of liver resection of specialized centers, it is still burdened by relatively high rates of postoperative morbidity (4.09%-47.7%) and mortality (0.24%-9.7%). This review article focuses on the major postoperative issues after hepatic resection and presents the current management.
REVIEW_ARTICLE_HEPATECTOMY_COMPLICATIONS
PANCREATIC PSEUDOCYST

Classroom: Principles of Pancreatic Surgery
The pancreatic pseudocyst is a collection of pancreatic secretions contained within a fibrous sac comprised of chronic inflammatory cells and fibroblasts in and adjacent to the pancreas contained by surrounding structures. Why a fibrous sac filled with pancreatic fluid is the source of so much interest, speculation, and emotion amongst surgeons and gastroenterologists is indeed hard to understand. Do we debate so vigorously about bilomas, urinomas, or other abdominal collections of visceral secretions? Perhaps it is because the pancreatic pseudocyst represents a sleeping tiger, which though frequently harmless, still can rise up unexpectedly and attack with its enzymatic claws into adjacent visceral and vascular structures and cause lifethreatening complications. Another part of the debate and puzzlement about pancreatic pseudocysts is related to confusion about pancreatic pseudocyst definition and nomenclature. The Atlanta classification, developed in 1992, was a pioneering effort in describing and defining morphologic entities in acute pancreatitis. Since then, a working group has been revising this system to incorporate more modern experience into the terminology. In the latest version of this system, pancreatitis is divided into acute interstitial edematous pancreatitis (IEP) and necrotizing pancreatitis (NP), based on the presence of pancreatic tissue necrosis. The fluid collections associated with these two “types” of pancreatitis are also differentiated. Early (<4 weeks into the disease course) peripancreatic fluid collections in IEP are referred to as acute peripancreatic fluid collections (APFC), whereas in NP, they are referred to as postnecrotic peripancreatic fluid collections (PNPFC). Late (>4 weeks) fluid collections in IEP are called pancreatic pseudocysts, and in NP, they are called walled-off pancreatic necrosis (WOPN).
Review of POSTGASTRECTOMY SYNDROMES

The first postgastrectomy syndrome was noted not long after the first gastrectomy was performed: Billroth reported a case of epigastric pain associated with bilious vomiting as a sequel of gastric surgery in 1885. Several classic treatises exist on the subject; we cannot improve on them and merely provide a few references for the interested reader. Surgical procedures on the stomach, performed for reasons such as peptic ulcer disease, cancer, obesity, or gastroesophageal reflux disease, can result in various post-gastrectomy syndromes. These syndromes include chronic symptoms that range from mild discomfort to life-altering conditions. This guide covers the most common syndromes and their characteristics.
GASTRECTOMY VIDEO SURGERY
Dumping Syndrome
Dumping Syndrome is characterized by gastrointestinal and vasomotor symptoms that occur after food intake due to rapid gastric emptying. This syndrome can occur after surgeries that alter the regulation of gastric emptying or gastric compliance, such as gastrectomy, proximal vagotomy, sleeve gastrectomy, fundoplication, pyloroplasty, and gastrojejunostomy (GJ). Depending on the speed of emptying and the osmolarity of gastric contents, symptoms can vary.
- Early Dumping: Occurs within 30 minutes after food intake and is characterized by palpitations, tachycardia, fatigue, a need to lie down after meals, flushing or pallor, sweating, dizziness, hypotension, headache, and possibly syncope. Abdominal symptoms include early satiety, epigastric fullness, abdominal pain, bloating, hypermotility, and splenic blood pooling.
- Late Dumping: Appears 1 to 3 hours after eating, due to reactive hypoglycemia caused by an initially high glucose load leading to an inappropriately high insulin response. Symptoms include sweating, faintness, difficulty concentrating, and altered levels of consciousness.
Diagnosis is confirmed through an oral glucose tolerance test or a gastric emptying scintigraphy study.
Post-Vagotomy Diarrhea
Post-vagotomy diarrhea is a common complication after vagotomy, characterized by frequent episodes of watery diarrhea. It can be attributed to changes in intestinal motility and bile secretion.
Gastric Stasis
Gastric stasis or delayed gastric emptying can occur due to disruption of normal gastric motility. Symptoms include nausea, vomiting, and a feeling of fullness. Diagnosis is confirmed through gastric emptying studies.
Bile Reflux Gastritis
Bile reflux gastritis is caused by the reflux of bile into the stomach, resulting in epigastric pain and bilious vomiting. Diagnosis can be confirmed through upper endoscopy and gastric pH monitoring.
Afferent and Efferent Loop Syndromes
Afferent loop syndrome occurs after Billroth II reconstruction and is characterized by abdominal pain, bilious vomiting, and distention. Efferent loop syndrome occurs when there is an obstruction of the efferent loop, leading to similar symptoms.
Roux Syndrome
Roux syndrome is a complication of Roux-en-Y procedures, characterized by postprandial abdominal pain and vomiting. Diagnosis is made through a contrast gastrointestinal transit study.
Therapeutic Approach
Management of post-gastrectomy syndromes includes dietary modifications, such as eating small frequent meals, separating liquids and solids, increasing protein and fat intake, and reducing simple sugars. In some cases, additional pharmacological or surgical interventions may be necessary. Understanding these syndromes and their therapeutic approaches is crucial to providing effective care and improving the quality of life for post-gastrectomy patients.
This article focuses on the small proportion of patients with severe, debilitating symptoms; these symptoms can challenge the acumen of the surgeon who is providing the patient’s long-term follow-up and care.
POSTGASTRECTOMY_SYNDROMES_REVIEW_ARTICLE
Complications of HEMORROIDH SURGERY

Symptomatic hemorrhoids require a number of therapeutic interventions each of which has its own complications. Office-based therapy such as rubber band ligation carries the risk of pain and bleeding, which are self-limited, but also carries the risk of rare complications such as sepsis, which may be life threatening. Operative treatment of hemorrhoids includes conventional hemorrhoidectomy, stapled hemorrhoidectomy, and the use of energy devices. Complications of pain and bleeding are common but self-limited. Late complications such as stenosis and fecal incontinence are rare. Recurrent disease is related to the initial grade and therapeutic approach. Treatment of recurrent hemorrhoids should be individualized based on previous treatments and the grade of disease. Anesthetic complications, especially urinary retention, are common and related to the anesthetic technique. Practitioners should council their patients as to the risks of the various approaches to treating symptomatic hemorrhoids.
Intra Abdominal Infections
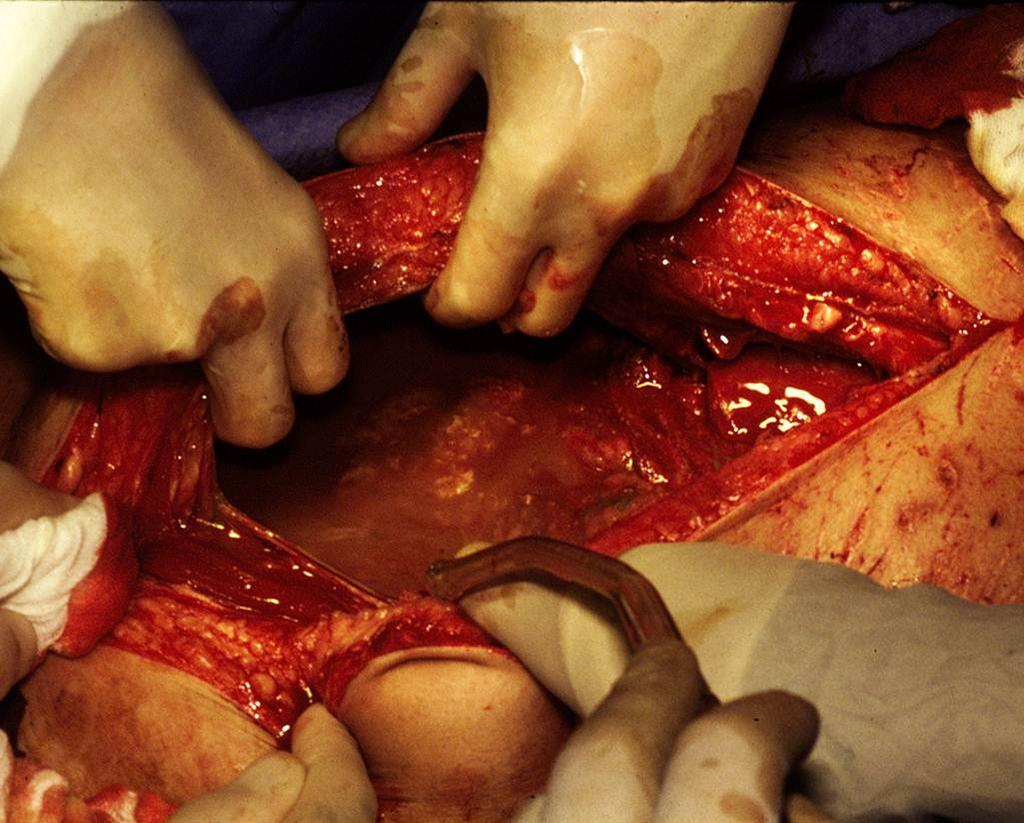
With intra-abdominal infection being one of the most common reasons for surgical consultation, understanding the evaluation and management of these processes becomes paramount in the day- to-day practice of the surgeon. The very broad nature of who is affected coupled with the interplay of patient comorbidities and their medications make dealing with intra-abdominal infections a challenge. As with most complex problems in medicine, it is often useful to break them down into simpler and smaller parts. One useful way to categorize intra-abdominal infections is to divide them into those originating from previous abdominal trauma or operations and those presenting in a “virgin” abdomen.
The latter group most commonly includes those patients presenting with specific organ-based infectious processes such as appendicitis, cholecystitis, or diverticulitis. These individual diseases are covered extensively in other chapters and are discussed only superficially in this chapter. The former are those patients who have sustained intra-abdominal trauma or have undergone previous abdominal interventions and are not recovering in the usual expected course. It is this group that taxes diagnostic and clinical skills and may require the most complex medical decision making.
Several factors should come into play once suspicion for an intra-abdominal infection is entertained. These include resuscitation, antibiotic usage, and source control itself. Patients who present with either a suspected or diagnosed intra-abdominal infection should have some form of volume resuscitation. Even without hypotension, there are several reasons why these patients might be volume depleted. These include nausea and vomiting, fluid sequestration within the abdominal cavity or lumen of the bowel, and poor oral intake. As the process progresses, the patient may develop tachypnea, which results in an evaporative fluid loss. By this time, one can often elicit orthostatic hypotension in most patients.
Fluid resuscitation should begin with the administration of isotonic crystalloid and in general be guided by evidence of end organ perfusion (adequate mental status, urine output, correction of acidosis). There is no utility-using colloid such as albumin or hetastarch in these circumstances, and some data suggest a worse outcome. Should the patient present with hypotension or evidence of poor perfusion, a more aggressive approach to volume resuscitation should be employed. Our recommendation is to follow the current surviving sepsis guidelines, which include fluid challenges, monitoring/assessment of filling pressures, and the potential use of pressors and steroids.
KIDNEY INJURY on perioperative period

ACUTE KIDNEY FAILURE_REVIEW ARTICLE
Alterations in renal function are common after surgical emergencies, trauma, and major operations. In these settings, successful recovery of renal function is dependent on prompt diagnosis and protective management strategies. Acute kidney injury (AKI) is characterized by an acute decrease in glomerular filtration rate (GFR). The true incidence of AKI and acute renal failure (ARF) has been difficult to define, given the broad and various definitions used to quantify and study altered renal function. Relatively recent introduction of consensus definitions, such as RIFLE (risk, failure, loss, and end-stage renal failure) criteria and AKIN (Acute Kidney Injury Network) staging, have provided standard definitions to facilitate more uniform outcome reporting. With use of these definitions, recent studies suggest that AKI occurs in up to two thirds of patients in the intensive care unit (ICU). Moreover, increasing severity of AKI is associated with increasing mortality. AKI is also associated with increased morbidity, such as increased hospital length of stay and cost of care, and has been linked to other in-hospital complications, such as increased difficulty in weaning from mechanical ventilation. Preoperative risk factors for development of AKI include older age, emergent surgery, hepatic disease, obesity, high-risk surgery, vascular disease, and chronic obstructive pulmonary disease (COPD). Prompt recognition of AKI facilitates effective treatment. Although the incidence rate of AKI appears to be rising, overall outcomes from AKI are gradually improving.
The reported mortality rate of AKI is 30% to 60%. If RRT is necessary, reported mortality rates are over 50%. The reason for such high mortality is that AKI now usually occurs as part of a spectrum of multiple organ failure, most often associated with severe sepsis or septic shock. The mortality in this setting is often determined by the underlying septic syndrome, rather than by complications of individual organ failure. Of surviving patients of AKI, a significant number have development of chronic renal insufficiency, which necessitates chronic dialysis. The precise rate of development of chronic renal failure varies greatly in the literature, depending on the patient populations. A recent review of AKI estimates that overall, the risk of necessary chronic dialysis is approximately 12%.
Laparoscopic Surgery for Morbid Obesity
The morbid obesity epidemic continues to spread throughout industrialized nations. It is a condition with a heterogeneous etiology, including genetic, psychosocial, and environmental factors. Prevention methods have currently been unable to halt the further spread of this disease. Obesity has been linked to increased healthcare costs, common physiologic derangements, reduced quality of life, and increased overall mortality. More than one third of adults and almost 17% of children in the United States are obese.
Medical therapy that can cause sustained significant weight loss may be years away. Bariatric surgery, when combined with a multidisciplinary team, continues to be the only proven method to achieve sustained weight loss in most patients. Bariatric procedures modify gastrointestinal anatomy and, in some cases, enteric hormone release to reduce caloric intake, reduce absorption, and alter metabolism to achieve weight loss. Currently, the three most common bariatric operations in the United States are Roux-en-Y gastric bypass, adjustable gastric band, and the vertical sleeve gastrectomy.
GOSSIPIBOMA
O Inimigo Oculto no Bloco Operatório e o Desafio Médico-Legal na Cirurgia Digestiva
Autor: Prof. Dr. Ozimo Gama (Tempo de Leitura: 11 minutos)
Introdução
No vasto e complexo universo da cirurgia do aparelho digestivo, poucos eventos adversos geram tanta perplexidade clínica e devastação médico-legal quanto o “gossipiboma”. O termo deriva do latim Gossypium (algodão) e do swahili boma (esconderijo), designando uma matriz de matéria têxtil envolvida por uma reação de corpo estranho. Também apelidado de “textiloma”, o seu primeiro caso foi descrito por Wilson em 1884. Embora gazes e compressas sejam as ferramentas mais básicas de qualquer laparotomia, o seu esquecimento no interior da cavidade abdominal transforma um material de hemostase num tumor iatrogénico. A incidência real dos gossipibomas é subnotificada — primariamente devido ao estigma e às pesadas implicações legais da sua deteção —, mas representa uma falha catastrófica nos protocolos de segurança do bloco operatório. Para o cirurgião e para toda a equipa, compreender a fisiopatologia, os fatores de risco e, sobretudo, os métodos de prevenção desta entidade é um dever ético inegociável.
Epidemiologia e Fatores de Risco
Estima-se que a retenção de material têxtil ocorra numa frequência de 1 a cada 1.000 a 1.500 operações intra-abdominais. A cavidade abdominal e pélvica é, de longe, o “esconderijo” mais comum devido à sua vasta anatomia e aos recessos profundos.
O gossipiboma não é um mero fruto do acaso; ele prospera no caos. A literatura científica identifica fatores predisponentes cruciais:
- Cirurgia de Emergência: A incidência é nove vezes maior nestes cenários.
- Mudança de Tática Intraoperatória: Alterações não planeadas no decorrer da intervenção elevam o risco em quatro vezes.
- Fatores do Doente e do Ambiente: Doentes com obesidade mórbida, perdas hemáticas maciças que exigem tamponamento rápido, tempo operatório prolongado e, criticamente, a troca de turnos do pessoal médico e de enfermagem (instrumentistas e circulantes) durante o ato cirúrgico.
Fisiopatologia e Evolução Clínica
O relógio biológico do gossipiboma é imprevisível. O tempo entre a operação primária e as manifestações clínicas pode variar de meros 10 dias a várias décadas. A patologia manifesta-se essencialmente através de duas reações orgânicas distintas:
- Resposta Assética Fibrinosa (Crónica): O material têxtil, se permanecer estéril, induz a produção de fibrina, originando aderências e o encapsulamento do corpo estranho (granuloma). O doente pode permanecer completamente assintomático durante anos, ou apresentar queixas inespecíficas e uma massa abdominal palpável que mimetiza uma neoplasia.
- Resposta Exsudativa (Aguda): Ocorre uma infeção secundária severa, culminando na formação de abcessos e fístulas. O material retido tenta encontrar uma via de exteriorização, podendo fistulizar para órgãos internos (estômago, intestino, cólon, bexiga) ou formar uma fístula externa na parede abdominal. Nestes casos, o doente apresenta um quadro florido: dor abdominal, náuseas, vómitos, febre, sépsis, hemorragia digestiva crómica ou síndrome de má absorção.
Diagnóstico, Tratamento e Prognóstico
A ausência de sintomas precoces ou a sua inespecificidade tornam o diagnóstico um autêntico desafio. O cirurgião deve manter um elevado índice de suspeição perante qualquer massa abdominal num doente com história de laparotomia prévia.
- O Padrão-Ouro Diagnóstico: A Tomografia Computorizada (TC) de abdómen é o exame de eleição. A imagem clássica revela uma lesão cística de aspeto “espongiforme” (padrão em miolo de pão), uma cápsula hiperdensa em camadas concêntricas e, ocasionalmente, calcificações murais. A presença de gás no interior da lesão sem evidência de perfuração intestinal é altamente sugestiva.
- Tratamento: A remoção cirúrgica (seja por via laparoscópica em casos altamente selecionados ou laparotomia) é o único tratamento curativo.
- Prognóstico: A excisão atempada é vital para evitar complicações que elevam a taxa de mortalidade para valores inaceitáveis de 11% a 35%. Se a retenção for crónica, a severidade das aderências pode exigir ressecções intestinais extensas e complexas.
Implicações Médico-Legais e Procedimentos Preventivos
O gossipiboma é indiscutivelmente uma falha grave na prestação de cuidados de saúde (malpractice). Do ponto de vista médico-legal, a responsabilidade é frequentemente partilhada entre o cirurgião principal — o “capitão do navio” — e a equipa de enfermagem responsável pela contagem.
A abordagem definitiva é, e sempre será, a Prevenção. A adoção de protocolos rígidos no bloco operatório salva vidas e carreiras:
- Contagem Meticulosa Universal: São mandatárias quatro contagens rigorosas do material cirúrgico: na montagem da mesa, imediatamente antes da incisão, no início do encerramento da aponevrose e durante a síntese da pele.
- Material Radiopaco: O uso exclusivo de compressas e gazes equipadas com filamentos radiopacos é obrigatório.
- Exploração Ativa: Autores como Dhillon e Park reforçam a necessidade primária da exploração manual e visual dos quatro quadrantes abdominais pelo cirurgião no final do procedimento, independentemente de uma contagem de compressas declarada “correta”.
- Conduta Perante Falha na Contagem: Se a contagem final for divergente, a síntese da cavidade não deve ser concluída até que o material seja localizado (a menos que haja instabilidade hemodinâmica crítica). A realização de uma radiografia intraoperatória imediata é mandatária.
Conclusões Aplicadas
O gossipiboma não é uma complicação inerente e aceitável do ato cirúrgico; é uma falha de sistema e de liderança. O aumento aparente da sua incidência exige que os métodos, a comunicação e a disciplina no interior do bloco operatório sejam revistos e aperfeiçoados. Para os jovens cirurgiões e residentes, a mensagem é clara: a cirurgia de excelência não termina na anastomose perfeita, mas sim na verificação obsessiva e no respeito incondicional pelos protocolos de segurança. A verdadeira destreza cirúrgica repousa na humildade de nunca presumir que a cavidade está vazia sem antes a inspecionar exaustivamente.
“A confiança é um sentimento nobre, mas no bloco operatório, a dupla verificação é a única garantia de segurança. Um erro de omissão pode ensombrar o mais brilhante dos procedimentos cirúrgicos.” — Aforismo da Segurança do Doente Cirúrgico.
Gostou ❔Deixe-nos um comentário ✍️ , partilhe nas suas redes sociais e|ou envie a sua dúvida pelo 💬 Chat On-line na nossa DM do Instagram.
Abdominal Hernia Surgical EMERGENCIES

A hernia is a weakness or disruption of the fibromuscular tissues through which an internal organ (or part of the organ) protrudes or slides through. Collectively, inguinal and femoral hernias are often lumped together into groin hernias. Surgery remains the only effective treatment, but the optimal timing and method of repair remain controversial. Although strangulation rates of 3% at 3 months have been reported by some investigators, the largest prospective randomized trial of (watchful waiting) men with minimally symptomatic inguinal hernias showed that watchful waiting is safe. Frequency of strangulation was only 2.4% in patients followed up for as long as 11.5 years. Long-term follow-up shows that more than two-thirds of men using a strategy of watchful waiting cross over to surgical repair, with pain being the most common reasons. This risk of crossover is higher in patients older than 65 years. Once an inguinal hernia becomes symptomatic, surgical repair is clearly indicated. Femoral hernias are more likely to present with strangulation and require emergency surgery and are thus repaired even when asymptomatic. Because this article focuses on incarcerated hernias, nonoperative options are not discussed.
10 Princípios da interação PACIENTE – CIRURGIÃO
Comunicação, Ética e Segurança na Prática Cirúrgica
Autor: Prof. Dr. Ozimo Gama (Tempo de Leitura: 11 minutos)
Introdução
Quando a perspectiva de uma intervenção cirúrgica se impõe — seja para a ressecção de uma neoplasia gástrica, a correção de uma hérnia complexa ou o tratamento metabólico da obesidade —, o medo, a apreensão e a sensação de perda de controle são reações viscerais e universais do ser humano. A visão da dor, o fantasma das complicações e a entrega do próprio corpo ao bisturi de outrem geram uma ansiedade que a mais avançada tecnologia robótica não é capaz de aplacar. No Brasil, onde realizamos milhões de procedimentos cirúrgicos anualmente pelo Sistema Único de Saúde (SUS) e pela Saúde Suplementar, estatísticas dos Conselhos Regionais de Medicina (CRMs) revelam um dado alarmante: mais de 70% das denúncias e processos ético-profissionais por suposto “erro médico” não nascem de falhas técnicas grosseiras, mas da quebra, deterioração ou inexistência de uma relação médico-paciente sólida e transparente. Para o estudante de medicina e o residente de cirurgia, compreender que a destreza manual deve ser precedida pela empatia relacional é o primeiro passo para a maestria.
Os 10 Princípios da Prática Cirúrgica Ética
Para enfrentar os desafios do perioperatório de forma eficaz e blindar a relação terapêutica contra ruídos e frustrações, estruturamos os 10 princípios fundamentais que regem a interação entre o cirurgião e o paciente:
1. Construção da Confiança Mútua
A cirurgia não é um ato comercial; é um pacto de confiança. O cirurgião deve dedicar tempo qualitativo na consulta, evitando o modelo impessoal e apressado (“medicina de linha de montagem”). Um relacionamento humanizado evita que insucessos terapêuticos se transformem em acusações injustas.
2. Clareza e Transparência na Informação
O consentimento deve ser genuinamente esclarecido, não apenas assinado. É imperativo banir o jargão técnico excessivo. Traduzir a fisiopatologia e o plano cirúrgico para uma linguagem acessível reduz o medo do desconhecido e prepara o paciente e seus familiares para o desdobramento natural do pós-operatório.
3. Alinhamento de Expectativas Realistas
Muitas frustrações cirúrgicas nascem do hiato entre a expectativa do paciente e a realidade biológica. É vital discutir os limites da medicina. Prometer “cura absoluta” ou “risco zero” é uma falácia ética.
4. Avaliação Abrangente de Riscos
O Risco Cirúrgico transcende a avaliação cardiológica (Escore de Goldman ou Lee). A avaliação pré-operatória moderna exige uma visão holística: o estado nutricional, a fragilidade (especialmente em idosos), a sarcopenia e, crucialmente, a saúde mental do paciente devem ser exaustivamente investigados.
5. O Papel Estratégico do Anestesiologista
O ato cirúrgico é indissociável do ato anestésico. A escolha da técnica anestésica (bloqueios, anestesia geral, monitorização multimodal) é uma decisão compartilhada. O cirurgião deve fomentar o encontro pré-operatório entre o paciente e a equipe de anestesiologia para dirimir receios e garantir as melhores práticas.
6. Preparação para Mudanças de Rota (O Imprevisto)
O paciente deve entrar no centro cirúrgico ciente de que a tática operatória pode ser alterada. O consentimento para uma laparoscopia deve invariavelmente incluir a possibilidade de conversão para via aberta. Surpresas intraoperatórias (como invasões tumorais insuspeitas) alteram o prognóstico, o tempo de internação e as necessidades de reabilitação.
7. Documentação Exaustiva e Irretocável
O prontuário médico é a testemunha ocular do cuidado. Detalhes das consultas preliminares, opções terapêuticas recusadas pelo paciente e as orientações fornecidas devem estar meticulosamente registrados. Como já abordamos em nosso artigo sobre o método S.O.A.P., documentação é proteção mútua.
8. Descrição Cirúrgica e Rastreabilidade
A descrição do ato operatório deve ser um relato literário da técnica executada. Além disso, a gestão de peças cirúrgicas (envio para exame anatomopatológico) exige rigor logístico. A falha na identificação ou a perda de uma biópsia é uma tragédia diagnóstica inaceitável.
9. Pós-Operatório: Presença e Cuidado Contínuo
O ato cirúrgico não termina no fechamento da pele. O acompanhamento pós-operatório (na UTI, na enfermaria e no ambulatório) exige a presença física e atenciosa do cirurgião principal. Delegar todo o pós-operatório a terceiros é uma das maiores fontes de ressentimento por parte dos pacientes.
10. Atenção ao Estado Emocional
A instabilidade emocional predispõe a uma resposta inflamatória exacerbada e a uma percepção amplificada da dor. Pacientes com ansiedade severa ou depressão pré-existente exigem suporte psicológico ou psiquiátrico adjuvante para garantir resiliência durante a convalescença.
Aplicação na Cirurgia Digestiva
Na cirurgia do aparelho digestivo, estes princípios encontram aplicação diária e visceral:
- Na Cirurgia Bariátrica: O alinhamento de expectativas (Princípio 3) é o alicerce do sucesso. O paciente deve compreender que o bisturi altera a anatomia (Restrição/Incretinas), mas não opera a mente. O reganho de peso é uma possibilidade real se não houver adesão multidisciplinar (Princípio 10).
- Na Cirurgia Oncológica: Informar um paciente sobre a possível necessidade de um estoma (colostomia ou ileostomia) definitivo ou temporário (Princípio 6) exige tato excepcional (Princípio 2). Esconder essa possibilidade para “evitar o sofrimento prévio” destrói a confiança se o paciente acordar com uma bolsa coletora no abdome.
- Na Cirurgia Biliar e Pancreática: Complicações temidas, como a fístula biliar ou pancreática, devem ser discutidas com transparência empática. Quando a complicação ocorre, a presença diária e incansável do cirurgião à beira do leito (Princípio 9) é o que diferencia o abandono do amparo.
Pontos-Chave para a Prática Diária
- Comunicação é Procedimento: Trate a conversa com o paciente e a família com o mesmo rigor técnico que você trata a dissecção de um hilo hepático.
- A Verdade Suportável: Nunca minta, mas adeque a entrega da informação à capacidade de absorção do paciente naquele momento.
- Consentimento Individualizado: Termos de consentimento (TCLE) padronizados e genéricos não possuem força legal. O TCLE deve espelhar as peculiaridades anatômicas e biológicas do paciente específico.
Conclusões Aplicadas
A ética na cirurgia moderna vai imensuravelmente além da destreza técnica, dos nós bem atados e da ausência de complicações infecciosas. Trata-se do respeito à autonomia daquele que se submete à lâmina. A prática cirúrgica de excelência exige que sejamos peritos em fisiologia e mestres em humanidade. O cirurgião do aparelho digestivo que domina estes 10 princípios navega pelas tempestades de uma fístula anastomótica não como um réu diante de um juiz (o paciente), mas como um comandante ao lado de seu companheiro de naufrágio, trabalhando juntos para alcançar a margem segura da cura.
“O bom cirurgião opera com a mão; o cirurgião brilhante opera com o cérebro; mas o cirurgião extraordinário opera com o coração. O bisturi corta tecidos, mas é a compaixão que cicatriza as feridas da alma.” — Adaptado dos princípios humanitários de Sir William Osler, pai da medicina moderna.
Gostou ❔Nos deixe um comentário ✍️ , compartilhe em suas redes sociais e|ou mande sua dúvida pelo 💬 Chat On-line em nossa DM do Instagram.
The General Surgery Job Market

There is a current shortage of general surgeons nationwide. A growing elderly population and ongoing trends toward increased health care use have contributed to a higher demand for surgical services, without a corresponding increase in the supply of surgeons. The number of general surgeons per 100,000 people in the United States declined by 26% from the 1980s to 2005. Cumulative growth in demand for general surgery is projected to exceed 25% by 2025. The Association of American Medical Colleges has projected a shortage of 41,000 general surgeons by 2025. General surgeons make up 33% of the total projected physician shortage, the second highest after primary care physicians, who make up 37% of the total shortage. Despite the demand for general surgeons, the percentage of general surgery trainees going directly into practice is decreasing while the percentage of trainees pursuing subspecialty training is increasing. A recent study reported that graduating residents who lacked confidence in their skills to operate independently were more likely to pursue subspecialty training. This suggests that some graduating residents are motivated to obtain subspecialty training to gain more experience rather than narrow their clinical scope of practice. Given the projected shortage of general surgeons, this will be a crucial distinction when reforming surgical education. General surgery trainees interested in career planning would benefit from understanding the demand for general and/or specialty skills in a job market heavily influenced by a constant stream of new graduates. However, little is currently known about the demand for subspecialty vs general surgical skills in the current job market. The goal of this study was to describe the current job market for general surgeons in the United States, using Oregon and Wisconsin as surrogates. Furthermore, we sought to compare the skills required by the job market with those of graduating trainees with the goal of gaining insight that might assist in workforce planning and surgical education reform.
PRINCIPLES OF OSTOMY MANAGEMENT

The creation of a stoma is a technical exercise. Like most undertakings, if done correctly, the stoma will usually function well with minimal complications for the remainder of the ostomate’s life. Conversely, if created poorly, stoma complications are common and can lead to years of misery. Intestinal stomas are in fact enterocutaneous anastomoses and all the principles that apply to creation of any anastomosis (i.e., using healthy intestine, avoiding ischemia and undue tension) are important in stoma creation.
MOST COMMOM POSTOPERATIVE PROBLEMS

Despite good preoperative assessment, surgical and anaesthetic technique and perioperative management, unexpected symptoms or signs arise after operation that may herald a complication. Detecting these early by regular monitoring and surgical review means early treatment can often forestall major deterioration. Managing problems such as pain, fever or collapse requires correct diagnosis then early treatment. Determining the cause can be challenging, particularly if the patient is anxious, in pain or not fully recovered from anaesthesia. It is vital to see and assess the patient and if necessary, arrange investigations, whatever the hour, when deterio-ration suggests potentially serious but often remediable complications. Consider also whether and when to call for senior help.
Survival Guide for SURGERY ROUND

SURGERY ROUND
Medical students are often attached to the various services. They can provide a significant contribution to patient care. However, their work requires supervision by the surgical intern/resident who takes primary clinical responsibility. Subinterns are senior medical students who are seeking additional clinical experience. Their assistance is needed and appreciated, but again, close supervision of their clinical responsibilities by the intern/resident is mandatory.Outside reading is recommended, including textbooks, reference sources, and monthly journals.Eating is prohibited in patient care areas.Maintain patient confidentiality at all times.At conferences use only patient initials in presentations; and speak carefully and respectfully on work rounds.
PRINCIPLES
1. Always be punctual (this includes ward rounds, operating room, clinics, conferences, morbidity and mortality). Personal appearance is very important. Maintain a high standard including clean shirt and tie (or equivalent) and a clean white coat. The day begins early. Be ready with all the data to start rounds with the senior resident or chief resident. Be sure to provide enough time each morning to examine your patients before rounds.
ABOUT NOTES
2.Aim to get all of your chart notes written as soon as possible; this will greatly increase your effi ciency during the day. Sign and print your name, and include your beeper number, date, and time. Progress notes on patients are required daily. Surgical progress notes should be succinct and accurate, briefl y summarizing the patient’s clinical status and plan of management. Someone unfamiliar with the case should be able to get a good understanding of the patient’s condition from one or two notes. Operative consent is obtained after admitting the patient, performing the history and physical examination, discussing the risks, benefi ts, and alternatives of the procedure(s), and having the patient’s nurse sign the consent with the patient. If you are unaware of the risks and benefi ts of a procedure, discuss this with the service chief resident. Blood transfusion attestation forms need to be signed by the counseling physician before each surgical procedure.
OPERATING ROOM
3. Arrive in the operating room with the patient and before the attending physician or chief resident. Make sure that the charts and all of the relevant x-rays are in the operating room. Make sure that the x-rays are on the x-ray view box prior to the commencement of the case. The intern or resident performing the case should be familiar with the patient’s history and physical exam, current medications, and comorbidities, and be familiar with the principles of the operation prior to arriving in the operating room. Make it a habit to introduce yourself to the patient before the operation. It is mandatory that the surgical resident involved with a case in the operating room attend the start of the case punctually. Scheduled operative cases do not necessarily occur at the listed time. For this reason, it is necessary to check with the operating room front desk frequently. Do not rely on being paged. Conduct in the operating room includes assisting with the preoperative positioning and preparation of the patient; this includes shaving, catheterization, protection of pressure points, and thromboembolism protection. The resident should escort the patient from the operating room to the intensive care unit (ICU) or the postanesthetic care unit with the anesthesiologists. The operating surgeon is responsible for dictating the case. The resident must record all cases performed. For cases admitted to the surgery ICU, a hand-over to the surgery ICU resident is mandatory.This includes discussing all the preoperative assessment, operative details, and postoperative management of the case with the ICU resident.
ROUNDS
4. Signing out to cross-cover services must be performed in a meticulous and careful fashion. All patients should be discussed between the surgical intern and the cross-covering intern to cover all potential problems. A sign-out list containing all the patients, patient locations, and the responsible attendings should be given personally to the cross-cover intern. Any investigations performed at night (e.g., lab studies, chest x-ray, electrocardiogram [ECG]) should be checked that night by the covering intern. No test order should go unchecked. Abnormal lab values should be reviewed and discussed with the senior resident or the attending staff, especially on preoperative patients. Starting antibiotics should be a decision left to the senior resident or attending staff. If consultants are asked to see patients, their recommendations mustbe discussed with your senior resident or attending priorto initiating any new plans. Independent thought is good; independent action is bad.
SUPERVISION
5. Document all procedures performed on patients—including arterial lines, chest tubes, and central lines—with a short procedure note in the chart. Every patient contact should be documented in the patient record.If you see a patient in the middle of the night, write a short note to describe your assessment and plan. Remember, if there is no documentation, then nobody responded to the patient’s complaint or needs. Obtain appropriate supervision for procedures. There are always more senior residents available if your chief is not. Protect yourself; practice universal precautions! Wash your hands before and after examining a patient. Wear gloves. All wounds should be inspected every day by the surgical intern as part of the clinical examination. Please re-dress them; the nursing staff is not always immediately available to do so. There should never be any surprises in the morning.
RESIDENTS
Your senior resident is responsible for the service and should be kept aware of any problems, regardless of the time of day. If the senior resident is not available, the attending staff should be contacted directly. There are always senior residents in the hospital who are available to be used as resources for emergencies. Always be aware of who is in-house (i.e., consult resident, ICU resident, trauma chief). A surgery resident’s days are long. They start early and they fi nish late. Always remember the three A’s to being a successful resident: Affable, Available, and Able. Be prepared to maintain a flexible daily schedule depending on the workload of the service and the requirement for additional manpower.
PREVENTION COMPLICATIONS OF COLON SURGERY
COMPLICATIONS OF COLON SURGERY_REVIEW ARTICLE


Colon surgery represents a high number of patients treated at a department of gastrointestinal surgery and is not limited to colon cancer. It includes other non-neoplastic pathologies such as inflammatory bowel disease, diverticular disease or colonic volvulus. As with any major procedure, colon surgery patients may present serious or even fatal complications. The incidence of postoperative complications from colon surgery has been estimated at between 10% and 30% according to selected series. Preventive measures against surgical complications include selection of an appropriate procedure for the patient as well as good preoperative care, appropriate surgical technique and good postoperative management. When diagnosis has been established, risks for patient should be assessed according to patient’s health conditions and type of surgery accomplished. When the patient meets the surgical requirements, an appropriate course of preoperative care should be carried out including colon wash antibiotics and antithrombotic prophylaxis. Postoperative period will be equivalent to any major abdominal surgery. Typically, it was considered appropriate to wait a few days before initiating feeding in order to protect anastomosis; however, some authors agree that an early oral diet hours after intervention is not associated with a higher risk of anastomotic dehiscence and other complications.
Sleeve Gastrectomy: Complications and Management
SLEEVE GASTRECTOMY COMPLICATIONS_REVIEW ARTICLE
 Obesity is a common disease affecting adults and children. The incidence of obesity in worldwide is increasing. Laparoscopic sleeve gastrectomy (LSG) is a relatively new and effective procedure for weight loss. Owing to an increase in the number of bariatric surgical procedures, general surgeons should have an understanding of the complications associated with LSG and an approach for dealing with them. Early postoperative complications following LSG that need to be identified urgently include bleeding, staple line leak and development of an abscess. Delayed complications include strictures, nutritional deficiencies and gastresophageal reflux disease. We discuss the principles involved in the management of each complication.
Obesity is a common disease affecting adults and children. The incidence of obesity in worldwide is increasing. Laparoscopic sleeve gastrectomy (LSG) is a relatively new and effective procedure for weight loss. Owing to an increase in the number of bariatric surgical procedures, general surgeons should have an understanding of the complications associated with LSG and an approach for dealing with them. Early postoperative complications following LSG that need to be identified urgently include bleeding, staple line leak and development of an abscess. Delayed complications include strictures, nutritional deficiencies and gastresophageal reflux disease. We discuss the principles involved in the management of each complication.
“COMO PODEMOS CURAR A MEDICINA?”
“Nos últimos anos percebemos que estávamos na mais profunda crise da existência da medicina, devido a algo sobre o que você normalmente não pensa quando você é um médico preocupado em fazer o bem para as pessoas, que é o custo do tratamento de saúde. Não há um país no mundo que não esteja perguntando agora se podemos custear o que médicos fazem. A luta política que desenvolvemos tornou-se aquela sobre se o governo é o problema ou se as companhias de seguro são o problema. E a resposta é sim e não; é mais profundo que tudo isso. A causa de nossos problemas é, na verdade, a complexidade que a ciência nos deu. E para entender isso, voltarei algumas gerações…”
PERIOPERATIVE FLUID MANAGEMENT IN SURGERY
REVIEW ARTICLE_FLUID MANAGEMENT IN ELECTIVE SURGERY
The purpose of the thesis was to investigate the pathophysiology and functional outcomes of various fluid administration regimens in elective surgical procedures and describe factors of importance in perioperative fluid management. The goal was to create a rational physiologic background on which to design future ran-domized, clinical trials focusing on clinical outcomes aiming to produce evidence-based guidelines for rational perioperative fluid therapy. The main hypothesis of the thesis was thatthe ”liberal” fluid administration regimens seen in daily clinical practice may be detrimental and contribute to increased perioperative morbid-ity primarily due to increased functional demands of the cardi-opulmonary system and gastrointestinal tract as well as de-creased tissue oxygenation (impaired wound healing).

“CIRURGIA: PASSADO, PRESENTE e FUTURO ROBÓTICO”
A cirurgiã e inventora Catherine Mohr nos guia pela história da cirurgia (e seu passado pré-anestesia e pré-antissepsia), e depois demonstra algumas das mais novas ferramentas para cirurgias realizadas através de pequenas incisões, usando ágeis mãos robóticas.
EARLY COMPLICATIONS IN BARIATRIC SURGERY
REVIEW ARTICLE_BARIATRIC SURGERY COMPLICATIONS
 The risk of complications and mortality in bariatric surgery is associated with certain factors that are common to other patients and procedures, including age above 65 years, the presence of associated diseases (cardiovascular and pulmonary disease, chronic renal failure, liver cirrhosis, etc.), prior abdominal surgery, and the experience of the surgeon and the institution, especially concerning the ability to make an early diagnosis and address complications. The surgical complications observed in the early postoperative period following surgeries performed to treat severe obesity are similar to those associated with other major surgeries of the gastrointestinal tract. However, given the more frequent occurrence of medical comorbidities (such as diabetes, arterial hypertension, and sleep apnea), as well as the difficulty in making an early diagnosis of the complications (due to limitations of the clinical abdominal workup and imaging methods, such as ultrasonography and computed tomography, particularly in highly obese patients with body mass indices >50 kg/m²), these patients require special attention in the early post operative follow-up. Pulmonary thromboembolism, a complication associated with bariatric surgery, also requires greater attention from the medical team given the high mortality rate associated with this condition. Early diagnosis and appropriate treatment of these complications are directly associated with a greater probability of control.
The risk of complications and mortality in bariatric surgery is associated with certain factors that are common to other patients and procedures, including age above 65 years, the presence of associated diseases (cardiovascular and pulmonary disease, chronic renal failure, liver cirrhosis, etc.), prior abdominal surgery, and the experience of the surgeon and the institution, especially concerning the ability to make an early diagnosis and address complications. The surgical complications observed in the early postoperative period following surgeries performed to treat severe obesity are similar to those associated with other major surgeries of the gastrointestinal tract. However, given the more frequent occurrence of medical comorbidities (such as diabetes, arterial hypertension, and sleep apnea), as well as the difficulty in making an early diagnosis of the complications (due to limitations of the clinical abdominal workup and imaging methods, such as ultrasonography and computed tomography, particularly in highly obese patients with body mass indices >50 kg/m²), these patients require special attention in the early post operative follow-up. Pulmonary thromboembolism, a complication associated with bariatric surgery, also requires greater attention from the medical team given the high mortality rate associated with this condition. Early diagnosis and appropriate treatment of these complications are directly associated with a greater probability of control.
Ebook: Princípios da Cirurgia Hepatobiliar

Cirurgia Hepatobiliar
Considera-se que a cirurgia hepática começou após o advento da anestesia e da anti-sepsia. No entanto, muito antes disso, diversos autores já relatavam suas experiências com ressecções do fígado. As primeiras descrições de “cirurgias hepáticas” consistiam no relato de avulsões parciais ou totais de porções do fígado após lesões traumáticas do abdome. O relato de Elliot (1897) exemplifica muito dos temores dos cirurgiões da época: “O fígado (…) é tão friável, tão cheio de vasos e tão evidentemente impossível de ser suturado que parece ser improvável o manejo bem sucedido de grandes lesões de seu parênquima”.
CIRURGIA HEPATOBILIAR_ASPECTOS BÁSICOS
Lymph Node Dissection in Gastric Adenocarcinoma
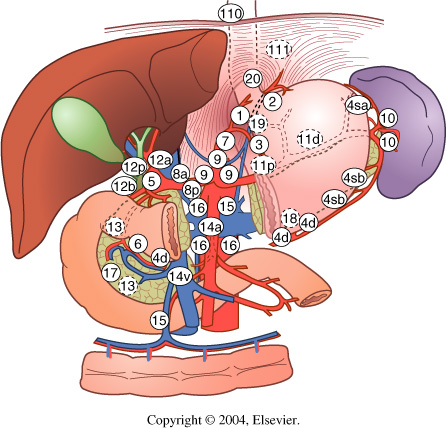
Extent of lymph node dissection has been an area of controversy in gastric adenocarcinoma for many years. Some surgeons believe that cancer metastasizes through a stepwise progression, and an extensive lymphadenectomy is necessary to improve survival and/or cure the patient. Other physicians argue that extensive ly-mphadenectomies only add pe-rioperative morbidity and mor-tality and do not improve survival. Asian countries have been performing extended lymphadenectomies routinely for many years with promising survival data, although Western countries have not been able to reproduce those results. Much of the controversy surrounding lymphadenectomies started in the 1980s when Japanese studies reported superior survival rates matched stage for stage, compared to the United States. This was theorized to be secondary to the more extensive lymphadenectomy performed in Japan compared to the United States.

A United Kingdom study randomized 400 patients to either a D1 or a D2 lymph node dissection. Those patients with tumors in the upper or middle third of the stomach underwent a distal pancreaticosplenectomy to obtain retropancreatic and splenic hilar nodes. While the 5-year survival rates were not statistically significant between the two groups, on multivariate analyses it was noted that those patients in the D2 group that did not undergo the distal pancreaticosplenectomy had an increased survival compared with the D1 group. A trial in the Netherlands randomized 380 gastric cancer patients to a D1 lymphadenectomy and 331 patients to a D2 lymphadenectomy. Similar to the United Kingdom study, there was not a significant difference in survival between the two groups, even when followed out to 11 years. There was a significant increase in postoperative complications in the D2 group compared with the D1 group (43 % vs. 25 %, respectively) as well as mortality (10 % vs. 4 %, respectively).
The data from these two studies suggest that a pancreaticosplenectomy performed to harvest lymph nodes seems to only add morbidity and mortality while not improving survival. One concern raised about the prior two studies was the variation in surgical technique and lack of standardization of surgeon experience. A Taiwanese study accounted for this by performing the study at a single institution with three surgeons, each of whom had completed at least 25 D3 lymph node dissections prior to the study. Patients with gastric cancer were randomized to a D1 lymph node dissection (defined as resection of perigastric lymph nodes along the lesser and greater curves of the stomach) or a D3 lymph node dissection (defined as resection of additional lymph nodes surrounding the splenic, common hepatic, left gastric arteries, nodes in the hepatoduodenal ligament, and retropancreatic lymph nodes). There was an overall 5-year survival benefit with the D3 group of 60 % compared with the D1 group of 54 %. A Japanese study evaluated a more aggressive lymph node dissection and randomized patients to a D2 dissection or a para-aortic lymph node dissection (PAND). There was no significant difference in 5-year survival between the two groups with a trend toward an increase in complications in the PAND group. Multiple studies have shown that the number of positive lymph nodes is a significant predictor of survival. Current AJCC guidelines stipulate that at least 15 lymph nodes are needed for pathologic examination to obtain adequate staging.
Laparoscopic techniques have become an integral part of surgical practice over the past several decades. For gastric cancer, multiple retrospective studies have reported the advantages of laparoscopic gastrectomy (LG) over open gastrectomy (OG). A recent meta-analysis of 15 nonrandomized comparative studies has also shown that although LG had a longer operative time than OG, it was associated with lower intraoperative blood loss, overall complication rate, fewer wound-related complications, quicker recovery of gastrointestinal motility with shorter time to first flatus and oral intake, and shorter hospital stay. A randomized prospective trial comparing laparoscopic assisted with open subtotal gastrectomy reported that LG had a significantly lower blood loss (229 ± 144 ml versus 391 ± 136 ml; P< 0.001), shorter time to resumption of oral intake (5.1 ± 0.5 days versus 7.4 ± 2 days; P< 0.001), and earlier discharge from hospital (10.3 ± 3.6 days versus 14.5 ± 4.6 days; P< 0.001).
Como funciona o GRAMPEADOR INTESTINAL ?
A Busca pela Segurança e Eficiência na Cirurgia Moderna
Introdução O objetivo primordial de qualquer cirurgião, ao iniciar uma intervenção, é garantir que o procedimento seja seguro e eficiente. A “regra de ouro” da cirurgia moderna permanece clara: o ato operatório deve ser o mais breve possível, gerando o menor trauma tecidual e restaurando a função do órgão. O resultado esperado é sempre a minimização das intercorrências no pós-operatório. Embora a cirurgia atual atinja esses objetivos de forma bastante satisfatória, as complicações relacionadas às suturas e à cicatrização ainda são desafios presentes na rotina hospitalar.
A Evolução Histórica e os Desafios da Cicatrização A confiabilidade das suturas gastrointestinais, por exemplo, é uma conquista relativamente recente. Foi apenas no final do século XIX que a compreensão dos princípios básicos da cicatrização tecidual permitiu avanços significativos nesta área. Sabemos hoje que o sucesso do reparo tecidual não depende apenas da técnica empregada, mas é uma equação complexa que envolve o paciente e a área operada. Diversos fatores podem retardar ou prejudicar drasticamente a cicatrização, entre eles:
-
Isquemia (falta de suprimento sanguíneo);
-
Edema (inchaço excessivo);
-
Infecção local ou sistêmica;
-
Desnutrição do paciente.
O Fator Humano e o Surgimento da Tecnologia Existe uma variável crítica na cirurgia: a habilidade manual. Naturalmente, há uma variação na destreza e na técnica entre diferentes cirurgiões. Foi justamente essa disparidade que motivou o desenvolvimento de novos dispositivos cirúrgicos. O objetivo da inovação tecnológica na cirurgia é superar as diferenças individuais, funcionando como um equalizador. Ao utilizar dispositivos que padronizam etapas críticas (como as suturas mecânicas), permite-se que técnicas complexas sejam executadas adequadamente, independente de quem opera.
Conclusão Para que a medicina avance, uma técnica não pode depender apenas do talento de poucos. Ela deve ser reproduzível de forma confiável pelo maior número possível de cirurgiões. Somente através dessa padronização e do auxílio tecnológico é que os resultados cirúrgicos podem ser amplamente adotados, reconhecidos como eficazes e, acima de tudo, seguros para o paciente.