Síndrome de Mirizzi

Abordagem Multimodal e Estratificação Tática no Manejo da Síndrome de Mirizzi
Autor: Prof. Dr. Ozimo Gama
Categoria: Cirurgia Hepatobilipancreática / Emergências Cirúrgicas / Anatomia Aplicada
Tempo de Leitura: 13 minutos
Introdução
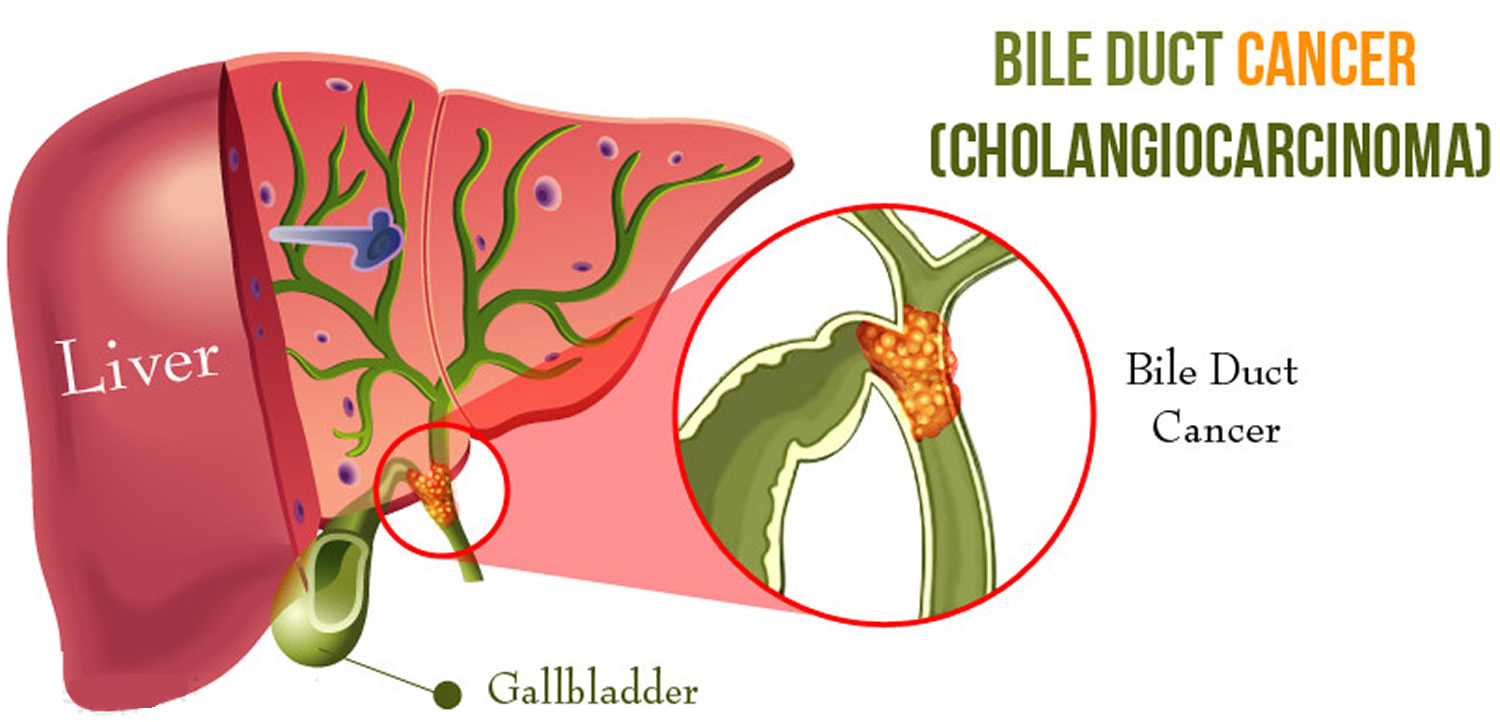
A Síndrome de Mirizzi, descrita originalmente por Pablo Luis Mirizzi em 1948 como um “síndrome hepático funcional”, constitui uma das complicações mais complexas e desafiadoras da colelitíase crônica. Inicialmente atribuída a um espasmo fisiológico do ducto hepático, sua fisiopatologia é hoje claramente compreendida como uma obstrução mecânica extrínseca do ducto hepático comum ou do colédoco, secundária ao impacto crônico de cálculos no infundíbulo da vesícula biliar (difundido como bolsa de Hartmann) ou no ducto cístico. Trata-se de uma entidade nosológica incomum, acometendo entre 0,05% e 5,7% dos pacientes submetidos a procedimentos cirúrgicos biliares no Ocidente. O grande desafio reside na intensa reação inflamatória local que oblitera os planos de clivagem anatômicos, culminando, frequentemente, em erosão parietal e formação de fístula biliobiliárea (colecistobiliar). Além disso, a estase biliar crônica associa esta síndrome ao carcinoma de vesícula biliar em até 28% dos casos. O objetivo desta revisão é estabelecer um algoritmo operacional reprodutível para o manejo terapêutico da Síndrome de Mirizzi, correlacionando a estratificação anatômica de Csendes às abordagens cirúrgicas e endoscópicas contemporâneas.
Classificação de Csendes e Propedêutica Armada
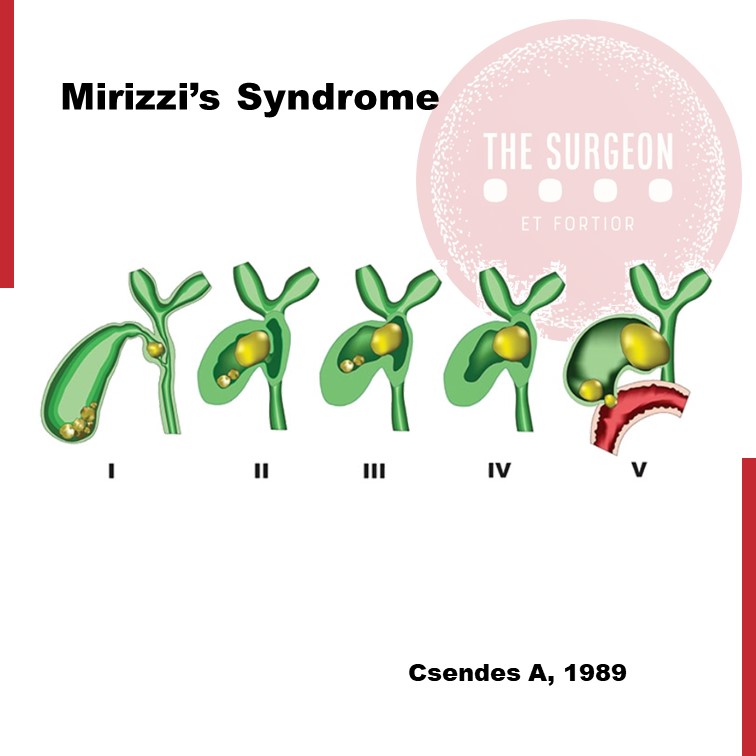
O manejo seguro e a prevenção de lesões iatrogênicas da via biliar principal exigem o estrito mapeamento da destruição tecidual. A classificação de Csendes organiza a apresentação da doença em cinco tipos anatômicos e dita a escalada terapêutica:
Classificação Temática de Csendes para Orientação Tática
| Tipo | Alteração Anatômica Estrutural | Abordagem Terapêutica de Escolha |
| Tipo I | Compressão extrínseca do ducto hepático comum por cálculo impactado, sem fístula. | Colecistectomia total (clássica) ou subtotal, via fundus-first. |
| Tipo II | Presença de fístula colecistobiliar envolvendo menos de 1/3 da circunferência da via biliar. | Colecistectomia subtotal + coledocoplastia com retalho da vesícula ou fechamento sobre tubo em T. |
| Tipo III | Fístula colecistobiliar que compromete entre 1/3 e 2/3 da circunferência do ducto. | Coledocoplastia com remanescente vesicular ou anastomose bilioentérica (Roux-en-Y). |
| Tipo IV | Destruição completa da parede da via biliar principal (> 2/3 da circunferência). | Reconstrução biliar definitiva por Hepático-jejunostomia em Y de Roux. |
| Tipo V | Qualquer tipo (I a IV) associado à presença de fístula colecistoentérica (ex: colecistoduodenal). | Correção da fístula entérica + tratamento do componente biliar correspondente. |
Diagnóstico Semiológico e a Tríade de Imagem
O quadro clínico sobrepõe-se ao de outras afecções hepatobiliares, caracterizado por icterícia obstrutiva, dor em hipocôndrio direito, náuseas e episódios de febre (sinalizando colangite). Laboratorialmente, observa-se padrão colestático proeminente, com elevação acentuada de bilirrubinas e fosfatase alcalina. Havendo suspeita clínica em pacientes idosos com níveis expressivos de CA 19-9, o diagnóstico diferencial com colangiocarcinoma ou neoplasia de vesícula deve ser prontamente conduzido.
A arquitetura radiológica diagnóstica assenta-se em uma tríade clássica observada em exames de imagem, como a Colangiorressonância (CPRM) — método não invasivo de maior acurácia:
- Dilatação do sistema biliar a montante (acima do nível do infundíbulo vesicular).
- Presença de cálculo calcificado e fixo impactado no colo gástrico ou ducto cístico.
- Estreitamento abrupto e retorno ao calibre normal da via biliar abaixo do nível do cálculo.
Estratégias de Exposição e Intervenção
1. O Papel da Endoscopia de Alta Resolução
A Colangiopancreatografia Retrógrada Endoscópica (CPRE) desempenha uma função dual. Inicialmente, funciona como ferramenta de descompressão biliar tática através do posicionamento de próteses (stents) biliares, minimizando a colangite e limpando o “terreno” para o ato cirúrgico. Em doentes de alto risco cirúrgico ou extrema fragilidade, a colangioscopia direta associada à litotripsia eletrohidráulica ou a laser atinge taxas de sucesso de 90% a 100% na fragmentação do cálculo, atuando como tratamento definitivo.
2. Tática Cirúrgica Operacional: A Linha de Defesa contra a Iatrogenia
A cirurgia para a Síndrome de Mirizzi exige o abandono da dissecção habitual do triângulo de Calot. A intensa fibrose impede a obtenção da Critical View of Safety (CVS) de Strasberg por via anterógrada, elevando o risco de trsecção inadvertida do colédoco.
- Manobra Dome-Down / Fundus-First: A dissecção da vesícula biliar deve ser realizada de forma retrógrada, do fundo em direção ao infundíbulo. Ao atingir a transição vesicular, o órgão deve ser aberto longitudinalmente para a evacuação de todos os cálculos.
- Manejo do Coto e Coledocoplastia: Nos casos de Tipo I, se o cístico estiver obliterado, a colecistectomia subtotal com fechamento do remanescente mucoso em bolsa é segura. Nos casos Tipo II, a parede residual da vesícula biliar não deve ser totalmente ressecada; ela é utilizada como um retalho biológico vascularizado para recobrir a fístula sobre um dreno de Kahr (tubo em T), reduzindo o risco de estenose biliar tardia. Nos tipos III e IV, a destruição biliar impede o reparo primário, impondo a realização de uma anastomose hepático-jejunal em Y de Roux ipsilateral, preferencialmente conduzida por cirurgião hepatobiliar experiente.
Pontos-Chave
- Estratificação por Csendes: O planejamento operatório é rigidamente atrelado ao grau de acometimento da parede do colédoco.
- Dissecção Retrógrada (Fundus-First): Abordagem obrigatória para evitar lesões catastróficas da via biliar principal diante da distorção anatômica local.
- Rastreador de Malignidade: Alta correlação com o adenocarcinoma de vesícula; biópsias de congelação perioperatórias devem ser consideradas em áreas suspeitas.
- Racionalização da Laparoscopia: Embora viável no Tipo I em mãos habilitadas, a cirurgia apresenta taxas de conversão elevadas (8% a 76%), não devendo o cirurgião postergar a conversão em caso de dúvida anatômica.
- Descompressão Precoce: A CRE pré-operatória com colocação de stent reduz a fricção cirúrgica ao delimitar a via biliar principal durante a dissecção.
Conclusões Aplicadas à Prática
A Síndrome de Mirizzi permanece como um dos cenários mais complexos da cirurgia do aparelho digestivo, testando os limites do julgamento clínico e da destreza técnica. Esta revisão demonstra que o sucesso terapêutico não decorre do imediatismo operatório, mas de uma abordagem diagnóstica precisa e integrada. O cirurgião moderno deve despir-se do dogma da colecistectomia laparoscópica total sistemática frente a uma anatomia congelada. A adoção da colecistectomia subtotal e o uso estratégico de retalhos vesiculares ou derivações biliodigestivas em Y de Roux constituem medidas de prudência científica que protegem o paciente contra disfunções hepáticas crônicas. Em suma, o manejo da Síndrome de Mirizzi corrobora que a segurança operatória fundamenta-se na simbiose entre o respeito à anatomia patológica e a flexibilidade tática da equipe cirúrgica.
“A anatomia biliar na Síndrome de Mirizzi é um labirinto onde a pressa e a autoconfiança excessiva operam como aliadas do desastre; a paciência tática e a dissecação retrógrada são as únicas vias seguras de retorno.” — Adaptado dos ensinamentos clássicos da Cirurgia Hepatobiliar.
Gostou ❔Nos deixe um comentário ✍️ , compartilhe em suas redes sociais e|ou mande sua dúvida pelo 💬 Chat On-line em nossa DM do Instagram.
Hashtags:
#SindromeDeMirizzi #CirurgiaHepatobiliar #ViaBiliar #CirurgiaDigestiva #SegurancaDoPaciente
Tratamento Cirúrgico do Abscesso Hepático Piogênico
Introdução
O abscesso hepático piogênico (AHP) é uma condição infecciosa grave caracterizada por uma coleção encapsulada de material purulento no fígado. Frequentemente, essa condição é resultante de infecções bacterianas, originárias do trato biliar ou de fontes intra-abdominais, como diverticulite. O manejo do AHP requer uma abordagem multidisciplinar, combinando diagnóstico rápido, antibioticoterapia e, em muitos casos, intervenção cirúrgica. No Brasil, a mortalidade associada a essa condição pode variar de 10% a 20%, sendo particularmente elevada em pacientes com comorbidades, como diabetes e cirrose. A presente revisão discute as abordagens cirúrgicas no tratamento do AHP, com ênfase nos critérios de intervenção, técnicas cirúrgicas e melhores práticas para o cirurgião do aparelho digestivo.
Diagnóstico e Classificação
O diagnóstico precoce do AHP é essencial para determinar a abordagem terapêutica mais adequada. Exames de imagem, como ultrassonografia (USG) e tomografia computadorizada (TC), são as ferramentas primárias para identificar a extensão da lesão e guiar a tomada de decisões. A classificação dos abscessos hepáticos baseia-se em seu tamanho e características morfológicas:
- Abscessos pequenos (menores que 3 cm) podem, muitas vezes, ser tratados com antibioticoterapia isolada.
- Abscessos maiores (geralmente >5 cm) e multiloculados exigem drenagem percutânea ou intervenção cirúrgica.
A etiologia do AHP no Brasil é predominantemente associada a bactérias como Escherichia coli e Klebsiella pneumoniae, e pacientes imunocomprometidos, como diabéticos, estão em maior risco de desenvolver complicações graves.
Abordagem Terapêutica
O tratamento do AHP é multimodal e deve ser adaptado à gravidade do caso, com o uso combinado de antibióticos, drenagem percutânea e intervenção cirúrgica, quando necessário. As diretrizes atuais propõem um algoritmo terapêutico baseado no tamanho e nas características dos abscessos.
1. Antibioticoterapia
A antibioticoterapia empírica deve ser iniciada imediatamente após o diagnóstico, visando cobertura para bactérias gram-negativas e anaeróbias. Ciprofloxacina ou cefixima combinadas com metronidazol são frequentemente utilizadas no manejo de abscessos hepáticos não complicados. A escolha do antibiótico deve ser ajustada conforme os resultados das culturas de sangue e de amostras do abscesso, garantindo uma abordagem personalizada.
2. Drenagem Percutânea
A drenagem percutânea, guiada por USG ou TC, é o tratamento de escolha para abscessos maiores que 3 cm e uniloculares (Tipo II). Esse método minimamente invasivo apresenta uma alta taxa de sucesso, próxima a 90%, sendo eficaz na maioria dos casos. No entanto, falhas podem ocorrer em abscessos multiloculados ou com conteúdo viscoso ou necrótico, situações em que a drenagem percutânea se torna inadequada, necessitando de intervenção cirúrgica.
3. Intervenção Cirúrgica
A cirurgia está indicada em abscessos multiloculados grandes (>3 cm, Tipo III), em abscessos que não respondem à drenagem percutânea ou na presença de complicações, como ruptura do abscesso. A cirurgia pode envolver drenagem minimamente invasiva ou ressecção hepática, dependendo da complexidade do abscesso e da experiência do cirurgião. Abscessos maiores que 10 cm apresentam maior risco de complicações, e nesses casos, a drenagem cirúrgica pode ser preferível. A laparotomia é recomendada em situações de peritonite ou quando o abscesso é de difícil acesso para drenagem percutânea.
4. Laparoscopia
A laparoscopia é uma alternativa minimamente invasiva à cirurgia aberta, indicada em abscessos uniloculares de tamanho moderado. Essa técnica oferece vantagens significativas, como menor tempo de internação e recuperação mais rápida, além de menor risco de complicações pós-operatórias.
Aplicação na Cirurgia Digestiva
O papel do cirurgião do aparelho digestivo é central no manejo dos abscessos hepáticos, especialmente em casos que requerem intervenção cirúrgica. A drenagem percutânea deve ser considerada a primeira linha de tratamento sempre que viável, mas o cirurgião deve estar preparado para realizar intervenções mais invasivas quando necessário. A laparoscopia tem demonstrado resultados promissores, reduzindo o tempo de internação e o risco de complicações. No Brasil, as infecções intra-abdominais complicadas são uma das principais causas de internação em emergências cirúrgicas, e o manejo adequado desses casos depende de uma sólida formação técnico-cirúrgica.
Algoritmo de Tratamento
Com base nas evidências disponíveis, um algoritmo de tratamento para o AHP pode ser delineado da seguinte forma:
- Abscessos pequenos (<3 cm, Tipo I): Tratamento com antibióticos isolados.
- Abscessos grandes uniloculares (>3 cm, Tipo II): Drenagem percutânea associada a antibioticoterapia.
- Abscessos grandes multiloculados (>3 cm, Tipo III): Intervenção cirúrgica.
Pontos-Chave
- Diagnóstico Precoce: O uso da TC com contraste é fundamental para o diagnóstico preciso do tamanho e da localização dos abscessos hepáticos, orientando a decisão terapêutica.
- Intervenção Cirúrgica: Abscessos multiloculados ou maiores que 5 cm frequentemente requerem intervenção cirúrgica, especialmente quando a drenagem percutânea falha.
- Abordagem Minimamente Invasiva: A laparoscopia oferece uma alternativa eficaz à cirurgia aberta, proporcionando uma recuperação mais rápida e com menor morbidade.
- Manejo Integral pelo Cirurgião Digestivo: O conhecimento técnico-cirúrgico é essencial para o manejo de abscessos hepáticos complexos, garantindo uma abordagem eficaz e personalizada.
Conclusão
O manejo do abscesso hepático piogênico exige uma abordagem multidisciplinar, sendo o cirurgião digestivo uma peça-chave no tratamento de casos complexos. A decisão entre drenagem percutânea e intervenção cirúrgica deve considerar múltiplos fatores, como o tamanho do abscesso, a resposta ao tratamento conservador e as condições clínicas do paciente. Como afirmou o Prof. Henri Bismuth: “Le traitement chirurgical n’est pas seulement une question de technique, mais de jugement. Le moment de l’intervention est aussi important que l’intervention elle-même.” Assim, o domínio técnico e a tomada de decisões precisas são fundamentais para o sucesso terapêutico no tratamento do AHP.
Gostou ❔Nos deixe um comentário ✍️, compartilhe em suas redes sociais e|ou mande sua dúvida pelo 💬 Chat On-line em nossa DM do Instagram.
#AbscessoHepatico #CirurgiaDigestiva #TratamentoAbscesso #DrenagemPercutanea #AparelhoDigestivo
Internal Hernia after Laparoscopic Gastric Bypass
The purpose of this review is to evaluate the incidence and management of internal hernias (with or without SBO) after LGBP.
INTRODUCTION
Laparoscopic Roux-en-Y gastric bypass (LGBP) has been shown to be an effective treatment for morbid obesity, both in terms of weight loss and improvement in multiple comorbidities. While the laparoscopic approach offers many advantages to the patient in terms of fewer wound complications, decreased length of hospital stay, and decreased postoperative pain, certain complications of this operation continue to pose difficult clinical problems as the number of procedures performed increases. One such complication is internal hernia through one of the mesenteric defects, which can result in small bowel obstruction, ischemia, or infarction and often requires reoperation.
An internal hernia is defined as a protrusion of intestine through a defect within the peritoneal cavity, as opposed to an external (or incisional) hernia that protrudes through all layers of the abdominal wall. Internal hernias almost always occur through iatrogenic defects created surgically.

Incisional hernias occur at a higher incidence after open gastric bypass (GBP) at a rate of about 20 percent. LGBP has a lower rate of incisional hernias. A recent study by Rosenthal, et al., showed a 0.2-percent rate of port site hernias in 849 patients using blunt-tip trocars at 3,744 port sites. Internal hernias, on the other hand, occur more frequently in LGBP than in the open procedure. This is a significant clinical problem, since internal hernia is the most common cause of small bowel obstruction (SBO) after LGBP. Retrospective reviews have found the incidence of SBO after LGBP to be between 1.8 and 9.7 percent. The incidence of internal hernia after LGBP is between 0.2 and 8.6 percent based on multiple studies.
This incidence is higher than that seen with open GBP, and this is presumably due to decreased adhesion formation after laparoscopic surgery compared to open surgery. The creation of potential space as a result of weight loss may also be a contributing factor in the etiology of internal hernias, which often present in a delayed fashion. In addition, the particular case of pregnancy— with the mass effect of an enlarging uterus—may predispose to this condition, as there have been three case reports in the literature of internal hernia during pregnancy, one of which resulted in intestinal ischemia and fetal demise. Due to the increasing scope of this problem and its potentially devastating consequences, surgeons should have a high clinical suspicion for internal hernia after LGBP.
An internal hernia can potentially occur through either two or three defects, depending on whether a retrocolic or antecolic technique is used for the Roux limb. Petersen’s defect is defined as the space between the Roux limb and the transverse mesocolon. A defect is also present between the biliopancreatic and Roux limbs at the jejunojejunostomy. If a retrocolic approach is used, a third defect in the transverse mesocolon is created. This is the most common site of internal hernia in most reports, which has prompted many surgeons to adopt an antecolic technique in order to eliminate this defect. Higa’s study of 2,000 patients showed an internal hernia distribution of 67 percent mesocolic, 21 percent jejunal, and 7.5 percent Petersen. However, some centers experience a higher rate of hernia in the jejunal or Petersen’s defects, despite the use of a retrocolic approach.
PRESENTATION
Patients with internal hernia most commonly present with abdominal pain, and may also have symptoms of small bowel obstruction. The time of presentation varies greatly and may occur within one week of the initial operation or up to three years postoperatively. However, the majority of cases occur between 6 and 24 months postoperative. Radiographic diagnosis of internal hernia presents a challenge since the characteristic findings on computed tomography (CT) scan are often missed.
Features suggestive of an internal hernia include small bowel loops in the upper quadrants; evidence of small bowel mesentery crossing the transverse mesocolon; presence of the jejunojejunostomy superior to the transverse colon; signs of small bowel obstruction; or twisting, swirling, crowding, stretching, or engorgement of the main mesenteric trunk and according to one study, the sensitivity and specificity of CT is 63 percent and 76 percent, respectively.
Another study showed that although the diagnosis was only made prospectively by CT scan in 64 percent of cases, a retrospective review of the images showed that diagnostic abnormalities were present in 97 percent of cases. A report of five cases of internal hernia by Onopchenko found that only one was diagnosed preoperatively by radiological reading, even though all five had findings suggestive of internal hernia to the bariatric surgeon. These findings emphasize the need for communication with the radiologist, careful attention to patient history, and high clinical suspicion for internal hernias. In rare cases, closed loop obstruction and extensive bowel ischemia and infarction can occur. This dreaded complication underscores the necessity of making a rapid diagnosis. If the patient has significant symptoms but radiologic studies are negative, a diagnostic laparoscopy is warranted to rule out internal hernia.
PREVENTION AND TREATMENT
Given the prevalence of internal hernias and the increasing popularity of bariatric surgery, it is important to prevent or minimize this complication at the time of the initial operation. Although there have been no randomized, controlled trials comparing different techniques of LGBP, some authors have anecdotally reported lower rates of internal hernia after modifying their technique from a retrocolic to antecolic approach. Champion and Williams reported a significant decrease in small bowel obstruction after changing to an antecolic position, and Felsher and colleagues found no internal hernias in their study after adopting the antecolic approach.
However, other studies support careful defect closure as the most important factor in reducing hernia rates. Dresel and colleagues report no internal hernias after modifying their technique to include closure of Petersen’s defect. Carmody and colleagues report a decreased hernia incidence when closing all defects, even with a retrocolic approach. DeMaria’s study reports anecdotal improvement after closing mesenteric defects in two layers, on the medial and lateral aspects of the defect.
The majority of internal hernias can be successfully treated laparoscopically, with reduction and defect closure. The laparoscopic approach is usually successful; however, because of the lack of adhesion formation after laparoscopy, Capella, et al., suggest laparotomy for patients who experience a second episode of bowel obstruction due to recurrent internal hernia after laparoscopic repair. The greater adhesion formation after laparotomy may help prevent future internal hernia formation.
CONCLUSION
One of the benefits of laparoscopy, decreased adhesion formation, is likely also responsible for the increasing prevalence of internal hernia as a complication following laparoscopic gastric bypass. Although it has not been borne out in randomized clinical trials, anecdotal evidence and expert opinion suggest that Roux limb position and mesenteric defect closure at the time of initial operation are important factors in ultimate rates of hernia formation. Careful attention must be paid to individual surgical techniques in order to prevent this potentially devastating complication. The benefits of LGBP are maximized when there is a low incidence of postoperative hernias and resultant obstruction.
Anatomia Cirúrgica Pancreática
A anatomia cirúrgica do pâncreas é um dos tópicos mais fascinantes e desafiadores da cirurgia do aparelho digestivo. Conhecer detalhadamente a estrutura e a topografia do pâncreas é crucial para a realização de procedimentos cirúrgicos seguros e eficazes. Neste artigo, vamos explorar os aspectos mais importantes da anatomia pancreática, abordando pontos-chave para estudantes de medicina e residentes de cirurgia do aparelho digestivo.
Estrutura Anatômica do Pâncreas
O pâncreas é uma glândula retroperitoneal situada transversalmente no abdome, na altura das vértebras L1-L2, abrangendo os principais vasos sanguíneos e a coluna vertebral. Ele é composto por cinco partes principais: cabeça, colo, corpo, cauda e processo uncinado.
- Cabeça: Localizada à direita da linha média, cercada pelo duodeno. A cabeça do pâncreas possui uma extensão inferior chamada processo uncinado, que está intimamente relacionada com a veia mesentérica superior e a artéria mesentérica superior.
- Colo: Uma parte estreita entre a cabeça e o corpo, situada anteriormente à veia porta, definida pela localização anatômica anterior à formação da veia porta, geralmente pela confluência das veias mesentérica superior e esplênica.
- Corpo: Estende-se para a esquerda, posterior ao estômago, com a superfície anterior coberta pelo peritônio, formando parte da parede posterior do saco menor.
- Cauda: Parte terminal que se estende até o hilo esplênico, confinada entre as camadas do ligamento esplenorrenal juntamente com a artéria esplênica e a origem da veia esplênica.
- Processo Uncinado: Considerado uma parte distinta do pâncreas devido à sua origem embriológica diferente, estendendo-se posteriormente aos vasos mesentéricos superiores.
Peso e Dimensões Normais
Em um adulto saudável, o pâncreas tem um peso médio de aproximadamente 80 a 120 gramas. As dimensões normais do pâncreas variam, mas geralmente medem cerca de 15 a 20 cm de comprimento, 4 a 5 cm de largura na cabeça, e 1,5 a 2,5 cm de espessura.
Vascularização do Pâncreas
A vascularização do pâncreas é complexa e vital para a compreensão cirúrgica. As principais artérias que irrigam o pâncreas são:
- Artéria Pancreatoduodenal Superior: Ramo da artéria gastroduodenal que irriga a cabeça do pâncreas.
- Artéria Pancreatoduodenal Inferior: Ramo da artéria mesentérica superior que também fornece sangue à cabeça do pâncreas.
- Ramos Pancreáticos da Artéria Esplênica: Irrigam o corpo e a cauda do pâncreas.
As veias pancreáticas drenam para a veia esplênica, veia mesentérica superior e, eventualmente, para a veia porta.
Ductos Pancreáticos
O pâncreas possui dois principais ductos: o ducto pancreático principal (ducto de Wirsung) e o ducto pancreático acessório (ducto de Santorini).
- Ducto Pancreático Principal (Ducto de Wirsung): Começa na cauda do pâncreas e percorre o corpo até a cabeça, onde geralmente se junta ao ducto biliar comum na ampola de Vater, regulada pelo esfíncter de Oddi. O diâmetro normal do ducto pancreático principal varia de 1 mm na cauda até 3 mm na cabeça.
- Ducto Pancreático Acessório (Ducto de Santorini): Corre superior e paralelo ao ducto de Wirsung, drenando parte da cabeça do pâncreas na papila duodenal menor.
O esfíncter de Oddi é uma estrutura única de fibras musculares lisas que regula o fluxo das secreções biliares e pancreáticas para o duodeno e impede o refluxo do conteúdo intestinal para o sistema ductal pancreatobiliar.
Considerações Cirúrgicas
Entender a anatomia pancreática é essencial para evitar complicações durante procedimentos cirúrgicos. Algumas das considerações importantes incluem:
- Ressecção Pancreática: Procedimentos como a pancreatoduodenectomia (procedimento de Whipple) requerem um conhecimento detalhado das relações anatômicas para garantir a remoção eficaz do tumor com a menor morbidade possível.
- Drenagem Biliar: A proximidade do pâncreas com o ducto biliar comum exige precisão ao evitar danos durante as cirurgias.
- Anastomoses Pancreáticas: A criação de anastomoses seguras entre o pâncreas e o intestino é crítica para prevenir complicações pós-operatórias, como fístulas pancreáticas.
Variações Anatômicas
As variações anatômicas do pâncreas e dos ductos pancreáticos são comuns e podem impactar significativamente a abordagem cirúrgica. Uma compreensão detalhada dessas variações é essencial para a personalização do plano cirúrgico. Por exemplo, o pâncreas anular é uma condição em que o tecido pancreático forma um anel ao redor do duodeno, podendo causar estenose duodenal.
Conclusão
A anatomia cirúrgica pancreática é um campo complexo e detalhado que exige estudo e prática contínuos. Compreender as nuances dessa anatomia é fundamental para qualquer cirurgião do aparelho digestivo. Como disse o renomado anatomista Andreas Vesalius: “A anatomia é a fundação de todas as ciências médicas.”
Gostou? Nos deixe um comentário ✍️, ou mande sua dúvida pelo 💬 Chat On-line em nossa DM do Instagram.
Hashtags
#AnatomiaPancreática #CirurgiaDigestiva #EstudantesDeMedicina #ResidentesDeCirurgia #Pancreas

ERCP Induced Perforations
In the epoch of minimally invasive management of biliary and pancreatic disorders, endoscopic retrograde cholangiopancreatography (ERCP) combined with endoscopic sphincterotomy (ES) has become a prevalent procedure all over the world. Even though ES is a safe procedure, it carries a small but significant number of serious complications which include pancreatitis, bleeding, cholangitis and perforation. As per old literature, ERCP-related perforations were reported in 0.5–2.1% of sphincterotomies with a mortality rate of 16–18%. However, the improvement in the experience and skill of the endoscopy specialists combined with advancements in technology have reduced the incidence of perforation to <0.5% over the years. Sphincterotomy (56%) and guidewire manipulation (23%) are widespread causes of perforations related to endoscopic retrograde cholangiopancreatography (ERCP). There is a dearth of evidence-based strategies with respect to the proper management of ERCP perforations. While one set of investigators promote on-demand conservative and surgical management, based on a clinical course, the others support operative repair in all cases on account of the complications associated with the delayed operative intervention.
INDICATIONS OF SURGICAL MANAGEMENT
1. Large extravasation of contrast at the time of ERCP defined as incomplete dissipation of contrast after 1 min on follow-up plain film.
2. If there is only a small amount of contrast extravasation, where there is complete dissipation after 1 min of ERCP, on follow-up plain film, then a UGI with contrast injection on fluoroscopy is performed in 2–8 h. If this shows extravasation, we recommend surgical exploration.
3. Follow-up CT scan showing a collection due to perforation in the retroperitoneum or intraperitoneum.
4. Retained hardware unable to be removed by endoscopy along with perforation.
5. Massive subcutaneous emphysema.
6. Failure of conservative management.
A delay in diagnosis or in surgery will lead to death. The reason is that there is a massive autodigestion of body tissues which is due to a constant release of enzymes, and this eventually leads to sepsis. The principle of treatment by surgery is the same as endoscopic treatment. Any case that is suspected to have ERCP-induced perforation is kept nil by mouth, and the gastric contents are decompressed by Ryles tube and intravenous antibiotics.
This is done by diverting bile, enteric and pancreatic juices away from the site of perforation. However simple drainage will also cause the juices to flow through the perforation site and body cavities before draining out of the tubes. This could be avoided by diverting the juices through well-controlled different paths which could be done by the following procedures:
1. T-tube in CBD;
2. Placement of duodenostomy tube—lateral/end duodenostomy;
3. Duodenal diverticulization;
4. Pyloric exclusion;
5. Roux-en-Y duodenojejunostomy.
The disadvantage of using Roux-en-Y duodenojejunostomy is that if the edges are inflamed, then the sutures will not hold properly. However other procedures can be used even when the edges are inflamed. Even though duodenostomy appears to be simple, a part of gastric and duodenal contents pass across the perforation site.
Duodenal diverticulization involves three things: (1) tube to divert duodenal and pancreatic juice, (2) T-tube in CBD to divert bile and (3) distal
gastrectomy and Billroth II anastomosis to provide an alternate pathway for food and gastric juice, thereby preventing these from passing through the site of perforation. Although this procedure has been proved to be successful, it is less widely used due to its complex nature. Pyloric exclusion is a simpler form in which the pylorus is closed by purse string by long-standing absorbing sutures like PDS 2.0 instead of distal gastrectomy. Similar to duodenal diverticulization, T-tube drainage of the CBD and loop gastrojejunostomy are done. The duodenal perforation is closed over a duodenostomy tube.
Whenever there is collection which is localized to the retroperitoneum, retroperitoneal surgical approach can be carried out. Advantages of this procedure are (1) it permits gravitational drainage, (2) avoids septic complication of the peritoneal cavity, (3) directs retroperitoneal necrosectomy with post-operative washes and (4) avoids complex intra-abdominal surgeries. However the disadvantage of this procedure is that it can be used only for retroperitoneal-contained perforations.
Surgeons and Performance
SURGEONS ARE HIGH PERFORMANCE ATHLETES
In a 2011 New Yorker article, Dr. Atul Gawande explored the idea that surgeons should consider a performance coach. Like athletes, he reasons, surgeons rely on complex physical movements to achieve their goals. Guidance and refinement by a trained eye could improve their performance.
Surgical coaching is a controversial topic (one which colleagues and I are actively investigating). But in the years following Dr. Gawande’s article, this idea opened the door to a broader concept: the “surgeon athlete.” An “athlete” is one whose performance depends on a carefully choreographed interplay between mind and body: heightened focus and anticipation along with quick decision-making and coordination. Combined with the reliance on teamwork and requisite stamina, this is wholly within the job description of a surgeon. Many surgeons are likely to find this concept silly. But our profession has imprudently encouraged surgical trainees to disregard the critical fine-tuning of their minds and bodies. We demand perfection, stamina, and encyclopedic knowledge, while discouraging the healthy habits that improve performance. Ironically, the sports world is more advanced in applying science to their training. And by ignoring this indisputable science, we are really hurting our patients. Because in order to best take care of them, we need to first take care of ourselves.
A especialização e a busca pela excelência

“Onde quer que a arte de curar é amada, também há um amor pela humanidade.” — Hipócrates
A especialização em órgãos e o volume de casos têm sido temas centrais nos últimos anos, revelando uma relação direta entre alto volume de procedimentos e melhores desfechos, conforme evidenciado pela literatura recente. Estudos mostram que a concentração de procedimentos de alto risco, como esofagectomias, pancreatectomias e ressecções hepáticas, em centros especializados pode reduzir significativamente a mortalidade pós-operatória anual. Embora procedimentos como tireoidectomias e ressecções do cólon mostrem um efeito semelhante, mas em menor escala, a redução da mortalidade pós-operatória em 5% pode ser tão eficaz quanto tratamentos adjuvantes tóxicos e deve ser uma prioridade na busca pela mais alta qualidade em cirurgia oncológica e digestiva. Além da redução da morbidade e mortalidade, há evidências de que a especialização pode levar a melhores resultados funcionais e financeiros. Às vezes, a atenção excessiva aos números anuais obscurece o fato de que hospitais menores, com equipes dedicadas, também podem alcançar bons resultados. É provável que não apenas o volume, mas também o treinamento e a especialização resultem em melhores desfechos. Definir um número absoluto de casos pode ser improdutivo e desviar a atenção de fatores essenciais, como reuniões multidisciplinares organizadas, infraestrutura adequada e disponibilidade de técnicas modernas.
O Foco na Otimização do Processo
O foco deve ser direcionado para a análise e otimização de todo o processo de diagnóstico e tratamento, já que este processo pode colocar o paciente em grave risco, especialmente durante o período hospitalar. A prevenção de erros tem recebido atenção significativa, levando ao surgimento do conceito de segurança do paciente. Desde a publicação do relatório To Err Is Human pelo Institute of Medicine, a abordagem para erros mudou drasticamente.
Em vez de focar exclusivamente no indivíduo, a abordagem sistêmica considera as condições em que as pessoas trabalham e tenta construir defesas para mitigar os efeitos dos erros. O modelo de queijo suíço ilustra bem essa abordagem: várias camadas de defesa, cada uma com suas falhas, são colocadas em torno de um procedimento. As falhas ativas e condições latentes criam buracos em cada camada. Em vez de apenas fechar os buracos na última camada de defesa, redesenhar o processo e fechar um buraco em uma camada anterior pode ser mais eficaz.
A análise de causa raiz é essencial para identificar pontos fracos no procedimento. Um exemplo é a colocação incorreta de uma colostomia após uma resseção abdominoperineal. Em vez de culpar o residente por não selecionar a posição correta durante a cirurgia ou marcar o ponto errado no dia anterior, uma solução mais eficaz seria o treinamento adequado do junior ou a marcação do ponto certo por um terapeuta de estomas durante a clínica ambulatorial.
A marcação do local correto no corpo tornou-se uma medida de segurança e o paciente deve ser instruído a exigir essa prática para sua própria segurança. É crucial eliminar a cultura de ‘culpa e vergonha’ e promover um ambiente mais aberto, onde erros e quase erros possam ser relatados. O clima de segurança em um departamento cirúrgico pode ser medido de forma validada e é um elemento essencial para uma cultura onde a segurança do paciente possa prosperar.
O Cuidado com os Detalhes e a Otimização de Resultados
A atenção meticulosa a cada detalhe durante o período pré-operatório e clínico pode reduzir eventos adversos. O que é chamado de “primeira vez em risco” deve ser considerado. Há também exemplos de ações para otimizar resultados que são mais específicas para o câncer. Por exemplo, o uso de técnicas que estimulam a cicatrização de feridas após uma resseção abdominoperineal, como a omentoplastia ou o retal abdominal flap, pode evitar atrasos no tratamento adjuvante para câncer retal.
A atenção cuidadosa à cicatrização de feridas em sarcoma pode evitar o adiamento da necessária radioterapia adjuvante. Omissão de uma tomografia computadorizada com contraste contendo iodo no diagnóstico de câncer de tireoide pode possibilitar um tratamento radioativo com iodo mais precoce, resultando em possíveis melhores resultados. A coleta de um número suficiente de linfonodos em câncer de cólon pode evitar discussões sobre a indicação de quimioterapia adjuvante.
A maioria dos exemplos de segurança do paciente no período clínico está relacionada ao uso ótimo de tratamento multimodal ou aos efeitos gerais da cirurgia. Às vezes, é necessário equilibrar o risco de aceitar um procedimento cirúrgico mais extenso, com uma morbidade mais alta, para alcançar um melhor resultado a longo prazo. O oposto também é possível, quando um bom resultado de curto prazo de uma excisão local em câncer retal deve ser equilibrado com uma maior taxa de recorrência local. A garantia de qualidade para todas as disciplinas participantes (diagnósticas e terapêuticas) é um elemento chave na configuração de ensaios clínicos prospectivos e randomizados.
“A prática é a maior professora, e o mais sábio cirurgião é aquele que aprende a valorizar o conhecimento não apenas pela sua acumulação, mas pela sua aplicação.” — William Osler
Anatomia Cirúrgica Hepática
O Mapa Fundamental para Ressecções e Transplantes
Autor: Prof. Dr. Ozimo Gama
Categoria: Cirurgia Hepatobiliar / Anatomia Aplicada / Transplante Hepático Tempo de Leitura: 12 minutos
“Um bom conhecimento da anatomia do fígado é um pré-requisito para a cirurgia moderna do fígado.” — H. Bismuth
Introdução
O fígado, o maior órgão sólido do corpo humano (representando 2-3% do peso corporal), é uma estrutura de complexidade arquitetônica fascinante. Para o cirurgião geral, e imperativamente para o cirurgião hepatobiliar, o domínio da anatomia hepática transcende a memorização de nomes; trata-se de compreender as relações tridimensionais que ditam a segurança de uma hepatectomia e o sucesso de um transplante. Neste artigo, dissecaremos a anatomia hepática sob uma ótica cirúrgica, indo além da morfologia externa para explorar a segmentação funcional e as nuances vasculares vitais para a prática operatória de excelência.
1. Meios de Fixação e Mobilização Cirúrgica
O fígado é envolto pela cápsula de Glisson e peritônio, exceto na “área nua” diafragmática e no hilo. Seus ligamentos não são apenas estruturas de sustentação, mas marcos anatômicos cruciais para a mobilização segura do órgão:
-
Ligamentos Coronários e Triangulares: A mobilização destes permite a exposição da veia cava inferior (VCI) e das veias hepáticas.
-
Ligamento Venoso (Arantius): Remanescente do ducto venoso fetal. Sua dissecção é uma manobra chave. Ao isolá-lo, o cirurgião ganha acesso ao tronco das veias hepáticas esquerda e média, facilitando o controle vascular em hepatectomias esquerdas ou transplantes.
-
Ligamento Hepatocaval (Makuuchi): Uma estrutura fibrosa (por vezes contendo parênquima) que fixa o lobo caudado à veia cava. Sua divisão cuidadosa é obrigatória para expor a veia hepática direita e para a mobilização completa do lobo direito em transplantes intervivos.
2. A Revolução de Couinaud
A anatomia clássica, que dividia o fígado em lobos direito, esquerdo, quadrado e caudado baseada apenas em marcos externos (como o ligamento falciforme), é insuficiente para a cirurgia moderna. A verdadeira divisão funcional segue a Linha de Cantlie, um plano imaginário que vai do leito da vesícula biliar à veia cava inferior. Esta linha divide o fígado em metades funcionalmente independentes (Direita e Esquerda), cada uma com sua própria irrigação arterial, portal e drenagem biliar.
Adotamos a Segmentação de Couinaud (1954), que organiza o fígado em 8 segmentos baseados na distribuição das veias hepáticas e pedículos portais:
-
Fígado Direito (Setores Anterior e Posterior): Segmentos V, VIII (Anterior) e VI, VII (Posterior).
-
Fígado Esquerdo: Segmentos II, III (Lateral) e IV (Medial).
-
Lobo Caudado (Segmento I): Uma entidade autônoma. Localizado dorsalmente, recebe sangue de ambos os ramos portais (direito e esquerdo) e drena diretamente na VCI através de veias curtas. Esta drenagem direta confere ao caudado uma “proteção” relativa em casos de Síndrome de Budd-Chiari, onde ele frequentemente se hipertrofia.
3. O Hilo Hepático e a Tríade Portal
A dissecção do hilo exige precisão milimétrica, especialmente em transplantes com doador vivo (LDLT). As estruturas da tríade portal seguem uma organização anteroposterior constante que guia o cirurgião:
-
Ducto Biliar: Mais ventral (anterior) e lateral.
-
Artéria Hepática: Medial e na camada intermédia.
-
Veia Porta: A estrutura mais dorsal (posterior).
Variações Vasculares Importantes
-
Artéria Hepática: A anatomia “clássica” (artéria hepática comum saindo do tronco celíaco) está presente em apenas 60% dos casos. Variações críticas incluem a Artéria Hepática Direita Substituída (da Mesentérica Superior), que passa posterior à veia porta, e a Artéria Hepática Esquerda Substituída (da Gástrica Esquerda). O não reconhecimento pode levar à necrose do enxerto ou isquemia biliar.
-
Veia Porta: Variações na bifurcação, como a ausência do tronco principal da veia porta direita (trifurcação), exigem reconstruções complexas em transplantes.
4. Drenagem Venosa: O Escoamento
As três veias hepáticas principais (Direita, Média e Esquerda) correm nas fissuras intersegmentares:
-
Veia Hepática Direita (RHV): Drena o setor posterior. É a maior veia.
-
Veia Hepática Média (MHV): Corre na fissura principal (Linha de Cantlie). Fundamental para a drenagem dos segmentos V e VIII. Em transplantes de lobo direito, a gestão dos tributários da MHV é crítica para evitar congestão do enxerto.
-
Veias Acessórias: Cerca de metade da população possui veias hepáticas acessórias inferiores (drenando os segmentos VI e VII diretamente na cava). Se calibrosas (>5mm), devem ser reimplantadas para garantir a função do enxerto.
5. A Via Biliar e sua Vascularização: O “Tendão de Aquiles”
A anatomia biliar é a mais variável e propensa a complicações.
-
Irrigação Biliar: Diferente do parênquima, os ductos biliares extra-hepáticos são irrigados exclusivamente por um plexo arterial peribiliar (artérias das 3h e 9h), derivado principalmente da artéria hepática direita e retroduodenal.
-
Pérola Cirúrgica: Durante a captação do fígado, a dissecção excessiva do ducto biliar pode desvascularizá-lo, levando a estenoses isquêmicas tardias. Preservar a bainha peribiliar e o tecido hilar é mandatório.
6. A Vesícula Biliar e o Triângulo de Calot
Embora a colecistectomia seja um procedimento comum, ela exige respeito absoluto à anatomia. O Triângulo de Calot (delimitado pelo ducto cístico, ducto hepático comum e borda hepática) é a zona de segurança. A artéria cística deve ser identificada aqui. Variações, como um ducto cístico curto ou inserção no ducto direito, ou uma artéria hepática direita tortuosa (“Hump”) invadindo o triângulo, são armadilhas para o cirurgião desatento.
Conclusão
A cirurgia hepática evoluiu de ressecções em cunha não anatômicas para segmentectomias precisas e transplantes de doadores vivos. Essa evolução foi sustentada por um aprofundamento do conhecimento anatômico. Para o cirurgião em formação, o estudo exaustivo destas estruturas, suas variações e suas relações vasculares não é apenas acadêmico — é a base ética para oferecer segurança e cura aos pacientes portadores de doenças hepatobiliares.
Gostou ❔Nos deixe um comentário ✍️ , compartilhe em suas redes sociais e|ou mande sua dúvida pelo 💬 Chat On-line em nossa DM do Instagram.
Hashtags: #AnatomiaHepatica #CirurgiaDoFigado #TransplanteHepatico #Couinaud #CirurgiaHPB
Hepatic Surgery: Portal Vein Embolization

INTRODUCTION
Portal vein Embolizations (PVE) is commonly used in the patients requiring extensive liver resection but have insufficient Future Liver Remanescent (FLR) volume on preoperative testing. The procedure involves occluding portal venous flow to the side of the liver with the lesion thereby redirecting portal flow to the contralateral side, in an attempt to cause hypertrophy and increase the volume of the FLR prior to hepatectomy.
PVE was first described by Kinoshita and later reported by Makuuchi as a technique to facilitate hepatic resection of hilar cholangiocarcinoma. The technique is now widely used by surgeons all over the world to optimize FLR volume before major liver resections.
PHYSIOPATHOLOGY
PVE works because the extrahepatic factors that induce liver hypertrophy are carried primarily by the portal vein and not the hepatic artery. The increase in FLR size seen after PVE is due to both clonal expansion and cellular hypertrophy, and the extent of post-embolization liver growth is generally proportional to the degree of portal flow diversion. The mechanism of liver regeneration after PVE is a complex phenomenon and is not fully understood. Although the exact trigger of liver regeneration remains unknown, several studies have identified periportal inflammation in the embolized liver as an important predictor of liver regeneration.

THECNICAL ASPECTS
PVE is technically feasible in 99% of the patients with low risk of complications. Studies have shown the FLR to increase by a median of 40–62% after a median of 34–37 days after PVE, and 72.2–80% of the patients are able to undergo resection as planned. It is generally indicated for patients being considered for right or extended right hepatectomy in the setting of a relatively small FLR. It is rarely required before extended left hepatectomy or left trisectionectomy, since the right posterior section (segments 6 and 7) comprises about 30% of total liver volume.
PVE is usually performed through percutaneous transhepatic access to the portal venous system, but there is considerable variability in technique between centers. The access route can be ipsilateral (portal access at the same side being resected) with retrograde embolization or contralateral (portal access through FLR) with antegrade embolization. The type of approach selected depends on a number of factors including operator preference, anatomic variability, type of resection planned, extent of embolization, and type of embolic agent used. Many authors prefer ipsilateral approach especially for right-sided tumors as this technique allows easy catheterization of segment 4 branches when they must be embolized and also minimizes the theoretic risk of injuring the FLR vasculature or bile ducts through a contralateral approach and potentially making a patient ineligible for surgery.
However, majority of the studies on contralateral PVE show it to be a safe technique with low complication rate. Di Stefano et al. reported a large series of contralateral PVE in 188 patients and described 12 complications (6.4%) only 6 of which could be related to access route and none precluded liver resection. Site of portal vein access can also change depending on the choice of embolic material selected which can include glue, Gelfoam, n-butyl-cyanoacrylate (NBC), different types and sizes of beads, alcohol, and nitinol plus. All agents have similar efficacy and there are no official recommendations for a particular type of agent.
RESULTS
Proponents of PVE believe that there should be very little or no tumor progression during the 4–6 week wait period for regeneration after PVE. Rapid growth of the FLR can be expected within the first 3–4 weeks after PVE and can continue till 6–8 weeks. Results from multiple studies suggest that 8–30% hypertrophy over 2–6 weeks can be expected with slower rates in cirrhotic patients. Most studies comparing outcomes after major hepatectomy with and without preoperative PVE report superior outcomes with PVE. Farges et al. demonstrated significantly less risk of postoperative complications, duration of intensive care unit, and hospital stay in patients with cirrhosis who underwent right hepatectomy after PVE compared to those who did not have preoperative PVE. The authors also reported no benefit of PVE in patients with a normal liver and FLR >30%. Abulkhir et al. reported results from a meta-analysis of 1088 patients undergoing PVE and showed a markedly lower incidence of Post Hepatectomy Liver Failure (PHLF) and death compared to series reporting outcomes after major hepatectomy in patients who did not undergo PVE. All patients had FLR volume increase, and 85% went on to have liver resection after PVE with a PHLF incidence of 2.5% and a surgical mortality of 0.8%. Several studies looking at the effect of systemic neoadjuvant chemotherapy on the degree of hypertrophy after PVE show no significant impact on liver regeneration and growth.
VOLUMETRIC RESPONSE

The volumetric response to PVE is also a very important factor in understanding the regenerative capacity of a patient’s liver and when used together with FLR volume can help identify patients at risk of poor postsurgical outcome. Ribero et al. demonstrated that the risk of PHLF was significantly higher not only in patients with FLR ≤ 20% but also in patients with normal liver who demonstrated ≤5% of FLR hypertrophy after PVE. The authors concluded that the degree of hypertrophy >10% in patients with severe underlying liver disease and >5% in patients with normal liver predicts a low risk of PHLF and post-resection mortality. Many authors do not routinely offer resection to patients with borderline FLR who demonstrate ≤5% hypertrophy after PVE.
Predicting LIVER REMNANT Function
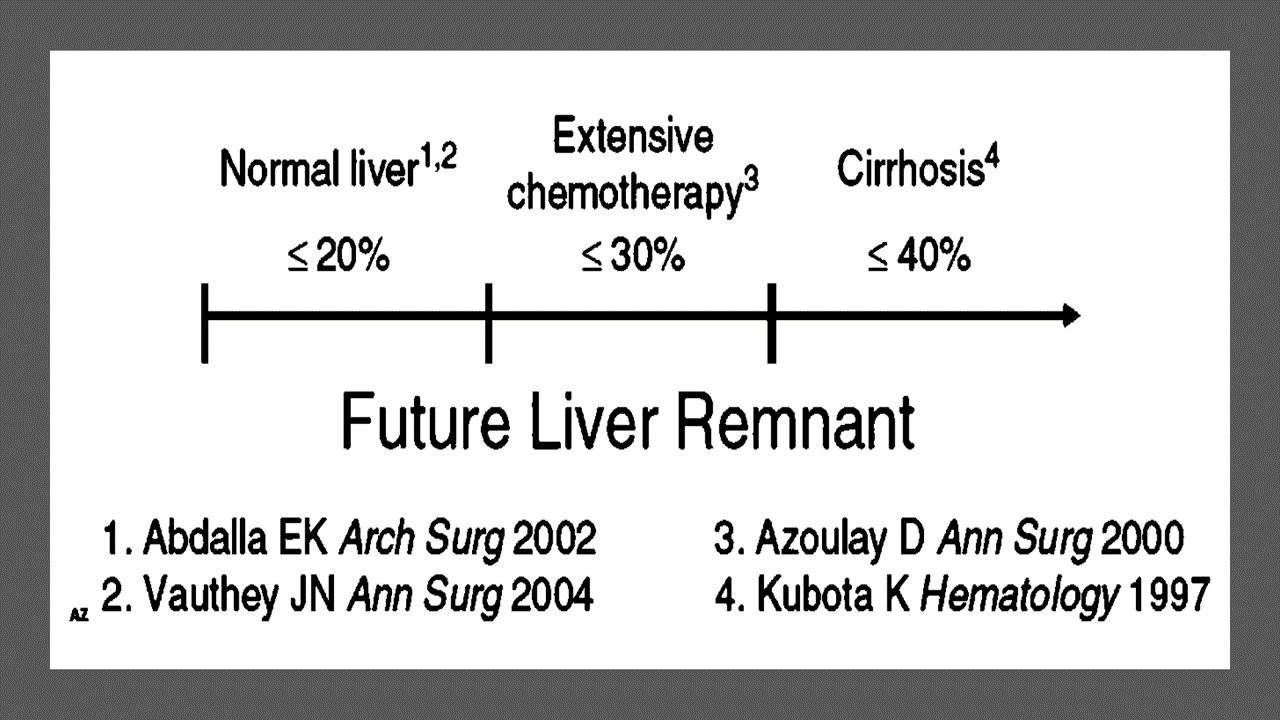
Careful analysis of outcome based on liver remnant volume stratified by underlying liver disease has led to recommendations regarding the safe limits of resection. The liver remnant to be left after resection is termed the future liver remnant (FLR). For patients with normal underlying liver, complications, extended hospital stay, admission to the intensive care unit, and hepatic insufficiency are rare when the standardized FLR is >20% of the TLV. For patients with tumor-related cholestasis or marked underlying liver disease, a 40% liver remnant is necessary to avoid cholestasis, fluid retention, and liver failure. Among patients who have been treated with preoperative systemic chemotherapy for more than 12 weeks, FLR >30% reduces the rate of postoperative liver insufficiency and subsequent mortality.
When the liver remnant is normal or has only mild disease, the volume of liver remnant can be measured directly and accurately with threedimensional computed tomography (CT) volumetry. However, inaccuracy may arise because the liver to be resected is often diseased, particularly in patients with cirrhosis or biliary obstruction. When multiple or large tumors occupy a large volume of the liver to be resected, subtracting tumor volumes from liver volume further decreases accuracy of CT volumetry. The calculated TLV, which has been derived from the association between body surface area (BSA) and liver size, provides a standard estimate of the TLV. The following formula is used:
TLV (cm3) = –794.41 + 1267.28 × BSA (square meters)
Thus, the standardized FLR (sFLR) volume calculation uses the measured FLR volume from CT volumetry as the numerator and the calculated TLV as the denominator: Standardized FLR (sFLR) = measured FLR volume/TLV Calculating the standardized TLV corrects the actual liver volume to the individual patient’s size and provides an individualized estimate of that patient’s postresection liver function. In the event of an inadequate FLR prior to major hepatectomy, preoperative liver preparation may include portal vein embolization (PVE).
Classroom: Principles of Hepatic Surgery
Surgical Management of Cholangiocarcinoma
Cholangiocarcinoma (CCA) is a rare but lethal cancer arising from the bile duct epithelium. As a whole, CCA accounts for approximately 3 % of all gastrointestinal cancers. It is an aggressive disease with a high mortality rate. Unfortunately, a significant proportion of patients with CCA present with either unresectable or metastatic disease. In a retrospective review of 225 patients with hilar cholangiocarcinoma, Jarnagin et al. reported that 29 % of patients had either unresectable disease were unfit for surgery. Curative resection offers the best chance for longterm survival. Whereas palliation with surgical bypass was once the preferred surgical procedure even for resectable disease, aggressive surgical resection is now the standard.
Classroom: Surgical Management of Cholangiocarcinoma
Strangulation in GROIN HERNIAS
Importance
Declining Mortality Rates
In both the UK and the USA, the annual death rate due to inguinal and femoral hernias has significantly decreased over the past two to three decades. In the UK, deaths from these hernias declined by 22% to 55% between 1975 and 1990. Similarly, in the USA, the annual deaths per 100,000 population for patients with hernia and intestinal obstruction decreased from 5.1 in 1968 to 3.0 in 1988. For patients with obstructed inguinal hernias, 88% underwent surgery, with a remarkably low mortality rate of 0.05%. These improvements suggest that elective groin hernia surgery has played a crucial role in reducing overall mortality rates.
Elective Surgery and Strangulation Rates
Supporting this observation, the USA has lower rates of strangulation compared to the UK, possibly due to the threefold higher rate of elective hernia surgeries in the USA. Nevertheless, statistics indicate that the rate of elective hernia surgeries in the USA per 100,000 population decreased from 358 to 220 between 1975 and 1990, although this may be an artifact of data collection rather than a genuine decline.
Mortality Analysis from UK and Denmark Studies
During 1991–1992, the UK National Confidential Enquiry Into Perioperative Deaths investigated 210 deaths following inguinal hernia repair and 120 deaths following femoral hernia repair. This inquiry, which focuses on the quality of surgery, anesthesia, and perioperative care, found that many patients were elderly (45 were aged 80–89 years) and significantly infirm; 24 were ASA grade III and 21 ASA grade IV. The majority of postoperative mortality was attributed to preexisting cardiorespiratory issues.
A nationwide study in Denmark of 158 patients who died after acute groin hernia repair by Kjaergaard et al. also found that these patients were old (median age 83 years) and frail (>80% with significant comorbidity), with frequent delays in diagnosis and treatment. These findings highlight the need for high-quality care by experienced surgeons and anesthetists, especially for patients with high ASA grades.
Postoperative Care Recommendations
Postoperative care for these patients should occur in a high-dependency unit or intensive therapy unit. This might necessitate transferring selected patients to appropriate hospitals and facilities. Decisions about interventional surgery should be made in consultation with the relatives of extremely elderly, frail, or moribund patients, adopting a humane approach that may rule out surgery.
Emergency Admissions and Prioritization
Forty percent of patients with femoral hernias are admitted as emergency cases with strangulation or incarceration, while only 3% of patients with direct inguinal hernias present with strangulation. This disparity has implications for prioritizing patients on waiting lists when these hernias present electively in outpatient clinics.
Risk of Strangulation
A groin hernia is at its greatest risk of strangulation within three months of onset. For inguinal hernias, the cumulative probability of strangulation is 2.8% at three months after presentation, rising to 4.5% after two years. The risk is much higher for femoral hernias, with a 22% probability of strangulation at three months, rising to 45% at 21 months. Right-sided hernias have a higher strangulation rate than left-sided hernias, potentially due to anatomical differences in mesenteric attachment. The decline in hernia-related mortality in both the UK and USA underscores the importance of elective hernia surgery. Ensuring timely surgery, especially for high-risk femoral hernias, and providing high-quality perioperative care for elderly and frail patients are crucial steps in further reducing mortality and improving patient outcomes.
Evidence-Based Medicine
In a randomized trial, evaluating an expectative approach to minimally symptomatic inguinal hernias, Fitzgibbons et al. in the group of patients randomized to watchful waiting found a risk of an acute hernia episode of 1.8 in 1,000 patient years. In another trial, O’Dwyer and colleagues, randomizing patients with painless inguinal hernias to observation or operation, found two acute episodes in 80 patients randomized to observation. In both studies, a large percentage of patients randomized to nonoperative care were eventually operated due to symptoms. Neuhauser, who studied a population in Columbia where elective herniorrhaphy was virtually unobtainable, found an annual rate of strangulation of 0.29% for inguinal hernias.
Management of Strangulation
The diagnosis of hernias is primarily based on clinical symptoms and signs, supplemented by imaging studies when necessary. Pain at the hernia site is a constant symptom. In cases of obstruction with intestinal strangulation, patients may present with colicky abdominal pain, distension, vomiting, and constipation. Physical examination may reveal signs of dehydration, with or without central nervous system depression, especially in elderly patients with uremia, along with abdominal signs of intestinal obstruction.
Femoral hernias can be easily missed, particularly in obese women, making a thorough physical examination essential for an accurate diagnosis. However, physical examination alone is often insufficient to confirm the presence of a strangulated femoral hernia versus lymphadenopathy or a lymph node abscess. In such cases, urgent radiographic studies, such as ultrasound or CT scan, may be necessary.
The choice of incision depends on the type of hernia if the diagnosis is clear. When there is doubt, a half Pfannenstiel incision, 2 cm above the pubic ramus extending laterally, provides adequate access to all types of femoral or inguinal hernias. The fundus of the hernia sac is exposed, and an incision is made to assess the viability of its contents. If nonviability is detected, the transverse incision should be converted into a laparotomy incision, followed by the release of the constricting hernia ring, reduction of the sac’s contents, resection, and reanastomosis. Precautions must be taken to avoid contamination of the general peritoneal cavity by gangrenous bowel or intestinal contents.
In most cases, once the constriction of the hernia ring is released, circulation to the intestine is restored, and viability returns. The intestine that initially appears dusky or non-peristaltic may regain color with a short period of warming with damp packs. If viability is doubtful, resection should be performed. Resection rates are highest for femoral or recurrent inguinal hernias and lowest for simple inguinal hernias. Other organs, such as the bladder or omentum, should be resected as needed.
After peritoneal lavage and formal closure of the laparotomy incision, specific repair of the hernia should be performed. Prosthetic mesh should not be used in a contaminated operative field due to the high risk of wound infection. Hernia repair should follow the general principles of elective hernia repair. It is important to remember that in this predominantly frail and elderly patient group with a high postoperative mortality risk, the primary objective of the operation is to stop the vicious cycle of strangulation, with hernia repair being a secondary objective.
Key Point
The risk of an acute groin hernia episode is of particular relevance, when discussing indication for operation of painless or minimally symptomatic hernias. A sensible approach in groin hernias would be, in accordance with the guidelines from the European Hernia Society to advise a male patient, that the risk of an acute operation, with an easily reducible (“disappears when lying down”) inguinal hernia with little or no symptoms, is low and that the indication for operation in this instance is not absolute, but also inform, that usually the hernia after some time will cause symptoms, eventually leading to an operation. In contrast, female patients with a groin hernia, due to the high frequency of femoral hernias and a relatively high risk of acute hernia episodes, should usually be recommended an operation.
Minimally Invasive Approach to Choledocholithiasis
Introduction
The incidence of choledocholithiasis in patients undergoing cholecystectomy is estimated to be 10 %. The presence of common bile duct stones is associated with several known complications including cholangitis, gallstone pancreatitis, obstructive jaundice, and hepatic abscess. Making the diagnosis early and prompt management is crucial. Traditionally, when choledocholithiasis is identified with intraoperative cholangiography during the cholecystectomy, it has been managed surgically by open choledochotomy and place- ment of a T-tube. This open surgical approach has a morbidity rate of 10–15 %, mortality rate of <1 %, with a <6 % incidence of retained stones. Patients who fail endoscopic retrieval of CBD stones, as well as cases in which an endoscopic approach is not appropriate, should be explored surgically.
Clinical Manifestation
Acute obstruction of the bile duct by a stone causes a rapid distension of the biliary tree and activation of local pain fibers. Pain is the most common presenting symptom for choledocholithiasis and is localized to either the right upper quadrant or to the epigastrium. The obstruction will also cause bile stasis which is a risk factor for bacterial over- growth. The bacteria may originate from the duodenum or the stone itself. The combination of biliary obstruction and colo- nization of the biliary tree will lead to the development of fevers, the second most common presenting symptom of cho- ledocholithiasis. Biliary obstruction, if unrelieved, will lead to jaundice. When these three symptoms (pain, fever, and jaundice) are found simultaneously, it is known as Charcot’s triad. This triad suggests the diagnosis of acute ascending cholangitis, a potentially life-threatening condition. If not treated promptly, this can lead to hypotension and decreased metal status, both signs of severe sepsis. When combined with Charcot’s triad, this constellation of symptoms is commonly referred to as Reynolds pentad.
Laparoscopic common bile duct exploration
Laparoscopic common bile duct exploration (LCBDE) allows for single stage treatment of gallstone disease, reducing overall hospital stay, improving safety and cost-effectiveness when compared to the two-stage approach of ERCP and laparoscopic cholecystectomy. Bile duct clearance can be confirmed by direct visualization with a choledochoscope. But, before the advent of choledochoscope, bile duct clearance was uncertain, and blind instrumentation of the duct resulted in accentuated edema and inflammation. Due to advancement in instruments, optical magnification, and direct visualization, laparoscopic exploration of the CBD results in fewer traumas to the bile duct. This has led to an increasing tendency to close the duct primarily, reducing the need for placement of T-tubes. Still, laparoscopic bile duct exploration is being done in only a few centers. Apart from the need for special instruments, there is also a significant learning curve to acquire expertise to be able to perform a laparoscopic bile duct surgery.
Morbidity and mortality rates of laparoscopic exploration are comparable to ERCP (2–17 and 1–5 %), and there is no clear difference in primary success rates between the two approaches. However, the endoscopic approach may be preferable for elderly and frail patients, who are at higher risk with surgery. Patients older than 70–80 years of age have a 4–10 % mortality rate with open duct exploration. It may be as high as 20 % in elderly patients undergoing urgent procedures. In comparison, advanced age and comor- bidities do not have a significant impact on overall complication rates for ERCP. A success rate of over 90 % has been reported with laparoscopic CBD exploration. Availability of surgical expertise and appropriate equipment affect the success rate of laparoscopic exploration, as does the size, number of the CBD stones, as well as biliary anatomy. Over the years, laparoscopic exploration has become efficient, safe, and cost effective. Complications include CBD laceration, stricture formation, bile leak, abscess, pancreatitis, and retained stones.
In cases of failure of laparoscopic CBD exploration, a guidewire or stent can be passed through the cystic duct, common bile duct, and through the ampulla into the duodenum followed by cholecystectomy. This makes the identification and cannulation of the ampulla easier during the post- operative ERCP. Laparoscopic common bile duct exploration is traditionally performed through a transcystic or transductal approach. The transcystic approach is appropriate under certain circumstances. These include a small stone (<10 mm) located in the CBD, presence of small common bile duct (<6 mm), or if there is poor access to the common duct. The transductal approach is preferable in cases of large stones, stones in proximal ducts (hepatic ducts), large occluding stones in a large duct, presence of multiple stones, or if the cystic duct is small (<4 mm) or tortuous. Contraindications for laparoscopic approach include lack of training, and severe inflammation in the porta hepatis making the exploration difficult and risky.
Key Points
With advancement in imaging technology, laparoscopic and endoscopic techniques, management of common bile duct stone has changed drasti- cally in recent years. This has made the treatment of this condition safe and more efficient. Many options are now available to manage this condition, and any particular modality for treatment should be chosen carefully based on the patient related factors, institutional protocol, available expertise, resources, and cost-effectiveness.
Classroom: M.I.A. of Choledocholithiasis
IPMN Surgical Management

INTRODUCTION
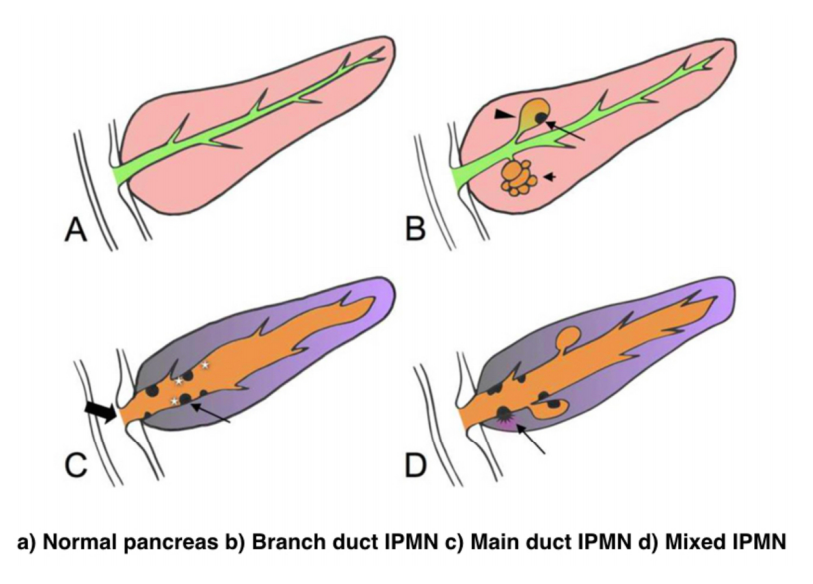
IPMNs were first recognized in 1982 by Ohashi, but the term IPMN was not officially used until 1993. IPMNs are defined in the WHO Classification of Tumors of the Digestive System as an intraductal, grossly visible epithelial neoplasm of mucin-producing cells. Using imaging and histology, IPMNs can be classified into three types based on duct involvement:
1. Main-duct IPMN (approximately 25% of IPMNs): Segmental or diffuse dilation of the main pancreatic duct (>5 mm) in the absence of other causes of ductal obstruction.
2. Branch-duct IPMN (approximately 57% of IPMNs): Pancreatic cysts (>5 mm) that communicate with the main pancreatic duct.
3. Mixed type IPMN (approximately 18% of IPMNs): Meets criteria for both main and branch duct.
Due to the asymptomatic nature of the disease, the overall incidence of IPMNs is difficult to define but is thought to account for approximately 3% to 5% of all pancreatic tumors. Most IPMNs are discovered as incidental lesions from the workup of an unrelated process by imaging or endoscopy. IPMNs are slightly more prevalent in males than in females, with a peak incidence of 60 to 70 years of age. Branch-duct IPMNs tend to occur in a slightly younger population and are less associated with malignancy compared with main-duct or mixed variants.
Because a majority of IPMNs are discovered incidentally, most are asymptomatic. When symptoms do occur, they tend to be nonspecific and include unexplained weight loss, anorexia, abdominal pain, and back pain. Jaundice can occur with mucin obstructing the ampulla or with an underlying invasive carcinoma. The obstruction of the pancreatic duct can also lead to pancreatitis. IPMNs may represent genomic instability of the entire pancreas. This concept, known as a “field defect,” has been described as a theoretical risk of developing a recurrent IPMN or pancreatic adenocarcinoma at a site remote from the original IPMN. The three different types of IPMNs, main duct, branch duct, and mixed duct, dictate different treatment algorithms.
MAIN DUCT IPMNs
Main-duct IPMNs should be resected in all patients unless the risks of existing comorbidities outweigh the benefits of resection. The goal of operative management of IPMNs is to remove all adenomatous or potentially malignant epithelium to minimize recurrence in the pancreas remnant. There are two theories on the pathophysiologic basis of IPMNs. The first groups IPMNs into a similar category as an adenocarcinoma, a localized process involving only a particular segment of the pancreas. The thought is that removal of the IPMN is the only treatment necessary. In contrast, some believe IPMNs to represent a field defect of the pancreas. All of the ductal epithelium remains at risk of malignant degeneration despite removal of the cyst. Ideally, a total pancreatectomy would eliminate all risk, but this is a radical procedure that is associated with metabolic derangements and exocrine insufficiency. Total pancreatectomy should be limited to the most fit patients, with a thorough preoperative assessment and proper risk stratification prior to undertaking this surgery.
There is less uncertainty with treatment of main-duct IPMNs. The high incidence of underlying malignancy associated with the IPMNs warrants surgical resection. IPMNs localized to the body and tail (approximately 33%) can undergo a distal pancreatectomy with splenectomy. At the time of surgery, a frozen section of the proximal margin should be interpreted by a pathologist to rule out high-grade dysplasia. A prospective study identified a concordance rate of 94% between frozen section and final pathologic examination. If the margin is positive (high-grade dysplasia, invasion) additional margins may be resected from the pancreas until no evidence of disease is present. However, most surgeons will proceed to a total pancreatectomy after two subsequent margins demonstrate malignant changes. This more extensive procedure should be discussed with the patient prior to surgery, and the patient should be properly consented regarding the risks of a total pancreatectomy.
IPMNs localized to the head or uncinate process of the pancreas should undergo a pancreaticoduodenectomy. A frozen section of the distal margin should be analyzed by pathology for evidence of disease. As mentioned before, after two additional margins reveal malignant changes, a total pancreatectomy is usually indicated (approximately 5%). The absence of abnormal changes in frozen sections does not equate to negative disease throughout the pancreas remnant. Rather, skip lesions involving the remainder of the pancreas can exist and thus patients ultimately still require imaging surveillance after successful resection. A prophylactic total pancreatectomy is rarely performed because the subsequent pancreatic endocrine (diabetes mellitus) and exocrine deficits (malnutrition) carry an increased morbidity.
BRANCH DUCT IPMNs
Localized branch-duct IPMN can be treated with a formal anatomic pancreatectomy, pancreaticoduodenectomy, or distal pancreatectomy, depending on the location of the lesion. However, guidelines were established that allow for nonoperative management with certain branch- type IPMN characteristics.
These include asymptomatic patients with a cyst size less than 3 cm and lack of mural nodules. The data to support this demonstrate a very low incidence of malignancy (approximately 2%) in this patient group. Which nearly matches the anticipated mortality of undergoing a formal anatomic resection. In approximately 20% to 30% of patients with branch- duct IPMNs, there is evidence of multifocality. The additional IPMNs can be visualized on high-resolution CT or MRI imaging. Ideally, patients with multifocal branch-duct IPMNs should undergo a total pancreatectomy. However, as previously mentioned, the increased morbidity and lifestyle alterations associated with a total pancreatectomy allows for a more conservative approach. This would include removing the most suspicious or dominant of the lesions in an anatomic resection and follow-up imaging surveillance of the remaining pancreas remnant. If subsequent imaging demonstrates malignant charac- teristics, a completion pancreatectomy is usually indicated.
RECURRENCE RATES
Recurrence rates with IPMNs are variable. An anatomic resection of a branch-duct IPMN with negative margins has been shown to be curative. The recurrence of a main- duct IPMN in the remnant gland is anywhere from 0% to 10% if the margins are negative and there is no evidence of invasion. Most case series cite a 5-year survival rate of at least 70% after resection of noninvasive IPMNs. In contrast, evidence of invasive disease, despite negative margins, decreases 5-year survival to 30% to 50%. The recurrence rate in either the pancreatic remnant or distant sites approaches 50% to 90% in these patients. Histopathologic subtype of the IPMN is correlated with survival. The aggressive tubular subtype has a 5-year survival ranging from 37% to 55% following surgical resection, whereas the colloid subtype has 5-year survival ranging from 61% to 87% post resection. Factors associated with decreased survival include tubular subtype, lymph node metastases, vascular invasion, and positive margins. IPMNs with evidence of invasion should be treated similar to pancreatic adenocarcinomas. Studies show that IPMNs tend to have better survival than pancreatic adenocarcinoma. This survival benefit may be secondary to the less aggressive tumor biology or the earlier diagnosis of IPMNs.
SURVEILLANCE
All patients who have a resected IPMN should undergo imaging surveillance. There is continual survival benefit with further resection if an IPMN does recur. International Consensus Guidelines published in 2017 offer recom- mendations for the frequency and modality of imaging surveillance after resection. Routine serum measurement of CEA and CA 19-9 has a limited role for detection of an IPMN recurrence. Of note, a new pancreatic lesion discovered on imaging after resection could represent a postoperative pseudocyst, a recurrence of the IPMN from inadequate resection, a new IPMN, or an unrelated new neoplastic process. IPMNs may also be associated with extrapancreatic neoplasms (stomach, colon, rectum, lung, breast) and pancreatic ductal adenocarcinoma. It is unclear if this represents a true genetic syndrome. However, patients with IPMNs should have a discussion about the implications of their disease with their physician and are encouraged to undergo colonoscopy to exclude a synchronous neoplastic process.
The incidence of PANCREATIC CYSTIC LESIONS will continue to increase as imaging technology improves. EUS, cytology, and molecular panels have made differentiating the type of PCN less problematic. The importance of an accurate preoperative diagnosis ensures that operative management is selectively offered to those with high-risk lesions. Management beyond surgery, including adjuvant therapy and surveillance, continue to be active areas of research.
The century of THE SURGEONS
Surgery is a profession defined by its authority to cure by means of bodily invasion. The brutality and risks of opening a living person’s body have long been apparent, the benefits only slowly and haltingly worked out. Nonetheless, over the past two centuries, surgery has become radically more effective, and its violence substantially reduced — changes that have proved central to the development of mankind’s abilities to heal the sick.
Consider, for instance, amputation of the leg.
The procedure had long been recognized as lifesaving, in particular for compound fractures and other wounds prone to sepsis, and at the same time horrific. Before the discovery of anesthesia, orderlies pinned the patient down while an assistant exerted pressure on the femoral artery or applied a tourniquet on the upper thigh.
Surgeons using the circular method proceeded through the limb in layers, taking a long curved knife in a circle through the skin first, then, a few inches higher up, through the muscle, and finally, with the assistant retracting the muscle to expose the bone a few inches higher still, taking an amputation saw smoothly through the bone so as not to leave splintered protrusions. Surgeons using the flap method, popularized by the British surgeon Robert Liston, stabbed through the skin and muscle close to the bone and cut swiftly through at an oblique angle on one side so as to leave a flap covering the stump.
The limits of patients’ tolerance for pain forced surgeons to choose slashing speed over precision. With either the flap method or the circular method, amputation could be accomplished in less than a minute, though the subsequent ligation of the severed blood vessels and suturing of the muscle and skin over the stump sometimes required 20 or 30 minutes when performed by less experienced surgeons.
No matter how swiftly the amputation was performed, however, the suffering that patients experienced was terrible. Few were able to put it into words. Among those who did was Professor George Wilson. In 1843, he underwent a Syme amputation — ankle disarticulation — performed by the great surgeon James Syme himself. Four years later, when opponents of anesthetic agents attempted to dismiss them as “needless luxuries,” Wilson felt obliged to pen a description of his experience:
“The horror of great darkness, and the sense of desertion by God and man, bordering close on despair, which swept through my mind and overwhelmed my heart, I can never forget, however gladly I would do so. During the operation, in spite of the pain it occasioned, my senses were preternaturally acute, as I have been told they generally are in patients in such circumstances. I still recall with unwelcome vividness the spreading out of the instruments: the twisting of the tourniquet: the first incision: the fingering of the sawed bone: the sponge pressed on the flap: the tying of the blood-vessels: the stitching of the skin: the bloody dismembered limb lying on the floor.”
It would take a little while for surgeons to discover that the use of anesthesia allowed them time to be meticulous. Despite the advantages of anesthesia, Liston, like many other surgeons, proceeded in his usual lightning-quick and bloody way. Spectators in the operating-theater gallery would still get out their pocket watches to time him. The butler’s operation, for instance, took an astonishing 25 seconds from incision to wound closure. (Liston operated so fast that he once accidentally amputated an assistant’s fingers along with a patient’s leg, according to Hollingham. The patient and the assistant both died of sepsis, and a spectator reportedly died of shock, resulting in the only known procedure with a 300% mortality.)
The Surgical Personality

Surgical stereotypes are remnants of the days of pre-anaesthesia surgery and include impulsivity, narcissism, authoritativeness, decisiveness, and thinking hierarchically. Medical students hold these stereotypes of surgeons early in their medical training. As Pearl Katz says in the The Scalpel’s Edge: ‘Each generation perpetuates the culture and passes it on by recruiting surgical residents who appear to resemble them and training these residents to emulate their thinking and behaviour.’ The culture of surgery has evolved, and certain behaviours are rightly no longer seen as acceptable, Non-technical skills such as leadership and communication have become incorporated into surgical training. Wen Shen, Associate Professor of Clinical Surgery at University of California San Francisco, argues that this has gone too far: ‘Putting likeability before surgical outcomes is like judging a restaurant by the waiters and ignoring the food,’ I would argue that operative and communication skills are indivisible, An aggressive surgeon is a threat to patient safety if colleagues are frightened to speak up for fear of a colleague shouting or, worse, throwing instruments. Conversely, a flattened hierarchy promotes patient safety.
Read More
Article: The Surgical Personality
The “GOOD” Surgeon
Surgery is an extremely enjoyable, intellectually demanding and satisfying career, and many more people apply to become surgeons each year than there are available places.
Those who are successful have to be ready not just to learn a great deal, but have the right kind of personality for the job.
Is a surgical career right for you?
Read the link…
THE GOOD SURGEON
Modern Concepts of Pancreatic Surgery
 Operations on the gallbladder and bile ducts are among the surgical procedures most commonly performed by general surgeons. In most hospitals, cholecystectomy is the most frequently performed operation within the abdomen. Pancreatic surgery is less frequent , but because of the close relation between the biliary system and the pancreas, knowledge of pancreatic problems is equally essential to the surgeon. Acute and chronic pancreatitis and cancer of the pancreas are often encountered by surgeons, with apparently increasing frequency; their treatment remains difficult and perplexing. This review demonstrates the modern aspects of pancreatic surgery. Good study.
Operations on the gallbladder and bile ducts are among the surgical procedures most commonly performed by general surgeons. In most hospitals, cholecystectomy is the most frequently performed operation within the abdomen. Pancreatic surgery is less frequent , but because of the close relation between the biliary system and the pancreas, knowledge of pancreatic problems is equally essential to the surgeon. Acute and chronic pancreatitis and cancer of the pancreas are often encountered by surgeons, with apparently increasing frequency; their treatment remains difficult and perplexing. This review demonstrates the modern aspects of pancreatic surgery. Good study.
AULA: PRÍNCIPIOS MODERNOS DA CIRURGIA PANCREÁTICA
Palestras e Vídeoaulas
Vejam nos links a seguir algumas de nossas palestras disponíveis para download no Canal do SlideShare e Videoaulas presentes no You Tube.
O TEMPLO DO CIRURGIÃO.

BLOCO CIRÚRGICO: O TEMPLO DO CIRURGIÃO.
Templo (do latim templum, “local sagrado”) é uma estrutura arquitetônica dedicada ao serviço religioso. O termo também pode ser usado em sentido figurado. Neste sentido, é o reflexo do mundo divino, a habitação de Deus sobre a terra, o lugar da Presença Real. É o resumo do macrocosmo e também a imagem do microcosmo: ‘o corpo é o templo do Espírito Santo’ (I, Coríntios, 6, 19).
Dos locais especiais, O corpo humano (morada da alma), a Cavidade Peritoneal e o Bloco Cirúrgico, se bem analisados, são muito semelhantes e merecem atitudes e comportamentos respeitáveis. O Templo, em todos os credos, induz à meditação, absoluto silêncio tentando ouvir o Ser Supremo. A cavidade peritoneal | abdominal , espaço imaculado da homeostase, quando injuriada, reage gritando em dor, implorando uma precoce e efetiva ação terapêutica.
O Bloco Cirúrgico, abrigo momentâneo do indivíduo solitário, que mudo e quase morto de medo, recorre à prece implorando a troca do acidente, da complicação, da recorrência, da seqüela, da mutilação, da iatrogenia e do risco de óbito pela agressiva e controlada intervenção que lhe restaure a saúde, patrimônio magno de todo ser vivo.
O Bloco Cirúrgico clama por respeito ao paciente cirúrgico, antes mesmo de ser tomado por local banal, misturando condutas vulgares, atitudes menores, desvio de comportamento e propósitos secundários. Trabalhar no Bloco Cirúrgico significa buscar a perfeição técnica, revivendo os ensinamentos de William Stewart Halsted , precursor da arte de operar, dissecando para facilitar, pinçando e ligando um vaso sangüíneo, removendo tecido macerado, evitando corpos estranhos e reduzindo espaço vazio, numa síntese feita com a ansiedade e vontade da primeira e a necessidade e experiência da última.
Mas, se a cirurgia e o cirurgião vêm sofrendo grande evolução, técnica a primeira e científica o segundo, desde o início do século, a imagem que todo doente faz persiste numa simbiose entre mitos e verdades. A cirurgia significa enfrentar ambiente desconhecido chamado “sala de cirurgia” onde a fobia ganha espaço rumo ao infinito. O medo ainda prepondera em muitos.
A confiança neste momento além de um reconhecimento é um troféu que o cirurgião recebe dos pacientes e seus familiares. Tanto a CONFIANÇA quanto a SEGURANÇA têm que ser preservadas a qualquer custo. Não podem correr o risco de serem corroídas por palavras e atitudes de qualquer membro da equipe cirúrgica. Não foi tarefa fácil transformar, para a população, o ato cirúrgico numa atividade científica, indispensável, útil e por demais segura. Da conquista da cirurgia, como excelente arma terapêutica para a manutenção de um alto padrão de qualidade técnica, resta a responsabilidade dos cirurgiões, os herdeiros do suor e sangue, que se iniciou com o trabalho desenvolvido por Billroth, Lister, Halsted, Moyniham, Kocher e uma legião de figuras humanas dignas do maior respeito, admiração e gratidão universal.
No ato operatório os pacientes SÃO TODOS SEMELHANTES EM SUAS DIFERENÇAS, desde a afecção, ao prognóstico, ao caráter da cirurgia e especialmente sua relação com o ato operatório. Logo, o cirurgião tem por dever de ofício entrar no bloco cirúrgico com esperança e não deve sair com dúvida. Nosso trabalho é de equipe, cada um contribui com uma parcela, maior ou menor, para a concretização do todo, do ato cirúrgico por completo, com muita dedicação, profissionalismo e sabedoria. Toda tarefa, da limpeza do chão ao ato de operar, num crescendo, se faz em função de cada um e em benefício da maioria, o mais perfeito possível e de uma só vez, quase sempre sem oportunidade de repetição e previsão de término.
O trabalho do CIRURGIÃO é feito com carinho, muita dignidade, humildade e executado em função da alegria do resultado obtido aliado a dimensão ética do dever cumprido que transcende a sua existência. A vida do cirurgião se materializa no ato operatório e o bloco cirúrgico, palco do nosso trabalho não tolera e jamais permite atitudes menores, inferiores, ambas prejudiciais a todos os pacientes e a cada cirurgião. Como ambiente de trabalho de uma equipe diversificada, precisamos manter, a todo custo, o controle de qualidade, eficiência, eficácia e efetividade técnina associados aos mais altos valores ético, pois lidamos com o que há de mais precioso da criação divina na Terra: O SER HUMANO.
“Tem presença de Deus, como já a tens. Ontem estive com um doente, um doente a quem quero com todo o meu coração de Pai, e compreendo o grande trabalho sacerdotal que os médicos levam a cabo. Mas não se ponham orgulhosos, porque todas as almas são sacerdotais. Devem pôr em prática esse sacerdócio! Ao lavares as mãos, ao vestires a bata, ao calçares as luvas, pensa em Deus, e pensa nesse sacerdócio real de que fala São Pedro, e então não se te meterá a rotina: farás bem aos corpos e às almas” São Josemaria Escriva
Bariatric Complications

Over the past decade, following the publication of several long-term outcome studies that showed a significant improvement in cardiovascular risk and mortality after bariatric surgery, the number of bariatric procedures being carried out annually in the UK has grown exponentially. Surgery remains the only way to produce significant, sustainable weight loss and resolution of comorbidities. Nevertheless, relatively few surgeons have developed an interest in this field. Most bariatric surgery is now performed in centres staffed by surgeons with a bariatric interest, usually as part of a multidisciplinary team.
The commonest weight loss procedures performed around the world at present are the gastric band, the gastric bypass and the sleeve gastrectomy. In very obese patients, an alternative operation is the duodenal switch, while the new ileal transposition procedure represents one of the few purely metabolic operations designed specifically for the treatment of type II diabetes. Older operations such as vertical banded gastroplasty and jejuno-ileal bypass are now obsolete, although patients who have undergone such procedures in the distant past may still present to hospital with complications. The main endoscopic option at present is insertion of a gastric balloon, with newer procedures like the endoscopic duodenojejunal barrier and gastric plication on the horizon. Implantable neuroregulatory devices (gastric ‘pacemakers’) represent a new direction for surgical weight control by harnessing neural feedback signals to help control eating.
It should be within the capability of any abdominal surgeon to manage the general complications of bariatric surgery, which include pulmonary atelectasis/pneumonia, intra-abdominal bleeding, anastomotic or staple-line leak with or without abscess formation, deep vein thrombosis (DVT)/pulmonary embolus and superficial wound infections. Patients may be expected to present with malaise, pallor, features of sepsis or obvious wound problems. However, clinical features may be difficult to recognise owing to body habitus. Abdominal distension, tenderness and guarding may be impossible to determine clinically due to the patient’s obesity. Pallor is non-specific. Fever and leucocytosis may be absent. Wound collections may be very deep. These complications in a bariatric patient should be actively sought with appropriate investigations. In particular, it is vital for life-threatening complications such as bleeding, sepsis and bowel obstruction to be recognised promptly and treated appropriately. A persistent tachycardia may be the only sign heralding significant complications and should always be taken seriously. It is useful to classify complications as ‘early’, ‘medium’ and ‘late’ because, from the receiving clinician’s point of view, the differential diagnosis will differ accordingly.
Complications of bariatric surgery presenting to the GENERAL SURGEON
A “PROFISSÃO” CIRÚRGICA
 “A arte de curar vem do coração e da mente mais do que das mãos.” – Hipócrates
“A arte de curar vem do coração e da mente mais do que das mãos.” – Hipócrates

Na complexa tapeçaria da sociedade moderna, as profissões desempenham papéis fundamentais na organização dos serviços necessários ao bem-estar coletivo. Definida pelo American College of Surgeons, uma profissão é um campo onde a maestria de um corpo complexo de conhecimento e habilidades é essencial. É uma vocação em que o conhecimento científico ou a prática de uma arte, fundamentada nesse conhecimento, é empregada em benefício dos outros. O compromisso com a competência, a integridade e a moralidade forma a base de um contrato social entre a profissão e a sociedade, que concede à profissão um monopólio sobre o uso de seu conhecimento, considerável autonomia na prática e o privilégio da auto-regulação. Em troca, a profissão deve prestar contas a quem serve e à sociedade como um todo.
Os Elementos Essenciais da Profissão
No cerne de toda profissão estão quatro elementos fundamentais:
- Monopólio do Conhecimento Especializado: Profissionais detêm o direito exclusivo de utilizar conhecimentos e habilidades especializados, o que lhes confere uma posição única na sociedade.
- Autonomia e Auto-Regulação: Em troca deste monopólio, profissionais desfrutam de uma relativa autonomia na prática e são responsáveis pela sua própria regulação.
- Serviço Altruísta: A profissão deve servir tanto indivíduos quanto a sociedade de forma altruísta, colocando o bem-estar do paciente acima de outros interesses.
- Responsabilidade pela Manutenção e Expansão do Conhecimento: Profissionais são responsáveis por atualizar e expandir continuamente seu conhecimento e habilidades.
O Que é Profissionalismo?
Profissionalismo descreve as qualidades cognitivas, morais e colegiais de um profissional. É o conjunto de razões pelas quais um pai se orgulha de dizer que seu filho é um médico e cirurgião. Profissionalismo é mais do que apenas conhecimento técnico; é uma combinação de ética, respeito e dedicação ao ofício e ao paciente.
Por Que Precisamos de um Código de Conduta Profissional?
A confiança é o alicerce da prática cirúrgica. O Código de Conduta Profissional esclarece a relação entre a profissão cirúrgica e a sociedade que serve, frequentemente referido como contrato social. Para os pacientes, o código cristaliza o compromisso da comunidade cirúrgica em relação aos indivíduos e suas comunidades. A confiança é construída, tijolo por tijolo.
O Código de Conduta Profissional
O Código de Conduta Profissional aplica os princípios gerais do profissionalismo à prática cirúrgica e serve como a fundação sobre a qual os privilégios profissionais e a confiança dos pacientes e do público são conquistados. Durante o cuidado pré-operatório, intraoperatório e pós-operatório, os cirurgiões têm a responsabilidade de:
- Advogar Eficazmente pelos interesses dos pacientes.
- Divulgar Opções Terapêuticas incluindo seus riscos e benefícios.
- Divulgar e Resolver Conflitos de Interesse que possam influenciar as decisões de cuidado.
- Ser Sensível e Respeitoso com os pacientes, compreendendo sua vulnerabilidade durante o período perioperatório.
- Divulgar Completamente Eventos Adversos e Erros Médicos.
- Reconhecer Necessidades Psicológicas, Sociais, Culturais e Espirituais dos pacientes.
- Incorporar Cuidados Especiais para Pacientes Terminais.
- Reconhecer e Apoiar as Necessidades das Famílias dos Pacientes.
- Respeitar o Conhecimento, Dignidade e Perspectiva de outros profissionais de saúde.
A Necessidade do Código de Profissionalismo para Cirurgiões
Procedimentos cirúrgicos são experiências extremas que impactam os pacientes fisiológica, psicológica e socialmente. Quando os pacientes se submetem a uma experiência cirúrgica, devem confiar que o cirurgião colocará seu bem-estar acima de todas as outras considerações. O código escrito ajuda a reforçar esses valores, garantindo que a confiança e o compromisso sejam mantidos.
Princípios Fundamentais do Código de Conduta Profissional
- Primazia do Bem-Estar do Paciente: Os interesses do paciente sempre devem vir em primeiro lugar. O altruísmo é central para esse conceito, e é o altruísmo do cirurgião que fomenta a confiança na relação médico-paciente.
- Autonomia do Paciente: Pacientes devem entender e tomar suas próprias decisões informadas sobre o tratamento. Os médicos devem ser honestos para que os pacientes façam escolhas educadas, garantindo que essas decisões estejam alinhadas com práticas éticas.
- Justiça Social: Como médicos, devemos advogar pelos pacientes individuais enquanto promovemos a saúde do sistema de saúde como um todo. Precisamos equilibrar as necessidades dos pacientes (autonomia) sem desviar recursos escassos que beneficiariam a sociedade (justiça social).
“Não há maior coisa a ser conquistada do que a confiança dos pacientes e da sociedade, pois ela é a base sobre a qual construímos nossas práticas e nossa profissão.” – William Osler
Tratamento Cirúrgico da Hemorragia digestiva alta por varizes esofágicas | Hipertensão Porta
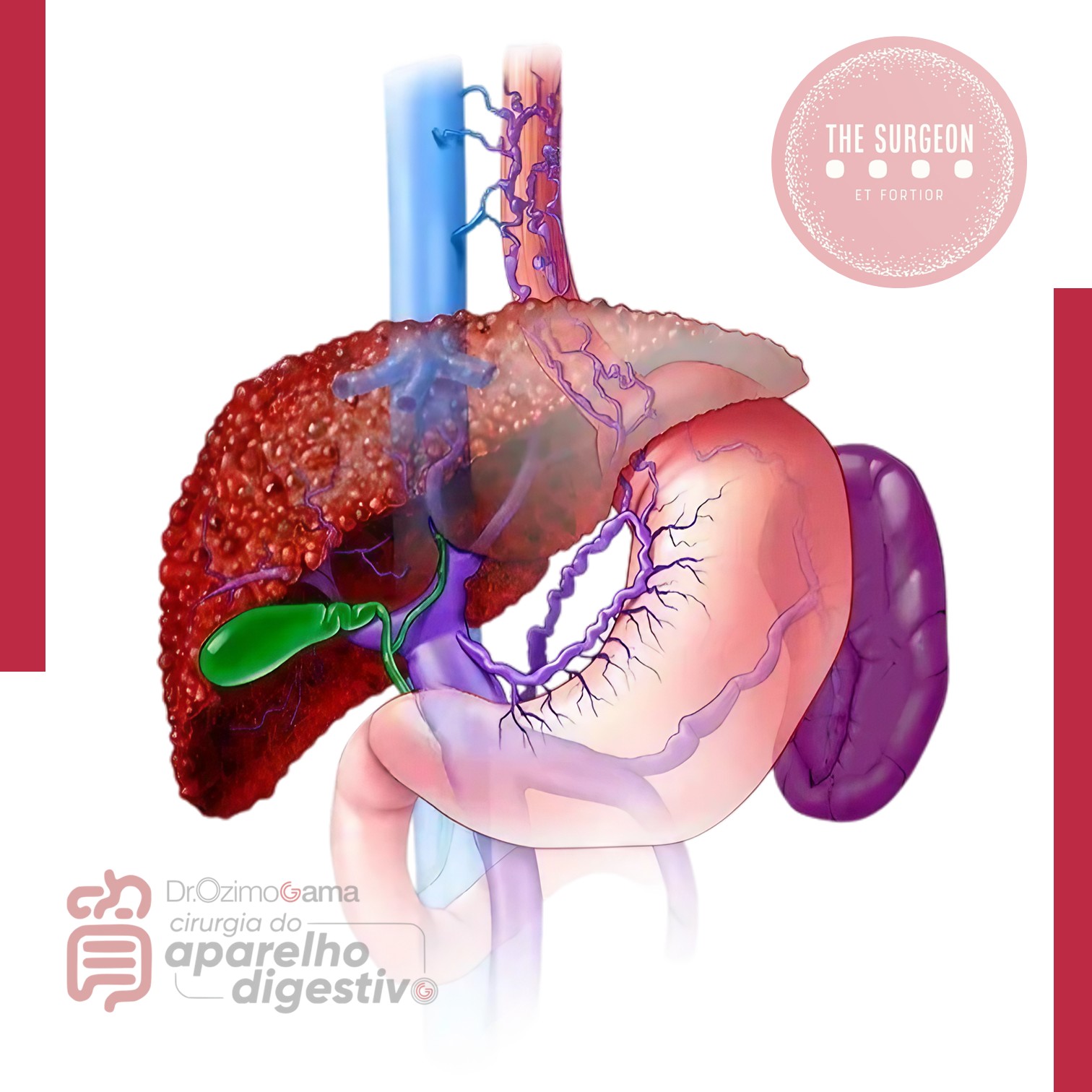
Introdução
A hipertensão portal é uma das principais complicações das doenças hepáticas crônicas e representa um dos maiores desafios da cirurgia do aparelho digestivo. Define-se classicamente como um aumento do gradiente de pressão portossistêmico acima de 5 mmHg, sendo clinicamente significativo quando ultrapassa 10–12 mmHg, nível a partir do qual surgem varizes gastroesofágicas e risco de hemorragia digestiva alta.
A cirrose hepática responde por cerca de 90% dos casos de hipertensão portal no mundo, sendo também a principal etiologia no Brasil. Estima-se que aproximadamente 50–60% dos pacientes cirróticos desenvolvem varizes esofágicas, e cerca de 30% destes apresentarão episódio de sangramento varicoso ao longo da vida.
Apesar dos avanços na terapia endoscópica e farmacológica, o tratamento cirúrgico da hipertensão portal permanece uma ferramenta essencial em casos selecionados, particularmente quando ocorre falha terapêutica ou quando há indicações específicas relacionadas à etiologia e à função hepática do paciente.
Neste artigo de educação médica continuada revisaremos os principais aspectos do tratamento cirúrgico da hipertensão portal, com foco em indicações, resultados comparativos entre técnicas e implicações na prática atual da cirurgia digestiva.
ARTIGO DE REVISÃO – HIPERTENSÃO PORTAL
Fisiopatologia da Hipertensão Portal
A hipertensão portal resulta do aumento da resistência ao fluxo portal associado ou não ao aumento do fluxo sanguíneo esplâncnico. Os mecanismos principais incluem:
- Aumento da resistência intra-hepática
- fibrose e distorção arquitetural na cirrose
- compressão sinusoidal
- disfunção endotelial hepática
- Aumento do fluxo portal
- vasodilatação esplâncnica mediada por óxido nítrico
- Formação de circulação colateral portossistêmica
- desenvolvimento de varizes esofagogástricas
- shunts espontâneos
As principais manifestações clínicas incluem:
- hemorragia digestiva alta por varizes
- ascite
- encefalopatia hepática
- hiperesplenismo
O tratamento cirúrgico visa reduzir a pressão portal ou interromper o fluxo varicoso, prevenindo novos episódios hemorrágicos.
Indicações do Tratamento Cirúrgico
Com o advento da ligadura elástica endoscópica, da terapia farmacológica vasoativa e do TIPS, as indicações cirúrgicas tornaram-se mais restritas. Atualmente, as principais indicações incluem:
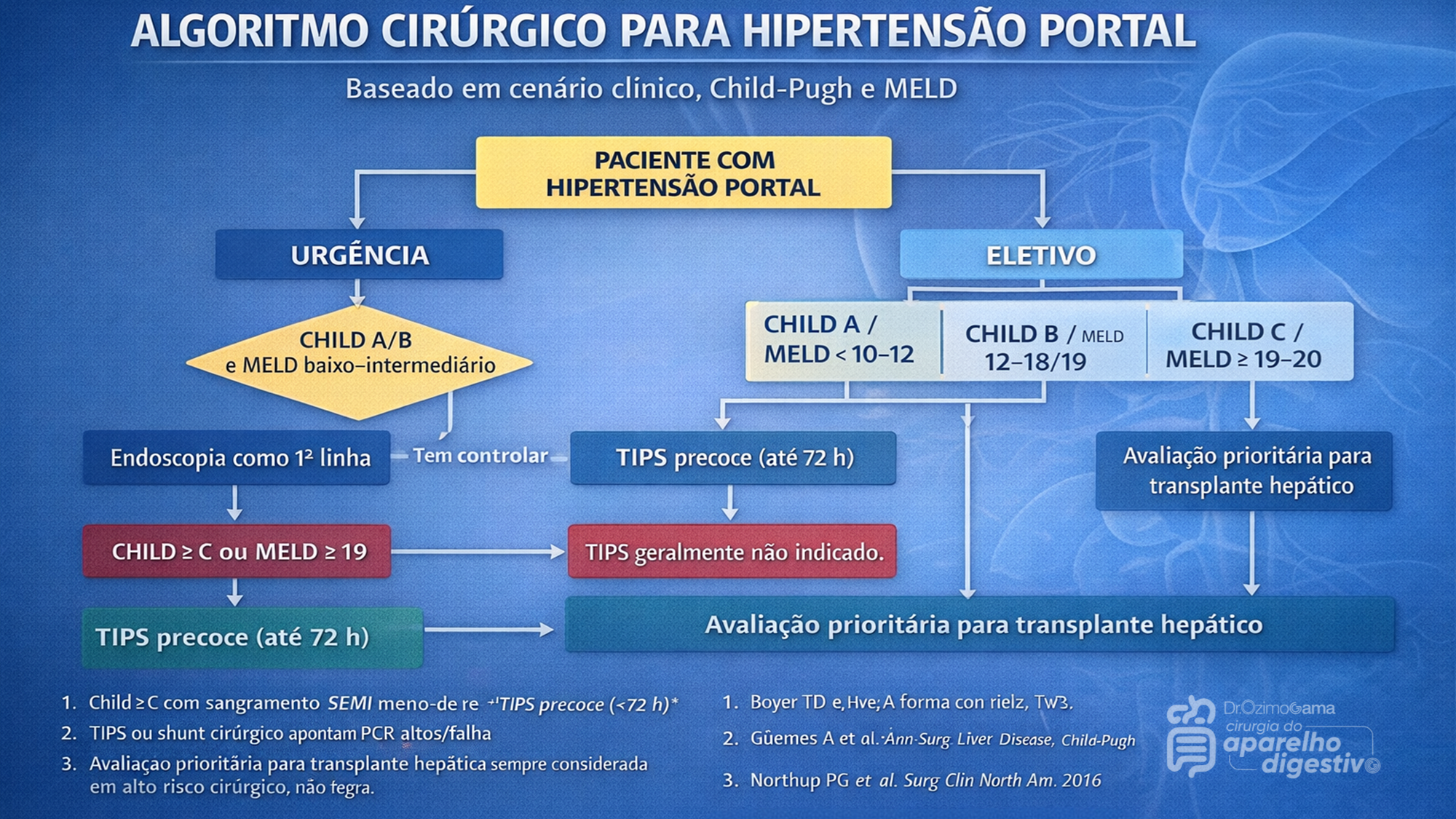
A indicação cirúrgica atual exige a aplicação rigorosa de escores prognósticos, notadamente o Child-Pugh e o MELD. Pacientes Child-Pugh A (MELD < 10 a 15) possuem baixo risco cirúrgico, sendo candidatos ideais para cirurgias eletivas, incluindo shunts e desvascularização. Por outro lado, pacientes descompensados (Child-Pugh C ou MELD > 19-20) apresentam alto risco de mortalidade pós-operatória, inclusive pós-TIPS, sendo o transplante hepático a via mandatória. O grande desafio recai sobre os pacientes limítrofes (Child-Pugh B ou MELD 15-19). Neste estrato de risco intermediário, shunts cirúrgicos tendem a oferecer maior sobrevida a longo prazo para aqueles com função hepática estável, enquanto o TIPS demonstra maior benefício na sobrevida de pacientes com ascite refratária ou sangramento agudo.
AULA: TRATAMENTO CIRÚRGICO DA HIPERTENSÃO PORTAL
Na prática contemporânea da cirurgia hepatobiliar, o manejo da hipertensão portal é multidisciplinar, envolvendo:
- hepatologistas
- endoscopistas
- radiologistas intervencionistas
- cirurgiões digestivos
O algoritmo terapêutico atual pode ser resumido da seguinte forma:
- Primeira linha
- terapia farmacológica
- ligadura elástica endoscópica
- Falha terapêutica
- TIPS
- Pacientes selecionados
- shunt cirúrgico
- desvascularização
- Doença hepática avançada
- transplante hepático
O cirurgião digestivo continua desempenhando papel fundamental, sobretudo em centros terciários e unidades de referência hepatobiliar.
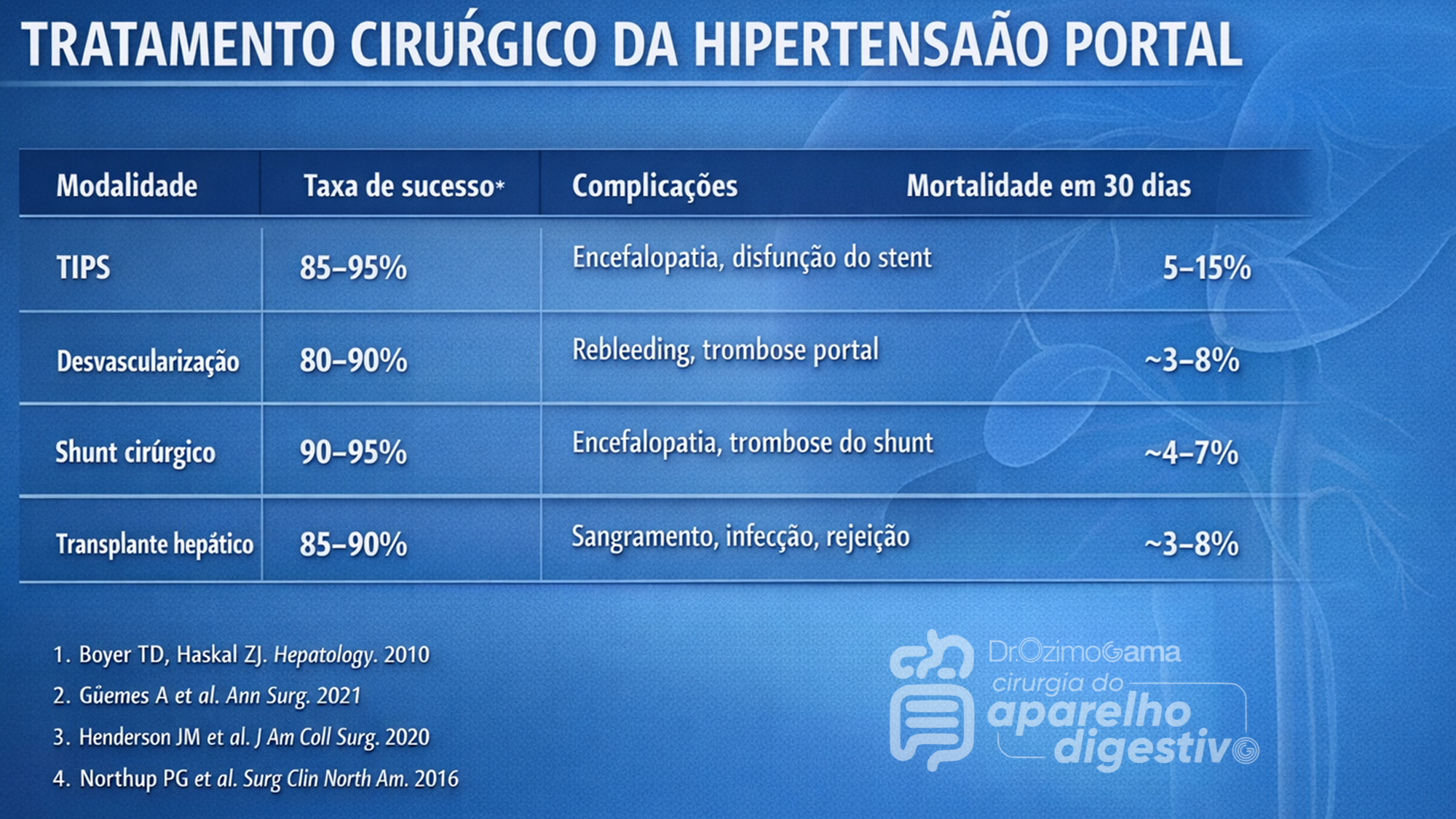
Pontos-chave para o Cirurgião Digestivo
- A hipertensão portal clinicamente significativa ocorre com gradiente >10–12 mmHg
- O sangramento varicoso continua sendo a complicação mais grave
- TIPS é hoje a principal estratégia de resgate após falha endoscópica
- Shunts cirúrgicos permanecem relevantes em pacientes selecionados
- A desvascularização gastroesofágica ainda possui papel importante na esquistossomose
- Transplante hepático é o único tratamento curativo da hipertensão portal associada à cirrose
Conclusão
Embora os avanços na radiologia intervencionista e na endoscopia tenham modificado profundamente o manejo da hipertensão portal, o tratamento cirúrgico permanece indispensável em situações específicas. A seleção adequada do paciente, baseada em função hepática, etiologia da hipertensão portal e recursos disponíveis, continua sendo o fator mais importante para bons resultados. Para o cirurgião digestivo moderno, compreender as diferentes estratégias — desde shunts portossistêmicos até o transplante hepático — é essencial para oferecer um tratamento individualizado e seguro.
PROF. DR. OZIMO GAMA
Gastroenterologia Cirúrgica
“O transplante de fígado e as complexas derivações portais nos ensinaram que não há limites absolutos na cirurgia, apenas fronteiras do conhecimento que aguardam para ser ultrapassadas com dedicação e ciência.” — Thomas Starzl
Gostou ❔Nos deixe um comentário ✍️ , compartilhe em suas redes sociais e|ou mande sua dúvida pelo 💬 Chat On-line em nossa DM do Instagram.
FERIDA PÓS-OPERATÓRIA

A avaliação e os cuidados de feridas pós-operatórias deve ser do domínio de todos os profissionais que atuam na clínica cirúrgica. O conhecimento a cerca dos processos relacionados a cicatrização tecidual é importante tanto nos cuidados como na prevenção de complicações, tais como: infecções e deiscência. Como tal, todos os profissionais médicos, sendo eles cirurgiões ou de outras especialidades, que participam do manejo clínico dos pacientes no período perioperatório devem apreciar a fisiologia da cicatrização de feridas e os princípios de tratamento de feridas pós-operatório. O objetivo deste artigo é atualizar os profissionais médicos de outras especialidades sobre os aspectos importantes do tratamento de feridas pós-operatório através de uma revisão da fisiologia da cicatrização de feridas, os métodos de limpeza e curativo, bem como um guia sobre complicações de feridas pós-operatórias mais prevalentes e como devem ser manejados nesta situação.
Esophagectomy: Anastomotic Complications (Leakage and Stricture)

Esophagectomy can be used to treat several esophageal diseases; it is most commonly used for treatment of esophageal cancer. Esophagectomy is a major procedure that may result in various complications. This article reviews only the important complications resulting from esophageal resection, which are anastomotic complications after esophageal reconstruction (leakage and stricture), delayed emptying or dumping syndrome, reflux, and chylothorax.
Causas de conversão da VIDEOCOLECISTECTOMIA
Atualmente, a colecistectomia laparoscópica é a abordagem preferida para o tratamento da litíase biliar, representando cerca de 90% dos procedimentos realizados, uma marca alcançada nos Estados Unidos em 1992. A popularidade dessa técnica se deve a suas vantagens evidentes: menos dor no pós-operatório, recuperação mais rápida, redução dos dias de trabalho perdidos e menor tempo de hospitalização. Apesar de ser considerada o padrão-ouro na cirurgia biliar, a colecistectomia laparoscópica não está isenta de desafios. Entre 2% e 15% dos casos podem exigir a conversão para cirurgia convencional. Os motivos mais comuns para essa conversão incluem dificuldades na identificação da anatomia, suspeita de lesão da árvore biliar e controle de sangramentos. Identificar os fatores que contribuem para uma maior taxa de conversão é essencial para a equipe cirúrgica. Isso não apenas permite uma avaliação mais precisa da complexidade do procedimento, mas também ajuda na preparação do paciente para possíveis riscos e na mobilização de cirurgiões mais experientes quando necessário. Em um cenário onde a precisão e a segurança são cruciais, a compreensão dos desafios e a preparação adequada podem fazer toda a diferença no resultado da cirurgia.
Relacionados ao Paciente: 1. Obesidade (IMC > 35), 2. Sexo Masculino, 3. Idade > 65 anos, 4. Diabetes Mellitus e 5. ASA > 2.
Relacionadas a Doença: 1. Colecistite Aguda, 2. Líquido Pericolecístico, 3. Pós – CPRE, 4. Síndrome de Mirizzi e 5. Edema da parede da vesícula > 5 mm.
Relacionadas a Cirurgia: 1. Hemorragia, 2. Aderências firmes, 3. Anatomia obscura, 4. Fístulas internas e 5. Cirurgia abdominal prévia.
Review of POSTGASTRECTOMY SYNDROMES

The first postgastrectomy syndrome was noted not long after the first gastrectomy was performed: Billroth reported a case of epigastric pain associated with bilious vomiting as a sequel of gastric surgery in 1885. Several classic treatises exist on the subject; we cannot improve on them and merely provide a few references for the interested reader. Surgical procedures on the stomach, performed for reasons such as peptic ulcer disease, cancer, obesity, or gastroesophageal reflux disease, can result in various post-gastrectomy syndromes. These syndromes include chronic symptoms that range from mild discomfort to life-altering conditions. This guide covers the most common syndromes and their characteristics.
GASTRECTOMY VIDEO SURGERY
Dumping Syndrome
Dumping Syndrome is characterized by gastrointestinal and vasomotor symptoms that occur after food intake due to rapid gastric emptying. This syndrome can occur after surgeries that alter the regulation of gastric emptying or gastric compliance, such as gastrectomy, proximal vagotomy, sleeve gastrectomy, fundoplication, pyloroplasty, and gastrojejunostomy (GJ). Depending on the speed of emptying and the osmolarity of gastric contents, symptoms can vary.
- Early Dumping: Occurs within 30 minutes after food intake and is characterized by palpitations, tachycardia, fatigue, a need to lie down after meals, flushing or pallor, sweating, dizziness, hypotension, headache, and possibly syncope. Abdominal symptoms include early satiety, epigastric fullness, abdominal pain, bloating, hypermotility, and splenic blood pooling.
- Late Dumping: Appears 1 to 3 hours after eating, due to reactive hypoglycemia caused by an initially high glucose load leading to an inappropriately high insulin response. Symptoms include sweating, faintness, difficulty concentrating, and altered levels of consciousness.
Diagnosis is confirmed through an oral glucose tolerance test or a gastric emptying scintigraphy study.
Post-Vagotomy Diarrhea
Post-vagotomy diarrhea is a common complication after vagotomy, characterized by frequent episodes of watery diarrhea. It can be attributed to changes in intestinal motility and bile secretion.
Gastric Stasis
Gastric stasis or delayed gastric emptying can occur due to disruption of normal gastric motility. Symptoms include nausea, vomiting, and a feeling of fullness. Diagnosis is confirmed through gastric emptying studies.
Bile Reflux Gastritis
Bile reflux gastritis is caused by the reflux of bile into the stomach, resulting in epigastric pain and bilious vomiting. Diagnosis can be confirmed through upper endoscopy and gastric pH monitoring.
Afferent and Efferent Loop Syndromes
Afferent loop syndrome occurs after Billroth II reconstruction and is characterized by abdominal pain, bilious vomiting, and distention. Efferent loop syndrome occurs when there is an obstruction of the efferent loop, leading to similar symptoms.
Roux Syndrome
Roux syndrome is a complication of Roux-en-Y procedures, characterized by postprandial abdominal pain and vomiting. Diagnosis is made through a contrast gastrointestinal transit study.
Therapeutic Approach
Management of post-gastrectomy syndromes includes dietary modifications, such as eating small frequent meals, separating liquids and solids, increasing protein and fat intake, and reducing simple sugars. In some cases, additional pharmacological or surgical interventions may be necessary. Understanding these syndromes and their therapeutic approaches is crucial to providing effective care and improving the quality of life for post-gastrectomy patients.
This article focuses on the small proportion of patients with severe, debilitating symptoms; these symptoms can challenge the acumen of the surgeon who is providing the patient’s long-term follow-up and care.
POSTGASTRECTOMY_SYNDROMES_REVIEW_ARTICLE
The General Surgery Job Market

There is a current shortage of general surgeons nationwide. A growing elderly population and ongoing trends toward increased health care use have contributed to a higher demand for surgical services, without a corresponding increase in the supply of surgeons. The number of general surgeons per 100,000 people in the United States declined by 26% from the 1980s to 2005. Cumulative growth in demand for general surgery is projected to exceed 25% by 2025. The Association of American Medical Colleges has projected a shortage of 41,000 general surgeons by 2025. General surgeons make up 33% of the total projected physician shortage, the second highest after primary care physicians, who make up 37% of the total shortage. Despite the demand for general surgeons, the percentage of general surgery trainees going directly into practice is decreasing while the percentage of trainees pursuing subspecialty training is increasing. A recent study reported that graduating residents who lacked confidence in their skills to operate independently were more likely to pursue subspecialty training. This suggests that some graduating residents are motivated to obtain subspecialty training to gain more experience rather than narrow their clinical scope of practice. Given the projected shortage of general surgeons, this will be a crucial distinction when reforming surgical education. General surgery trainees interested in career planning would benefit from understanding the demand for general and/or specialty skills in a job market heavily influenced by a constant stream of new graduates. However, little is currently known about the demand for subspecialty vs general surgical skills in the current job market. The goal of this study was to describe the current job market for general surgeons in the United States, using Oregon and Wisconsin as surrogates. Furthermore, we sought to compare the skills required by the job market with those of graduating trainees with the goal of gaining insight that might assist in workforce planning and surgical education reform.
Survival Guide for SURGERY ROUND

SURGERY ROUND
Medical students are often attached to the various services. They can provide a significant contribution to patient care. However, their work requires supervision by the surgical intern/resident who takes primary clinical responsibility. Subinterns are senior medical students who are seeking additional clinical experience. Their assistance is needed and appreciated, but again, close supervision of their clinical responsibilities by the intern/resident is mandatory.Outside reading is recommended, including textbooks, reference sources, and monthly journals.Eating is prohibited in patient care areas.Maintain patient confidentiality at all times.At conferences use only patient initials in presentations; and speak carefully and respectfully on work rounds.
PRINCIPLES
1. Always be punctual (this includes ward rounds, operating room, clinics, conferences, morbidity and mortality). Personal appearance is very important. Maintain a high standard including clean shirt and tie (or equivalent) and a clean white coat. The day begins early. Be ready with all the data to start rounds with the senior resident or chief resident. Be sure to provide enough time each morning to examine your patients before rounds.
ABOUT NOTES
2.Aim to get all of your chart notes written as soon as possible; this will greatly increase your effi ciency during the day. Sign and print your name, and include your beeper number, date, and time. Progress notes on patients are required daily. Surgical progress notes should be succinct and accurate, briefl y summarizing the patient’s clinical status and plan of management. Someone unfamiliar with the case should be able to get a good understanding of the patient’s condition from one or two notes. Operative consent is obtained after admitting the patient, performing the history and physical examination, discussing the risks, benefi ts, and alternatives of the procedure(s), and having the patient’s nurse sign the consent with the patient. If you are unaware of the risks and benefi ts of a procedure, discuss this with the service chief resident. Blood transfusion attestation forms need to be signed by the counseling physician before each surgical procedure.
OPERATING ROOM
3. Arrive in the operating room with the patient and before the attending physician or chief resident. Make sure that the charts and all of the relevant x-rays are in the operating room. Make sure that the x-rays are on the x-ray view box prior to the commencement of the case. The intern or resident performing the case should be familiar with the patient’s history and physical exam, current medications, and comorbidities, and be familiar with the principles of the operation prior to arriving in the operating room. Make it a habit to introduce yourself to the patient before the operation. It is mandatory that the surgical resident involved with a case in the operating room attend the start of the case punctually. Scheduled operative cases do not necessarily occur at the listed time. For this reason, it is necessary to check with the operating room front desk frequently. Do not rely on being paged. Conduct in the operating room includes assisting with the preoperative positioning and preparation of the patient; this includes shaving, catheterization, protection of pressure points, and thromboembolism protection. The resident should escort the patient from the operating room to the intensive care unit (ICU) or the postanesthetic care unit with the anesthesiologists. The operating surgeon is responsible for dictating the case. The resident must record all cases performed. For cases admitted to the surgery ICU, a hand-over to the surgery ICU resident is mandatory.This includes discussing all the preoperative assessment, operative details, and postoperative management of the case with the ICU resident.
ROUNDS
4. Signing out to cross-cover services must be performed in a meticulous and careful fashion. All patients should be discussed between the surgical intern and the cross-covering intern to cover all potential problems. A sign-out list containing all the patients, patient locations, and the responsible attendings should be given personally to the cross-cover intern. Any investigations performed at night (e.g., lab studies, chest x-ray, electrocardiogram [ECG]) should be checked that night by the covering intern. No test order should go unchecked. Abnormal lab values should be reviewed and discussed with the senior resident or the attending staff, especially on preoperative patients. Starting antibiotics should be a decision left to the senior resident or attending staff. If consultants are asked to see patients, their recommendations mustbe discussed with your senior resident or attending priorto initiating any new plans. Independent thought is good; independent action is bad.
SUPERVISION
5. Document all procedures performed on patients—including arterial lines, chest tubes, and central lines—with a short procedure note in the chart. Every patient contact should be documented in the patient record.If you see a patient in the middle of the night, write a short note to describe your assessment and plan. Remember, if there is no documentation, then nobody responded to the patient’s complaint or needs. Obtain appropriate supervision for procedures. There are always more senior residents available if your chief is not. Protect yourself; practice universal precautions! Wash your hands before and after examining a patient. Wear gloves. All wounds should be inspected every day by the surgical intern as part of the clinical examination. Please re-dress them; the nursing staff is not always immediately available to do so. There should never be any surprises in the morning.
RESIDENTS
Your senior resident is responsible for the service and should be kept aware of any problems, regardless of the time of day. If the senior resident is not available, the attending staff should be contacted directly. There are always senior residents in the hospital who are available to be used as resources for emergencies. Always be aware of who is in-house (i.e., consult resident, ICU resident, trauma chief). A surgery resident’s days are long. They start early and they fi nish late. Always remember the three A’s to being a successful resident: Affable, Available, and Able. Be prepared to maintain a flexible daily schedule depending on the workload of the service and the requirement for additional manpower.
“COMO PODEMOS CURAR A MEDICINA?”
“Nos últimos anos percebemos que estávamos na mais profunda crise da existência da medicina, devido a algo sobre o que você normalmente não pensa quando você é um médico preocupado em fazer o bem para as pessoas, que é o custo do tratamento de saúde. Não há um país no mundo que não esteja perguntando agora se podemos custear o que médicos fazem. A luta política que desenvolvemos tornou-se aquela sobre se o governo é o problema ou se as companhias de seguro são o problema. E a resposta é sim e não; é mais profundo que tudo isso. A causa de nossos problemas é, na verdade, a complexidade que a ciência nos deu. E para entender isso, voltarei algumas gerações…”
“CIRURGIA: PASSADO, PRESENTE e FUTURO ROBÓTICO”
A cirurgiã e inventora Catherine Mohr nos guia pela história da cirurgia (e seu passado pré-anestesia e pré-antissepsia), e depois demonstra algumas das mais novas ferramentas para cirurgias realizadas através de pequenas incisões, usando ágeis mãos robóticas.
Ebook: Princípios da Cirurgia Hepatobiliar

Cirurgia Hepatobiliar
Considera-se que a cirurgia hepática começou após o advento da anestesia e da anti-sepsia. No entanto, muito antes disso, diversos autores já relatavam suas experiências com ressecções do fígado. As primeiras descrições de “cirurgias hepáticas” consistiam no relato de avulsões parciais ou totais de porções do fígado após lesões traumáticas do abdome. O relato de Elliot (1897) exemplifica muito dos temores dos cirurgiões da época: “O fígado (…) é tão friável, tão cheio de vasos e tão evidentemente impossível de ser suturado que parece ser improvável o manejo bem sucedido de grandes lesões de seu parênquima”.
CIRURGIA HEPATOBILIAR_ASPECTOS BÁSICOS
Lymph Node Dissection in Gastric Adenocarcinoma
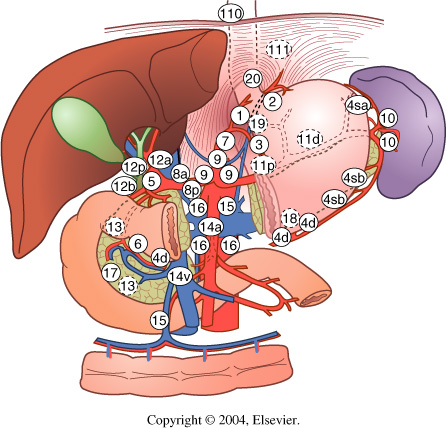
Extent of lymph node dissection has been an area of controversy in gastric adenocarcinoma for many years. Some surgeons believe that cancer metastasizes through a stepwise progression, and an extensive lymphadenectomy is necessary to improve survival and/or cure the patient. Other physicians argue that extensive ly-mphadenectomies only add pe-rioperative morbidity and mor-tality and do not improve survival. Asian countries have been performing extended lymphadenectomies routinely for many years with promising survival data, although Western countries have not been able to reproduce those results. Much of the controversy surrounding lymphadenectomies started in the 1980s when Japanese studies reported superior survival rates matched stage for stage, compared to the United States. This was theorized to be secondary to the more extensive lymphadenectomy performed in Japan compared to the United States.

A United Kingdom study randomized 400 patients to either a D1 or a D2 lymph node dissection. Those patients with tumors in the upper or middle third of the stomach underwent a distal pancreaticosplenectomy to obtain retropancreatic and splenic hilar nodes. While the 5-year survival rates were not statistically significant between the two groups, on multivariate analyses it was noted that those patients in the D2 group that did not undergo the distal pancreaticosplenectomy had an increased survival compared with the D1 group. A trial in the Netherlands randomized 380 gastric cancer patients to a D1 lymphadenectomy and 331 patients to a D2 lymphadenectomy. Similar to the United Kingdom study, there was not a significant difference in survival between the two groups, even when followed out to 11 years. There was a significant increase in postoperative complications in the D2 group compared with the D1 group (43 % vs. 25 %, respectively) as well as mortality (10 % vs. 4 %, respectively).
The data from these two studies suggest that a pancreaticosplenectomy performed to harvest lymph nodes seems to only add morbidity and mortality while not improving survival. One concern raised about the prior two studies was the variation in surgical technique and lack of standardization of surgeon experience. A Taiwanese study accounted for this by performing the study at a single institution with three surgeons, each of whom had completed at least 25 D3 lymph node dissections prior to the study. Patients with gastric cancer were randomized to a D1 lymph node dissection (defined as resection of perigastric lymph nodes along the lesser and greater curves of the stomach) or a D3 lymph node dissection (defined as resection of additional lymph nodes surrounding the splenic, common hepatic, left gastric arteries, nodes in the hepatoduodenal ligament, and retropancreatic lymph nodes). There was an overall 5-year survival benefit with the D3 group of 60 % compared with the D1 group of 54 %. A Japanese study evaluated a more aggressive lymph node dissection and randomized patients to a D2 dissection or a para-aortic lymph node dissection (PAND). There was no significant difference in 5-year survival between the two groups with a trend toward an increase in complications in the PAND group. Multiple studies have shown that the number of positive lymph nodes is a significant predictor of survival. Current AJCC guidelines stipulate that at least 15 lymph nodes are needed for pathologic examination to obtain adequate staging.
Laparoscopic techniques have become an integral part of surgical practice over the past several decades. For gastric cancer, multiple retrospective studies have reported the advantages of laparoscopic gastrectomy (LG) over open gastrectomy (OG). A recent meta-analysis of 15 nonrandomized comparative studies has also shown that although LG had a longer operative time than OG, it was associated with lower intraoperative blood loss, overall complication rate, fewer wound-related complications, quicker recovery of gastrointestinal motility with shorter time to first flatus and oral intake, and shorter hospital stay. A randomized prospective trial comparing laparoscopic assisted with open subtotal gastrectomy reported that LG had a significantly lower blood loss (229 ± 144 ml versus 391 ± 136 ml; P< 0.001), shorter time to resumption of oral intake (5.1 ± 0.5 days versus 7.4 ± 2 days; P< 0.001), and earlier discharge from hospital (10.3 ± 3.6 days versus 14.5 ± 4.6 days; P< 0.001).
Como funciona o GRAMPEADOR INTESTINAL ?
A Busca pela Segurança e Eficiência na Cirurgia Moderna
Introdução O objetivo primordial de qualquer cirurgião, ao iniciar uma intervenção, é garantir que o procedimento seja seguro e eficiente. A “regra de ouro” da cirurgia moderna permanece clara: o ato operatório deve ser o mais breve possível, gerando o menor trauma tecidual e restaurando a função do órgão. O resultado esperado é sempre a minimização das intercorrências no pós-operatório. Embora a cirurgia atual atinja esses objetivos de forma bastante satisfatória, as complicações relacionadas às suturas e à cicatrização ainda são desafios presentes na rotina hospitalar.
A Evolução Histórica e os Desafios da Cicatrização A confiabilidade das suturas gastrointestinais, por exemplo, é uma conquista relativamente recente. Foi apenas no final do século XIX que a compreensão dos princípios básicos da cicatrização tecidual permitiu avanços significativos nesta área. Sabemos hoje que o sucesso do reparo tecidual não depende apenas da técnica empregada, mas é uma equação complexa que envolve o paciente e a área operada. Diversos fatores podem retardar ou prejudicar drasticamente a cicatrização, entre eles:
-
Isquemia (falta de suprimento sanguíneo);
-
Edema (inchaço excessivo);
-
Infecção local ou sistêmica;
-
Desnutrição do paciente.
O Fator Humano e o Surgimento da Tecnologia Existe uma variável crítica na cirurgia: a habilidade manual. Naturalmente, há uma variação na destreza e na técnica entre diferentes cirurgiões. Foi justamente essa disparidade que motivou o desenvolvimento de novos dispositivos cirúrgicos. O objetivo da inovação tecnológica na cirurgia é superar as diferenças individuais, funcionando como um equalizador. Ao utilizar dispositivos que padronizam etapas críticas (como as suturas mecânicas), permite-se que técnicas complexas sejam executadas adequadamente, independente de quem opera.
Conclusão Para que a medicina avance, uma técnica não pode depender apenas do talento de poucos. Ela deve ser reproduzível de forma confiável pelo maior número possível de cirurgiões. Somente através dessa padronização e do auxílio tecnológico é que os resultados cirúrgicos podem ser amplamente adotados, reconhecidos como eficazes e, acima de tudo, seguros para o paciente.
POSTOPERATIVE ILEUS
POSTOPERATIVE ILEUS_REVIEW ARTICLE
 In systems that try to minimize hospital stay after abdominal surgery, one of the principal limiting factors is the recovery of adequate bowel function, which can delay discharge or lead to readmission. Postoperative ileus (POI) is the term given to the cessation of intestinal function following surgery. Although all surgical procedures put the patient at risk for POI, gastrointestinal tract surgeries in particular are associated with a temporary cessation of intestinal function. The duration of POI varies, lasting from a few hours to several weeks. Prolonged postoperative ileus, also known as pathologic postoperative ileus, can be caused by a myriad of pathologic processes that are treated with limited success by clinical and pharmacologic management. Studies of large administrative databases show that, on average, patients with a diagnosis of POI stay 5 days longer in hospital after abdominal surgery than patients without POI. Over the last decade, substantial efforts have been made to minimize the duration of POI, as there appears to be no associated physiologic benefit, and it is currently the primary factor delaying recovery for most patients. In this review, we define POI, describe the pathogenesis and briefly discuss clinical management before detailing current pharmacologic management options.
In systems that try to minimize hospital stay after abdominal surgery, one of the principal limiting factors is the recovery of adequate bowel function, which can delay discharge or lead to readmission. Postoperative ileus (POI) is the term given to the cessation of intestinal function following surgery. Although all surgical procedures put the patient at risk for POI, gastrointestinal tract surgeries in particular are associated with a temporary cessation of intestinal function. The duration of POI varies, lasting from a few hours to several weeks. Prolonged postoperative ileus, also known as pathologic postoperative ileus, can be caused by a myriad of pathologic processes that are treated with limited success by clinical and pharmacologic management. Studies of large administrative databases show that, on average, patients with a diagnosis of POI stay 5 days longer in hospital after abdominal surgery than patients without POI. Over the last decade, substantial efforts have been made to minimize the duration of POI, as there appears to be no associated physiologic benefit, and it is currently the primary factor delaying recovery for most patients. In this review, we define POI, describe the pathogenesis and briefly discuss clinical management before detailing current pharmacologic management options.
Prontuário Médico
Evolução Cirúrgica S.O.A.P.
A Engenharia do Prontuário Médico, Ética, LGPD e Defesa Profissional
Autor: Prof. Dr. Ozimo Gama (Tempo de Leitura: 12 minutos)

Introdução
O prontuário médico transcende a simples formalidade administrativa; ele é o repositório sagrado do segredo médico, o espelho da qualidade assistencial e a testemunha silenciosa de cada decisão clínica tomada na beira do leito. No ambiente de alta complexidade da cirurgia do aparelho digestivo, onde o limiar entre a recuperação fisiológica e a complicação catastrófica é estreito, a evolução médica diária exige uma precisão quase matemática. A prática de preencher o prontuário é uma obrigação legal e uma responsabilidade intransferível do médico assistente. Em hospitais de ensino — o berço da formação cirúrgica —, acadêmicos de medicina e médicos residentes (especializandos) realizam as anotações sob a estrita supervisão, correção e responsabilidade solidária de seus preceptores ou médicos do staff. É uma prática antiética, ilegal e frontalmente condenável delegar o preenchimento da evolução clínica a qualquer profissional que não seja um médico habilitado perante o Conselho Regional de Medicina (CRM) ou um acadêmico em treinamento devidamente supervisionado. Historicamente e na atualidade, o prontuário médico corretamente preenchido tem sido a principal, e muitas vezes a única, peça de defesa do cirurgião em casos de denúncias por suposto mau atendimento, imperícia, imprudência ou negligência. Quando a polícia, o Poder Judiciário ou as Câmaras Técnicas do CRM são acionados, o prontuário é o primeiro documento requisitado. Se a sua técnica cirúrgica no bloco operatório for irretocável, mas a sua evolução na enfermaria for omissa, perante a lei, o cuidado não existiu.
Aspectos Históricos e a Gênese do Modelo S.O.A.P.
Até meados do século XX, os prontuários médicos eram estruturados de forma cronológica e narrativa, assemelhando-se a um diário confuso, onde informações vitais perdiam-se num mar de textos desorganizados. A revolução ocorreu na década de 1960, quando o Dr. Lawrence L. Weed publicou o artigo seminal “Medical records that guide and teach” (N Engl J Med; 1968). Weed propôs uma inversão de paradigma: o Problem-Oriented Medical Record (Prontuário Médico Orientado por Problemas). No Brasil, este modelo foi amplamente adotado e adaptado sob a sigla POPE (Prontuário Orientado por Problemas e Evidências), destacando a necessidade de fundamentar cada passo clínico em evidências científicas sólidas. A espinha dorsal deste modelo é a nota de evolução estruturada no formato S.O.A.P., que divide o raciocínio médico em quatro quadrantes fundamentais: Subjetivo, Objetivo, Avaliação e Plano. Esta sistematização traz objetividade, clareza, facilidade de auditoria e, principalmente, permite que qualquer membro da equipe multidisciplinar (enfermagem, fisioterapia, nutrição) compreenda imediatamente o estado clínico e as metas terapêuticas do paciente cirúrgico.
A Estrutura do S.O.A.P. Cirúrgico
Na rotina da enfermaria de cirurgia digestiva, a evolução deve seguir um rigor técnico absoluto. O cabeçalho deve, obrigatoriamente, conter a identificação completa do paciente (Nome, Idade, Registro Hospitalar), a Enfermaria/Leito, o Diagnóstico Principal, o Nome da Cirurgia Realizada, o Dia de Pós-Operatório (ex: PO2 de Gastrectomia Total) e o Horário exato do atendimento.
Abaixo, detalhamos como cada componente da sigla S.O.A.P. deve ser preenchido sob a ótica cirúrgica:
1. “S” – Dados Subjetivos (A Voz do Paciente)
Compreende as queixas do paciente, sua percepção sobre a evolução e informações fornecidas por acompanhantes. Em cirurgia, não basta escrever “passou bem”. É imperativo interrogar ativamente sobre:
- Dor: Utilizar escalas validadas (ex: Escala Visual Analógica – EVA de 0 a 10). A dor é em cólica? É contínua? Piora à mobilização?
- Trato Gastrointestinal: Houve náuseas ou episódios de êmese? Houve eliminação de flatos (sinal crucial de retorno do trânsito intestinal)? Houve evacuação? Como foi a aceitação da dieta oferecida?
- Mobilização: O paciente deambulou? Conseguiu sentar na poltrona? (Dados vitais para a profilaxia de trombose venosa profunda e atelectasia).
- Exemplo: “Paciente refere dor incisional leve (EVA 2/10), com boa aceitação de dieta líquida. Nega náuseas. Refere eliminação de flatos durante a madrugada. Deambulou no corredor hoje cedo.”
2. “O” – Dados Objetivos (A Visão do Cirurgião)
Inclui os dados vitais irrefutáveis, o exame físico focado e os resultados de exames complementares laboratoriais ou de imagem. Este é o terreno da evidência mensurável.
- Sinais Vitais: Frequência Cardíaca (FC), Pressão Arterial (PA), Frequência Respiratória (FR), Temperatura (T) e Saturação de O2. A taquicardia inexplicada no pós-operatório de uma anastomose intestinal é o primeiro grito de socorro de uma fístula, antes mesmo da febre ou da dor peritonítica.
- Exame Físico Específico: * Abdome: Globoso? Flácido? Ruídos hidroaéreos presentes? Dor à palpação (diferenciar dor incisional de irritação peritoneal)?
- Ferida Operatória (FO): Limpa e seca? Hiperemiada? Presença de secreção (serosa, purulenta, hemática)?
- Drenos: Tipo de dreno (ex: Jackson-Pratt, Blake, Penrose). Qual o aspecto do débito (seroso, sero-hemático, bilioso, entérico, fecaloide)? Qual o volume em 24 horas?
- Estomas: Colostomia/Ileostomia com mucosa rósea (vitalidade)? Edemaciada? Isquêmica? Estoma funcionante (presença de fezes na bolsa)?
- Exemplo: “PA: 120×70 mmHg; FC: 88 bpm; FR: 16 irpm; T: 36,8ºC. Abdome: flácido, RHA+, indolor à palpação profunda. FO: sem hiperemia, curativo limpo. Dreno de Blake em FIE: débito de 30ml sero-hemático em 24h. Labs (05/10): Hb 11.2, Leucócitos 8.500 (sem desvio), PCR 12 (em queda).”
3. “A” – Avaliação (O Raciocínio Clínico)
A Avaliação é a síntese. É o momento em que o cirurgião processa os dados Subjetivos e Objetivos para emitir o seu juízo de valor sobre o estado do paciente. Não é a repetição dos diagnósticos da internação, mas a avaliação do momento atual.
- O paciente está evoluindo conforme o esperado para o dia de pós-operatório?
- Há suspeita de complicações (íleo paralítico prolongado, infecção de sítio cirúrgico, fístula anastomótica, sangramento, pneumonia)?
- Exemplo: “Paciente no 2º PO de Colectomia Direita Videolaparoscópica por Adenocarcinoma. Evolução clínica e laboratorial amplamente favorável. Trânsito intestinal restabelecido. Sem sinais de complicações infecciosas ou hemorrágicas no momento.”
4. “P” – Plano (A Conduta e o Futuro)
O Plano define as ações imediatas e de médio prazo. É a conduta terapêutica e diagnóstica fundamentada na avaliação recém-feita.
- Terapêutica: Progressão ou regressão de dieta? Transição de analgesia venosa para via oral? Suspensão de fluidos intravenosos? Descalonamento ou suspensão de antibioticoterapia profilática/terapêutica?
- Procedimentos: Retirada de dreno? Troca de curativo? Retirada de Sonda Vesical de Demora (SVD)?
- Diagnóstico: Solicitação de novos exames laboratoriais ou tomografia de abdome (se suspeita de complicação)?
- Educação/Alta: Orientações ao paciente e preparo para alta hospitalar.
- Exemplo: “1. Progredir para dieta pastosa; 2. Suspender hidratação venosa e manter acesso salinizado; 3. Trocar analgesia para via oral; 4. Retirar dreno de Blake hoje; 5. Programar alta hospitalar para amanhã, caso mantenha tolerância à dieta.”
Aspectos Éticos, Legais e Atualizações Normativas
A prática médica contemporânea exige que a evolução cirúrgica esteja blindada contra vulnerabilidades legais. A doutrina da “medicina de defesa” tem dado lugar à Prevenção Jurídica Ativa, onde o prontuário é o escudo. Segundo o Código de Ética Médica (Resolução CFM nº 2.217/2018), em seu Capítulo X, é vedado ao médico negar acesso ao prontuário ao paciente, bem como é infração ética grave deixar de elaborar prontuário legível para cada paciente.
O Código Penal e a Falsidade Ideológica
As anotações devem refletir a estrita verdade temporal e clínica. O Artigo 299 do Código Penal Brasileiro é taxativo quanto ao crime de falsidade ideológica: “Omitir, em documento público ou particular, declaração que dele devia constar, ou nele inserir ou fazer inserir declaração falsa ou diversa da que devia ser escrita…”. A pena varia de 1 a 5 anos de reclusão. Evoluções “clonadas” (o infame “copiar e colar” do dia anterior no prontuário eletrônico sem verificar o paciente) que não relatam a mudança do estado clínico (ex: o paciente apresentou febre à noite, mas a evolução matinal diz “afebril” por cópia da véspera) podem caracterizar este crime, além de negligência médica. No papel, rasuras anulam o valor probatório; deve-se usar a expressão “digo” ou “em tempo” para retificações.
O Prontuário Eletrônico do Paciente (PEP) e a Certificação Digital
A Resolução CFM nº 1.638/2002 tornou obrigatória a legibilidade do prontuário em papel (o fim definitivo da “letra de médico” ilegível). Contudo, a grande revolução normativa reside no Prontuário Eletrônico. De acordo com a Resolução CFM nº 1.821/2007 (e suas atualizações, como a Resolução 2.299/2021), para que um documento médico eletrônico tenha validade legal e elimine a necessidade do papel, ele deve utilizar sistema de segurança com Nível de Garantia de Segurança 2 (NGS2), que exige a Assinatura Digital com certificado ICP-Brasil (Infraestrutura de Chaves Públicas Brasileira). Sem o token ou certificado digital em nuvem assinado pelo médico, a evolução digitada não tem presunção de veracidade jurídica plena. A senha do sistema do hospital não substitui a assinatura digital. A prática de fornecer seu login e token para que o residente ou interno assine por você é falta ética gravíssima, equiparada à quebra de sigilo e falsidade ideológica.
A Lei Geral de Proteção de Dados (LGPD – Lei 13.709/2018)
O prontuário cirúrgico contém dados sensíveis (informações sobre saúde). A implementação da LGPD obriga as instituições e os médicos a garantirem o acesso restrito a essas informações. A evolução clínica SOAP não pode ser fotografada pelo celular do médico e enviada em grupos de mensagens (como WhatsApp) sem a desidentificação completa do paciente ou consentimento expresso. Vazamentos de dados contidos no prontuário geram pesadas multas pela Autoridade Nacional de Proteção de Dados (ANPD) e processos civis por dano moral.
Pontos-Chave para a Prática Diária do Residente
- Tempo é Documento: A data e a hora do atendimento são cruciais. A evolução médica reflete o paciente naquele minuto exato. A cronologia dos eventos salva ou condena o cirurgião em uma sindicância.
- O Perigo do Copiar/Colar: No prontuário eletrônico, o recurso de copiar a evolução do dia anterior induz ao erro, perpetuando dados vitais antigos ou ignorando exames recentes. Cada dia exige uma avaliação autêntica e original.
- Assinatura e Carimbo: No papel, carimbo e assinatura legível com CRM. No eletrônico, Assinatura Digital (ICP-Brasil). A validação de quem prescreve ou evolui é intransferível.
- Comunicação Multidisciplinar: A evolução SOAP não é escrita apenas para o juiz ou para o CRM; ela é lida pelo enfermeiro que administrará o antibiótico, pelo fisioterapeuta que mobilizará o paciente e pelo nutrólogo que ajustará a dieta. Clareza é respeito pela equipe e segurança para o doente.
Conclusões Aplicadas à Prática do Cirurgião Digestivo
A evolução cirúrgica é a radiografia do intelecto do médico. O método S.O.A.P. obriga o cirurgião do aparelho digestivo a estruturar seu pensamento científico de maneira cartesiana, garantindo que nenhum dreno, ostomia ou sintoma de alarme passe despercebido na enfermaria. Em uma era dominada pela alta tecnologia robótica e laparoscópica no centro cirúrgico, é na beira do leito e na frente da tela do Prontuário Eletrônico que o pós-operatório é vencido. Compreender as legislações vigentes, a obrigatoriedade da certificação digital e a rigidez da LGPD protege o patrimônio e a carreira do profissional, permitindo que ele exerça a arte da cirurgia com paz de espírito, sabendo que sua conduta está não apenas eticamente correta, mas juridicamente blindada.
“O prontuário não é apenas um registro de doenças, mas sim o livro de memórias de uma batalha travada em conjunto pelo médico e pelo paciente. Uma palavra mal escrita ou omitida pode ser tão letal quanto um bisturi mal empunhado na sala de operações.” — Aforismo da Educação Médica Cirúrgica.
Gostou ❔Nos deixe um comentário ✍️ , compartilhe em suas redes sociais e|ou mande sua dúvida pelo 💬 Chat On-line em nossa DM do Instagram.
LIFE AS A SURGEON
Life as a Surgeon
Surgical careers begin long before one is known as a surgeon. Medicine in general, and surgery in particular, is competitive from the start. As the competition begins, in college or earlier, students are confronted with choices of doing what interests them and what they may truly enjoy vs doing what is required to get to the next step. It is easy to get caught up in the routine of what is required and to lose track of why one wanted to become a doctor, much less a surgeon, in the first place. The professions of medicine and surgery are vocations that require extensive knowledge and skill. They also require a high level of discretion and trustworthiness. The social contract between the medical profession and the public holds professionals to very high standards of competence and moral responsibility. Tom Krizek goes on to explain that a profession is a declaration of a way of life ‘‘in which expert knowledge is used not primarily for personal gain, but for the benefit of those who need that knowledge.’’
For physicians, part of professionalism requires that when confronted with a choice between what is good for the physician and what is good for the patient, they choose the latter. This occurs and is expected sometimes to the detriment of personal good and that of physicians’ families. Tom Krizek even goes so far as to question whether surgery is an ‘‘impairing profession.’’ This forces one to consider the anticipated lifestyle. In sorting this out, it is neither an ethical breach nor a sign of weakness to allocate high priority to families and to personal well-being. When trying to explain why surgery may be an impairing profession, Krizek expands with a cynical description of the selection process. Medical schools seek applicants with high intelligence; responsible behavior; a studious, hard-working nature; a logical and scientific approach to life and academics; and concern for living creatures. He goes further to explain that in addition to these characteristics, medical schools also look for intensity and drive, but are often unable to make distinctions among those who are too intense, have too much drive, or are too ingratiating.
Medical School
There are many ethical challenges confronting medical students. As they start, medical students often have altruistic intentions, and at the same time are concerned with financial security. The cost of medical education is significant. This can encourage graduates to choose specialty training according to what will provide them the most expedient means of repaying their debt. This can have a significant, and deleterious, impact on the health care system in that the majority of medical graduates choose to pursue specialty training, leaving a gap in the availability of primary care providers. As medical students move into their clinical training, they begin interacting with patients. One concern during this time is how medical students should respond and carry on once they believe that a mistake on their part has resulted in the injury or death of another human being. In addition, the demands of studying for tests, giving presentations, writing notes, and seeing patients can be overwhelming. The humanistic and altruistic values that medical students have when they enter medical school can be lost as they take on so much responsibility. They can start to see patient interactions as obstacles that get in the way of their other work requirements. During their clinical years, medical students decide what field they will ultimately pursue. For students to make an informed decision about a career in surgery, they need to know what surgeons do, why they do it, and how surgery differs from other branches of medicine. It is important for them to be aware of what the life of a surgeon entails and whether it is possible for them to balance a surgical career with a rewarding family life.
Surgical Residency
Beginning residents are confronted with a seemingly unbearable workload, and they experience exhaustion to the point where the patient may seem like ‘‘the enemy.’’ At the same time, they must learn how to establish strong trusting relationships with patients. For the first time, they face the challenge of accepting morbidity and death that may have resulted directly from their own actions. It is important that residents learn ways to communicate their experience to friends and family, who may not understand the details of a surgeon’s work but can provide valuable support. The mid-level resident confronts the ethical management of ascending levels of responsibility and risks, along with increasing emphasis on technical knowledge and skills. It is at this level that the surgical education process is challenged to deal with the resident who does not display the ability to gain the skills required to complete training as a surgeon. Residents at this level also must deal with the increasing level of responsibility to the more junior residents and medical students who are dependent on them as teacher, organizer, and role model. All of this increasing responsibility comes at a time when the resident must read extensively, maintain a family life, and begin to put long-range plans into practice in preparation for the last rotation into the chosen final career path. The senior surgical resident should have acquired the basics of surgical technique and patient management, accepting nearly independent responsibility for patient care. The resident at this level must efficiently and fairly coordinate the functioning team, engage in teaching activities, and work closely with all complements of the staff. As far as ethics education is concerned, residents at this stage should be able to teach leadership, teamwork, and decision-making. They should be prepared to take on the value judgments that guide the financial and political aspects of the medical and surgical practice.
The Complete Surgeon
The trained surgeon must be aware of the need to differentiate between the business incentives of medical care and doing what is right for a sick individual. As financial and professional pressures become more intense, the challenge increases to appropriately prioritize and balance the demands of patient care, family, education, teaching, and research. For example, how does the surgeon deal with the choice between attending a child’s graduation or operating on an old patient who requests him rather than an extremely well-trained associate who is on call? How many times do surgeons make poor choices with respect to the balance of family vs work commitments? Someone else can
competently care for patients, but only parents can be uniquely present in the lives of their children. Time flies, and surgeons must often remind themselves that their lives and the lives of their family members are not just a dress rehearsal.
Knowing When to Quit
A 65-year-old surgeon who maintains a full operating and office schedule, is active in community and medical organizations, and has trained most of her surgical colleagues is considering where to go next with her career. Recently, her hospital acquired the equipment to allow robotic dissection in the area where she does her most complicated procedures. She has just signed up to learn this new technology, but is beginning to reflect on the advisability of doing this. How long should she continue at this pace, and how does she know when to slow down and eventually quit operating and taking the responsibility of caring for patients? Murray Brennan summarizes the dilemma of the senior surgeon well. The senior surgeon is old enough and experienced enough to do what he does well. He yearns for the less complicated days where he works and is rewarded for his endeavors. He becomes frustrated by restrictive legislation, the tyranny of compliance, and the loss of autonomy. Now regulated, restricted, and burdened with compliance, with every medical decision questioned by an algorithm or guideline, he watches his autonomy of care be ever eroded. Frustrated at not being able to provide the care, the education, and the role model for his juniors, he abandons the challenge.
Finishing with Grace
Each surgeon should continuously map a career pathway that integrates personal and professional goals with the outcome of maintaining value, balance, and personal satisfaction throughout his or her professional career. He or she should cultivate habits of personal renewal, emotional self-awareness, and connection with colleagues and support systems, and must find genuine meaning in work to combat the many challenges. Surgeons also need to set an example of good health for their patients. Maintaining these values and healthy habits is the work of a lifetime. Rothenberger describes the master surgeon as a person who not only knows when rules apply, recognizes patterns, and has the experience to know what to do, but also knows when rules do not apply, when they must be altered to fit the specifics of an individual case, and when inaction is the best course of action. Every occasion is used to learn more, to gain perspective and nuance. In surgery, this is the rare individual who puts it all together, combining the cognitive abilities, the technical skills, and the individualized decision-making needed to tailor care to a specific patient’s illness, needs, and preferences despite incomplete and conflicting data. The master surgeon has an intuitive grasp of clinical situations and recognizes potential difficulties before they become major problems. He prioritizes and focuses on real problems. He possesses insight and finds creative ways to manage unusual and complex situations. He is realistic, self-critical, and humble. He understands his limitations and is willing to seek help without hesitation. He adjusts his plans to fit the specifics of the situation. He worries about his decisions, but is emotionally stable.
Cystic Disorders of the Bile Ducts
 OVERVIEW
OVERVIEW
Cystic disorders of the bile ducts, although rare, are well-defined malformations of the intrahepatic and/or extrahepatic biliary tree. These lesions are commonly referred to as choledochal cysts,which is a misnomer, as these cysts often extend beyond the common bile duct (choledochus).
EPIDEMIOLOGY
Cystic disorders of the bile ducts account for approximately 1% of all benign biliary disease. Also, biliary cysts are four times more common in females than males. The majority of patients (60%) with bile duct cysts are diagnosed in the first decade of life, and approxi-mately 20% are diagnosed in adulthood.
CLASSIFICATION
Cystic dilatation of the bile ducts occurs in various shapes—fusi-form, cystic, saccular, and so on—and in different locations through-out the biliary tree. The most commonly used classification is the Todani modification of the Alonso-Lej classification.
ETIOLOGY
The exact etiology of biliary cysts is unknown.
CLINICAL PRESENTATION
The initial clinical presentation varies significantly between children and adults. In children, the most common symptoms are intermittent abdominal pain, nausea and vomiting, mild jaundice, and an abdom-inal mass. The classical triad of abdominal pain, jaundice, and a pal-pable abdominal mass associated with choledochal cyst is observed in only 10% to 15% of children, and it is rarely seen in adults. Symp-toms in adults often mimic those seen in patients with biliary tract disease or pancre-atitis.
SURGICAL MANAGEMENT
The definitive treatment of bile duct cysts usually includes surgical excision of the abnormal extrahepatic bile duct with biliary-enteric reconstruction. This approach relieves biliary obstruction, prevent-ing future episodes of cholangitis, stone formation, or biliary cirrho-sis and thus interrupting the inflammatory liver injury cycle. It also stops pancreatic juice reflux, and more importantly, it removes tissue at risk of malignant transformation.
Câncer de Esôfago
Epidemiologia, Diagnóstico Precoce e a Complexidade do Tratamento Multimodal
Autor: Prof. Dr. Ozimo Gama
Categoria: Oncologia Cirúrgica / Cirurgia do Aparelho Digestivo
Tempo de Leitura: 9 minutos
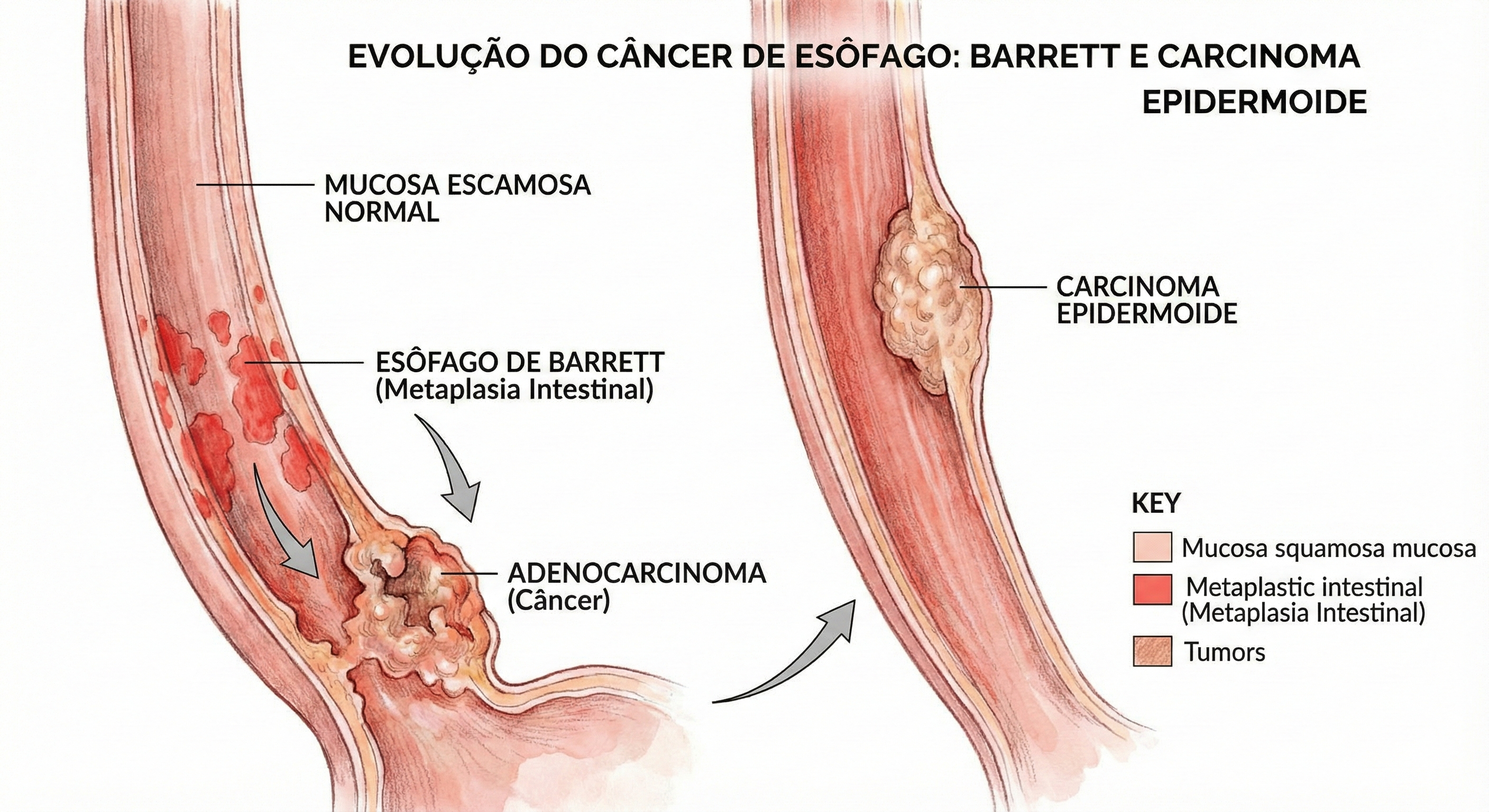
CEC
Introdução
O esôfago, um tubo musculomembranoso de aproximadamente 25 a 30 centímetros, desempenha a função vital de transportar o bolo alimentar da hipofaringe ao estômago através de peristalse coordenada. Apesar de sua anatomia aparentemente simples, desprovida de serosa, este órgão é sítio de uma das neoplasias mais agressivas e desafiadoras para o cirurgião do aparelho digestivo: o câncer de esôfago. Esta patologia é caracterizada por sua latência clínica. Em fases iniciais, a doença é assintomática, o que retarda o diagnóstico e compromete o prognóstico. Para o estudante de medicina e o residente de cirurgia, compreender a dualidade histológica predominante — Carcinoma Epidermoide (CEC) versus Adenocarcinoma — e seus respectivos fatores de risco é fundamental para a suspeição clínica e o rastreamento adequado.
Epidemiologia e o Cenário Brasileiro
O câncer de esôfago é uma questão de saúde pública global, com alta incidência em regiões do “cinturão do câncer de esôfago” (que se estende da China ao norte do Irã). No Brasil, a doença mantém-se relevante e letal. Dados atualizados da Estimativa 2023-2025 do Instituto Nacional de Câncer (INCA) projetam cerca de 10.990 novos casos anuais no país. A incidência é marcadamente maior no sexo masculino, ocupando a 6ª posição entre os tipos de câncer mais frequentes nos homens (excetuando-se o câncer de pele não melanoma). Historicamente, o Carcinoma Epidermoide representa a grande maioria dos casos (cerca de 96% em séries históricas brasileiras), intimamente ligado ao tabagismo e etilismo. Contudo, observamos uma transição epidemiológica importante: o Adenocarcinoma distal tem apresentado um crescimento exponencial, impulsionado pela epidemia de obesidade e pela Doença do Refluxo Gastroesofágico (DRGE) que culmina no Esôfago de Barrett.
Fatores de Risco e Prevenção
A gênese do câncer esofágico é multifatorial, e a prevenção passa pela mitigação destes agentes:
- Tabagismo e Etilismo: A combinação destes dois fatores tem efeito sinérgico, multiplicando exponencialmente o risco para o tipo Epidermoide.
- Hábitos Alimentares: O consumo frequente de bebidas em temperaturas muito elevadas (comum em certas culturas regionais brasileiras) causa dano térmico crônico à mucosa. Dietas pobres em frutas e vegetais também são fatores predisponentes.
- Condições Precursoras:
- Acalasia: A estase alimentar crônica promove inflamação da mucosa.
- Tilose: Hiperqueratose palmoplantar associada a alto risco de CEC.
- Esôfago de Barrett: A metaplasia intestinal causada pelo refluxo ácido crônico é a lesão precursora do Adenocarcinoma.
- Outros: Síndrome de Plummer-Vinson, ingestão de cáusticos e infecção pelo HPV.
Quadro Clínico: O Desafio do Silêncio
O grande obstáculo no manejo do câncer de esôfago é a ausência de sintomas precoces. A distensibilidade da parede esofágica permite que o tumor cresça significativamente antes de causar obstrução. Quando sintomático, o paciente tipicamente apresenta:
- Disfagia Progressiva: Inicialmente para sólidos, evoluindo para pastosos e líquidos.
- Perda Ponderal: Frequentemente severa (>10% do peso corporal), devido à disfagia e ao catabolismo tumoral.
- Odinofagia e Dor Retroesternal: Indicativos de invasão local ou ulceração.
Propedêutica e Diagnóstico
O padrão-ouro para o diagnóstico é a Endoscopia Digestiva Alta (EDA) com biópsia.

CEC
Para o cirurgião e endoscopista, o uso de cromoscopia é vital. O Lugol é utilizado para corar o epitélio escamoso normal (rico em glicogênio), deixando áreas neoplásicas ou displásicas “não coradas” (amarelo-claras), facilitando a biópsia dirigida no Carcinoma Epidermoide. Já o Azul de Toluidina ou métodos digitais (NBI/FICE) auxiliam na detecção do Barrett e Adenocarcinoma precoces. O estadiamento deve ser rigoroso, utilizando Tomografia Computadorizada (tórax e abdome superior) e, idealmente, a Ecoendoscopia (Ultrassom Endoscópico) para avaliar a invasão da parede (T) e linfonodos regionais (N), além do PET-CT para exclusão de metástases à distância.
Abordagem Terapêutica: Multimodalidade
O tratamento depende estritamente do estadiamento e da localização tumoral (Cervical, Torácico ou Junção Esôfago-Gástrica).
- Doença Precoce (Tis/T1a): Pode ser passível de Ressecção Endoscópica (Mucosectomia ou ESD), preservando o órgão com taxas de cura elevadas (98%).
- Doença Localmente Avançada: A cirurgia isolada raramente é suficiente. O padrão atual envolve Terapia Neoadjuvante (Quimioterapia + Radioterapia pré-operatória) seguida de Esofagectomia com Linfadenectomia. A cirurgia é de alta complexidade, podendo ser realizada por via aberta, laparoscópica ou robótica (técnicas de Ivor Lewis ou McKeown).
- Doença Metastática ou Irressecável: O foco torna-se paliativo. A inserção de próteses autoexpansíveis (stents) endoscópicos restaura a via oral e a dignidade do paciente. A radioterapia e braquiterapia também desempenham papel no controle local da disfagia e sangramento.
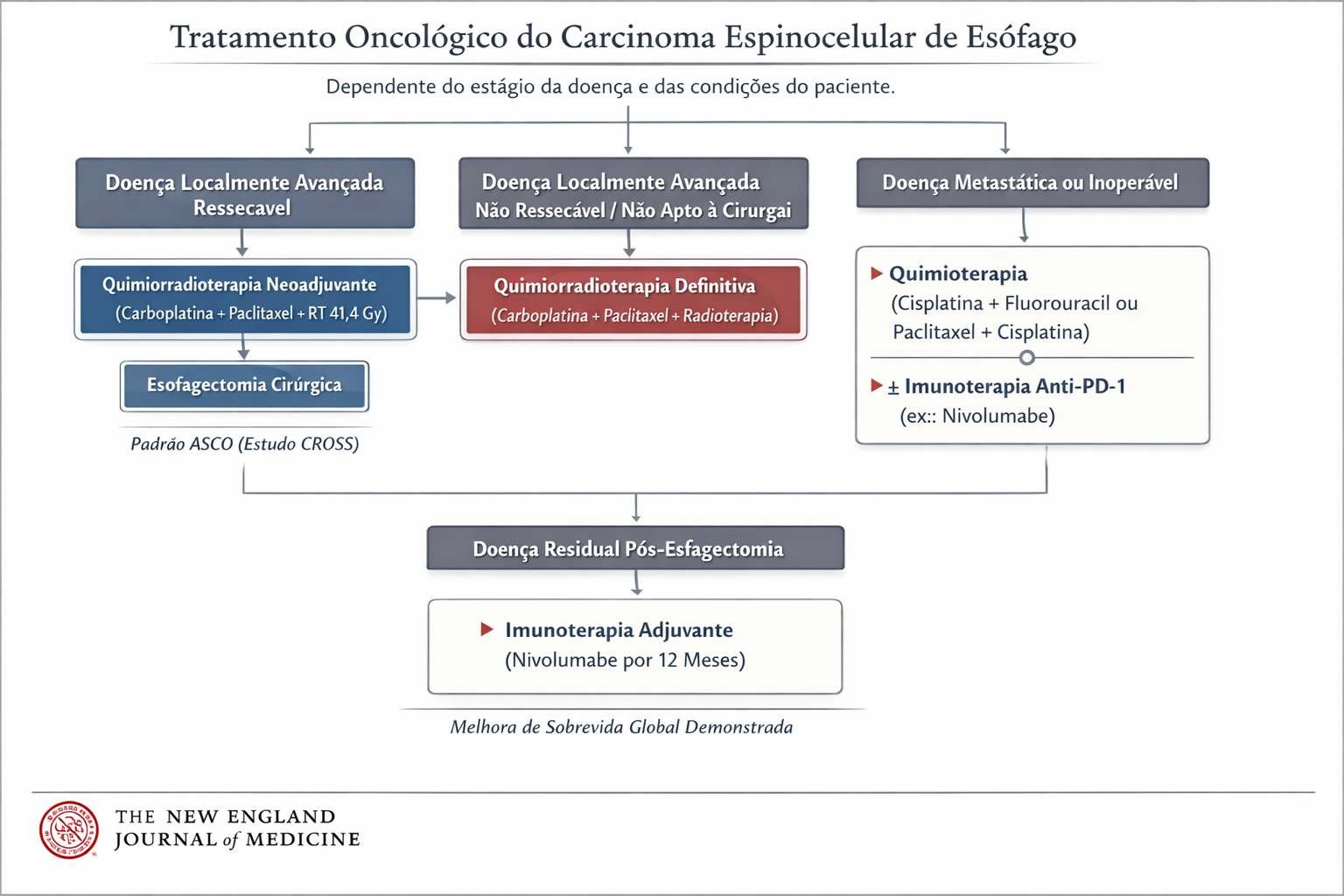
Fluxograma
Pontos-Chave para a Prática Cirúrgica
- Rastreamento: Pacientes com DRGE crônico (há mais de 5-10 anos) ou sintomas de alarme devem ser submetidos a endoscopia para rastreio de Barrett.
- Anatomia: O esôfago não possui serosa, o que facilita a invasão precoce de estruturas mediastinais (traqueia, aorta, pericárdio).
- Diagnóstico: Disfagia em adulto deve ser investigada com EDA imediatamente; não assuma benignidade sem visualização direta.
Conclusão
O câncer de esôfago exemplifica a necessidade da medicina moderna ser multidisciplinar. O cirurgião do aparelho digestivo não atua isolado, mas em concerto com o oncologista clínico, o radio-oncologista e o endoscopista. O diagnóstico precoce continua sendo a arma mais poderosa; contudo, mesmo em estágios avançados, a evolução das técnicas cirúrgicas e das terapias adjuvantes tem oferecido novas perspectivas de sobrevida e qualidade de vida aos nossos pacientes.
“A abordagem cirúrgica do esôfago foi, até recentemente, uma história de frustração. (…) O esôfago é um órgão que tolera a cirurgia mal, exceto quando executada com precisão absoluta.” — Ivor Lewis (1946), cirurgião galês que revolucionou o tratamento do câncer de esôfago com a técnica de esofagectomia transtorácica.
Gostou ❔Nos deixe um comentário ✍️ , compartilhe em suas redes sociais e|ou mande sua dúvida pelo 💬 Chat On-line em nossa DM do Instagram.
Hashtags: #CancerDeEsofago #CirurgiaDoAparelhoDigestivo #Oncologia #Esofagectomia #MedicinaBaseadaEmEvidencias
Ethics in Surgery : R.I.S.K.
Renewed public attention is being paid to ethics today. There are governmental ethics commissions, research ethics boards, and corporate ethics committees. Some of these institutional entities are little more than window dressing, whereas others are investigative bodies called into being, for example, on suspicion that financial records have been altered or data have been presented in a deceptive manner. However, many of these groups do important work, and the fact that they have been established at all suggests that we are not as certain as we once were, or thought we were, about where the moral boundaries are and how we would know if we overstepped them. In search of insight and guidance, we turn to ethics. In the professions, which are largely self-regulating, and especially in the medical profession, whose primary purpose is to be responsive to people in need, ethics is at the heart of the enterprise.
Responsibility to the patient in contemporary clinical ethics entails maximal patient participation, as permitted by the patient’s condition, in decisions regarding the course of care. For the surgeon, this means arriving at an accurate diagnosis of the patient’s complaint, making a treatment recommendation based on the best knowledge available, and then talking with the patient about the merits and drawbacks of the recommended course in light of the patient’s life values. For the patient, maximal participation in decision making means having a conversation with the surgeon about the recommendation, why it seems reasonable and desirable, what the alternatives are, if any, and what the probable risks are of accepting the recommendation or pursuing an alternative course.
This view of ethically sound clinical care has evolved over the latter half of the 20th century from a doctor-knows-best ethic that worked reasonably well for both patients and physicians at a time when medical knowledge was limited and most of what medicine could do for patients could be carried in the doctor’s black bag or handled in a small, uncluttered office or operating room. What practical steps can be taken by clinicians to evaluate patient attitudes and behavior relative to the patient’s cultural context so that the physician and patient together can reach mutually desired goals of care? Marjorie Kagawa-Singer and her colleagues at the University of California, Los Angeles, developed a useful tool for ascertaining patients’ levels of cultural influence. It goes by the acronym RISK:
Resources: On what tangible resources can the patient draw, and how readily available are they?
Individual identity and acculturation: What is the context of the patient’s personal circumstances and her degree of integration within her community?
Skills: What skills are available to the patient that allow him to adapt to the demands of the condition?
Knowledge: What can be discerned from a conversation with the patient about the beliefs and customs prevalent in her community and relevant to illness and health, including attitudes about decision making and other issues that may affect the physician-patient relationship.
TRATAMENTO DA TROMBOSE HEMORROIDÁRIA

A trombose hemorroidária é uma condição dolorosa e desconfortável que ocorre quando um coágulo de sangue se forma dentro de uma hemorróida. Essa condição é mais comum em gestantes, pessoas com constipação intestinal crônica, e em situações que aumentam a pressão intra-abdominal, como exercícios físicos intensos e levantamento de peso. Neste artigo, exploraremos as causas, sintomas e opções de tratamento para a trombose hemorroidária, ajudando você a entender melhor essa condição e a buscar a melhor abordagem para o seu caso.
Causas da Trombose Hemorroidária
A trombose hemorroidária geralmente está relacionada a fatores de estilo de vida e hábitos pessoais. Os principais gatilhos incluem:
- Obstipação (prisão de ventre): O esforço excessivo para evacuar aumenta a pressão nas veias do ânus, e as fezes endurecidas podem causar traumatismo no tecido anal.
- Gravidez: A pressão adicional no abdômen durante a gravidez pode contribuir para o desenvolvimento da trombose.
- Esforços prolongados e levantamento de peso: Atividades que aumentam a pressão intra-abdominal são fatores de risco.
- Higiene inadequada: A falta de cuidados apropriados na região anal pode exacerbar a condição.
- Fatores adicionais: Permanecer sentado por longos períodos, consumo excessivo de alimentos picantes e bebidas alcoólicas, e prática de sexo anal.
Sintomas da Trombose Hemorroidária
Os principais sinais de trombose hemorroidária incluem:
- Dor intensa na região anal: A dor é geralmente súbita e pode ser bastante severa.
- Sangramento: Frequentemente observado durante a evacuação.
- Inchaço e aumento de volume: Um nódulo na região anal pode se tornar arroxeado ou preto, indicando a presença de um trombo.
Tratamentos Indicados
O tratamento da trombose hemorroidária varia conforme a gravidade da condição. Entre as abordagens recomendadas estão:
- Uso de analgésicos e pomadas anestésicas: Para alívio da dor e desconforto.
- Banhos de assento: Utilizar água morna para aliviar os sintomas e reduzir o inchaço.
- Correção dos hábitos alimentares: Aumentar a ingestão de fibras e líquidos para prevenir a obstipação.
- Tratamento cirúrgico: Em casos mais graves, pode ser necessário realizar uma cirurgia para remover a hemorróida e o trombo.
Se você apresenta sintomas semelhantes, é crucial consultar um médico para uma avaliação adequada e receber o tratamento adequado.
Gostou ❔ Nos deixe um comentário ✍️, ou mande sua dúvida pelo 💬 Chat On-line.
Lembre-se: A informação aqui fornecida é para orientação geral. Sempre consulte seu médico para aconselhamento específico sobre sua situação.
Não Deixe Sua Saúde Esperar! Entre em Contato Conosco Agora!
☎️ CHAT ONLINE 📞
Entre em contato conosco através da nossa central de atendimento dedicada. Nossos especialistas estão prontos para fornecer orientações personalizadas e responder a todas as suas perguntas. Juntos, podemos trabalhar para garantir o melhor para a sua saúde.
🩺(98)991304454 & (98)988664454📲
ATENDIMENTO REMOTO (TELEMEDICINA)
🤳🏻 Agende com os nossos #especialistas pelo WhatsApp ou Telefone
📲 👩🏽⚕️ Clínico: (98) 9 9130 4454
📲 👨🏻⚕️ Cirúrgico: (98) 9 8866 4454
#TromboseHemorroidária #SaúdeDigestiva #TratamentoHemorroidário #BemEstar #CuidadosComASaúde
VEJA AQUI ONDE FAZER UMA AVALIAÇÃO ESPECIALIZADA E RECEBER UMA SEGUNDA OPINIÃO
Leadership in SURGICAL TEAM

Leadership is a process of social influence in which one person can enlist the aid and support of others in the accomplishment of a common task. Successful leaders can predict the future and set the most suitable goals for organizations. Effective leadership among medical professionals is crucial for the efficient performance of a healthcare system. Recently, as a result of various events and reports such as the ‘Bristol Inquiry’, and ‘To Err is Human’ by the Institute of Medicine, the healthcare organizations across different regions have emphasized the need for effective leadership at all levels within clinical and academic fields. Traditionally, leadership in clinical disciplines needed to display excellence in three areas: patient care, research and education.
Within the field of surgery, the last decade has seen various transformations such as technology innovation, changes to training requirements, redistribution of working roles, multi-disciplinary collaboration and financial challenges. Therefore, the current concept of leadership demands to set up agendas in line with the changing healthcare scenario. This entails identifying the needs and initiating changes to allow substantive development and implementation of up-to-date evidence. This article delineates the definition and concept of leadership in surgery. We identify the leadership attributes of surgeons and consider leadership training and assessment. We also consider future challenges and recommendations for the role of leadership in surgery.
PRINCIPLES OF LEADERSHIP FOR GENERAL SURGEONS
BILIARY-ENTERIC ANASTOMOSIS
 The operative conduct of the biliary-enteric anastomosis centers around three technical steps: 1) identification of healthy bile duct mucosa proximal to the site of obstruction; 2) preparation of a segment of alimentary tract, most often a Roux-en-Y jejunal limb; and 3) construction of a direct mucosa-to-mucosa anastomosis between these two. Selection of the proper anastomosis is dictated by the indication for biliary decompression and the anatomic location of the biliary obstruction. A right subcostal incision with or without an upper midline extension or left subcostal extension provides adequate exposure for construction of the biliary-enteric anastomosis. Use of retractors capable of upward elevation and cephalad retraction of the costal edges are quite valuable for optimizing visual exposure of the relevant hilar anatomy.
The operative conduct of the biliary-enteric anastomosis centers around three technical steps: 1) identification of healthy bile duct mucosa proximal to the site of obstruction; 2) preparation of a segment of alimentary tract, most often a Roux-en-Y jejunal limb; and 3) construction of a direct mucosa-to-mucosa anastomosis between these two. Selection of the proper anastomosis is dictated by the indication for biliary decompression and the anatomic location of the biliary obstruction. A right subcostal incision with or without an upper midline extension or left subcostal extension provides adequate exposure for construction of the biliary-enteric anastomosis. Use of retractors capable of upward elevation and cephalad retraction of the costal edges are quite valuable for optimizing visual exposure of the relevant hilar anatomy.

Division of the ligamentum teres and mobilization of the falciform ligament off the anterior surface of the liver also facilitate operative exposure; anterocephalad retraction of the ligamentum teres and division of the bridge of tissue overlying the umbilical fissure are critical for optimal visualization of the vascular inflow and biliary drainage of segments II, III, and IV. Cholecystectomy also exposes the cystic plate, which runs in continuity with the hilar plate. Lowering of the hilar plate permits exposure of the left hepatic duct as it courses along the base of segment IVb. In cases of unilateral hepatic atrophy as a result of long-standing biliary obstruction or preoperative portal vein embolization, it is critical to understand that the normal anatomic relationships of the portal structures are altered. In the more common circumstance of right-sided atrophy, the portal and hilar structures are rotated posteriorly and to the right; as a result, the portal vein, which is typically most posterior, is often encountered first; meticulous dissection is necessary to identify the common bile duct and hepatic duct deep within the porta hepatis.
BILIARY-ENTERIC ANASTOMOSIS_THECNICAL ASPECTS
GASTROINTESTINAL STROMAL TUMORS (GIST)

INTRODUÇÃO
GIST, da sigla em inglês gastrointestinal stromal tumors, pertence a um grupo de tumores chamados sarcoma de partes moles. Essa neoplasia se diferencia dos outros tipos de tumores por iniciar-se na parede dos órgãos, junto às camadas musculares do trato gastrointestinal, mais especificamente, nas células do plexo mioenterico, chamadas células de Cajal. Tais células são responsáveis pela motilidade intestinal, sendo consideradas o marca-passo do trato gastrointestinal.
O tumor de GIST é relativamente raro, com estudos atuais mostrando uma prevalência anual em torno de 20 a 40 casos por milhão de habitantes. É mais comum entre pessoas de 50 a 60 anos de idade, sendo extremamente raros até os 20 anos. Por representar um tumor raro, recomenda-se que seja tratado por serviços especializados com cirurgiões do aparelho digestivo, que tenham experiência multidisciplinar na condução e no tratamento dos pacientes com este tumor.
O GIST pode se originar em qualquer local do trato gastrointestinal, do esôfago ao ânus. Em relação à distribuição, 50% a 60% das lesões são provenientes do estômago, 20% a 30% do intestino delgado, 10% do intestino grosso, 5% do esôfago e 5% de outros locais da cavidade abdominal.
DIAGNÓSTICO
A apresentação clínica dos pacientes portadores de GIST não é especifica e depende da localização e do tamanho do tumor. O GIST tem uma característica biológica que é uma mutação genética, com ativação do proto-oncogene Kit e a superexpressão do receptor tirosina quinase (c-Kit). Geralmente, o diagnóstico é feito por uma biópsia da lesão, que a depender da localização, pode ser feita por endoscopia, colonoscopia, ou ecoendoscopia. A tomografia computadorizada do abdômen é importante para avaliação da extensão do tumor e também pode ser utilizada em alguns casos para realização de biópsia do tumor. Não apresentam sinais e/ou sintomas específicos. Podem causar náuseas, vômitos, hemorragias intestinais (vômitos com sangue ou evacuações com sangue ou fezes enegrecidas), sensação de plenitude após alimentação, dor e distensão abdominal, ou presença de uma massa ou tumor palpável no abdômen.
TRATAMENTO
O tratamento padrão para pacientes com GIST não metastático, ou seja, não provenientes de outros órgãos, é a ressecção cirúrgica completa da lesão. Muitas vezes é necessária a cirurgia radical e de grande porte, com a retirada de estruturas e órgãos aderidos, oferecendo a maior chance de cura. O tratamento com imatinib, e mais atualmente ao sunitinib, é utilizado para doença metastática ou irressecável, com intuito de diminuir o tamanho da lesão para que a cirurgia possa ser realizada em melhores condições locais. Tais drogas também podem ser utilizadas após a cirurgia. Para o tratamento sistêmico pode ser necessário estudo genético específico para saber qual a mutação presente no tumor, com intuito de guiar a terapia em relação à dose e tipo de medicação utilizada.
FATORES DE RISCO
Não há fatores de risco diretamente relacionados a essa neoplasia. Manter hábitos de vida saudáveis, uma alimentação balanceada e a prática de exercícios físicos ajudam, de maneira geral, na prevenção do câncer.
PARA MAIS INFORMAÇÕES: http://www.gistsupport.org/
“Not only SURGEONS…”

“… We need a system… which will produce not only surgeons but surgeons of the highest type,…men to study surgery and to devote their energy and their lives to raising the standard of surgical science…”
WS Halsted – Bull Johns Hopkins Hosp 15: 267, 1904.
Avanços no tratamento cirúrgico das METÁSTASES HEPÁTICAS DE ORIGEM COLORRETAL

O câncer colorretal é o terceiro tumor mais frequente no ocidente. Cerca de 50% dos pacientes desenvolvem metástases hepáticas na evolução da doença, as quais são responsáveis por, no mínimo, dois terços das mortes. O avanço nas técnicas cirúrgicas e a melhora dos esquemas quimioterápicos têm permitido oferecer tratamento com intuito curativo a um número cada vez maior de pacientes. Os avanços recentes do tratamento das metástases hepáticas, incluindo estratégias para aumentar as ressecções (por exemplo: embolização da veia porta, ablação por radiofrequência, hepatectomia em dois tempos, quimioterapia de conversão e estratégia inversa de tratamento) e hepatectomias na presença de doença extra-hepática possibilitam uma melhor sobrevida dos pacientes.
TRANSPLANTE DE FÍGADO
Este artigo é destinado a pacientes que irão passar por um transplante hepático e seus familiares. Ele visa esclarecer dúvidas comuns e fornecer informações importantes para enfrentar a experiência de forma mais tranquila e informada.
1. Quando está indicado o transplante?
O transplante hepático é recomendado em casos de:
- Cirrose Hepática: Quando exames mostram função hepática diminuída ou sintomas como ascite, sangramento digestivo, encefalopatia hepática ou peritonite bacteriana.
- Hepatocarcinoma: Tumores originários do fígado, muitas vezes associados à cirrose, podem ser tratados com transplante.
- Colangite Esclerosante e Obstrução Intratável de Vias Biliares: Doenças que causam obstrução das vias biliares e infecções graves.
- Hepatite Fulminante e Perda do Fígado Transplantado: Em casos de hepatite grave ou perda do enxerto transplantado dentro de 30 dias, a urgência é priorizada.
2. Quais são as contra-indicações ao transplante hepático?
Não é indicado realizar o transplante em situações como:
- Doença avançada em outros órgãos.
- Tumores fora do fígado.
- Abuso atual de drogas ou álcool.
- Incapacidade de seguir orientações médicas.
- Infecção ativa (o transplante pode ser realizado após a infecção ser controlada).
A idade avançada não é mais uma contra-indicação absoluta, mas deve ser avaliada individualmente.
3. A fila de transplante
Atualmente, a fila de transplante no Brasil é organizada pelo sistema Meld/Peld, que prioriza pacientes com base na gravidade da doença. A fila é subdividida por grupo sanguíneo (A, B, AB, O) e compatibilidade com o tamanho do paciente. Pacientes com grupo sanguíneo raro (AB) podem receber órgãos de todos os grupos.
4. O fígado “não ideal” (marginal)
Órgãos “não ideais” ou marginais podem ter características menos perfeitas, como mais gordura ou doadores com condições subótimas. Eles são destinados a pacientes com necessidades urgentes, como aqueles com tumores hepáticos.
5. A equipe
A equipe de transplante é composta por diversos profissionais, incluindo médicos, enfermeiros, nutricionistas, psicólogos e fisioterapeutas. Cada paciente passa por avaliações detalhadas de todos esses profissionais.
6. Como proceder em caso de emergências durante a espera pelo transplante
Em situações urgentes, dirija-se ao pronto-socorro ou entre em contato com sua equipe médica. As emergências incluem:
- Vômitos com sangue.
- Fezes com sangue ou escurecidas.
- Queda de pressão, mal-estar súbito.
- Colangite (febre, dor abdominal, icterícia).
- Peritonite (infecção abdominal).
7. As reuniões com a Coordenação de Enfermagem de Transplantes
Reuniões regulares são realizadas para pacientes na fila e seus familiares, oferecendo a oportunidade de trocar experiências, fazer perguntas e receber atualizações sobre a lista de espera.
8. A doação de órgãos através de doador em morte encefálica
A doação é um ato voluntário feito com consentimento familiar. O paciente deve estar em morte encefálica, uma condição onde não há atividade cerebral, mas o coração e outros órgãos ainda funcionam. A entidade responsável é o Rio Transplante e os dados do doador são confidenciais.
9. Chamada para o transplante
Mantenha-se disponível e acessível para a equipe de transplante, com telefone atualizado e a uma distância máxima de duas horas do hospital. Caso seja chamado, esteja preparado para o possível ajuste no órgão doado.
A CIRURGIA DE TRANSPLANTE HEPÁTICO
A cirurgia dura entre 5 a 8 horas e é dividida em duas etapas principais:
- Captação: Retirada do fígado doado, que pode ser considerado apto, marginal ou inapto.
- Transplante: O fígado doente é retirado e o novo órgão é implantado, com a realização das anastomoses das veias, artéria hepática e via biliar.
Pós-operatório Imediato
Você será monitorado na UTI por aproximadamente 48 horas. Equipamentos como tubos respiratórios, eletrodos, sondas e drenos serão usados para garantir segurança e monitoramento.
Pós-operatório
A internação média é de 2 semanas, variando conforme o paciente. É importante realizar exames regularmente e seguir orientações médicas para movimentação e exercícios respiratórios.
Medicação
Os imunosupressores, fornecidos pelo SUS, são essenciais para evitar a rejeição do transplante. Familiarize-se com o processo de obtenção e renovação desses medicamentos. Outras medicações de rotina devem ser providenciadas pela família.
Intercorrências após o Transplante
Monitorar sinais de rejeição e infecções é crucial. Mantenha-se saudável, evite álcool e siga as orientações médicas rigorosamente.
Alta Hospitalar
Antes da alta, você receberá orientações detalhadas e agendamentos para consultas e exames. Siga as recomendações de fisioterapia, nutrição e outros cuidados necessários.
Seguimento Inicial e Tardio
O acompanhamento pós-transplante é fundamental. As consultas variam ao longo do tempo, com exames laboratoriais e visitas regulares ao hospital.
Efeitos Colaterais
Os imunosupressores podem causar efeitos colaterais, como tremores e aumento da glicose. Informe seu médico sobre qualquer efeito adverso e não suspenda a medicação por conta própria.
Cuidados Gerais
Controle o peso, colesterol, glicose e pressão arterial. Evite bebidas alcoólicas, use máscara em locais públicos, evite contato com pessoas doentes e exposição solar excessiva. Mantenha acompanhamento ginecológico e dentário regular e consulte seu médico antes de tomar novos medicamentos. Este artigo é uma referência para ajudar você a entender e gerenciar o processo de transplante hepático. Mantenha-se em contato com sua equipe médica para qualquer dúvida ou preocupação.
A cirurgia é uma forma de terapia para as doenças que é motivada pelo CORAÇÃO, planejada na CABEÇA e executada pelas MÃOS.
“A cirurgia é uma forma de terapia para as doenças que é motivada pelo CORAÇÃO, planejada na CABEÇA e executada pelas MÃOS.”
Prof . Phd. Tom DeMeester
DEFINIÇÃO DE CIRURGIA (By Tom DeMeester / Gastrão 2012)










