30 de Julho | Dia do Cirurgião Geral
A jornada cirúrgica começa muito antes de alguém ser reconhecido como cirurgião. Desde cedo, na faculdade ou até antes, os estudantes enfrentam a competitividade intensa da medicina, especialmente na cirurgia. As escolhas entre seguir o que realmente gostam ou o que é necessário para alcançar o próximo passo são constantes. É fácil perder de vista o porquê de querer se tornar médico ou cirurgião em primeiro lugar, ao se prender ao que é exigido pelo caminho.

A medicina e a cirurgia são profissões que requerem conhecimento extenso e habilidades apuradas. Também exigem discrição e confiabilidade, com um contrato social que mantém os profissionais a padrões elevados de competência e responsabilidade moral. Como Tom Krizek explica, uma profissão é uma declaração de um modo de vida “em que o conhecimento especializado é usado não primariamente para ganho pessoal, mas para o benefício daqueles que precisam desse conhecimento.”
Desafios Éticos na Escola de Medicina
Os desafios éticos para os estudantes de medicina são muitos. Inicialmente, chegam com intenções altruístas e preocupações com a segurança financeira, dada a alta despesa da educação médica. Isso pode influenciar os graduados a escolherem especializações que permitam pagar suas dívidas mais rapidamente, impactando negativamente o sistema de saúde ao reduzir a disponibilidade de provedores de cuidados primários.
Durante a formação clínica, os estudantes começam a interagir com pacientes e enfrentam dilemas sobre como lidar com as opções de tratamento e os eventos adversos associados. As demandas acadêmicas podem ser avassaladoras, e os valores humanísticos podem se perder, fazendo com que vejam as interações com pacientes como obstáculos. Nesse período, decidem qual especialidade seguirão e precisam entender a vida de um cirurgião e se conseguem equilibrar essa carreira com uma vida familiar satisfatória.
Residência Cirúrgica: Teste de Resistência e Resiliência
Os residentes cirúrgicos iniciantes enfrentam uma carga de trabalho imensa e exaustão, vendo, por vezes, a doença como “o inimigo” a ser vencido. Precisam aprender a construir relações de confiança com os pacientes e lidar com a morbidade e mortalidade resultantes de suas ações. É crucial que compartilhem suas experiências com amigos e familiares para obter suporte. Nos níveis intermediários, a responsabilidade aumenta, com ênfase no conhecimento técnico e na ética, além de ensinar e liderar residentes mais novos. O residente sênior deve coordenar eficientemente a equipe, ensinar e tomar decisões complexas, preparando-se para a carreira definitiva.
O Cirurgião Completo: Equilíbrio Entre Pressão e Ética
O cirurgião treinado precisa diferenciar entre incentivos financeiros e o que é certo para o paciente. As pressões profissionais intensificam o desafio de equilibrar cuidados com pacientes, família, educação, ensino e pesquisa. Tomar decisões corretas, como escolher entre um evento familiar importante e uma cirurgia, é um dilema frequente. É essencial lembrar que a presença na vida dos filhos é única e insubstituível.
Sabendo Quando Parar
Para os cirurgiões seniores, como aqueles acima de 65 anos considerando aprender nova tecnologia robótica, surge a reflexão sobre quando desacelerar ou parar. Murray Brennan resume bem o dilema do cirurgião sênior que se sente frustrado com a perda de autonomia devido às regulamentações e restrições, levando muitos a abandonar a prática.
Concluindo com Graça
Cada cirurgião deve continuamente traçar um caminho que integre objetivos pessoais e profissionais, mantendo valor, equilíbrio e satisfação. Devem cultivar hábitos de renovação pessoal, autoconsciência emocional e conexão com colegas, encontrando significado genuíno no trabalho para enfrentar os desafios. Como descrito por Rothenberger, o cirurgião mestre sabe quando aplicar ou alterar regras e quando a inação é a melhor opção. Esse indivíduo raro combina habilidades cognitivas, técnicas e de tomada de decisão para atender às necessidades específicas do paciente, demonstrando intuição clínica, criatividade e humildade.
“Um cirurgião é tão bom quanto seu último procedimento, mas é a reflexão constante e a busca pela melhoria que define a excelência.”
Gostou❓ Nos deixe um comentário ✍️, ou mande sua dúvida pelo 💬 Chat On-line em nossa DM do Instagram.
#Medicina #Cirurgia #CarreiraCirúrgica #VidaDeCirurgião #ÉticaMédica
A Essência de uma Carreira Cirúrgica: Você Está Pronto?
Ingressar em uma carreira cirúrgica é uma jornada para uma profissão intelectualmente exigente, profundamente satisfatória e incrivelmente recompensadora. A cada ano, mais pessoas se candidatam a se tornar cirurgiões do que há vagas disponíveis, destacando o atrativo e o prestígio desse campo. No entanto, ter sucesso nesse caminho requer mais do que apenas excelência acadêmica; exige uma combinação única de habilidades e atributos pessoais.
A Cirurgia é a Carreira Certa para Você?
Para se destacar na cirurgia, você deve possuir as seguintes qualidades:
- Conhecimento Especializado: Diagnósticos precisos dependem de um extenso conhecimento médico.
- Habilidades de Comunicação: A interação eficaz com equipes médicas, pacientes e famílias é crucial. Ouvir e conquistar confiança são componentes chave.
- Destreza Manual: A habilidade manual é essencial para a prática cirúrgica.
- Experiência em Cuidados: Experiência em cuidados pré e pós-operatórios é indispensável.
- Adaptabilidade: À medida que a medicina evolui, suas habilidades e técnicas também devem evoluir.
- Liderança: Orientar uma equipe e mentorar futuros cirurgiões requer liderança forte.
- Resiliência Emocional: Lidar com situações difíceis com calma e apoiar sua equipe são vitais.
- Curiosidade Intelectual: O desejo de aprender continuamente e melhorar é essencial.

Características de um Bom Cirurgião
Ser um bom cirurgião é subjetivo e varia de acordo com as perspectivas de colegas, pacientes e a comunidade em geral. No entanto, os elementos fundamentais permanecem consistentes:
- Destreza Manual: Esta é a base do trabalho cirúrgico. Sem mãos habilidosas, um cirurgião não pode operar.
- Conhecimento Clínico: Uma compreensão abrangente dos princípios médicos e científicos é vital.
Equilibrando Habilidades e Conhecimento
Os cirurgiões frequentemente se destacam em habilidades técnicas ou conhecimento teórico, mas os melhores combinam ambos. Um técnico brilhante pode carecer de profundidade em teoria médica, enquanto um cirurgião bem instruído pode não ser tão habilidoso na sala de operações. O cirurgião ideal encontra um equilíbrio entre esses extremos, proporcionando um atendimento abrangente.
Traços de Personalidade
Resiliência física e psicológica, capacidade de trabalhar sob pressão e a capacidade de improvisar são indispensáveis. Capacidade intelectual, honestidade, coragem e comunicação eficaz definem ainda mais um cirurgião de sucesso. Liderança e a habilidade de inspirar confiança tanto em pacientes quanto em membros da equipe também são críticas.
O Papel do Bom Senso
O bom senso preenche a lacuna entre o conhecimento teórico e a aplicação prática. É uma qualidade inata que permite a alguns cirurgiões interpretar intuitivamente os dados dos pacientes e tomar decisões acertadas. Aqueles com bom senso podem dissecar tecidos com precisão e tomar a difícil decisão de quando não operar, garantindo os melhores resultados para seus pacientes.
Conclusão
“A cirurgia requer um equilíbrio de habilidades e conhecimento, aprimorados pela resiliência e pelo bom senso. Como René Leriche afirmou de forma eloquente, ‘Devemos pensar no propósito da nossa arte e entender especialmente o lado humano de alguns problemas terapêuticos.'”
Gostou? Nos deixe um comentário ✍️, ou mande sua dúvida pelo 💬 Chat On-line em nossa DM do Instagram.
#CarreiraCirúrgica #EducaçãoMédica #HabilidadesCirúrgicas #FuturosCirurgiões #TreinamentoCirúrgico
Código de Conduta Cirúrgica (NOTTS3)
Imagine um ambiente onde a precisão é vital, a comunicação é essencial e cada membro da equipe desempenha um papel crucial no bem-estar do paciente. Este é o cenário da sala de cirurgia (OR). Se a etiqueta da OR representa um código de conduta – respeito, comunicação, modelo mental compartilhado e trabalho em equipe – as boas maneiras representam os comportamentos que personificam esse código. Regras simples que deveriam ter sido aprendidas desde cedo, mas que, com algumas orientações, podem integrar de maneira eficaz residentes juniores e estudantes na equipe da OR.
Aqui estão algumas diretrizes essenciais:
- Seja educado.
- Seja respeitoso.
- Seja humilde.
- Aprenda os nomes de todos.
- Ofereça ajuda sem ser solicitado.
- Peça ajuda quando necessário.
- Agradeça aos seus colegas.
- Mantenha o paciente no centro de todas as suas ações.
Comportamentos rudes, disruptivos ou desrespeitosos não são tolerados. Não grite nem faça comentários sarcásticos. Evite piadas com temas sexuais ou raciais. Não fofoque nem calunie os outros. Muitos cirurgiões gostam de ouvir música na sala de cirurgia, mas ao escolher uma playlist, esteja ciente de que algumas músicas podem ter letras ofensivas que não devem ser reproduzidas no local de trabalho. É mais educado perguntar antes de tocar música e verificar as preferências musicais, pois nem todos na OR podem apreciar um metal pesado e estridente. A música deve ser desligada durante momentos críticos, como a pausa inicial.
Os cirurgiões utilizam as redes sociais como muitas outras pessoas, mas a OR não é o lugar para verificar o Facebook ou o Instagram. Ao postar nas redes sociais, seja profissional – qualquer coisa postada na internet pode ser capturada em tela e espalhada, não importando quais configurações de privacidade você tenha ativado. Um estudo recente de postagens publicamente acessíveis no Facebook mostrou que 14,1% dos residentes em cirurgia postaram conteúdo potencialmente não profissional, e 12,2% postaram conteúdo claramente não profissional, com violações da privacidade do paciente sendo um dos problemas mais comuns, juntamente com descrições de bebedeiras e material ofensivo racial ou sexualmente. Especificamente na OR, esteja ciente de que postagens nas redes sociais com informações potencialmente identificáveis do paciente são absolutamente proibidas. Isso não precisa incluir o nome do paciente para ser informação identificável – alguns detalhes de um caso particularmente único e uma postagem com carimbo de data e hora podem ser suficientes para causar problemas.
Em suma, “As boas maneiras são a moeda da sala de cirurgia,” como uma vez disse William Halsted. Seguir essas diretrizes não só promoverá um ambiente mais harmonioso, mas também garantirá que o foco principal permaneça onde deve estar: no bem-estar do paciente.
Liderança no Centro Cirúrgico (NOTTS2)
A análise dos erros médicos mostrou que mais de dois terços envolvem questões de comunicação da equipe, contribuídas por problemas de cultura institucional e de equipe. Esses erros podem incluir comunicação perdida, comunicação imprecisa ou incapacidade ou falta de vontade dos membros da equipe de falar, todas relacionadas à cultura de uma equipe ou instituição e dramaticamente afetadas pelo tom e clima estabelecidos pelos líderes cirúrgicos, dentro e fora da sala de operação. Toda equipe e instituição têm uma ‘cultura de segurança’—as atitudes, comportamentos e expectativas que afetam os resultados dos pacientes para melhor ou pior. Há evidências crescentes de que essa cultura de segurança afeta diretamente tanto a morbidade quanto a mortalidade. Por exemplo, em um estudo de 31 hospitais na Carolina do Sul, a cultura de segurança institucional estava diretamente relacionada à morte de pacientes. Para cada mudança de 1 ponto (em uma escala de 7 pontos) nas pontuações dos hospitais em respeito, liderança clínica e assertividade, a mortalidade em 30 dias após a cirurgia diminuiu de 29% para 14%. Em outro exemplo, medidas de cultura de segurança em 22 hospitais em Michigan previram diretamente os resultados dos pacientes após a cirurgia bariátrica. Nesse estudo, quando as enfermeiras classificaram a coordenação das equipes do centro cirúrgico como aceitável, em vez de excelente, as complicações graves foram 22% mais prováveis.
A Equipe da Sala de Operação
Uma vez, Hipócrates disse: ‘O médico deve… ter dois objetivos especiais em vista com relação à doença, a saber, fazer o bem ou não causar dano.’ O ato de cirurgia é inerentemente baseado em equipe. Cada operação requer que o cirurgião trabalhe de perto e de forma eficaz com seus assistentes, provedores de anestesia, equipe de enfermagem, tecnólogos cirúrgicos e membros da equipe auxiliar para fazer a sala de operação funcionar. Os membros da equipe frequentemente entram e saem da sala de operação, com troca de turno ou para pausas, e membros adicionais da equipe podem ser necessários para cuidados especializados ou de emergência. O importante é lembrar que o paciente está no centro da equipe, assim a frase ‘cuidados centrados no paciente.’ Sempre tenha em mente que a segurança e o bem-estar do paciente estão no coração de todos os nossos esforços. É especialmente importante que todos os membros da equipe tenham um ‘modelo mental compartilhado’—uma compreensão comum das questões, tanto médicas quanto logísticas, que possam afetar o curso de uma operação. Isso permite uma maior eficiência, melhor consciência situacional e melhor capacidade de reconhecer e responder a problemas. Aqui descrevemos os indivíduos comumente encontrados na sala de operação.
Os Cirurgiões
Galeno certa vez observou: ‘Onde há amor pela arte da medicina, há amor pela humanidade.’ Cada equipe cirúrgica consistirá de um cirurgião titular, geralmente acompanhado por um ou mais assistentes. No ambiente de aprendizado, é importante que os cirurgiões discutam papéis e responsabilidades, bem como metas educacionais para o caso, que podem variar dependendo do nível de treinamento e experiência dos membros da equipe. Um conceito importante na educação cirúrgica é a ‘autonomia progressiva,’ na qual os aprendizes têm permissão para assumir cada vez mais responsabilidades em uma operação com base no seu nível de competência. Uma discussão pré-operatória entre o cirurgião e o residente é fundamental para uma compreensão clara de quais partes da operação o aprendiz pode realizar e quando o titular pode precisar assumir o controle do caso. É responsabilidade de cada membro da equipe do cirurgião revisar o caso do paciente em detalhes para entender seu histórico médico e cirúrgico passado, sua doença atual e como ela tem sido gerida até o momento, medicamentos relevantes e revisão de todos os estudos diagnósticos para antecipar dificuldades que possam ser encontradas durante a operação. Secundariamente, cabe a cada membro discutir o caso com outros membros da equipe para garantir que todos tenham um modelo mental compartilhado do plano operatório, do plano pós-operatório e de quaisquer dificuldades antecipadas. Durante a operação, o paciente é o foco da equipe. Cada indivíduo é esperado para fazer sua parte para avançar a operação enquanto ajuda outros membros da equipe a fazer o mesmo. Após a operação, é importante discutir o cuidado pós-operatório, como manejo da dor, restrições alimentares, profilaxia de tromboembolismo venoso e a necessidade de novos ou existentes medicamentos prescritos.
Hierarquia Cirúrgica
Embora a sala de operação possa parecer um ambiente altamente regimentado, cada membro da equipe cirúrgica servirá como ‘líder’ e ‘seguidor’ em diferentes momentos durante a operação. Isso inclui todos, desde o cirurgião titular mais experiente até o estudante de medicina mais júnior. Dentro da sala de operação, o cirurgião titular tem a responsabilidade final pelo paciente. No entanto, os residentes cirúrgicos muitas vezes atuam como líderes para residentes juniores e estudantes de medicina. No contexto de ‘autonomia progressiva’ para residentes cirúrgicos, o cirurgião titular também pode formal ou informalmente ceder o controle do caso ao residente ou bolsista e pode assumir um papel de seguidor ele mesmo. De fato, mais frequentemente do que não, o cirurgião titular assistirá um residente sênior durante um caso, em vez de realizar a operação com a assistência do residente. Na sala de operação, o líder da equipe é responsável por definir a cultura de segurança e abordar as questões em questão, apoiar a equipe e fornecer feedback quando a equipe se desvia do curso esperado. Notavelmente, os papéis de líderes e seguidores não são fixos—equipes eficazes permitem que os indivíduos se movam entre os dois papéis de forma fluida conforme as necessidades da equipe ditam. Assim, na sala de operação, todos os membros da equipe devem ser tanto líderes quanto seguidores eficazes conforme a situação exigir. Nas palavras de William Osler, “O bom médico trata a doença; o grande médico trata o paciente que tem a doença.” Em última análise, o coração da comunicação eficaz na sala de operação é uma cultura de respeito mútuo, modelos mentais compartilhados e o compromisso de cada membro da equipe em priorizar a segurança do paciente acima de tudo. Ao abraçar esses princípios, podemos reduzir erros, melhorar os resultados e fornecer o mais alto padrão de cuidado aos nossos pacientes.
Comunicação Cirúrgica (NOTTS1)
Uma das determinantes mais importantes para uma operação bem-sucedida é a comunicação contínua e eficaz entre todos os membros da equipe cirúrgica. O objetivo é que cada membro da equipe tenha um entendimento comum sobre o paciente, a operação proposta e o fluxo esperado do caso – o chamado “modelo mental compartilhado”. Uma das ferramentas de comunicação mais comuns usadas neste cenário é a pausa cirúrgica ou “time-out”. Embora muitas instituições usem uma pausa cirúrgica, muitas dessas são desestruturadas e, portanto, perdem uma oportunidade de incutir uma cultura de comunicação.
Para combater isso, recomendamos fortemente o uso de uma lista de verificação estruturada e formalizada como parte da pausa cirúrgica. O protótipo para esse tipo de processo estruturado é a Lista de Verificação de Segurança Cirúrgica da Organização Mundial da Saúde (OMS). Introduzida em 2008, a lista de verificação da OMS é composta por 19 pontos a serem usados em três momentos – imediatamente quando o paciente entra na sala de cirurgia (antes da indução da anestesia), pouco antes da incisão na pele e pouco antes de o paciente deixar a sala de cirurgia.
A lista de verificação foi testada em oito cidades ao redor do mundo para avaliar seu impacto na morbidade e mortalidade dos pacientes. Em um estudo de antes e depois, os investigadores descobriram que a implementação da lista de verificação estava associada a uma redução significativa na taxa de mortalidade (1,5% vs. 0,8%, p < 0,01) e complicações intra-hospitalares (11,0% vs. 7,0%, p < 0,01). Embora a lista de verificação tenha sido amplamente saudada como um sucesso, alguns críticos afirmam que não é a lista de verificação em si que reduz as complicações, mas sim o fato de que a lista de verificação proporciona uma oportunidade para que a equipe se reúna e discuta elementos críticos que não devem ser esquecidos. Em nossa opinião, não importa como a lista de verificação funciona, apenas que funcione.
Vários estudos adicionais mostraram outros benefícios da introdução de uma lista de verificação formalizada, incluindo a redução da mortalidade, morbidade e tempo de permanência hospitalar, conforme demonstrado em um estudo randomizado controlado recente que mostrou redução nas complicações de 19,9% para 11,5% com a introdução da lista de verificação. Apesar disso, alguns outros estudos de listas de verificação cirúrgicas não mostraram melhorias nos resultados. Isso parece ser devido a problemas de implementação, com grandes variações na implementação entre instituições e até mesmo entre diferentes especialidades dentro de uma instituição, sendo comum a implementação subótima.
Instituições que adotam uma lista de verificação apenas nominalmente, mas cujos membros da equipe ignoram ou minimizam o processo, dificilmente colherão os benefícios. Por outro lado, instituições que desenvolvem uma forte cultura de segurança com uma implementação robusta e obrigatória verão melhores resultados. Isso destaca a importância da etiqueta na sala de operação – o código de conduta que regula nossas ações. Para obter o máximo benefício da lista de verificação de segurança cirúrgica, todos os membros da equipe devem estar presentes e engajados ativamente no processo. A música deve ser desligada, conversas paralelas interrompidas, e toda a atenção deve estar focada nos itens da lista de verificação e em como eles se relacionam com o paciente.
Normalmente, é papel do cirurgião chefe, do fellow ou do residente liderar a lista de verificação. Como líder designado, é importante revisar e discutir cada item individual na lista de verificação. Isso inclui garantir que todos os membros da equipe se apresentem e deixar claro que todos na sala de operação estão capacitados para falar se perceberem uma situação potencialmente insegura. A lista de verificação pode ser modificada por hospitais ou serviços individuais para incluir itens relevantes específicos para sua população de pacientes. Por exemplo, se uma equipe cirúrgica específica tiver itens adicionais que não podem ser esquecidos (por exemplo, processos relacionados à circulação extracorpórea em cirurgia cardíaca), isso pode ser incluído.
Muitas listas de verificação também incluem uma seção de debriefing para uso ao final do caso, incluindo itens como processamento de espécimes, comunicação com a família do paciente e quem acompanhará o paciente para a unidade pós-anestésica ou unidade de terapia intensiva.
O Papel do Feedback na Educação Cirúrgica
O feedback ganhou um papel cada vez mais importante na educação cirúrgica. O feedback pode ser somativo e/ou formativo. O feedback somativo é frequentemente dado em pontos de tempo discretos, como no final de uma rotação, e é a culminação de observações de desempenho. O feedback formativo envolve uma avaliação contínua de habilidades ou conhecimento e pode ser dado ao longo de uma experiência educacional.
Há uma distinção frequentemente mal compreendida entre ensino e feedback. Por exemplo, o ensino é quando o cirurgião chefe corrige o ângulo da agulha do residente durante uma anastomose intestinal. O feedback é quando o cirurgião chefe e o residente se reúnem após o caso e discutem o desempenho – seja técnico ou não técnico. Por exemplo, uma sessão de feedback pode discutir a configuração da sala, eficiência, manobras técnicas e comunicação.
Dar e receber feedback são habilidades distintas que exigem que ambas as partes estejam atentas e abertas. Para facilitar esse processo, vários métodos foram descritos que transformam o feedback em um processo ativo para ambas as partes. Idealmente, o mentor e o trainee fazem um briefing antes do caso para definir objetivos de aprendizado e, em seguida, debriefing formal após o caso para discutir quão bem os objetivos de aprendizado foram alcançados, bem como maneiras de melhorar no futuro.
Na pressa das preocupações clínicas e no impulso pela eficiência, a sessão de debriefing é frequentemente pulada ou perdida. Cabe ao aprendiz, portanto, buscar especificamente e pedir feedback ao cirurgião chefe e, se necessário, agendar horários formais de reunião. Também é importante que o feedback flua em ambas as direções, e o cirurgião chefe deve pedir feedback aos residentes também. Uma boa metodologia para fornecer feedback é fazer uma pergunta aberta, como “Como você achou que essa operação foi?” Que pode ser seguida de “O que correu bem?” e “O que poderia ter sido melhor?” Isso permite que a pessoa que está fornecendo o feedback tenha uma linha de base para começar e permite a autorreflexão por parte do aprendiz. Isso pode ser seguido de feedback específico sobre um ou dois itens acionáveis, de preferência relacionados aos objetivos declarados durante o briefing inicial.
Uma comunicação eficaz e não violenta é a chave para construir um ambiente cirúrgico seguro e colaborativo, onde cada voz é ouvida e cada preocupação é abordada, garantindo que todos trabalhem em harmonia para o bem-estar do paciente. Afinal, uma cirurgia segura salva vidas.
Habilidades Não Técnicas para Cirurgiões (NOTSS)
Introdução ao NOTSS
O sistema de Habilidades Não Técnicas para Cirurgiões (NOTSS) foi desenvolvido por uma equipe na Universidade de Aberdeen, na Escócia, com financiamento do Royal College of Surgeons de Edimburgo e do NHS Education for Scotland. O investigador principal, Dr. Steven Yule, fez parte dessa equipe e agora traz sua experiência e expertise para os Estados Unidos com o Laboratório de Habilidades Não Técnicas no Brigham and Women’s Hospital e na Harvard Medical School. O NOTSS foi desenvolvido a partir do zero com um painel de especialistas em assuntos específicos (cirurgiões consultores e psicólogos) em vez de adaptar uma estrutura existente empregada por outras indústrias. O objetivo do projeto NOTSS era desenvolver e testar um sistema educacional para avaliação e treinamento com base em habilidades comportamentais observáveis na fase intraoperatória da cirurgia (Yule et al. Surg Clin N Am 2012;92:37-50).
O Sistema NOTSS
O sistema NOTSS foi escrito em linguagem cirúrgica para que cirurgiões treinados possam observar, avaliar e fornecer feedback sobre habilidades não técnicas de forma estruturada (Yule et al. Surg Clin N Am 2012;92:37-50). A taxonomia NOTSS é dividida em quatro categorias distintas de habilidades não técnicas: Consciência Situacional, Tomada de Decisão, Comunicação e Trabalho em Equipe, e Liderança (Yule et al. World J Surg 2008;32:548-556), cada uma com elementos associados. Comportamentos bons e ruins foram cuidadosamente escritos para cada elemento.
Fundamentos do Comportamento Aceitável na Sala de Cirurgia
Por mais que a cultura e a prática da cirurgia tenham mudado e evoluído nos últimos séculos, é verdade que a sala de cirurgia (SC) pode ser um lugar intimidador para estudantes de medicina ou residentes juniores. No passado, os cirurgiões muitas vezes tinham a reputação de serem arrogantes ou depreciativos, com histórias frequentes semelhantes a trotes de residentes juniores na SC, ou de comportamento impulsivo e disruptivo direcionado a membros da equipe, como equipe de enfermagem, equipe de anestesia e pessoal de apoio. De fato, esse tipo de comportamento “antiquado” não é mais aceitável, por muitas razões. A SC é um lugar especial, mas ainda é, no final das contas, um local de trabalho, e as normas de trabalho de respeito mútuo e comportamento educado devem ser aplicadas. Na era moderna, é claro que os cirurgiões devem trabalhar de maneira respeitosa e colaborativa com todos os membros da equipe de atendimento ao paciente. Cabe ao cirurgião criar uma atmosfera de respeito mútuo, confiança e comunicação. Isso é frequentemente chamado de “etiqueta da SC”, pois a etiqueta é definida como um código de conduta entre um grupo ou profissão.
Consciência Situacional A Consciência Situacional envolve a percepção e compreensão dos elementos do ambiente de trabalho e a projeção de seu status no futuro próximo. Para cirurgiões, isso inclui a monitorização contínua do paciente, da equipe e do progresso da cirurgia. A habilidade de manter uma visão global do que está acontecendo na SC é crucial para identificar e resolver problemas potenciais antes que se tornem críticos.
Tomada de Decisão A Tomada de Decisão refere-se ao processo de escolher entre diferentes opções de ação com base nas informações disponíveis. Na SC, decisões rápidas e eficazes podem ter um impacto significativo nos resultados do paciente. Cirurgiões devem ser capazes de avaliar situações complexas rapidamente e tomar decisões fundamentadas para garantir a segurança e o bem-estar do paciente.
Comunicação e Trabalho em Equipe A Comunicação e o Trabalho em Equipe são essenciais para o funcionamento eficiente da SC. Isso envolve a troca clara e concisa de informações entre todos os membros da equipe, garantindo que todos estejam cientes do plano cirúrgico e das possíveis complicações. Uma boa comunicação ajuda a coordenar ações, prevenir erros e responder rapidamente a mudanças na condição do paciente.
Liderança A Liderança na SC implica em guiar a equipe, manter a ordem e a disciplina, e ser um exemplo de comportamento profissional. Um bom líder cria um ambiente de trabalho positivo e de apoio, onde todos os membros da equipe se sentem valorizados e motivados a contribuir para o sucesso da cirurgia. Além disso, um líder eficaz é capaz de delegar tarefas adequadamente e fornecer feedback construtivo para melhorar continuamente a performance da equipe.
Conclusão As habilidades não técnicas são tão cruciais quanto as habilidades técnicas para o sucesso na sala de cirurgia. O sistema NOTSS fornece uma estrutura para avaliar e melhorar essas habilidades, promovendo um ambiente cirúrgico mais seguro e eficiente. Ao adotar práticas de Consciência Situacional, Tomada de Decisão, Comunicação e Trabalho em Equipe, e Liderança, os cirurgiões podem garantir que o comportamento aceitável e profissional prevaleça na SC, beneficiando tanto a equipe quanto os pacientes.
Requisitos Fundamentais da Clínica Cirúrgica
Atul Gawande, um autor celebrado por suas perspectivas perspicazes sobre a saúde, especialmente no campo cirúrgico, ofereceu insights valiosos que ressoam com profissionais médicos. Em seu livro “Complicações: Notas de um Cirurgião sobre Desempenho,” Gawande articula três requisitos fundamentais para o sucesso na medicina:
Diligência: Enfatiza a importância da atenção meticulosa aos detalhes para prevenir erros e superar desafios.
Fazer o Certo: Reconhece que a medicina é, inerentemente, uma profissão humana, destacando o imperativo ético de priorizar o bem-estar do paciente.
Ingenuidade: Incentiva uma mentalidade de inovação, instigando os praticantes a pensarem de maneira diferente, abraçar mudanças e aprender com os fracassos.
Gawande vai além de definir esses requisitos fundamentais e oferece cinco sugestões convincentes sobre como indivíduos podem causar um impacto positivo dentro de sua cultura profissional:
Faça uma Pergunta Não Roteirizada: Defende perguntas espontâneas que podem levar a descobertas inesperadas e fomentar uma cultura de comunicação aberta.
Não Reclame: Aconselha contra reclamações improdutivas, enfatizando que isso não resolve problemas nem contribui construtivamente para discussões. Incentiva os indivíduos a estarem preparados com tópicos alternativos para discussão.
Conte Algo: Promove a prática de quantificar aspectos do próprio trabalho. Gawande sugere que contar algo de interesse pessoal leva a insights valiosos e aprendizado contínuo.
Escreva Algo: Reconhece o poder transformador de escrever ou digitar. Encoraja os profissionais a documentarem experiências, insights e reflexões, aprimorando tanto o aprendizado pessoal quanto coletivo.
Mude—Seja um Adaptador Precoce: Reconhece a necessidade de abraçar mudanças, especialmente no panorama em rápida evolução da tecnologia cirúrgica. Instiga os indivíduos a serem adaptadores precoces, mantendo-se atualizados com inovações para aprimorar o cuidado ao paciente.
As orientações de Gawande vão além dos aspectos técnicos da medicina, adentrando os domínios da comunicação, mentalidade e desenvolvimento profissional. Esses princípios fornecem um roteiro para que os profissionais médicos não apenas se destaquem em suas capacidades individuais, mas também influenciem positivamente a cultura mais ampla na qual operam.
“O sucesso na medicina é cultivado não apenas através da habilidade técnica, mas pela dedicação incessante ao aprendizado, inovação e ao compromisso com o bem-estar do paciente.”
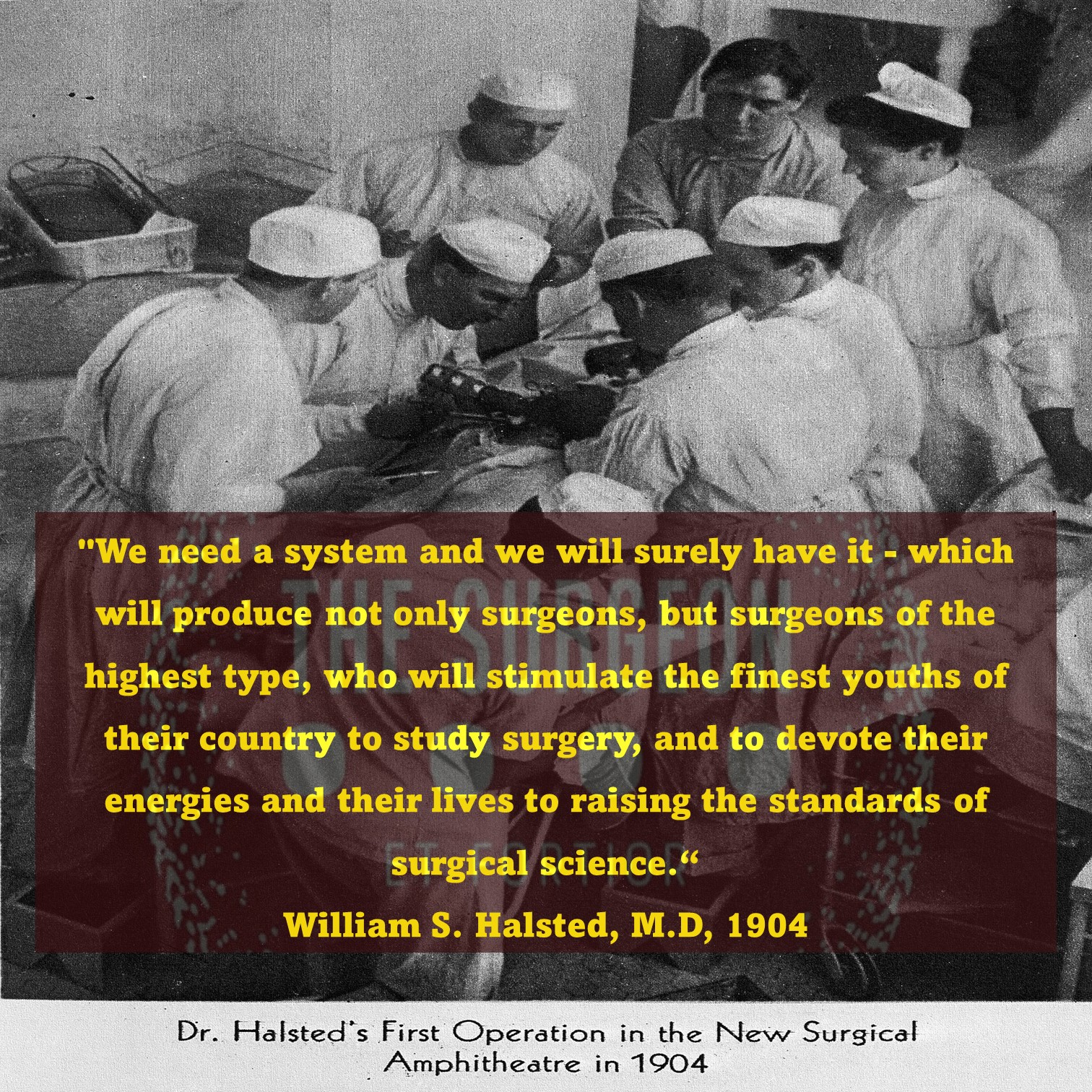
O Legado do Dr. William Stewart Halsted
Pioneiro da Cirurgia Moderna
A história da medicina é marcada por avanços revolucionários que transformaram a prática clínica, o ensino e os cuidados aos pacientes. Entre os nomes que se destacam neste cenário, o do cirurgião norte-americano William Stewart Halsted (1852–1922) é, sem dúvidas, um dos mais influentes. Halsted não apenas elevou os padrões da cirurgia, mas também criou um modelo de treinamento que se tornou a base para a formação de cirurgiões em todo o mundo, com aplicações diretas no tratamento das doenças do aparelho digestivo.
O Início de uma Jornada Brilhante
Nascido em Nova York, Halsted iniciou sua formação acadêmica com forte ênfase em anatomia e fisiologia, que mais tarde se tornariam a base de suas contribuições à medicina. Após se formar na College of Physicians and Surgeons, em 1877, ele ampliou seus horizontes ao estudar em centros de excelência europeus, como Viena e Hamburgo, onde foi influenciado por cirurgiões renomados como Theodor Billroth e Johannes von Mikulicz.
Contribuições ao Tratamento Cirúrgico do Aparelho Digestivo
Entre os muitos campos em que Halsted deixou sua marca, destaca-se a cirurgia do aparelho digestivo. Seu estudo experimental sobre suturas intestinais, realizado no início de sua carreira em Baltimore, estabeleceu as bases para anastomoses seguras e eficazes. Ele demonstrou que a submucosa é a camada crítica para sustentação das suturas, um conceito que permanece fundamental até hoje. Outro marco foi seu pioneirismo em ressecções gastrointestinais e controle de sangramentos intra-abdominais. Sua abordagem técnica, caracterizada por dissecação cuidadosa e manuseio gentil dos tecidos, minimizou complicações como infecção e deiscências, ampliando significativamente as chances de sucesso em cirurgias de alta complexidade.
O Modelo Halstediano de Treinamento Cirúrgico
Um dos legados mais duradouros de Halsted foi seu modelo de residência médica, implementado no Hospital Johns Hopkins. Ele estabeleceu um sistema hierárquico com responsabilidades graduais, permitindo que residentes desenvolvessem habilidades progressivamente. Esse método não apenas garantiu um treinamento mais completo, mas também formou líderes que perpetuaram suas ideias. Para a cirurgia do aparelho digestivo, essa abordagem foi crucial. O treinamento intensivo em anatomia, fisiopatologia e técnicas operatórias sofisticadas possibilitou avanços significativos no manejo de doenças como cânceres gastrointestinais, doenças inflamatórias intestinais e patologias biliares.
Avanços e a Influência no Ensino Moderno
Embora o modelo Halstediano tenha sido modificado ao longo das décadas, seus princípios básicos continuam sendo a espinha dorsal da educação cirúrgica. Programas atuais incorporam avanços tecnológicos, como cirurgia robótica e simulações, mas a ética da responsabilidade progressiva e a atenção aos detalhes, promovida por Halsted, permanecem inalteradas.
Reflexão Final
O legado de William Stewart Halsted é inestimável. Suas contribuições estabeleceram os alicerces da cirurgia moderna, com implicações diretas na melhora do cuidado ao paciente e na educação médica. Para estudantes e residentes, entender sua história é compreender as origens de muitas práticas e conceitos que hoje são considerados padrão na formação e prática cirúrgica.
“A grandeza de um cirurgião não reside apenas em suas habilidades técnicas, mas na sua dedicação contínua em aprimorar a arte de curar.” – William Stewart Halsted.
Gostou ❔ Nos deixe um comentário ✍️ , compartilhe em suas redes sociais e|ou mande sua dúvida pelo 💬 Chat On-line em nossa DM do Instagram.
Hashtags:
#CirurgiaDigestiva #EducaçãoMédica #HistóriaDaCirurgia #ResidênciaMédica #WilliamHalsted
Maestria na Cirurgia Digestiva
Em seu aclamado livro “Fora de Série: Outliers – Descubra Por Que Algumas Pessoas Têm Sucesso e Outras Não”, Malcolm Gladwell explora a essência da maestria, destacando a regra das 10.000 horas popularizada pelo neurologista Daniel Levitin. Esta regra postula que são necessárias impressionantes 10.000 horas de prática dedicada para alcançar a maestria e a excelência em qualquer campo. Gladwell examina diversos campos, de compositores e jogadores de basquete a escritores de ficção e cirurgiões, encontrando o fio condutor recorrente da marca de 10.000 horas.
A Discrepância no Treinamento Cirúrgico ⏰🔍
No contexto do treinamento cirúrgico, no entanto, uma diferença marcante surge. Residentes chefes de cirurgia em formação são encarregados de documentar aproximadamente 850 casos, muito aquém do marco das 10.000 horas. Mesmo considerando uma estimativa de 2 horas por caso, as horas acumuladas ficam significativamente aquém. A ênfase do Coach Carril no trabalho em equipe, na atenção meticulosa e na importância do momento presente alinha-se com o conceito de prática deliberada. Nesses 850 casos, os residentes são incentivados a focar no aprimoramento de técnicas e a aproveitar cada oportunidade de desenvolvimento de habilidades.
Trabalho em Equipe, Fundamentos e Prática Deliberada 🤝📚
Os princípios do Coach Carril ecoam a necessidade de trabalho em equipe e concentração nos aspectos fundamentais, ressoando com as percepções de Gladwell. O princípio nº 18 de Carril, que enfatiza a importância da tarefa presente, alinha-se com a ideia de prática deliberada—imersão total na experiência de aprendizado atual. Residentes, assim como jogadores de basquete que aprimoram suas habilidades, encontram valor na prática focada e intencional para superar a lacuna de treinamento.
Cirurgia: A Tríade Satisfatória de Autonomia, Complexidade e Conexão 🌐💼💡
Gladwell ainda postula três atributos-chave que tornam o trabalho satisfatório para os indivíduos: autonomia, complexidade e uma conexão tangível entre esforço e recompensa. A cirurgia, por sua própria natureza, encapsula esses elementos. A autonomia reina na tomada de decisões e nas habilidades procedimentais, a complexidade se manifesta nos intrincados aspectos de várias cirurgias, e a conexão entre esforço e recompensa é evidente tanto para o paciente quanto para o praticante.
A Recompensa do Cirurgião: A Sobrevivência do Paciente e a Compensação Pessoal 🏥💰
No cerne da satisfação cirúrgica está a profunda conexão entre o esforço do cirurgião e o bem-estar do paciente. Navegar com sucesso por cenários complexos pode ser uma recompensa gratificante, epitomizando a essência da cirurgia. Além disso, os esforços mais amplos de um cirurgião, medidos em operações realizadas e pacientes atendidos, correlacionam-se com a compensação pessoal e o reconhecimento profissional.
À medida que o treinamento cirúrgico evolui, a delicada interação entre prática, trabalho em equipe e as recompensas intrínsecas da cirurgia permanece um alicerce. A jornada para a maestria pode não aderir estritamente à regra das 10.000 horas, mas os princípios de prática deliberada, trabalho em equipe e a natureza gratificante do trabalho cirúrgico persistem como faróis orientadores no domínio da cirurgia. 🌟🔪
“A busca pela maestria cirúrgica é um contínuo equilíbrio entre prática intencional, colaboração e a profunda satisfação de transformar vidas.”
Cirurgia: Uma Sinfonia de Habilidade e Trabalho em Equipe
No intricado domínio da cirurgia, onde anos de treinamento rigoroso moldam as mãos e mentes dos cirurgiões gerais, uma verdade profunda emerge—cirurgia não é um empreendimento solitário. A narrativa transcende a sala de operação, destacando a sinfonia de profissionais dentro do ecossistema de saúde. Enquanto o cirurgião navega pelas complexidades do cuidado ao paciente, um esforço colaborativo se desenrola, semelhante ao funcionamento harmonioso de uma equipe.
Treinamento como um Cadinho para os Fundamentos 🎓⚙️
Enfrentando a árdua jornada da faculdade de medicina e uma exigente residência cirúrgica, o arsenal de um cirurgião é forjado. Conhecimento, destreza técnica e resistência tornam-se os pilares, fortalecendo a base sobre a qual a prática cirúrgica se sustenta. No entanto, o pilar central é o trabalho em equipe, uma realização que surge para todo praticante ao ingressar na dança intricada da prestação de cuidados de saúde.
O Maestro Cirúrgico: A Sabedoria de Pete Carril 🏀📘
Buscando inspiração de uma fonte inesperada, o treinador Pete Carril, o ilustre técnico de basquete da Universidade de Princeton, torna-se um farol de sabedoria. Além da quadra de basquete, os ensinamentos de Carril encapsulam princípios universais aplicáveis à vida e, surpreendentemente, à cirurgia. No volume sucinto, “The Smart Take from the Strong”, co-escrito com Dan White e introduzido pelo venerável Bobby Knight, Carril transmite sabedoria atemporal.
25 Pequenas Coisas: Um Paradigma para a Cirurgia e a Vida 🌐📜
As “25 pequenas coisas a lembrar” do Coach Carril ecoam com relevância não apenas no basquete, mas ressoam nos corredores da cirurgia e da vida. Explorando algumas, como “cada pequena coisa conta”, “você quer ser bom naquelas coisas que acontecem muito” e “a maneira como você pensa afeta o que você vê e faz”, os paralelos com a cirurgia tornam-se surpreendentemente aparentes. A filosofia de Carril torna-se um guia para cirurgiões, enfatizando a importância da atenção aos detalhes, prática e a profunda interação entre pensamento e ação.
Além da Quadra: Cirurgia como um Esporte de Equipe 🤝🔬
Em uma sincronia reminiscente de uma equipe de basquete, o cirurgião harmoniza-se com um coro de profissionais de saúde—enfermeiros, anestesiologistas, equipe de apoio, administradores e mais. A cadência do sucesso é ditada não apenas pela habilidade individual, mas pelo esforço coletivo da equipe. Visão, antecipação e dedicação inabalável convergem, não apenas na quadra de basquete, mas também no teatro da cirurgia.
Enquanto o Coach Carril permanece um espectador silencioso nos sagrados salões de Princeton, testemunhando uma nova geração lutando pela vitória, os cirurgiões também encontram inspiração na busca coletiva pela excelência. Trabalho em equipe, um espírito indomável e um compromisso com o crescimento pessoal e coletivo emergem como os marcos do sucesso, tanto na quadra quanto na sala de operações. 🏀🌟🔪
“A verdadeira maestria cirúrgica não reside apenas nas mãos que operam, mas na harmonia da equipe que, unida, transforma vidas.”
Os Dez Princípios Cirúrgicos
A jornada da vida é um mosaico tecido com fios de orientação de pais, irmãos e mentores. Este artigo transcende o mundano, abraçando a filosofia e o testemunho pessoal na construção de uma carreira cirúrgica triunfante. Revelamos uma lista dos dez principais mandamentos que serve como uma bússola para cirurgiões aspirantes:
Os Dez Princípios Cirúrgicos do Dr. Thirlby 📜🌐
- O Treinamento é Divertido (Você Nunca Vai Esquecê-lo): Um aceno para o aprendizado contínuo, reconhecendo a metamorfose perpétua nas carreiras cirúrgicas.
- Segurança no Emprego: Cirurgiões gerais, vitais e requisitados, encontram posições em diversos cenários, desde centros urbanos movimentados até expansões rurais serenas.
- A Remuneração é Boa: Uma compensação confortável, acima das médias da sociedade, promete estabilidade financeira.
- Sua Mãe Se Orgulhará de Você: Um orgulho familiar ressoa, estendendo-se além das mães para pais, tias e um tapete de familiares.
- Cirurgiões Têm Estilo: Abraçando a personalidade cirúrgica e a cultura única que envolve os reinos cirúrgicos.
- Você Terá Heróis; Você Será um Herói: Cirurgiões, moldados por influenciadores, retribuem tornando-se faróis de esperança para pacientes gratos.
- Existe Espiritualidade, se Você Quiser: As recuperações inexplicáveis, os momentos milagrosos que desafiam as normas estatísticas.
- Você Vai Mudar a Vida dos Pacientes: Uma profunda satisfação pessoal derivada do impacto tangível no destino dos pacientes.
- Pacientes Vão Mudar Sua Vida: Lições diárias dos pacientes promovem humildade, não julgamento e uma jornada contínua para se tornar um ser humano melhor.
- Eu Amo “Dissecar”: Uma reflexão poética da alegria derivada da arte meticulosa dos procedimentos cirúrgicos, executados com precisão para o bem maior.
Os Mandamentos da Vida Cirúrgica 🌌📜
Acrescentando profundidade à narrativa, como mandamentos atemporais, o Dr. James D. Hardy contribui com uma lista que transcende milênios, gravada na versão King James da Bíblia Sagrada.
- Conheça Seu Poder Superior: Uma homenagem ao aspecto espiritual da vida e à santidade do dia de descanso.
- Respeite Suas Raízes: Um reconhecimento da importância dos pais e dos laços familiares.
- Não Faça Mal: Um ethos antigo ressoa através da proibição de ações como assassinato, adultério, roubo, mentir e cobiçar os pertences dos outros.
- Busque a Excelência: Uma busca incessante pelo crescimento pessoal e profissional, incorporando eficiência, excelência e preservação da integridade.
- Prepare-se para a Liderança: Um chamado para formar líderes, enfatizando a importância do crescimento educacional e profissional.
- Cultive Relacionamentos Profissionais: Reconhecendo o valor dos mentores, preservando a sabedoria transmitida através das gerações.
- Lembre-se de Suas Origens: Um eco dos dez mandamentos pessoais do Dr. Hardy, incentivando os indivíduos a honrar sua origem e representá-la com orgulho.
- Valorize a Família: Um lembrete gentil para passar tempo de qualidade com a família, reconhecendo o impacto profundo do amor nos filhos.
- Passe Tempo Sozinho: Defendendo momentos de solidão, promovendo o pensamento criativo e a reflexão pessoal.
- Encontre Alegria em Seu Trabalho: Uma verdade profunda encapsulada na sustentação derivada da busca diária por um trabalho significativo que se gosta genuinamente.
Nesta amalgamação dos dez principais mandamentos do Dr. Thirlby e dos mandamentos do Dr. Hardy, um roteiro se desenrola — um guia não apenas para uma carreira cirúrgica, mas para uma vida plena e com propósito. 🌈🔍🔬
“A verdadeira liderança em cirurgia é esculpida não apenas pelas mãos que operam, mas pelo coração que guia e inspira.”
Liderança no Campo da Cirurgia
O campo da cirurgia está em constante evolução, exigindo não apenas habilidades técnicas de alta qualidade, mas também capacidades de liderança excepcionais. No entanto, a formação tradicional dos cirurgiões raramente inclui treinamento formal em liderança, deixando muitos profissionais despreparados para assumir posições de liderança. Este artigo explora a importância da liderança na cirurgia, os diferentes tipos de liderança, suas características e oferece recomendações para o desenvolvimento de líderes cirúrgicos.
A Importância da Liderança na Cirurgia
Historicamente, os cirurgiões eram vistos como líderes incontestáveis dentro de um modelo de treinamento de aprendizado, onde a experiência pessoal e o julgamento clínico guiavam as práticas. No entanto, a modernização da medicina, impulsionada pela tecnologia e pela disponibilidade de dados, transformou o ambiente cirúrgico em um campo mais colaborativo e complexo. A liderança eficaz agora é crucial para navegar esse ambiente volátil, incerto, complexo e ambíguo. Como disse Napoleão Bonaparte, “Um líder é um negociador de esperanças.” Na cirurgia, liderar é guiar equipes em meio a incertezas, mantendo sempre a esperança e a confiança nos melhores resultados para os pacientes.
Desenvolvimento da Liderança Cirúrgica
Apesar da importância, muitos cirurgiões recém-formados não recebem treinamento formal em liderança durante a residência. Ao contrário de outras profissões, onde a liderança é um componente central da formação, os médicos devem aprender habilidades de liderança na prática ou através da observação de líderes bem-sucedidos. Programas de desenvolvimento de liderança, semelhantes aos oferecidos a oficiais militares e executivos de negócios, poderiam beneficiar grandemente os cirurgiões. George S. Patton afirmou: “Não diga às pessoas como fazer as coisas, diga-lhes o que fazer e deixe que elas surpreendam você com seus resultados.” Essa filosofia pode ser aplicada na cirurgia, incentivando a autonomia e a inovação dentro das equipes cirúrgicas.
Tipos de Liderança em Cirurgia
Diversos estilos de liderança podem ser aplicados no campo da cirurgia, cada um com suas características únicas:
- Liderança Autoritária:
- Caracterizada por decisões centralizadas e controle rígido.
- Pode ser eficaz em situações de emergência onde decisões rápidas são necessárias.
“O verdadeiro gênio reside na capacidade de avaliar informações incertas, conflitantes, e perigosas.” Winston Churchill
- Liderança Hierárquica:
- Baseada em uma estrutura de comando clara.
- Útil em ambientes estruturados com protocolos bem definidos.
Sun Tzu, em “A Arte da Guerra”, escreveu: “Aquele que é prudente e espera por um inimigo imprudente será vitorioso.”
2. Liderança Transacional:
- Focada em recompensas e punições para alcançar resultados.
- Pode ser útil para manter a eficiência e a produtividade.
Douglas MacArthur disse: “Os soldados devem ter ganho pessoal de suas ações; isso estimula o cumprimento do dever.”
3. Liderança Transformacional:
- Inspira e motiva a equipe a alcançar metas além das expectativas.
- Promove inovação e mudanças positivas na prática cirúrgica.
“O maior líder não é necessariamente aquele que faz as maiores coisas. Ele é aquele que faz as pessoas fazerem as maiores coisas.” – Ronald Reagan
4. Liderança Adaptativa:
- Envolve a capacidade de ajustar-se a novas situações e desafios.
- Crucial em ambientes cirúrgicos dinâmicos e em constante mudança.
Dwight D. Eisenhower afirmou: “Os planos são inúteis, mas o planejamento é tudo.”
5. Liderança Situacional:
- Adapta o estilo de liderança com base nas necessidades específicas da equipe e da situação.
- Proporciona flexibilidade e resposta eficaz a diferentes cenários clínicos.
Como observou Alexander, o Grande: “Não há nada impossível para aquele que tentará.”
6. Liderança Servidora:
- Foca no bem-estar e no desenvolvimento dos membros da equipe.
- Constrói uma cultura de apoio e colaboração.
“O melhor dos líderes é aquele cujo trabalho é feito, cujas pessoas dizem: ‘Nós fizemos isso sozinhos.'” – Lao-Tzu
Características de um Líder Cirúrgico Eficaz
Um líder cirúrgico eficaz deve possuir várias qualidades essenciais, incluindo visão, flexibilidade, motivação, inteligência emocional (EI), empatia, adaptabilidade, confiança, confiabilidade, responsabilidade e habilidades de gestão. A visão permite ao líder definir e perseguir objetivos claros, enquanto a flexibilidade e a adaptabilidade são necessárias para navegar em um ambiente em rápida mudança. Napoleão Bonaparte afirmou: “A liderança é uma combinação de estratégia e caráter. Se você precisar dispensar um, dispense a estratégia.” Essa citação reflete a importância do caráter e da integridade na liderança cirúrgica. A inteligência emocional e a empatia são fundamentais para a comunicação eficaz e para a construção de relacionamentos sólidos dentro da equipe. A confiabilidade e a responsabilidade asseguram que o líder seja um exemplo a ser seguido, promovendo uma cultura de confiança e responsabilidade mútua.
Recomendações para o Desenvolvimento de Líderes Cirúrgicos
Para desenvolver habilidades de liderança, os cirurgiões devem buscar oportunidades de treinamento formal em liderança, participar de workshops e seminários, e buscar orientação de mentores experientes. A autoavaliação honesta e o feedback contínuo são essenciais para o crescimento pessoal e profissional. Além disso, a incorporação de programas de liderança nos currículos de residência cirúrgica pode preparar melhor os futuros cirurgiões para os desafios do campo. Estabelecer um ambiente que encoraje a liderança colaborativa e o desenvolvimento contínuo também é crucial para a formação de líderes eficazes.
Conclusão
A liderança no campo da cirurgia é essencial para enfrentar os desafios de um ambiente médico moderno e complexo. Desenvolver habilidades de liderança em cirurgiões pode melhorar significativamente os resultados dos pacientes e promover uma prática cirúrgica mais eficiente e colaborativa. Ao reconhecer a importância da liderança e investir em seu desenvolvimento, a comunidade cirúrgica pode assegurar um futuro mais brilhante e inovador para a medicina.
Fricção Cirúrgica: Desafios e Realidades no Centro Cirúrgico
Fricção Cirúrgica: Desafios e Realidades no Centro Cirúrgico
No universo da teoria militar, Carl von Clausewitz introduziu o conceito de “fricção” para descrever as dificuldades e imprevistos que complicam a execução dos planos de guerra. Esse conceito, no entanto, transcende o campo de batalha e encontra paralelos surpreendentes em outros cenários complexos e de alta pressão, como o centro cirúrgico. A “fricção cirúrgica” refere-se às diversas dificuldades que cirurgiões e equipes médicas enfrentam durante procedimentos, afetando a eficiência e os resultados esperados.
Imprevisibilidade e Complexidade
Assim como na guerra, a cirurgia está repleta de elementos imprevisíveis. Mesmo com um planejamento meticuloso e uma equipe altamente treinada, fatores inesperados podem surgir. Complicações anatômicas, reações adversas a medicamentos e condições pré-existentes do paciente são apenas alguns exemplos de imprevistos que podem alterar drasticamente o curso de uma operação.
“Tudo na guerra é simples, mas a coisa mais simples é difícil.” – Carl von Clausewitz
Equipamentos e Tecnologia
Embora a tecnologia moderna tenha revolucionado a medicina, ela também introduz sua própria forma de fricção. Equipamentos sofisticados podem falhar ou não funcionar conforme esperado. A calibração inadequada de máquinas, falhas de software em dispositivos médicos e até problemas de energia podem criar obstáculos significativos durante uma cirurgia. Manter e operar esses equipamentos requer um nível elevado de expertise técnica e atenção constante.
“A fricção é o único conceito que distingue amplamente a guerra real da guerra no papel.” – Carl von Clausewitz
Comunicação e Coordenação
A comunicação é crucial em um centro cirúrgico, onde cada membro da equipe desempenha um papel vital. Qualquer falha na transmissão de informações pode ter consequências sérias. Mal-entendidos entre cirurgiões, anestesistas, enfermeiros e técnicos podem levar a erros críticos. A coordenação eficaz é essencial para garantir que todos os procedimentos sejam executados sem problemas, desde a preparação do paciente até a conclusão da cirurgia.
“A mais triviais coisas, vistas no contexto de uma operação militar, parecem ir contra você.” – Carl von Clausewitz
Fatores Humanos
A fricção também emerge das variáveis humanas. Fadiga, estresse e pressão emocional podem afetar o desempenho dos profissionais de saúde. Cirurgiões e enfermeiros frequentemente trabalham em turnos longos e intensos, o que pode levar a lapsos de concentração e julgamento. A capacidade de um profissional de saúde de manter a calma e tomar decisões rápidas e precisas é testada continuamente no ambiente cirúrgico.
“A guerra é o domínio da incerteza; três quartos dos fatores sobre os quais a ação é baseada estão enfiados na névoa de maior ou menor incerteza.” – Carl von Clausewitz
Logística e Suprimentos
A logística desempenha um papel crítico no funcionamento suave de um centro cirúrgico. A disponibilidade de instrumentos estéreis, medicamentos e outros suprimentos médicos é fundamental. Qualquer atraso na entrega de suprimentos ou problemas com a esterilização de instrumentos pode interromper um procedimento e aumentar os riscos para o paciente.
“A guerra é a área da atividade humana mais suscetível à fricção.” – Carl von Clausewitz
Mitigando a Fricção Cirúrgica
Assim como os comandantes militares desenvolvem estratégias para mitigar a fricção na guerra, as equipes cirúrgicas adotam várias práticas para reduzir as dificuldades inesperadas. Treinamento rigoroso e contínuo, simulações de procedimentos complexos e protocolos claros de comunicação são essenciais. Além disso, a manutenção regular de equipamentos e a implementação de sistemas de redundância podem ajudar a minimizar falhas técnicas.
“A habilidade de um líder militar reside na manutenção de uma visão clara e objetiva apesar da fricção.” – Carl von Clausewitz
A fricção cirúrgica, como descrita por Clausewitz em um contexto militar, reflete a realidade desafiadora do centro cirúrgico. Reconhecer e preparar-se para essas dificuldades é crucial para garantir a segurança do paciente e o sucesso das operações. Em última análise, a habilidade das equipes médicas em gerenciar a fricção cirúrgica determina a eficácia e a eficiência das intervenções cirúrgicas.
Charlie Munger’s 25 Cognitive Biases Applied to Digestive Surgery
In the demanding field of digestive surgery, excellence is not just a goal but a necessity. By integrating the profound insights of Charlie Munger on cognitive biases with the motivational principles of Zig Ziglar, surgeons can achieve superior performance and enhance patient care. This comprehensive guide offers actionable recommendations and illustrative examples tailored to the unique challenges of digestive surgery, ensuring that every decision is informed, balanced, and patient-centered. Charlie Munger is a renowned investor and philosopher known for his ability to identify and avoid judgment errors, often rooted in cognitive biases. For a digestive surgeon, understanding and mitigating these biases can significantly enhance clinical decision-making and performance. This summary outlines Munger’s 25 biases and provides specific examples and recommendations for surgical practice.
The 25 Cognitive Biases
- Reward and Punishment Super-Response Tendency
- Example: Opting for procedures with higher financial incentives despite less lucrative alternatives being more appropriate for the patient.
- Recommendation: Always evaluate the long-term benefits for the patient over immediate rewards.
- Liking/Loving Tendency
- Example: Ignoring a team member’s faults because you like them, compromising care quality.
- Recommendation: Maintain objective and impartial evaluations of all team members’ performance.
- Disliking/Hating Tendency
- Example: Dismissing valuable suggestions from colleagues due to personal dislike.
- Recommendation: Prioritize the efficacy of suggestions and patient safety, regardless of who proposes them.
- Doubt-Avoidance Tendency
- Example: Sticking to familiar procedures and avoiding new techniques with better outcomes due to fear of the unknown.
- Recommendation: Stay updated with best practices and be willing to explore new, evidence-based approaches.
- Inconsistency-Avoidance Tendency
- Example: Persisting with outdated surgical techniques to remain consistent with past practices.
- Recommendation: Regularly review clinical guidelines and adapt as necessary.
- Curiosity Tendency
- Example: Spending excessive time researching rare conditions not relevant to daily practice.
- Recommendation: Focus on continuous updates in areas directly related to daily clinical work.
- Kantian Fairness Tendency
- Example: Treating all cases identically without considering individual patient needs.
- Recommendation: Personalize care to meet the unique needs of each patient.
- Envy/Jealousy Tendency
- Example: Allowing jealousy of colleagues’ success to affect the work environment.
- Recommendation: Focus on personal and collaborative professional development, celebrating others’ successes.
- Reciprocity Tendency
- Example: Rewarding personal favors with clinical decisions, like preferences for shifts or cases.
- Recommendation: Maintain professionalism and base decisions on clinical and ethical criteria.
- Simple, Pain-Avoiding Psychological Denial
- Example: Avoiding discussions about poor prognoses to evade emotional discomfort.
- Recommendation: Address all clinical situations honestly and sensitively, providing appropriate support.
- Excessive Self-Regard Tendency
- Example: Overestimating personal skills and refusing assistance or second opinions.
- Recommendation: Recognize personal limitations and seek collaboration when necessary.
- Over-Optimism Tendency
- Example: Underestimating surgical risks and failing to prepare patients for potential complications.
- Recommendation: Conduct comprehensive risk assessments and communicate realistically with patients.
- Deprival-Superreaction Tendency
- Example: Overreacting to resource shortages impulsively.
- Recommendation: Plan ahead and stay calm to find effective solutions.
- Social-Proof Tendency
- Example: Adopting practices simply because they are popular among peers without assessing their efficacy.
- Recommendation: Base clinical decisions on robust evidence and recognized medical guidelines.
- Contrast-Misreaction Tendency
- Example: Underestimating a postoperative complication because it seems minor compared to a recent severe case.
- Recommendation: Evaluate each case individually and objectively, avoiding subjective comparisons.
- Stress-Influence Tendency
- Example: Making hasty decisions under high-pressure situations.
- Recommendation: Develop stress management techniques and make decisions calmly and deliberately.
- Availability-Misweighing Tendency
- Example: Making decisions based primarily on recent experiences instead of comprehensive historical data.
- Recommendation: Maintain detailed records and review long-term data to inform decisions.
- Use-It-or-Lose-It Tendency
- Example: Assuming surgical skills remain unchanged without regular practice.
- Recommendation: Regularly participate in training and simulations to keep skills up-to-date.
- Drug-Misinfluence Tendency
- Example: Underestimating the effects of postoperative analgesics.
- Recommendation: Carefully monitor medication use and adjust as needed.
- Senescence-Misinfluence Tendency
- Example: Resisting learning new surgical techniques due to age.
- Recommendation: Engage in continuous medical education and remain open to innovation.
- Authority-Misinfluence Tendency
- Example: Blindly following a senior colleague’s outdated practices.
- Recommendation: Question and validate all practices against current evidence and standards.
- Twaddle Tendency
- Example: Engaging in irrelevant discussions during surgical planning.
- Recommendation: Focus on relevant, evidence-based information.
- Reason-Respecting Tendency
- Example: Failing to explain the rationale behind surgical decisions to patients.
- Recommendation: Always provide clear, logical explanations to patients and their families.
- Lollapalooza Tendency
- Example: Multiple biases leading to a major error in patient care.
- Recommendation: Be vigilant about recognizing and mitigating multiple biases simultaneously.
- Tendency to Overweight Recent Information
- Example: Giving undue importance to the most recent piece of information received.
- Recommendation: Balance recent information with a thorough review of all relevant data.
Just as Charlie Munger highlights the importance of avoiding cognitive biases for effective decision-making, Zig Ziglar teaches us the significance of attitude and continuous improvement. For a digestive surgeon, applying these principles can transform clinical practice, leading to exceptional performance and superior patient care. Zig Ziglar said, “You don’t have to be great to start, but you have to start to be great.” Every step taken towards overcoming cognitive biases and adopting evidence-based practices is a step towards excellence. By recognizing and mitigating these 25 cognitive biases, you position yourself for an assistive performance that not only treats but truly cares for patients.
Recommendations from Zig Ziglar for Digestive Surgeons
- Believe in Yourself: “If you can dream it, you can achieve it.” Trust in your ability to learn and grow continually.
- Set Clear Goals: “A goal properly set is halfway reached.” Define clear objectives to enhance your skills and knowledge.
- Maintain a Positive Attitude: “Your attitude, not your aptitude, will determine your altitude.” Face challenges with a positive and resilient mindset.
- Learn from Every Experience: “Failure is an event, not a person.” Use every situation, good or bad, as a learning opportunity.
- Serve Others with Excellence: “You can have everything in life you want if you will just help enough other people get what they want.” Focus on patient well-being in all decisions.
By integrating Munger’s lessons and Ziglar’s motivational wisdom, you will not only become a better surgeon but also an inspiring leader and a true advocate for excellence in medicine. Remember always: “Success is doing the best we can with what we have.” Keep evolving, seeking knowledge, and above all, serving your patients with dedication and compassion. Together, let’s transform the practice of digestive surgery, one step at a time, towards the excellence our patients deserve.
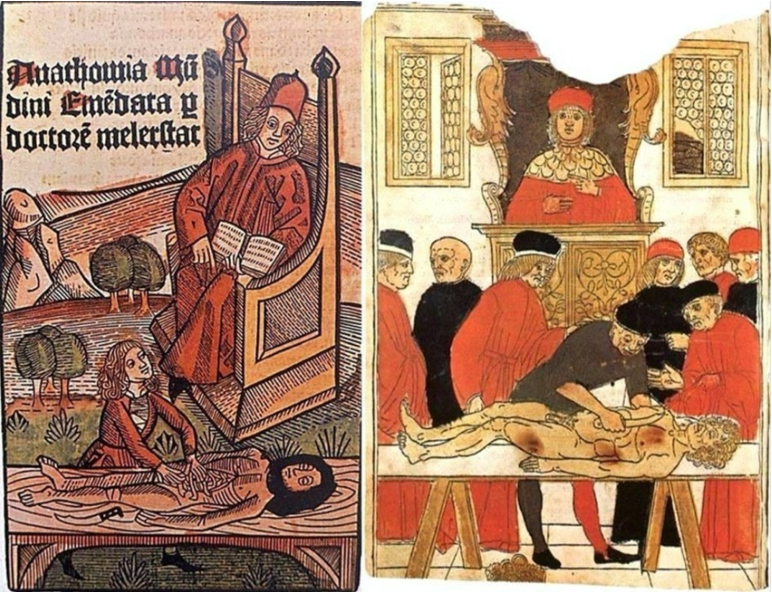
Mondino de Luzzi (1270-1326) e o surgimento do MONITOR DE ANATOMIA
Mondino, oriundo de Bolonha, nasceu e concluiu seus estudos em sua cidade natal, obtendo sua graduação por volta do ano de 1290. A partir de 1306, tornou-se membro do corpo docente da universidade local. Ele recebeu instrução de Tadeu, compartilhando a mesma época de estudo com Mondeville, e dedicou-se de maneira sistemática à Anatomia, realizando dissecações públicas do corpo humano. Mondino é reconhecido como o pioneiro na “restauração” da Anatomia. Em 1316, publicou o tratado intitulado “Anothomia”, considerado o primeiro trabalho “moderno” na área, distinguindo-se por sua abordagem prática e original, diferenciando-se de simples traduções de textos clássicos.
A obra de Mondino apresenta desafios, conforme apontado por Singer (1996), destacando-se a nomenclatura confusa e as condições peculiares da dissecação naquela época. A ausência de conservantes apropriados, apesar do conhecimento acumulado pelos egípcios em técnicas de embalsamamento, tornava a dissecação um processo extenuante, preferencialmente realizado no inverno e em até quatro dias específicos para cada região do corpo.
Apesar de imprecisões anatômicas, como apontado por Friedman e Friedman (2001), Mondino desempenhou um papel crucial na instituição da dissecação como componente essencial do estudo anatômico. Essa prática foi posteriormente integrada ao currículo médico da Universidade de Bolonha, permitindo, até o final do século XVI, que as execuções de criminosos fossem realizadas de maneira que não comprometesse o trabalho anatômico, representando um avanço no uso do corpo humano na construção do conhecimento.
A contribuição de Mondino foi duradoura, pois sua obra foi uma das principais fontes de conhecimento em Anatomia humana por mais de duzentos anos, até o advento da obra de Vesalius no século XVI. Ao assumir a cátedra da disciplina, Mondino introduziu uma nova dinâmica nas aulas de Anatomia, afastando-se da dissecação e inserindo o ostensor (aluno) e o demonstrator ou incisore (técnico) para conduzirem os procedimentos, enquanto os alunos observavam.
As técnicas predominantes, como dissecação a fresco, maceração e preparações secas ao sol, eram utilizadas por Mondino e seus contemporâneos. Apesar de suas reservas quanto à maceração, essa técnica continuou a ser praticada, como confirmado pelos textos de Guido de Vigevano em 1345, representando a persistência do uso da dissecação para fins educacionais em Bolonha.
Mondino não expandiu significativamente o conhecimento anatômico existente, mas contribuiu para a formação de anatomistas que perpetuaram a tradição da disciplina em Bolonha, Pádua e em outros países. Notáveis estudiosos, como Gabrielle de Gerbi e Alessandro Achillini, aprimoraram e ampliaram as descrições anatômicas de Mondino em suas próprias contribuições.
A anatomia permanece como alicerce fundamental para o desenvolvimento da medicina ao oferecer conhecimentos cruciais para o adequada exercício profissional. O legado de anatomistas como Mondino, que enfrentaram desafios significativos em suas dissecações pioneiras, ecoa nas salas de aula modernas. A persistência do estudo anatômico é essencial para a formação médica, e os monitores de anatomia desempenham um papel vital nesse processo educativo. Atuando como elo entre a teoria e a prática, esses monitores, herdeiros contemporâneos do ostensor de Mondino, desempenham um papel crucial ao auxiliar na orientação dos alunos nas complexidades da dissecação e na compreensão da anatomia humana. Sua contribuição atual é inseparável do legado histórico, garantindo que o conhecimento anatômico continue a florescer, moldando as futuras gerações de profissionais de saúde e consolidando a anatomia como um pilar indispensável no edifício da medicina.
ODE AOS MESTRES ANATÔMICOS
Ser mestre é perpetuar juventude, Afrontando o inexorável fio do tempo, Desdobrando-se, multiplicando-se, Nas almas dos discípulos, criando ensejo.
Escolas germinam quando a maturidade, Se entrelaça à força do nobre sentimento, O mestre, sábio, fala à mente e coração, Exemplo luminoso, toque profundo, alento.
Na odisseia do saber, mestre é guia, Navegando oceanos de experiência viva, Com luz, desbrava trilhas no pensamento.
O mestre, como sol em seu zênite, Aquece a jornada do aprendizado, Conservando-se jovem, eternamente, erudito.
Assim, na sala de aula, é o comandante, Que com alma e sabedoria encanta, O mestre, semeando luz e meta.
Small desires have a life as short as the journey of those who pursue them.
The will is the road: those who want, move forward; those who don’t, justify.
Those who want find the way; those who don’t, know the reasons.
Those who want make sacrifice meaningful.
Those who don’t want declare the barriers that ease guilt.
Those who don’t want turn restriction into prohibition, limit into decision.
Those who want decide for the outcome to be achieved.
Those who don’t want decide based on the difficulty encountered.
What is challenging for one is motivating for another.
What is sacrifice for one is commitment for the other.
The challenge, for both, changes – irritating or exciting, obstacle or opportunity. Those who want accept and persist.
Those who don’t want retreat and give up.
The drive of man is his GREAT desire.
Small desires have a life as short as the journey of those who pursue them.
O Estoicismo Cirúrgico
Aplicando Princípios Filosóficos na Prática Cirúrgica
O campo da cirurgia, especialmente no tratamento das doenças do aparelho digestivo, exige não apenas habilidades técnicas refinadas, mas também resiliência emocional e ética sólida. A prática cirúrgica, por sua natureza, envolve decisões difíceis, momentos de pressão extrema e desafios inesperados. Nesse contexto, os princípios do estoicismo, filosofia praticada por pensadores como Sêneca, Epicteto e o imperador Marco Aurélio, oferecem ferramentas valiosas para que o cirurgião enfrente a complexidade emocional e ética de sua profissão.
Neste artigo, direcionado a estudantes de medicina, residentes de cirurgia geral e pós-graduandos em cirurgia do aparelho digestivo, vamos explorar como os princípios estoicos podem ser aplicados à prática cirúrgica, promovendo não apenas a eficiência técnica, mas também a excelência ética. Abordaremos as virtudes estoicas que podem moldar o comportamento de um cirurgião, aprimorando sua capacidade de lidar com adversidades e tomar decisões sábias no centro cirúrgico.
1. Aceitação das Limitações: “Primum non nocere” em Ação
O princípio estoico de aceitar o que não pode ser mudado é fundamental para o cirurgião. Em um procedimento cirúrgico, o inesperado pode surgir a qualquer momento. O estoicismo ensina que devemos focar no que está sob nosso controle – nossas ações e reações – e aceitar com serenidade aquilo que foge ao nosso alcance, como complicações imprevistas ou resultados adversos. Essa atitude fortalece o cirurgião, permitindo-lhe manter a calma e a clareza mental em situações críticas.
“O que está no meu poder é como reajo ao que acontece. O resto está fora do meu controle.” – Marco Aurélio
2. A Virtude da Perseverança em Meio às Adversidades
A cirurgia, especialmente nas doenças do aparelho digestivo, frequentemente envolve longos procedimentos, altos níveis de complexidade e a necessidade de ajustes rápidos. O estoicismo valoriza a perseverança diante de dificuldades, uma virtude essencial para o cirurgião que deve persistir no cuidado dos pacientes, mesmo em cenários complicados. A capacidade de continuar com foco e determinação, mesmo em circunstâncias adversas, é o que distingue o cirurgião estoico.
“A adversidade é uma oportunidade para a virtude.” – Marco Aurélio
3. Disciplina e Autocontrole no Centro Cirúrgico
O autocontrole é uma das virtudes centrais do estoicismo, e no campo cirúrgico, é vital que o cirurgião mantenha o controle emocional durante procedimentos complexos. O estoicismo nos ensina a não sermos controlados por emoções passageiras, como medo ou frustração, mas sim a agir com racionalidade. No centro cirúrgico, isso se traduz em decisões conscientes e calculadas, que priorizam o bem-estar do paciente, mantendo a objetividade diante de situações estressantes.
“Não é o que acontece, mas como você reage que importa.” – Marco Aurélio
4. Justiça e a Importância de Tratar Todos os Pacientes com Equidade
Para o cirurgião, a justiça, outro pilar estoico, é essencial. Todo paciente, independentemente de sua condição socioeconômica, deve receber o mesmo nível de cuidado e atenção. A prática cirúrgica ética requer que o cirurgião trate cada paciente com equidade, aplicando os princípios da medicina de maneira justa, sem preconceitos ou favoritismos. O cirurgião estoico vê em cada paciente uma oportunidade de exercer a sua profissão com justiça e integridade.
“A justiça consiste em fazer o que é correto, não o que é popular.” – Marco Aurélio
5. Coragem e Resiliência na Tomada de Decisões Difíceis
A cirurgia muitas vezes exige coragem para tomar decisões difíceis, especialmente em situações de risco à vida do paciente. A filosofia estoica valoriza a coragem como uma virtude indispensável. Para o cirurgião, isso significa enfrentar com firmeza e clareza os dilemas éticos e clínicos, mesmo quando há incertezas. A coragem estoica permite que o cirurgião aja com confiança e serenidade, tomando decisões informadas e moralmente corretas, mesmo em momentos críticos.
“A coragem é a dignidade sob pressão.” – Marco Aurélio
Conclusão
A prática cirúrgica é muito mais do que um conjunto de habilidades técnicas; é uma arte que exige um equilíbrio entre conhecimento, ética e resiliência emocional. Ao adotar os princípios estoicos, o cirurgião pode enfrentar os desafios diários com serenidade, perseverança e justiça, sempre em busca do bem maior para seus pacientes. O estoicismo oferece uma base filosófica robusta para lidar com as pressões da vida cirúrgica, fortalecendo o profissional em sua jornada por excelência técnica e moral.
“A felicidade de sua vida depende da qualidade de seus pensamentos.” – Marco Aurélio
Gostou ❔ Nos deixe um comentário ✍️, compartilhe em suas redes sociais e|ou mande sua dúvida pelo 💬 Chat On-line em nossa DM do Instagram.
#cirurgiageral #filosofiaestoica #éticaemcirurgia #estoicismonaetica #resiliencia
The Surgical Coach (P7)
Importance of OR Etiquette and Professionalism
The NOTTS emphasizes the significance of operating room (OR) etiquette and the evolution of surgical culture towards a more respectful and collaborative environment. Key points include:
- Changing Dynamics in the OR: The historical reputation of surgeons as being arrogant or demeaning, engaging in hazing practices, or displaying disruptive behavior is no longer acceptable. Modern surgeons are expected to create an atmosphere of mutual respect, trust, and communication.
- Cultural Shift towards Respect and Safety: A culture of safety and respect in the OR correlates with improved patient outcomes. It also enhances team communication, fosters professionalism, and contributes to a positive educational experience for all involved.
- Introduction to OR Etiquette: The concept of “OR etiquette” is introduced as a code of conduct among professionals that governs how they act and work together. This is distinct from manners, which are specific behaviors reflecting attitudes toward others.
- Components of OR Etiquette: The chapter covers various aspects of OR etiquette, including communication skills, leadership and followership, giving and receiving feedback, and available programs for improving team communication and culture.
- Team Members in the OR:
- Private Practice Setting: An attending surgeon, possibly with one or more assistants, which may include a second attending surgeon, certified surgical assistant (CSA), or physician assistant (PA).
- Academic Setting: Assistants may include medical students, residents, or fellows. Fellows are fully trained surgeons undergoing additional subspecialty training.
- Learning Environment: Progressive autonomy is a crucial concept, allowing learners to take on more responsibilities based on their competency level.
- Preoperative Discussion: Clear communication between the surgeon and the team members before the operation is essential. This includes discussing roles, responsibilities, and educational goals for the case.
- Patient-Centered Approach: Team members are responsible for reviewing the patient’s case in detail, understanding medical history, current disease status, medications, and diagnostic studies. A shared mental model of the operative and postoperative plan is crucial.
- Intraoperative Focus: During the operation, the patient becomes the central focus. Each team member is expected to contribute to the progress of the operation and assist others in doing the same.
- Postoperative Care Discussion: After the operation, discussions should cover postoperative care aspects, such as pain management, dietary restrictions, venous thromboembolism prophylaxis, and prescription medications.
The series posts (The Surgical Coach) aims to guide professionals in developing a positive OR culture through adherence to etiquette, emphasizing teamwork, respect, and effective communication for improved patient outcomes and a better working environment.
The Surgical Coach (P6)
Promoting a Positive OR Environment: Manners and Etiquette
Maintaining a respectful and collaborative atmosphere in the operating room (OR) is crucial for effective teamwork and patient safety. The author outlines key manners and etiquette that contribute to a positive OR environment:
- Politeness: Being courteous and considerate in interactions with colleagues fosters a harmonious atmosphere.
- Respect: Treating everyone in the OR with respect, regardless of their role or position, is essential for teamwork.
- Humility: Remaining humble helps create a collaborative environment where everyone’s input is valued.
- Learning Names: Taking the time to learn and use the names of all team members enhances personal connections.
- Offering Help: Anticipating needs and offering assistance without being asked demonstrates a proactive and cooperative attitude.
- Asking for Help: Being willing to seek assistance when needed promotes a culture of mutual support.
- Expressing Gratitude: Thanking colleagues for their contributions acknowledges their efforts and encourages teamwork.
- Patient-Centered Focus: Keeping the patient at the center of all actions emphasizes the ultimate goal of providing quality care.
Avoiding Disruptive Behavior:
- Rude, disruptive, or disrespectful behavior is not tolerated.
- Avoid yelling, making sarcastic comments, or engaging in inappropriate jokes.
- Refrain from gossiping or denigrating others.
- When playing music, be considerate of others’ preferences, and turn it off during critical times like the initial time-out.
Social Media Etiquette in the OR:
- Stay professional when using social media in the OR.
- Avoid checking Facebook or Instagram during surgery.
- Exercise caution when posting online, as anything posted can be captured and spread.
- Refrain from posting identifiable patient information.
Effective Communication and Surgical Pause:
- Ongoing effective communication among the surgical team is crucial.
- Emphasizes the importance of the surgical pause or “time-out” to establish a shared mental model.
- Recommends using a structured checklist, such as the World Health Organization Surgical Safety Checklist, during the surgical pause.
- Highlights the checklist’s positive impact on reducing mortality, complications, and hospital length of stay.
- Encourages active engagement of all team members during the checklist process.
Customizing the Checklist:
- The surgical safety checklist can be modified by hospitals or services to include relevant items specific to their patient population.
- Designated leaders should review and discuss each item, ensuring that all team members are introduced and empowered to speak up if they identify potential safety concerns.
- Customization may include a debriefing section at the end of the case to address additional items relevant to the team’s specific practices.
In summary, promoting positive manners and etiquette, avoiding disruptive behavior, and utilizing effective communication tools contribute to a culture of safety and collaboration in the OR. The surgical safety checklist serves as a valuable tool when implemented with commitment and engagement from all team members.
The Surgical Coach (P5)
The Surgery Success Pyramid: Insights from Coach Wooden
Drawing inspiration from the legendary basketball coach John Wooden and his “pyramid of success,” the author has adapted the concept to create the “surgery success pyramid.” This modified pyramid is tailored to the field of surgery, emphasizing key elements for professional and personal success.
Foundational (1st Tier) Elements:
- Industriousness: Hard work and diligence remain foundational to success in surgery.
- Friendship: Emphasizes the importance of teamwork, collaboration, and camaraderie within the surgical profession.
- Loyalty: Stresses the significance of loyalty to colleagues, patients, and the profession.
- Cooperation: Highlights the need for effective collaboration and cooperation among members of the surgical team.
- Enthusiasm: Encourages a positive and passionate approach to the practice of surgery.
2nd Tier Elements:
- Self-Control: The ability to maintain composure and discipline in challenging situations.
- Alertness: Staying vigilant and aware of the evolving surgical environment.
- Initiative: Taking proactive steps to address challenges and improve surgical practices.
- Intentness: Maintaining a focused and determined mindset toward achieving surgical goals.
While the foundational and second-tier elements retain Wooden’s original principles, modifications have been made to better reflect the nuances of the surgical profession.
Take-Home Points for Success in Surgery:
The author concludes with practical advice for success at different stages of a surgical career:
- Medical Student Success:
- Study or practice for an average of 4 hours per day.
- Write at least one paper for the literature per year.
- Engage in lab work and aim for a minimum of three papers per year.
- Read medical journals regularly.
- Strive for academic excellence, including achieving membership in one surgical association.
- Keep a journal or log of patient encounters and lessons learned.
- Prioritize physical fitness.
- Resident Success:
- Dedicate at least 2 hours a day to deliberate practice and study.
- Write one paper per clinical year and a minimum of three papers per year during lab experience.
- Be a positive deviant by identifying and improving inefficient processes.
- Keep a journal or log of valuable clinical insights.
- Maintain physical fitness and well-being.
- Fulfill all residency requirements promptly.
- Junior Faculty Success :
- Focus on mastering surgical practice.
- Seek mentorship and engage in a mentor-mentee relationship.
- Embrace new challenges in education, research, and administration.
- Plan for a full career by considering long-term well-being and financial planning.
- Prioritize life outside the hospital, spending time with family and friends.
- Contribute to the literature and engage in teaching.
- Value colleagues and foster a sense of community within the surgical field.
The author underscores the fulfillment derived from a life dedicated to surgery, emphasizing the value of hard work, continuous learning, and contributions to the field.
The Surgical Coach (P4)
Atul Gawande’s Insights: Navigating Medicine’s Core Requirements
Atul Gawande, a celebrated author known for his insightful perspectives on healthcare, especially in the surgical realm, has provided valuable insights that resonate with medical professionals. In his book “Better: A Surgeon’s Notes on Performance,” Gawande articulates three fundamental requirements for success in medicine:
- Diligence:
- Emphasizes the importance of meticulous attention to detail to prevent errors and overcome challenges.
- Do Right:
- Acknowledges that medicine is inherently a human profession, highlighting the ethical imperative to prioritize patient well-being.
- Ingenuity:
- Encourages a mindset of innovation, urging practitioners to think differently, embrace change, and learn from failures.
Gawande goes beyond defining these core requirements and offers five compelling suggestions on how individuals can make a positive impact within their professional culture:
- Ask an Unscripted Question:
- Advocates for spontaneous inquiries that can lead to unexpected discoveries and foster a culture of open communication.
- Don’t Complain:
- Advises against unproductive complaining, emphasizing that it neither solves problems nor contributes constructively to discussions. Encourages individuals to be prepared with alternative topics for discussion.
- Count Something:
- Promotes the practice of quantifying aspects of one’s work. Gawande suggests that counting something of personal interest leads to valuable insights and continuous learning.
- Write Something:
- Recognizes the transformative power of writing or typing. Encourages professionals to document experiences, insights, and reflections, enhancing both personal and collective learning.
- Change—Be an Early Adopter:
- Acknowledges the necessity of embracing change, especially in the rapidly advancing landscape of surgical technology. Urges individuals to be early adopters, staying abreast of innovations to enhance patient care.
Gawande’s guidance extends beyond the technical aspects of medicine, delving into the realms of communication, mindset, and professional development. These principles provide a roadmap for medical professionals to not only excel in their individual capacities but also positively influence the broader culture within which they operate.
The Surgical Coach (P3)
Legacy of Dr. William Stewart Halsted: Pioneer of Modern Surgery
In the annals of American surgery, the towering figure of Dr. William Stewart Halsted looms large, leaving an indelible mark on the field. Born in 1852 and educated at Andover and Yale, Halsted earned his medical degree from the College of Physicians and Surgeons in New York City in 1878. His illustrious career unfolded against the backdrop of transformative contributions to surgery, earning him the title of the “father of modern surgery.”
Innovations and Contributions 🌟💡
Halsted’s impact reverberated across various realms of surgery. He played a pivotal role in introducing cocaine’s use as a topical anesthetic, revolutionizing the management of pain during surgical procedures. His contributions to the “radical cure” of inguinal hernia, deployment of Listerian principles to reduce wound infections significantly, and groundbreaking surgeries for conditions like gallbladder disease, thyroid disease, periampullary cancer, aneurysm, and breast cancer underscore his multifaceted brilliance.
Halsted Residency Program 🏥👨⚕️
Central to his legacy is the renowned Halsted residency program, which yielded 17 chief residents within 33 years. Dr. Gerald Imber’s biography, “Genius on the Edge: The Bizarre Double Life of Dr. William Stewart Halsted,” encapsulates the complexity of Halsted’s character—rigid yet nurturing, compulsive yet negligent, and always devoted to advancing surgical science.
Halsted’s Reflections and Critique 📜🤔
In a reflective address at Yale in 1904, Halsted acknowledged the transformative strides made in surgery, with pain, hemorrhage, and infection no longer posing insurmountable challenges. However, he voiced concerns about the state of medical education in the United States, advocating for a system that produces surgeons of the highest caliber. His critique emphasized the need for reforms unburdened by tradition, offering ample opportunities for comprehensive training.
Legacy Through Teaching and Training 👩⚕️📚
Following Halsted’s passing in 1922, Dr. Rudolph Matas extolled his greatness as a clinician, scientist, and founder of a surgical school that stood unparalleled in scholarship and achievement. Matas highlighted Halsted’s unique ability to select and nurture a cadre of surgeons who would carry forth his teachings and principles.
The Goal of Training the Next Generation 🌱👩⚕️
Matas, in emphasizing Halsted’s enduring impact, touched upon a lofty aspiration—to train the next generation of surgeons for excellence. Indeed, an active surgeon’s noble pursuit involves imparting knowledge, skills, and a commitment to advancing surgical science to successors.
There Are No Time-Outs: Surgeon’s Lifelong Commitment ⏰💪
The training of a surgeon spans a lengthy, intricate, and challenging path, yet it is undeniably rewarding. Dr. Thirlby’s sentiments, expressed in his Top Ten list, echo the pride associated with surgical accomplishments. The narrative takes a turn toward addressing the often-unspoken topics of work-life balance and burnout. Dr. Thirlby reflects on the countless instances where a surgeon, even when “off duty,” is called upon to employ medical skills and surgical expertise, underscoring the ever-present nature of a surgeon’s commitment to patient care.
In the world of surgery, the white coat symbolizes an unwavering commitment. Driven by a sense of duty, surgeons find themselves intervening in various settings—restaurants, airplanes, theaters, sports fields—always ready to respond. The poignant illustration, “Once you put on the white coat, there are no substitutions, there are no time outs,” encapsulates the profound truth that defines a surgeon’s lifelong dedication to healing and serving others. 🩺👨⚕️🌐
The Surgical Coach (P2)
Mastery in Surgery: The 10,000-Hour Rule
In his acclaimed book “Outliers: The Story of Success,” Malcolm Gladwell delves into the essence of mastery, drawing attention to the 10,000-hour rule popularized by neurologist Daniel Levitin. This rule posits that a staggering 10,000 hours of dedicated practice are requisite for achieving mastery and excellence in any domain. Gladwell surveys diverse fields, from composers and basketball players to fiction writers and surgeons, finding the recurrent thread of the 10,000-hour benchmark.
The Discrepancy in Surgical Training ⏰🔍
However, in the context of surgical training, a stark contrast emerges. Graduating surgical chief residents are tasked with documenting approximately 850 cases, far from the 10,000-hour milestone. Even when considering an estimated 2 hours per case, the cumulative hours fall significantly short. Coach Carril’s emphasis on teamwork, meticulous attention, and the importance of the present moment aligns with the concept of deliberate practice. In those 850 cases, residents are encouraged to focus on refining techniques and embracing each opportunity for skill development.
Teamwork, Basics, and Deliberate Practice 🤝📚
Coach Carril’s principles echo the necessity for teamwork and concentration on fundamental aspects, resonating with Gladwell’s insights. Carril’s principle #18, emphasizing the significance of the present task, aligns with the idea of deliberate practice—immersing oneself fully in the current learning experience. Residents, akin to basketball players honing their skills, find value in focused and intentional practice to bridge the training gap.
Surgery: The Satisfying Triad of Autonomy, Complexity, and Connection 🌐💼💡
Gladwell further posits three key attributes that render work satisfying for individuals: autonomy, complexity, and a tangible connection between effort and reward. Surgery, by its very nature, encapsulates these elements. Autonomy reigns in decision-making and procedural skills, complexity manifests in the intricate facets of various surgeries, and the connection between effort and reward is evident at both the patient and practitioner levels.
The Surgeon’s Reward: A Patient’s Survival and Personal Compensation 🏥💰
At the heart of surgical satisfaction lies the profound connection between the surgeon’s effort and the patient’s well-being. Successfully navigating complex scenarios can be a gratifying reward, epitomizing the essence of surgery. Moreover, the broader efforts of a surgeon, measured in operations performed and patients attended to, correlate with personal compensation and professional recognition.
As surgical training evolves, the delicate interplay between practice, teamwork, and the intrinsic rewards of surgery remains a cornerstone. The journey to mastery may not strictly adhere to the 10,000-hour rule, but the principles of deliberate practice, teamwork, and the fulfilling nature of surgical work persist as guiding beacons in the realm of surgery. 🌟🔪
The Surgical Coach (P1)
Surgery: A Symphony of Skill and Teamwork
In the intricate realm of surgery, where years of rigorous training shape the hands and minds of general surgeons, a profound truth emerges—surgery is not a solitary endeavor. The narrative transcends beyond the operating room, highlighting the symphony of professionals within the healthcare ecosystem. As the surgeon navigates the complexities of patient care, a collaborative effort ensues, akin to the harmonious workings of a team.
Training as a Crucible for Fundamentals 🎓⚙️
Enduring the arduous journey of medical school and a demanding surgical residency, a surgeon’s arsenal is forged. Knowledge, technical prowess, and stamina become the pillars, fortifying the foundation upon which surgical practice rests. Yet, the linchpin is teamwork, a realization that dawns upon every practitioner as they step into the intricate dance of healthcare delivery.
The Surgical Maestro: Pete Carril’s Wisdom 🏀📘
Drawing inspiration from an unexpected quarter, Coach Pete Carril, the luminary basketball coach at Princeton University, becomes a beacon of wisdom. Beyond the basketball court, Carril’s teachings encapsulate universal principles applicable to life and, surprisingly, surgery. In the succinct volume, “The Smart Take from the Strong,” co-authored with Dan White and introduced by the venerable Bobby Knight, Carril imparts timeless wisdom.
25 Little Things: A Paragon for Surgery and Life 🌐📜
Coach Carril’s “25 little things to remember” echo with relevance not just in the realm of basketball but resonate in the corridors of surgery and life. Delving into a few, such as “every little thing counts,” “you want to be good at those things that happen a lot,” and “the way you think affects what you see and do,” the parallels with surgery become strikingly apparent. Carril’s philosophy becomes a guide for surgeons, emphasizing the importance of attention to detail, practice, and the profound interplay between thought and action.
Beyond the Hardwood: Surgery as a Team Sport 🤝🔬
In a synchrony reminiscent of a basketball team, the surgeon harmonizes with a chorus of healthcare professionals—nurses, anesthesiologists, support staff, administrators, and more. The cadence of success is dictated not just by individual skill but by the collective effort of the team. Vision, anticipation, and unwavering dedication converge, not only on the basketball court but also in the theater of surgery.
As Coach Carril remains a silent spectator in the hallowed halls of Princeton, witnessing a new generation striving for victory, surgeons too find inspiration in the collective pursuit of excellence. Teamwork, an indomitable spirit, and a commitment to personal and collective growth emerge as the hallmarks of success, both on the hardwood and in the operating room. 🏀🌟🔪
The Surgical Coach
Surgical Wisdom Unveiled: A Top Ten List and Commandments
Reflections on a Surgical Journey 🌟
Life’s journey is a mosaic woven with threads of guidance from parents, siblings, and mentors. This chapter transcends the mundane, embracing philosophy and personal testimony on sculpting a triumphant surgical career. Dr. Richard C. Thirlby, in the spirit of David Letterman, unfurls a top ten list that serves as a compass for aspiring surgeons.
Dr. Thirlby’s Top Ten Surgical Tenets 📜🌐
- Training is Fun (You’ll Never Forget It): A nod to lifelong learning, acknowledging the perpetual metamorphosis in surgical careers.
- Job Security: General surgeons, vital and in demand, find positions across diverse landscapes, from bustling urban centers to the serene rural expanses.
- The Pay is Not Bad: Comfortable compensation, soaring above societal averages, promises financial stability.
- Your Mother Will Be Proud of You: A familial pride resonates, extending beyond mothers to fathers, aunts, and a tapestry of family members.
- Surgeons Have Panache: Embracing the surgical personality and the unique culture that envelopes surgical realms.
- You Will Have Heroes; You Will Be a Hero: Surgeons, sculpted by influencers, reciprocate by becoming beacons of hope for grateful patients.
- There is Spirituality if You Want It: The inexplicable recoveries, the miraculous moments that defy statistical norms.
- You Will Change Patients’ Lives: A profound personal satisfaction derived from the tangible impact on patients’ destinies.
- Patients Will Change Your Life: Daily lessons from patients foster humility, nonjudgmentalism, and a continuous journey towards becoming a better human being.
- I Love to Cut: A poetic reflection of the joy derived from the meticulous artistry of surgical procedures, executed with precision for the greater good.
The Commandments of Surgical Living 🌌📜
Adding depth to the narrative, akin to timeless commandments, Dr. James D. Hardy contributes a list transcending millennia, etched in the New King James Version of the Holy Bible.
- Know Your Higher Power: An homage to the spiritual facet of life and the sanctity of the Sabbath day.
- Respect Your Roots: An acknowledgment of the significance of parents and the importance of familial bonds.
- Do No Harm: An ancient ethos resonates through the prohibition of actions such as murder, adultery, theft, lying, and coveting others’ belongings.
- Strive for Excellence: An unending pursuit of personal and professional growth, embodying efficiency, excellence, and the preservation of integrity.
- Prepare for Leadership: A call to groom leaders, emphasizing the importance of educational and professional growth.
- Nourish Professional Relationships: Recognizing the value of mentors, preserving the wisdom passed down through generations.
- Remember Your Roots: An echo from Dr. Hardy’s personal ten commandments, urging individuals to honor their origin and represent it with pride.
- Cherish Family: A gentle reminder to spend quality time with family, recognizing the profound impact of love on children.
- Spend Time Alone: Advocating for moments of solitude, fostering creative thinking and personal reflection.
- Find Joy in Your Work: A profound truth encapsulated in the sustenance derived from the daily pursuit of meaningful work one genuinely enjoys.
In this amalgamation of Dr. Thirlby’s top ten and Dr. Hardy’s commandments, a roadmap unfolds — a guide not just for a surgical career but for a fulfilling and purpose-driven life. 🌈🔍🔬
The Geriatric Patient
Navigating Surgical Challenges in an Aging Population: A Delicate Balance 🌐
The ongoing aging process within the American population brings forth a set of unique challenges that surgeons must adeptly navigate for decades to come. Elderly individuals, compared to their younger counterparts, often exhibit diminished physiological reserves. Their health is frequently influenced by medications that can alter normal physiological responses, such as β-blockers, or impact surgical outcomes, like warfarin or platelet aggregation–inhibiting agents. Additionally, baseline impairments, ranging from sensory issues to difficulties in ambulation or dementia, may complicate their ability to engage in everyday activities.
One perplexing dilemma faced by surgeons when caring for elderly patients revolves around the decision to pursue an aggressive intervention plan. Transparent communication between the patient and physician is paramount in determining the appropriate level of aggressiveness in the patient’s best interest. This conversation takes on heightened significance in the elderly population. Engaging in repeated discussions with patients and their families, starting before surgery and extending into the postoperative phase, is crucial. Generally, patients express a desire for aggressive medical care as long as there remains a reasonable chance for meaningful survival.
While these discussions may be uncomfortable, they are as integral to the patient’s care as any aspect of their medical history. It is imperative to recognize that surgical care is provided by individuals who genuinely care about the patient’s overall well-being. In certain situations, medical care may prioritize alleviating pain over prolonging life. Ideally, these conversations should occur in a serene and comfortable setting, free from distractions.
Moreover, it is essential to underscore that discussions about end-of-life matters are not legal proceedings. No forms need to be signed. These discussions are akin to any other conversation between a doctor and a patient regarding their care. The dialogue involves a careful consideration of the strengths and weaknesses of different approaches until a collaborative plan of action is determined. The only distinction lies in the profound nature of end-of-life discussions, offering patients the best opportunity to shape their destinies. Consequently, these discussions should be approached with the utmost reverence, acknowledging the gravity of the subject matter. 🤝💙
Estabelecendo Conexões Essenciais 💬
Técnicas de Entrevista na Medicina: Estabelecendo Conexões Essenciais 💬
A relação médico-paciente é uma parte vital do cuidado cirúrgico. O vínculo entre o cirurgião e o paciente deve ser construído, mantido e valorizado. Boas técnicas de entrevista são fundamentais para estabelecer essa relação. O alicerce para uma boa entrevista advém de uma preocupação genuína com as pessoas. Embora existam habilidades de entrevista que podem ser aprendidas, a qualidade da interação pode ser aprimorada. Estudantes de medicina devem reconhecer seu papel especial no cuidado do paciente, não se envergonhando de sua posição e compreendendo que são membros eficazes da equipe. Pacientes frequentemente veem os estudantes de medicina como acessíveis, compartilhando detalhes que poderiam ocultar de membros mais seniores da equipe. O papel do estudante é descobrir as queixas médicas principais do paciente, realizar uma história e exame físico focalizados e apresentar os achados à equipe. Uma entrevista eficaz requer a comunicação sobre quem você é e como se encaixa na equipe. 🏥
Desafios da Entrevista na Medicina: Adaptando-se a Diferentes Ambientes 🌐
Entrevistar bem pode ser desafiador devido à variedade de ambientes, como sala de cirurgia, unidade de terapia intensiva, consultório particular, leito hospitalar, sala de emergência e ambulatório. Cada ambiente apresenta desafios únicos à comunicação eficaz. Para construir boas relações médico-paciente, cirurgiões ajustam seus estilos a cada ambiente e à personalidade e necessidades de cada paciente. Algumas regras básicas são comuns a todas as entrevistas profissionais. A primeira regra é deixar claro ao paciente que, durante a história e o exame, nada além de uma emergência de vida ou morte terá maior importância do que a interação entre o cirurgião e o paciente naquele momento. Este é o primeiro e melhor momento para conectar-se com o paciente. É crucial que o paciente compreenda que um cirurgião cuidadoso, conhecedor e dedicado será seu parceiro na jornada pelo tratamento de doenças cirúrgicas. O cirurgião deve observar outras regras, incluindo dar atenção adequada à aparência pessoal para transmitir uma imagem profissional que inspire confiança, estabelecer contato visual, comunicar interesse, calor e compreensão, ouvir de forma não julgadora, aceitar o paciente como pessoa, ouvir a descrição do problema do paciente e ajudar o paciente a se sentir confortável na comunicação. 👩⚕️👨⚕️
Primeiros Minutos: Estabelecendo uma Base Sólida 🤝
Ao receber o paciente em um ambiente ambulatorial, os primeiros minutos são dedicados a cumprimentar o paciente pelo nome formal, apertar as mãos, se apresentar e explicar o papel do cirurgião. A atenção à privacidade do paciente, ajustando o estilo de conversação e o vocabulário às necessidades do paciente, descobrindo a atitude do paciente em relação à clínica, conhecendo a ocupação do paciente e entendendo o que o paciente sabe sobre sua condição são passos fundamentais. A seguir, ocorre a exploração do problema, movendo-se de perguntas abertas para perguntas fechadas. Técnicas importantes incluem o uso de transições, fazer perguntas específicas e claras e reformular o problema para verificação. É crucial determinar se o paciente tem alguma pergunta. No final da entrevista, o cirurgião explica quais serão os próximos passos e que realizará um exame no paciente. Por fim, verifica-se se o paciente está confortável. 🌟
Diferenças nos Ambientes de Atendimento: Adaptação e Compreensão 🏨
As técnicas utilizadas em ambientes ambulatoriais são igualmente adequadas para encontros em ambientes hospitalares e de pronto-socorro. Geralmente, mais tempo é dedicado ao paciente nas entrevistas iniciais e subsequentes do que em um ambiente ambulatorial. Na entrevista inicial, os pacientes podem estar com dor, preocupados com problemas financeiros e ansiosos com a falta de privacidade ou dietas desagradáveis. Eles também podem ter dificuldade para dormir, sentir medo do tratamento ou se sentir impotentes. É importante comunicar gentil e confiantemente o propósito da entrevista e quanto tempo levará. O paciente não apenas escuta, mas também observa o comportamento e a vestimenta do médico. O ambiente também afeta a entrevista. Por exemplo, um ambiente apertado, barulhento e lotado pode afetar a qualidade da comunicação. Pacientes podem ter sentimentos negativos devido a insensibilidades por parte do médico ou de outras pessoas. É fundamental evitar falar com o paciente na entrada do quarto, dar ou receber informações pessoais em um ambiente lotado, falar sobre um paciente em um elevador ou em outro espaço público, ou falar com um paciente sem fechar a cortina em uma enfermaria. 🌆
Conclusão: Construindo Relações de Confiança na Medicina 🌐
Em resumo, dominar as técnicas de entrevista na medicina é essencial para construir relações sólidas entre médico e paciente. Os cirurgiões habilmente ajustam suas abordagens a diferentes ambientes e personalidades dos pacientes, aplicando regras básicas universais. Os primeiros minutos são cruciais para estabelecer uma base sólida, enquanto a exploração cuidadosa do problema requer uma transição de perguntas abertas para fechadas. Adaptações ao ambiente e compreensão das preocupações do paciente são vitais para uma comunicação eficaz. Ao incorporar essas técnicas, os médicos podem garantir que a interação médico-paciente seja centrada no paciente, transmitindo confiança e dedicação à jornada conjunta pelo tratamento. 👨⚕️🤝👩⚕️
Navigating Your Clinical Experience in Surgery
Transitioning to the Role as a Junior Member of the Surgical Health Care Team: Navigating Your Clinical Experience in Surgery
Embarking on your surgical clerkship is an immersive clinical journey that extends beyond aspiring surgeons. This experience is a valuable opportunity to refine essential clinical skills applicable to any medical specialty. As you progress in your medical career, encounters with patients requiring surgical intervention will be inevitable. The insights gained during your surgery clerkship will empower you to identify surgical diseases, understand the need for surgical consultations, and develop empathy for the emotional, physiological, and logistical aspects patients and their families may face during operations or consultations.
Approaching Your Role: A Shift in Learning Dynamics
As a seasoned learner in medical school, your entry into the health care team during your 3rd year marks a profound transition. The focus is no longer solely on memorization; it now involves understanding patients’ complaints and diseases. Balancing voluminous information, time constraints, and determining the depth of knowledge required for patient care present unique challenges. Successful clinical performance is influenced by various factors:
- Preparatory Coursework and Experience: Constructing new knowledge relies on existing foundations. Deep knowledge, especially in anatomy, facilitates a seamless connection between new information and prior understanding.
- Quality of Study Methods: Active learning demands taking responsibility for your education. Maintaining a disciplined study plan aligned with your learning style is essential.
- Organizational Skills: Successful learners adeptly manage time and priorities to avoid last-minute cramming, reducing stress.
- Motivation and Emotion: Enthusiasm and positive feelings toward content, team, and environment significantly impact the clerkship experience and how you are perceived by patients and the team.
- Physical Health: The link between physical well-being and effective learning underscores the importance of attending to personal health needs.
- Distractibility and Concentration Skills: Active engagement in learning, whether through reading or listening, is crucial for processing and translating information into meaningful knowledge.
Maximizing Your Learning: Strategies for Success
1. Prepare, Practice, and Review:
- Preparation: Activate prior knowledge by pre-reading about upcoming topics, enhancing comprehension, and fostering long-term memory.
- Practice: Actively engage in learning, take notes, and generate questions. Studies show that self-generated notes enhance retention.
- Review: Ongoing review, coupled with self-assessment using test questions, patient management problems, and creating personal tests, reinforces information.
2. Organize Your Knowledge:
- Get the Big Picture: Familiarize yourself with learning objectives, chapter headings, and subheadings before reading. Listing questions beforehand guides focused reading.
- Review Charts and Diagrams: Key information in charts and diagrams aids study. Testing yourself on missing information enhances understanding.
- Emphasize Integration: Relate new information to patient encounters, lectures, or images. Create mind maps to organize information and identify patterns.
3. Know Expectations and Thyself:
- Clarify your role and responsibilities by reviewing syllabus materials and seeking guidance from experienced peers, residents, or faculty.
- Define personal learning goals and learning style, being proactive in your approach to studying.
4. Ask! Ask! Ask!:
- Be persistent and assertive in seeking clarification, feedback, or assistance.
- Utilize the wealth of expertise within the surgical team, including nurses, physician assistants, pharmacists, social workers, and technicians.
Maximizing Your Emotional Intelligence: Strategies for Well-Being
1. Focus Forward with a Positive Attitude:
- Make decisions with a positive end in mind, maintaining situational awareness in varied scenarios.
- Cultivate open-mindedness, positive energy, and enthusiasm to contribute constructively to patient care and the team.
2. Set Goals and Celebrate Successes:
- Define short- and long-range goals, including personal, financial, and relationship goals.
- Document achievements, reinforcing a sense of accomplishment and self-confidence.
3. Promote a Supportive Learning Environment:
- Take responsibility for mistakes, learn from them, and foster trust within the team.
- Avoid negativity by steering clear of individuals with persistent negative attitudes or behaviors.
In conclusion, approach your surgery clerkship with a proactive mindset. Maximize both your intellectual capabilities and emotional intelligence to derive the utmost benefit from this transformative experience. Keep in mind the wisdom of John Wooden, emphasizing the importance of being the best version of yourself. This principle not only ensures success in your surgery clerkship but resonates throughout your medical journey.
The Stoic Surgeon: Drawing Inspiration from Marcus Aurelius in Medical Practice
Introduction
The practice of medicine and surgery, while profoundly rewarding, can also be challenging and emotionally demanding. In these moments, many professionals seek guidance and inspiration to navigate the inherent difficulties in human healthcare. A rich source of timeless wisdom can be found in the words of the philosopher-emperor Marcus Aurelius, whose Stoic teachings resonate powerfully in the context of contemporary medicine. Let’s explore how Marcus Aurelius’s ideas can illuminate and fortify medical and surgical practice.
Development
- “What we control is what we calmly accept.” – In moments of uncertainty and pressure in the operating room, the serene acceptance of circumstances is crucial for maintaining composure and focus.
- “Do not expect the doctors to do everything for you.” – Marcus Aurelius reminds us of the importance of recognizing our own limitations. Collaboration between doctor and patient is essential for effective treatment.
- “Pain is inevitable. Suffering is optional.” – When dealing with patients in painful situations, it’s vital to remember that our role extends beyond physical treatment to emotional support and alleviating suffering.
- “Doing what needs to be done when it needs to be done, to the best of our ability, is already enough.” – In a profession as demanding as medicine, it’s vital to remember that every effort dedicated to patient care is valuable and meaningful.
- “What is morally right is more important than what is legally right.” – In some situations, it may be necessary to make decisions that go beyond protocol, aiming for the best interest of the patient.
- “To wait is harmful. Not to wait is necessary.” – Readiness and agility in making medical decisions can be crucial in emergency situations.
- “Time is a river, and facts are currents; we cannot escape, we cannot choose where we will go, nor when, nor how.” – This reflection reminds us of life’s impermanence and the importance of cherishing every moment in medical practice.
- “Man’s health is our treasure.” – Marcus Aurelius emphasizes the valuable responsibility doctors have in preserving and restoring individuals’ health.
- “Every day that dawns brings some evil, which we must accept, for no day will be without it.” – Recognizing that challenges are part of the medical journey allows professionals to face them with courage and determination.
- “Where is the good, if not in doing good to those in need?” – The practice of medicine is a living testament to compassion and altruism. Through it, doctors have the opportunity to demonstrate the true essence of human kindness.
Conclusion
Just as Marcus Aurelius faced the challenges of the Roman Empire with serenity and wisdom, the modern surgeon finds in his words a guide to practicing medicine with virtue and humanity. By uniting technical skill with Stoic philosophy, the surgeon becomes not only a master of their craft but also an example of Stoic activity for the entire medical community. May each operating room be a temple of virtue and care, where the legacy of Marcus Aurelius lives on through the hands of Stoic surgeons.

The Art of Healing: Wisdom from Opus Dei for Medical Professionals
1. “Work is a path to holiness.” – Just as in Opus Dei, where work is considered a means to grow closer to God, in the field of medicine, every interaction with a patient, every diagnosis, and every surgery is an opportunity to serve and make a positive impact.
2. “In your daily work, offer up small sacrifices for your patients.” – Much like Opus Dei encourages offering up small sacrifices for spiritual growth, in medicine, dedicating extra time, attention, or effort for a patient’s well-being can be a powerful form of compassion.
3. “Strive for excellence in your field; it is a reflection of your dedication to your patients.” – Opus Dei emphasizes the pursuit of excellence in one’s profession as a form of service to God. Similarly, in medicine, continuous learning and improvement directly benefit the quality of care provided to patients.
4. “Treat each patient with dignity, respect, and kindness.” – This fundamental principle aligns with Opus Dei’s emphasis on valuing every individual. In medicine, showing compassion and empathy is as important as clinical expertise.
5. “Pray for guidance in making difficult decisions.” – Just as Opus Dei encourages seeking spiritual guidance in challenging situations, in medicine, turning to one’s faith for moral and ethical dilemmas can provide clarity and a sense of purpose.

6. “Foster a culture of trust and collaboration among colleagues.” – Opus Dei emphasizes unity and mutual support among its members. Similarly, in the medical field, teamwork and open communication are vital for providing the best possible care for patients.
7. “Never underestimate the power of a kind word or gesture.” – Small acts of kindness, like those encouraged in Opus Dei, can have a profound impact on a patient’s experience and recovery in the medical setting.
8. “Cultivate a spirit of gratitude for the opportunity to serve others.” – Recognizing the privilege of being able to heal and alleviate suffering is a perspective shared by Opus Dei and medical professionals alike.
9. “Strive for balance between professional and personal life.” – Opus Dei emphasizes the importance of a balanced life. In medicine, maintaining a healthy work-life balance is crucial for sustaining a long and fulfilling career.
10. “Embrace the challenges of medicine as opportunities for growth and service.” – Opus Dei encourages embracing life’s challenges as a means of spiritual growth. Likewise, in medicine, facing the complexities and difficulties of healthcare with dedication and compassion can lead to profound personal and professional development.
Incorporating these principles from Opus Dei into the practice of medicine can not only enhance the quality of care provided but also contribute to a more compassionate and fulfilling healthcare experience for both practitioners and patients alike.
Liderança Inspiradora de Lord Nelson: Lições para Cirurgiões Contemporâneos
A história nos presenteou com inúmeros líderes notáveis, cujas habilidades e características têm inspirado gerações ao longo dos séculos. Um desses ícones é Lord Nelson, o lendário almirante britânico do século XVIII, conhecido por sua coragem e maestria tática nas batalhas navais. Surpreendentemente, as características de liderança de Lord Nelson têm aplicações valiosas mesmo na prática contemporânea da cirurgia. Neste artigo, exploraremos algumas dessas qualidades e como nós cirurgiões podemos aplicá-las para alcançar o sucesso em nossas batalhas cirúrgicas.
“Eu sou inabalável em minha determinação, como nunca estive em minha vida, desde que coloquei o pé no convés de um navio.”
1. Determinação Inabalável: Lord Nelson era conhecido por sua determinação inabalável em alcançar seus objetivos. Ele enfrentou inúmeras adversidades e desafios durante suas batalhas navais, mas nunca desistiu diante das dificuldades. Os cirurgiões contemporâneos podemos aprender com essa qualidade, mantendo-se resilientes diante de obstáculos, buscando soluções mesmo nas situações mais desafiadoras e garantindo o melhor atendimento possível para nossos pacientes. Durante a Batalha do Nilo, em 1798, Nelson enfrentou condições adversas quando a frota britânica ficou encalhada em bancos de areia. Enfrentando uma situação aparentemente desesperadora, ele permaneceu determinado a superar os obstáculos para alcançar a vitória. Com habilidades táticas brilhantes, Nelson conseguiu finalmente manobrar sua frota para fora dos bancos de areia e alcançar uma vitória decisiva sobre a frota francesa.
“Eu sempre fui um covarde em tudo, exceto nesta profissão.”
2. Coragem sob Pressão: Durante a Batalha de Copenhague, em 1801, Nelson foi ordenado a se retirar pelo comandante em chefe, mas ele ignorou a ordem e ergueu o telescópio em seu olho cego para afirmar que não conseguia ver o sinal. Ele então liderou seu esquadrão em um ataque corajoso, superando uma poderosa defesa dinamarquesa. Sua determinação e coragem sob pressão foram fundamentais para a vitória britânica. Em meio ao caos e perigo das batalhas navais, Lord Nelson demonstrou coragem excepcional. Seu exemplo inspirador pode nos lembrar da importância de permanecermos calmos e focados, mesmo durante procedimentos complexos ou emergências médicas. A coragem para tomar decisões rápidas e precisas pode fazer a diferença entre a vida e a morte em uma sala de cirurgia.
“A vontade não pode ser chamada de coragem, mas dever, o resultado da força da mente; e qualquer um que possua esse poder, quando chega a hora de agir, encontrará a coragem que necessita.”
3. Liderança Carismática: Lord Nelson conquistou o respeito e a admiração de sua tripulação com sua liderança carismática. Durante a Batalha do Nilo, quando o perigo era iminente e a tripulação estava nervosa, Nelson subiu ao convés e enfrentou corajosamente o inimigo, encorajando seus marinheiros a seguirem seu exemplo. Sua presença inspiradora foi fundamental para manter o moral elevado e motivar sua equipe a lutar com determinação. Lord Nelson era conhecido por sua liderança carismática e inspiradora. Ele conquistou o respeito e a lealdade de sua tripulação com sua empatia e capacidade de se conectar emocionalmente com seus marinheiros. Os cirurgiões contemporâneos também podem se beneficiar ao desenvolver uma liderança que inspire confiança e motivação em suas equipes médicas, promovendo um ambiente colaborativo e eficiente.
“Eu planejo que cada homem atue de acordo com o que vê melhor, mas qualquer homem que venha entre as duas frotas, não pode ser errado, portanto, não pode ser chamado de insubordinação, mas uma obediência em que cada oficial julga por si mesmo o que é melhor a ser feito.”
4. Capacidade de Adaptação: Durante a Batalha de Trafalgar, a estratégia inicial de Nelson era enfrentar a frota inimiga de maneira mais tradicional. No entanto, quando percebeu que a formação inimiga era mais forte do que o esperado, ele rapidamente adaptou sua tática e implementou a “manobra de Nelson”, cortando a linha inimiga e concentrando seu poder de fogo para alcançar a vitória. Durante suas batalhas, Lord Nelson enfrentou situações imprevistas e mudanças de planos. Sua capacidade de adaptação e flexibilidade permitiu-lhe ajustar suas estratégias conforme necessário. Na cirurgia contemporânea, os profissionais também devem ser ágeis e adaptáveis, prontos para responder a mudanças repentinas durante procedimentos cirúrgicos complexos ou emergências médicas.
“Seja qual for a estação em que você estiver, carregue consigo o pensamento de que todos os olhos estão voltados para você. Comande a si mesmo sempre que for o exemplo de todos os outros.”
5. Comunicação Efetiva: Lord Nelson era conhecido por sua habilidade de comunicação clara e direta com sua equipe. Antes da Batalha do Nilo, ele escreveu uma carta aos marinheiros enfatizando a importância da vitória e oferecendo palavras de encorajamento. Sua mensagem sincera e motivadora demonstrava sua preocupação com o bem-estar de sua tripulação e ajudou a criar um senso de propósito comum entre seus homens. A comunicação efetiva era uma das principais características de liderança de Lord Nelson. Ele sabia como transmitir suas ordens com clareza e também valorizava o feedback de sua equipe. Cirurgiões contemporâneos podem seguir esse exemplo, enfatizando a comunicação transparente com seus colegas e pacientes para garantir que todos estejam alinhados quanto aos procedimentos e tratamentos.
Em suma, a história de Lord Nelson nos ensina que as características de liderança transcendem as épocas e têm aplicação valiosa em diversas áreas, incluindo a medicina. Ao incorporar a determinação, coragem, carisma, adaptação e comunicação efetiva de Lord Nelson, podemos nos inspirar e tornar líderes excepcionais em nossas práticas médicas, promovendo um atendimento de qualidade e impactando positivamente a vida dos pacientes. A frase ‘A Inglaterra espera que cada um faça sua parte’ tornou-se um lema inspirador e atemporal, capturando a essência da liderança de Lord Nelson na Batalha de Trafalgar. Essas palavras ecoam através dos séculos, lembrando-nos da importância da responsabilidade individual e do trabalho em equipe para alcançar o sucesso em qualquer empreendimento. Assim como os marinheiros da frota britânica foram impulsionados por esse chamado à ação, também podemos aplicar essa mensagem em nossas próprias vidas e carreiras. Como cirurgiões, somos lembrados da nossa obrigação de desempenhar cada procedimento com diligência e dedicação, e ao mesmo tempo, liderar nossas equipes com empatia e coragem. A mensagem de Lord Nelson nos inspira a superar desafios, enfrentar pressões e trabalhar juntos para alcançar os melhores resultados possíveis em nossas práticas médicas. Ao seguir esse exemplo atemporal de liderança podemos oferecer o melhor atendimento possível aos nossos pacientes e à sociedade.
Ortodoxia Cirúrgica
Embora “Ortodoxia” seja uma obra filosófica e teológica escrita por G.K. Chesterton, suas ideias podem ter algumas aplicações interessantes e reflexivas no cotidiano da cirurgia. Claro que a relação direta pode não ser evidente, mas certos princípios filosóficos podem fornecer perspectivas valiosas para os cirurgiões. Aqui estão algumas maneiras pelas quais as ideias de “Ortodoxia” podem ser aplicadas no contexto cirúrgico:
- Valorizar o pensamento paradoxal: A cirurgia é uma disciplina complexa e muitas vezes ambígua, onde os médicos devem tomar decisões cruciais em situações desafiadoras. Valorizar o pensamento paradoxal pode ajudar os cirurgiões a considerar opções diversas e até opostas antes de tomar decisões importantes.
- Reconhecimento da complexidade humana: Chesterton destaca a importância de compreender a natureza complexa da realidade. No contexto cirúrgico, isso se traduz em tratar cada paciente como um indivíduo único, com suas próprias circunstâncias médicas, emocionais e sociais. Isso pode ajudar os cirurgiões a abordar cada caso com uma mente aberta e livre de preconceitos.
- Equilíbrio entre tradição e inovação: Assim como Chesterton valoriza a tradição cultural, os cirurgiões podem se beneficiar de uma abordagem equilibrada entre as técnicas tradicionais e as inovações médicas. Combinar o conhecimento estabelecido com as mais recentes pesquisas e tecnologias pode levar a melhores resultados para os pacientes.
- Enfrentar a incerteza: A cirurgia pode ser imprevisível, e os resultados nem sempre são garantidos. A ortodoxia de Chesterton nos encoraja a aceitar a incerteza e a enfrentar os desafios com coragem e confiança. Essa mentalidade pode nos ajudar a enfrentar situações complicadas e se adaptar a cenários imprevistos.
- Importância da ética e moralidade: Chesterton enfatiza a importância da moralidade e da virtude. Na cirurgia, esses princípios são essenciais para garantir a melhor qualidade de atendimento ao paciente, respeitando sempre a dignidade e os direitos humanos.
- Valorizar a imaginação: A imaginação é uma parte essencial do trabalho cirúrgico, permitindo aos médicos visualizar procedimentos, simular situações e pensar em soluções criativas. A capacidade de imaginar possibilidades pode ajudar os cirurgiões a planejar cuidadosamente cada intervenção.
Embora “Ortodoxia” não tenha sido escrito com o objetivo específico de se aplicar à cirurgia, as ideias e princípios contidos na obra podem inspirar uma reflexão mais profunda e nos guiar de forma mais consciente, sensível e equilibrada.
As virtudes cardinais cirúrgicas
A prática cirúrgica é uma forma de arte que exige habilidade técnica e precisão, mas vai além disso. Os cirurgiões não apenas dominam as técnicas e procedimentos, mas também são desafiados a aplicar virtudes cardinais em cada etapa do ato operatório. A diérese, exérese, hemostasia e síntese, as quatro fases cruciais da cirurgia, podem ser vistas como um reflexo das virtudes cardinais: prudência, justiça, fortaleza e temperança. Vamos explorar como essas virtudes se manifestam na rotina de um cirurgião comprometido com o bem-estar dos pacientes.
Diérese (A Prudência como Guia) : A primeira etapa da cirurgia, a diérese, é o momento em que o cirurgião realiza uma incisão precisa para acessar o local a ser tratado. A prudência, virtude da sabedoria prática, entra em cena através do domínio da anatomia. O cirurgião deve avaliar cuidadosamente cada caso, analisar os riscos e tomar decisões fundamentadas. A prudência orienta a escolha das melhores abordagens cirúrgicas, levando em consideração a saúde geral do paciente, suas necessidades individuais e o objetivo final da intervenção.
Exérese (A Justiça na Busca pelo Equilíbrio): Na fase de exérese, o cirurgião remove tecidos ou estruturas comprometidas pela doença. Aqui, a justiça desempenha um papel essencial. O cirurgião deve agir com equidade, buscando remover apenas o que é necessário, sem excessos ou negligências. A justiça implica em tratar cada paciente com equidade, respeito e imparcialidade, levando em consideração os melhores interesses do indivíduo e buscando o bem comum. É um compromisso em garantir que o procedimento cirúrgico seja realizado com integridade e sempre em benefício do paciente.
Hemostasia (A Fortaleza para Enfrentar Desafios) : Durante a fase de hemostasia, o cirurgião aplica técnicas para controlar o sangramento e garantir um campo cirúrgico claro. Nesse momento, a fortaleza se faz presente. A cirurgia pode apresentar situações imprevistas, complicações ou momentos de grande pressão. A fortaleza permite ao cirurgião manter-se firme, agir com coragem diante de adversidades e tomar decisões rápidas, mas sábias, para proteger a vida e o bem-estar do paciente. A fortaleza é a virtude que impulsiona o cirurgião a enfrentar desafios com firmeza e superar obstáculos através de uma alma inabalável, mantendo durante todo o procedimento uma determinação com o melhor prognóstico do paciente.
Síntese (A Temperança na Busca do Equilíbrio Final) : A última etapa, a síntese, envolve a restauração da integridade do tecido por meio de suturas ou outros meios. Nesse momento, a temperança se revela. A temperança é a virtude que permite ao cirurgião exercer controle e moderação, evitando excessos e buscando a harmonia. A escolha adequada do material de sutura, a técnica precisa e o cuidado meticuloso são fundamentais. A temperança assegura que a finalização do ato operatório seja feita com prudência, justiça e fortaleza, considerando o bem-estar a longo prazo do paciente.
Logo, podemos concluir que a prática da cirurgia transcende a habilidade técnica e exige o cultivo das virtudes cardinais. A prudência, a justiça, a fortaleza e a temperança tornam-se guias éticos para o cirurgião comprometido com o cuidado ao paciente. A diérese, exérese, hemostasia e síntese, cada uma refletindo uma virtude cardinal, são etapas cruciais em busca da excelência médica. Quando o cirurgião incorpora essas virtudes em sua rotina, ele se torna não apenas um técnico habilidoso, mas um verdadeiro médico que busca o bem-estar e a cura integral do paciente. A arte da cirurgia, assim, se revela não apenas como uma expressão de destreza manual, mas como uma expressão do cuidado compassivo e virtuoso que o médico oferece ao paciente.
Sobre o FUTURO
Aos cinco anos, o que você queria ser quando crescesse?
Médico.
Tudo começou quando eu tinha por volta de 4 – 5 anos e após um acidente domiciliar, precisei passar por uma cirurgia na mão. A forma como aquele profissional que nos atendeu acalmou a angústia dos meus pais e tratou com habilidade o ferimento me marcou profundamente. Apesar de não ter ideia do que isso significaria na minha jornada futura, aquele sentimento de ação e resolução se tornou uma paixão que me acompanha até hoje.

Anatomia Cirúrgica da REGIÃO INGUINAL
A hérnia inguinal é uma condição comum que ocorre quando um órgão abdominal protraí através de uma fraqueza na parede abdominal na região abdominal. O orifício miopectineal é a principal área de fraqueza na parede abdominal onde a hérnia inguinal pode se desenvolver. O conhecimento da anatomia da parede abdominal é importante para entender a patofisiologia da hérnia inguinal e para ajudar no diagnóstico e tratamento dessa condição médica comum.
A Arte da Anatomia (EBook)
Desde a Antiguidade, os médicos, anatomistas e artistas se dedicaram a descrever e representar o corpo humano, por meio de desenhos, pinturas, esculturas e outras formas de representação artística. Com o passar dos séculos, houve uma evolução significativa na forma como as ilustrações anatômicas eram produzidas, desde as primeiras representações rudimentares até as ilustrações altamente detalhadas e realistas que temos hoje.
Boa Leitura!!!
Michelangelo Buonarroti
5 Segredos de Anatomia Escondidos na Capela Sistina: A Neuroanatomia Clandestina de Michelangelo
Autor: Prof. Dr. Ozimo Gama (Tempo de Leitura: 10 minutos)
Onde a Fé e o Bisturi se Encontram
Na formação médica contemporânea, o estudo da anatomia topográfica num laboratório de dissecação é o rito de passagem fundamental para qualquer cirurgião. No Brasil, apesar dos desafios atuais na captação de cadáveres para estudo nas faculdades de medicina, a dissecação continua a ser a base insubstituível da técnica cirúrgica. Contudo, no século XVI, o estudo do corpo humano além da superfície era um tabu severo, vigiado de perto pelas leis civis e canónicas. Michelangelo Buonarroti, celebrado mundialmente pela sua terribilità — aquela força emocional e técnica avassaladora —, viveu um paradoxo perigoso. O artista profundamente religioso era também um anatomista clandestino. Desafiando os dogmas de sua época, ele dedicou inúmeras noites à dissecação de cadáveres, buscando nos tendões, fáscias e vísceras a geometria da perfeição biológica. O que a humanidade demorou 500 anos para perceber é que Michelangelo não utilizou este conhecimento apenas para conferir realismo hipertrófico às suas figuras; ele codificou verdadeiras lições de neuroanatomia diretamente no teto da Capela Sistina. O santuário do conclave papal guarda um mapa do intelecto humano, sugerindo que a verdadeira centelha divina reside na intrincada arquitetura do sistema nervoso central. Abaixo, dissecamos os 5 segredos anatómicos ocultos nesta obra-prima.
A Anatomia Oculta nos Afrescos
1. O Cérebro como a “Faísca Divina” em A Criação de Adão
Em 1990, o médico norte-americano Frank Meshberger publicou uma descoberta no prestigiado Journal of the American Medical Association (JAMA) que alterou o curso da história da arte e da medicina. Ele demonstrou que a figura de Deus, envolta num manto avermelhado e cercada por anjos, compõe um corte sagital milimetricamente exato de um cérebro humano. A genialidade reside nos detalhes: o contorno inferior do manto segue com precisão o sulco lateral (Fissura de Sylvius). O braço estendido do Criador atravessa exatamente o giro do cíngulo. Um “anjo” posicionado inferiormente desenha o trajeto da artéria basilar, enquanto o pé bifurcado de um querubim representa a glândula pituitária (hipófise). Para Michelangelo, o que Adão recebe no toque não é apenas o fôlego biológico, mas o intelletto — a razão suprema.
2. O Tronco Encefálico no Pescoço de Deus
A análise de A Criação de Adão revela o cérebro macroscópico, mas o painel central A Separação da Luz das Trevas aprofunda-se em estruturas neurais complexas. Em 2010, os investigadores Ian Suk e Rafael Tamargo, neurocirurgiões da Universidade Johns Hopkins, identificaram um detalhe audacioso. O pescoço de Deus exibe uma anatomia irregular que foge à hipertrofia muscular renascentista padrão. Utilizando um escorço dramático (técnica de perspetiva que encurta a figura), Michelangelo camuflou uma visão ventral do tronco encefálico humano. Estão lá, representados com rigor de atlas cirúrgico, o bulbo, a ponte e a estrutura em forma de “Y” característica dos nervos óticos e do quiasma ótico.
3. Arquitetura Neural: Ventrículos e o Corpo Caloso
A investigação ganhou novos contornos em 2015, quando Ciurea et al. identificaram como o mestre utilizou a técnica do chiaroscuro (luz e sombra) aplicando o princípio da Gestalt para ocultar formas. Na mesma cena da Separação da Luz das Trevas, os olhos treinados de um neuroanatomista conseguem completar as figuras:
- Área A: O quarto ventrículo perfeitamente delineado.
- Área B: A ponte de Varólio, formada pela curvatura da coxa direita da divindade, exibindo a oliva pontina e o sulco colateral anterior.
- Área C: O manto superior que emula uma imagem espelhada do corpo caloso (a via de comunicação entre os hemisférios cerebrais). A inversão da imagem serviu para manter o fluxo estético sem perder a mensagem anatómica.
4. O Anatomista Clandestino de Santo Spirito
Para que um artista atingisse tal nível de detalhe no século XVI — superando as obras de Galeno (que se baseavam em dissecações de macacos e porcos) —, a observação clínica superficial não bastaria. Aos 18 anos, Michelangelo firmou um acordo secreto com o prior da Igreja de Santo Spirito, em Florença. Em troca da escultura de um crucifixo de madeira, o prior permitia-lhe dissecar cadáveres humanos no hospital da igreja durante a madrugada. armado com um bisturi primitivo, ele antecipou descobertas que a medicina oficial, com Andreas Vesalius, só documentaria décadas mais tarde.

5. Uma Mensagem de Protesto e Subversão (A Costela Oculta)
O anatomista era também um livre-pensador influenciado pelo Neoplatonismo florentino. O investigador Deivis Campos (2019) identificou uma “costela extra” no lado esquerdo do torso de Adão. Ao invés de pintar uma costela a ser removida para a criação de Eva (como ditava o dogma), Michelangelo pintou uma costela extra e oculta. Esta representação anatómica subversiva sugere que as essências feminina e masculina coexistem na natureza humana original, uma alusão ao misticismo da Cabala e um protesto velado contra a interpretação literal das escrituras.
Pontos-Chave para a Formação Médica
- A Observação é a Base da Medicina: O génio de Michelangelo prova que a capacidade de observar minuciosamente a anatomia é o que separa o conhecimento superficial da verdadeira maestria.
- Integração Arte e Ciência: As estruturas neurais (fissura de Sylvius, tronco encefálico, quiasma ótico) pintadas no século XVI mostram que a medicina e a arte nasceram da mesma curiosidade intrínseca sobre o milagre da vida.
- O Cérebro como Sede da Consciência: Ao colocar o sistema nervoso central no epicentro do ato da Criação, Michelangelo antecipou em séculos a premissa da neurociência moderna: somos o nosso cérebro.
Conclusões Aplicadas à Prática do Cirurgião
Para o cirurgião do aparelho digestivo, ou de qualquer outra especialidade, a história de Michelangelo traz uma lição de humildade e reverência. Quando entramos no centro cirúrgico e realizamos uma incisão, não estamos apenas a manipular tecidos e órgãos; estamos a interagir com a mais sublime e complexa arquitetura do universo conhecido. Se o maior segredo do Renascimento — o mapeamento do nosso intelecto na morada do papado — permaneceu oculto por cinco séculos à vista de todos, devemos questionar-nos diariamente: o que mais estamos a falhar em enxergar nos nossos doentes devido à pressa ou à desatenção clínica? A medicina de excelência exige o olhar crítico do cientista e a sensibilidade meticulosa do artista.
“Onde o espírito não conduz a mão do artista, não há arte. E onde o conhecimento da anatomia não conduz a mão do médico, não há cura. A estrutura do corpo humano é a obra-prima inquestionável do Criador.” — Adaptado dos pensamentos do Renascimento Médico.
Gostou ❔Nos deixe um comentário ✍️ , compartilhe em suas redes sociais e|ou mande sua dúvida pelo 💬 Chat On-line em nossa DM do Instagram.
Specific Competence of Surgical Leadership
Surgeons are uniquely prepared to assume leadership roles because of their position in the operating room (OR). Whether they aspire to the title or not, each and every surgeon is a leader, at least within their surgical team. Their clinical responsibilities offer a rich variety of interpretations that prepare them for a broader role in health care leadership. They deal directly with patients and their families, both in and out of the hospital setting, seeing a perspective that traditional health care administrative leaders rarely experience. They work alongside other direct providers of health care, in varied settings, at night, on weekends, as well as during the typical workday. They understand supply-chain management as something more than lines on a spreadsheet.
The Challenges for a Surgical Leader
Surgeons prefer to lead, not to be led. Surgical training has traditionally emphasized independence, self-reliance, and a well-defined hierarchy as is required in the OR. However, this approach does not work well outside the OR doors. With colleagues, nurses, staff, and patients, they must develop a collaborative approach. Surgeons are entrusted with the responsibility of being the ultimate decision maker in the OR. While great qualities in a surgeon in the OR, it hinders their interactions with others. They have near-absolute authority in the OR, but struggle when switching to a persuasive style while in committees and participating in administrative activities. Most surgeons do not realize they are intimidating to their patients and staff. With patients, a surgeon needs to be empathetic and a good listener. A surgeon needs to slow the pace of the discussion so that the patient can understand and accept the information they are receiving. As perfectionists, surgeons demand a high level of performance of themselves. This sets them up for exhaustion and burnout, becoming actively disengaged, going through the motions, but empty on the inside. Given the many challenges surgeons face, it is difficult for them to understand the leadership role, given its complex demands.
Specific Competencies
Authority
Although teams and all team members provide health care should be allowed input, the team leader makes decisions. The leader must accept the responsibility of making decisions in the presence of all situations. They will have to deal with conflicting opinions and advice from their team, yet they must accept that they will be held accountable for the performance of their team. The surgeon–leader cannot take credit for successes while blaming failures on the team. Good teamwork and excellent communication do not relieve the leader of this responsibility.
Leadership Style
A surgeon often has a position of authority based on their titles or status in an organization that allows them to direct the actions of others. Leadership by this sort of mandate is termed “transactional leadership” and can be successful in accomplishing specific tasks. For example, a surgeon with transactional leadership skills can successfully lead a surgical team through an operation by requesting information and issuing directives. However, a leader will never win the hearts of the team in that manner. The team will not be committed and follow through unless they are empowered and feel they are truly heard. A transformational leader is one who inspires each team member to excel and to take action that supports the entire group. If the leader is successful in creating a genuine atmosphere of cooperation, less time will be spent giving orders and dealing with undercurrents of negativity. This atmosphere can be encouraged by taking the time to listen and understand the history behind its discussion. Blame should be avoided. This will allow the leader to understand the way an individual thinks and the group processes information to facilitate the introduction of change. While leadership style does not guarantee results, the leader’s style sets the stage for a great performance. At the same time, they should be genuine and transparent. This invites the team members to participate, creating an emotional connection. Leaders try to foster an environment where options are sought that meet everyone’s desires.
Conflict Management
Conflict is pervasive, even in healthy, well-run organizations and is not inherently bad. Whether conflict binds an organization together or divides it into factions depends on whether it is constructive or destructive. A good leader needs to know that there are four essential truths about conflict. It is inevitable, it involves costs and risks, the strategies we develop to deal with the conflict can be more damaging than the conflict itself, and conflict can be permanent if not addressed. The leader must recognize the type of conflict that exists and deal with the conflict appropriately. Constructive discussion and debate can result in better decision making by forcing the leader to consider other ideas and perspectives. This dialog is especially helpful when the leader respects the knowledge and opinions of team members with education, experience, and perspective different from the leader’s. Honesty, respect, transparency, communication, and flexibility are all elements that a leader can use to foster cohesion while promoting individual opinion. The leader can create an environment that allows creative thinking, mutual problem solving, and negotiation. These are the hallmarks of a productive conflict. Conflict is viewed as an opportunity, instead of something to be avoided.
Communication Skills
Communication is the primary tool of a successful leader. On important topics, it is incumbent on the leader to be articulate, clear, and compelling. Their influence, power, and credibility come from their ability to communicate. Research has identified the primary skills of an effective communicator. They are set out in the LARSQ model: Listening, Awareness of Emotions, Reframing, Summarizing, and Questions. These are not set in a particular order, but rather should move among each other freely. In a significant or critical conversation, it is important for a leader to listen on multiple levels. The message, body language, and tone of voice all convey meaning. You cannot interrupt or over-talk the other side. They need an opportunity to get their entire message out. Two techniques that enhance listening include pausing and the echo statement. Pausing before speaking allows the other conversant time to process what they have said to make sure the statement is complete and accurate. Echo statements reflect that you have heard what has been said and focuses on a particular aspect needing clarification. Good listening skills assure that the leader can get feedback that is necessary for success.
Vision, Strategy, Tactics, and Goals
One of the major tasks of a leader is to provide a compelling vision, an overarching idea. Vision gives people a sense of belonging. It provides them with a professional identity, attracts commitment, and produces an emotional investment. A leader implements vision by developing strategy that focuses on specific outcomes that move the organization in the direction of the vision. Strategy begins with sorting through the available choices and prioritizing resources. Through clarification, it is possible to set direction. Deficits will become apparent and a leader will want to find new solutions to compensate for those shortfalls. For example, the vision of a hospital is to become a world class health care delivery system. Strategies might include expanding facilities, improving patient satisfaction, giving the highest quality of care, shortening length of hospital stay with minimal readmissions, decreased mortality, and a reduction in the overall costs of health care. Tactics are specific behaviors that support the strategy with the aim to achieve success. Tactics for improving patient satisfaction may include reduced waiting time, spending more time with patients, taking time to communicate in a manner that the patient understands, responding faster to patient calls, etc. These tactics will then allow a leader to develop quantitative goals. Patient satisfaction can be measured. The surgical leader can then construct goals around each tactic, such as increasing satisfaction in specific areas. This information allows a surgical leader to identify barriers and they can take steps to remedy problem areas. This analysis helps a leader find the weakest links in their strategies as they continue toward achieving the vision.
Change Management
The world of health care is in continuous change. The intense rate of political, technical, and administrative change may outpace an individual’s and institution’s ability to adapt. Twenty-first century health care leaders face contradictory demands. They must navigate between competing forces. Leaders must traverse a track record of success with the ability to admit error. They also must maintain visionary ideas with pragmatic results. Individual accountability should be encouraged, while at the same time facilitating teamwork. Most leaders do not understand the change process. There are practical and psychological aspects to change. From an institutional perspective, we know that when 5% of the group begins to change, it affects the entire group. When 20% of a group embraces change, the change is unstoppable.
Succession Planning and Continuous Learning
An often-overlooked area of leadership is planning for human capital movement. As health care professionals retire, take leaves of absences, and move locations, turmoil can erupt in the vacuum. Leaders should regularly be engaging in activities to foster a seamless passing of institutional knowledge to the next generation. They also should seek to maintain continuity to the organization. Ways to accomplish this include senior leaders actively exposing younger colleagues to critical decisions, problem solving, increased authority, and change management. Leaders should identify promising future leaders, give early feedback for areas of improvement, and direct them toward available upward career tracks. Mentoring and coaching help prepare the younger colleagues for the challenges the institution is facing. Teaching success at all levels of leadership helps create sustainable high performance.
Aula de Anatomia do Dr Nicolaes Tulp (1632)
O valor da obra “A Aula de Anatomia do Dr. Nicolaes Tulp” é incalculável, pois ela pertence ao acervo do Mauritshuis, em Haia, na Holanda, e é considerada uma das mais importantes e valiosas obras do museu. Além disso, a pintura é uma das mais famosas obras de Rembrandt e uma das mais importantes do período Barroco holandês. Por isso, é considerada uma obra-prima da arte ocidental e tem um valor histórico, artístico e cultural inestimável. Embora não haja um valor monetário exato para a pintura, pode-se dizer que é uma das obras mais valiosas e procuradas do mundo da arte, tanto pelo seu significado histórico quanto pela sua qualidade artística.
“A Aula de Anatomia do Dr. Nicolaes Tulp” é uma pintura a óleo sobre tela, criada por Rembrandt van Rijn em 1632. A obra mede 169,5 cm x 216,5 cm e está atualmente exposta no Mauritshuis, em Haia, na Holanda. A composição da pintura apresenta um grupo de homens em torno de uma mesa de dissecação, liderados pelo médico Nicolaes Tulp, que está realizando uma demonstração de anatomia. O corpo sendo dissecado é o de um criminoso enforcado chamado Aris Kindt. A composição apresenta uma disposição simétrica e organizada das figuras em torno da mesa, com Tulp no centro da imagem.
A luz na pintura é focada no corpo sendo dissecado, destacando-o em relação ao fundo escuro da sala. A técnica de chiaroscuro usada por Rembrandt acentua o realismo e o drama da cena. As figuras são pintadas em tons de marrom, cinza e preto, com destaques de branco. A obra apresenta detalhes precisos e realistas da anatomia do corpo, bem como das ferramentas médicas utilizadas na dissecação. O corpo do criminoso apresenta uma ferida na cabeça e uma perna amputada, o que sugere que ele pode ter sido executado por um crime violento.
No canto inferior direito da pintura, há um livro aberto com o título “Spiegel der Konst” (“Espelho da Arte”), um tratado de anatomia escrito por Adriaan van de Spiegel e utilizada pelos médicos da época. Em geral, a “Aula de Anatomia do Dr. Nicolaes Tulp” é uma obra-prima devido à sua técnica precisa e detalhada, bem como à sua habilidade em transmitir um senso de realismo e drama. A pintura é considerada uma das obras mais importantes do período Barroco holandês e é frequentemente citada como um exemplo do estilo de pintura de Rembrandt.
A seguir estão algumas das características artísticas e estéticas da obra:
- Composição: A pintura apresenta uma composição equilibrada e organizada, com as figuras dos membros da guilda cirúrgica em torno da mesa de dissecação centralizada.
- Luz e Sombra: Rembrandt usa uma técnica conhecida como chiaroscuro, ou contraste entre luz e sombra, para dar profundidade e dimensão à cena. A luz focaliza no cadáver e no médico principal, destacando-os do fundo escuro.
- Realismo: A pintura é altamente realista, mostrando detalhes precisos das ferramentas cirúrgicas, do cadáver e das expressões dos personagens.
- Cores: O uso limitado de cores em tons de marrom e cinza dá à pintura uma atmosfera austera e solene.
- Simbolismo: A pintura inclui vários elementos simbólicos, como a presença de uma coruja, que representa sabedoria, e a posição da mão do cadáver, que simboliza a morte.
- Técnica: A pintura foi executada com uma técnica de pincelada solta e fluida, que enfatiza a textura e a superfície da pintura.
Em geral, a “Aula de Anatomia do Dr. Nicolaes Tulp” é considerada uma obra-prima devido à sua habilidade técnica e sua capacidade de transmitir um senso de realismo e drama. A pintura é considerada uma das obras mais importantes do período Barroco holandês e é frequentemente citada como um exemplo do estilo de pintura de Rembrandt.

Role of The SURGEON

Attributes of a Good Surgeon
Realising the benefits that good leadership and teamwork can deliver requires commitment from all those involved in patient care. From the surgeon’s viewpoint there are numerous desirable attributes which are developed through medical school education, foundation training, core training and into professional practice. These are outlined below:
1. Clinical Care
An obvious consideration of what makes a “good surgeon” is the care provided to patients throughout the patient journey. This includes technical ability in the operating theatre and non-technical skills.
2. Maintenance and Improvement
Remaining up-to-date with innovations in surgical practice and patient are is an important attribute of a good surgeon. In doing so, one is able to inform patients and explain the reasons for and against procedures, allowing them to make an informed decision. Willingness to learn from others and improve from others by reviewing personal practice forms part of Continuing Professional Development; this is a requirement in a portfolio to meet revalidation and recertification criteria.
3. Teaching, Training and Supervision
Educating others forms part of professional development and surgeons frequently oversee projects for medical students or trainees. This requires knowledge of the objectives of the tasks undertaken, knowledge of what technical and non-technical skills should be improved and knowledge of how to encourage the development of these skills. The mentormentee relationship should work both ways, such that the mentee is able to approach their supervisor for assistance and is accepting of any constructive criticism delivered.
4. Relationships with Patients
Relationships with patients are fundamentally based on trust; the patient trusts that the surgeon will do all in their power to help them and their surgical journey. Obtaining informed consent prior to clinical care is based on trust and allows patient autonomy to be upheld. Developing relationships with patients begins from the first consultation and is continued after the day of an operation being undertaken. Acknowledging the needs of the individual and employing effective communication helps in developing an open relationship. In this way patients disclose their medical history and admit underlying fears, allowing better patient care to be delivered.
5. Relationships with Colleagues
Partnership with all members of the multidisciplinary clinical team, management, technicians and support staff fosters healthy working relationships. Consequently, patient care is enhanced through communication, enhanced productivity and an improved team dynamic. Understanding how a colleague works and taking action to facilitate a positive working environment is beneficial to all. Emotional intelligence forms an important component of working relationships, through the ability “to understand and recognize emotional states and to use that understanding to manage one’s self and other individuals or teams”.
6. Health
Maintenance of good personal health and knowing when you must stop working is important in the protection of patient safety. The relevant senior staff must be informed of communicable disease or blood-borne disease transmission. In addition, being vigilant of the health of colleagues forms part of protecting patient safety, for example, failure to report suspicion that the consultant consistently operates after several glasses of wine or that the CT2 has been seen smoking drugs can facilitate the propagation of errors in the workplace. Finally, surgeons are renowned for working at all hours, however acknowledgement that we all need rest is crucial in good patient care.
“Not Only SURGEONS…”
SURGERY, A NOBLE PROFESSION
Surgery is, indeed, one of the noblest of professions. Here is how Dictionary defines the word noble: 1) possessing outstanding qualities such as eminence, dignity; 2) having power of transmitting by inheritance; 3) indicating superiority or commanding excellence of mind, character, or high ideals or morals. These three attributes befit the profession of surgery. Over centuries, the surgical profession has set the standards of ethical and humane practice. Surgeons have made magnificent contributions in education, clinical care, and science. Their landmark accomplishments in surgical science and innovations in operative technique have revolutionized surgical care, saved countless lives, and significantly improved longevity and the quality of human life. Generations of surgeons have developed their craft and passed it on to succeeding generations, as they have to me and to each one of you, to take into the future.
Beyond its scientific and technical contributions, surgery is uniquely fulfilling as a profession. It has disciplined itself over the centuries and dedicated its practice to the best welfare of all human beings. In return, it has been accorded the respect of society, of other professions, and of policy makers. Its conservative stance has served it well and has been the reason for its constancy and consistency. At the beginning of the 21st century, however, profound changes are taking place at all levels and at a dizzying pace, providing both challenges and opportunities to the surgical profession. These changes are occurring on a global level, on the national level, in science and technology, in healthcare, and in surgical education and practice.
To retain its leadership position in innovation and its attractiveness as a career choice for students, surgery must evolve with the times. It is my belief that surgery needs to introduce changes to create new priorities in clinical practice, education, and research; to increase the morale and prestige of surgeons; and to preserve general surgery as a profession. I am reminded of a Chinese aphorism that says, “You cannot prevent the birds of unhappiness from flying over your head, but you can prevent them from building a nest in your hair.”
ADVANCES IN SCIENCE
The coalescence of major advances in science and technology made the end of the 20th century unique in human history. Notable among the achievements are the development of microchips and miniaturization, which fueled the explosion in information technology. The structure of the human genome is nearly completely elucidated, ushering in the genomic era in which genetic information will be used to predict, on an individual basis, susceptibility to disease and responsiveness to drug therapy. The field of nanotechnology allows scientists to work at a resolution of less than one nanometer, the size of the atom. By comparison, the DNA molecule is 2.5 nanometers.
In the last 50 years, biomedical research became increasingly reductionist, turning physiologists and anatomists into molecular biologists. As a result, two basic science fields—integrative physiology and gross anatomy—now have a lower standing in medical education and surgical science than they once did. Surgery and surgical departments can and possibly should claim these fields, but the window of opportunity is narrow. Research is now moving back from discipline-based reductionist science to multidisciplinary science of complexity, in which biomedical scientists work side by side with engineers, mathematicians, and bioinformatists. The ability of high-speed computers to quickly process tens of millions of pieces of data now allows for data-driven rather than hypothesis-based research. This collaboration among different disciplines has already been successful.
TRANSFORMATION OF HEALTHCARE SYSTEM
During the past 75 years, we have seen the entire healthcare system undergo a profound transformation. In the 1930s and for a considerable period thereafter, medical practice was fee-for-service, the doctor–patient relationship was strong, and the physician perceived himself or herself as being responsible nearly exclusively to his or her individual patients. The texture of medical practice started to change when the federal government became involved in the provision of healthcare in 1965. The committee on “Crossing the Quality Chasm” identified six key attributes of the 21st-century healthcare system. It must be:
- Safe, avoiding injuries to patients;
- Effective, providing services based on scientific knowledge;
- Patient-oriented, respectful of and responsive to individual patients’ needs, values, and preferences;
- Timely, reducing waits, eliminating harmful delays for both care receiver and caregiver;
- Efficient, avoiding wasted equipment, supplies, ideas, and energy;
- Equitable, providing equal care across genders, ethnicities, geographic locations, and socioeconomic strata;
No one knows at present what this 21st-century healthcare system will look like. While care in the old system was reactive, in the new system it will be proactive. The “find it, fix it” approach of the old system will be replaced by a “predict it, prevent it, and if you cannot prevent it, fix it” approach. Sporadic intervention, provided only when patients present with illness, will give way to a system in which physicians and other healthcare providers plan 1-, 5-, and 10-year care programs for each patient. Care will be more interactive, with patients taking a more important role in their own care. The technology-oriented system will become a system that provides graded intervention. Delivery systems will not be fractionated but integrated. Even more importantly, care will not be based simply on experience and clinical impression but on evidence of proven outcome measures. If the old system was cost-insensitive, the new system will be cost-sensitive.
SURGICAL PRACTICE
There are many reasons for the declining interest in general surgery, some of which parallel reasons for the drop in medical school applicants in general. One problem specific to surgery is that medical students are given less and less exposure to surgery, due to the shortening of required surgical rotations. Most important, however, is their perception that the life of the surgical resident is stressful, the work hours too long, and the time for personal and family needs inadequate. The workload of the surgical resident over the years has increased significantly both in amount and intensity, without concomitant increase in the number of residents and at a time when hospitals have significantly reduced the support personnel on the surgical ward and in the operating rooms. Students graduating with debts close to $100,000 simply find the years of training in surgery too long, followed by uncertain practice income after graduation.
From several recent studies, lifestyle is the critical and most pressing issue in surgical residency. Some studies have also shown that the best students tend to select specialties that provide controllable lifestyles, such as radiology, dermatology, and ophthalmology. We have a problem not only in the declining number of students applying for surgical training but also in the declining quality of those who do apply. In a preliminary survey of 153 responding general surgery programs, we found that attrition (i.e., categorical residents leaving the training programs) occurred at a rate of 13% to 19% in the last 5 years. In 2001, 46% of those leaving general surgery training programs cited lifestyle as the major reason.
Unless these trends are reversed, general surgery as a specialty is threatened, and a future shortage of general surgeons is inevitable. I know that the Council of the American Surgical Association is most concerned about the crisis in general surgery. We must do a better job of communicating to students and residents that the practice of surgery is as rewarding as ever and full of opportunities in this new era. Innovations in minimal access and computer-assisted surgery and simulation technology provide exciting new possibilities in surgical training. We must also look very carefully at the demands of surgical residency and improve the life of residents without compromising their surgical experience. Unless we deal with work hours and quality of life issues, we are likely to see continuing decline in the interest of medical students in surgical training.
CONCLUSIONS
In conclusion, the noble profession of surgery must rise to meet numerous challenges as the world in which it operates continues to undergo profound change. These challenges represent opportunities for the profession to develop an international perspective and a global outreach and to address the growing needs of an aging population undergoing major demographic and workforce shifts. The leadership of American surgery has a unique role to play in the formulation of a new healthcare system for the 21st century. This task will require commitment to quality of care and patient safety, and it will depend on harnessing the trust and support of the American public. Advances in science and technology—particularly in minimal access surgery, robotics, and simulation technology—provide unprecedented opportunity for surgeons to continue to make landmark contributions that will improve surgical care and the human condition. I believe it is also crucially important that we train surgeon-scientists who will keep surgery at the cutting edge in the genomic and bioinformatics era. Ours is a noble profession imbued with eminence, dignity, high ideals, and ethical values. It has a rich and proud heritage… and I quote, “The highest intellects, like the tops of mountains, are the first to catch and reflect the dawn.”
Source: Lecture from Haile T. Debas, MD (UCSF School of Medicine, San Francisco, California) Presented at the 122nd Annual Meeting of the American Surgical Association, April 25, 2002, The Homestead, Hot Springs, Virginia.
Adverse events in SURGERY
The surgical domain can be seen as more complex and high risk in its delivery of care than other non-interventional specialities. It is therefore not surprising that in the majority of studies of adverse events in healthcare, at least 50% occurred within the surgical domain and the majority of these in the operating theatre. Furthermore, at least half of these adverse events were also deemed preventable. Just as the multiple studies in the developed world have similar figures for adverse events in hospitalised patients across all specialities, there appears to be a similar rate of harm in surgery. A review of 14 studies, incorporating more than 16000 surgical patients, quoted an adverse event occurring in 14.4% of surgical patients. This was not simply minor harm; a full 3.6% of these adverse events were fatal, 10% severe and 34% moderately harmful. Gawande, a surgeon from Boston, made one of the first attempts to clarify the source of these adverse events.

This paper pioneered the concept that the majority of these adverse events were not due to lack of technical expertise or surgical skill on the part of the surgeon, finding instead that ‘systems factors’ were the main contributing factor in 86% of adverse events. The most common system factors quoted were related to the people involved and how they were functioning in their environment. Communication breakdown was a factor in 43% of incidents, individual cognitive factors (such as decision-making) were cited in 86%, with excessive workload, fatigue and the design or ergonomics of the environment also contributing.
These findings were confirmed in the systematic review of surgical adverse events, where it was found that errors in what were described as ‘nonoperative management’ were implicated in 8.32% of the study population versus only 2.5% contributed to by technical surgical error. In accordance with other high-risk industries, such as commercial aviation, the majority of these adverse events are therefore not caused by failures of technical skill on the part of the individual surgeon, but rather lie within the wider healthcare team, environment and system. Lapses and errors in communication, teamworking, leadership, situational awareness or decision-making all feature highly in post-hoc analysis of surgical adverse events. This knowledge of error causation has been prominent and acknowledged in most other high-risk industries for many years, but it is only recently that healthcare has appreciated this.
Ao Cadáver DESCONHECIDO
Hic locus est ubi mors gaudet succurrere vitae
“É este o lugar onde a morte se alegra de socorrer a vida”
Égide do respeito ao Cadáver no estudo da Anatomia Humana*.
A utilização do cadáver representa uma tríplice lição educativa:
- Instrutiva/Informativa: como meio de conhecimento da organização do corpo humano, procedendo ao estudo no vivo;
- Normativa/Disciplinadora: através do seu caráter metodológico e de precisão técnica da linguagem;
- Estético/Moral: pela natureza do material de estudo, o cadáver, e pelo método primeiro de aprendizado, a dissecção, que é experiência e trabalho repousante na contemplação da beleza e harmonia de construção do organismo humano.
Contudo e essencialmente, porém, lição de ética e de humildade, porque:
- Não é o cadáver, doado ou indigente, fato isolado da comunidade, mas seu reflexo, dela provindo. O cadáver que é o meio de aprendizado para adequada assistência do vivo, assim portanto tão importante para a sociedade como o é o paciente;
- Esses corpos sem vida são vivificados de forma reiteradas pelo calor da juventude estudiosa através do sentimento de gratidão; O cadáver, antes de tudo “um irmão em Humanidade, se entrega despojadamente ao conhecimento que proporciona aos futuros profissionais, de maneira anônima oriunda do jogo do acaso da vida;
- O cadáver anônimo ao receber este título – cadáver desconhecido – e assim ultrapassar o limite estreito de um nome e, despersonalizado, distribui elementos para o bem coletivo, sem ter conhecimento quer antes, durante ou depois de sua imolação, do seu destino a um tempo sublime e sagrado;
- O Cadáver desconhecido tudo oferece ao conhecimento sem nada haver recebido daquele que o estuda, que dá sem saber que dá e por isso, sem conhecer recompensa da gratidão e sem sentimento do valor da sua dádiva generosa, na mais nobre expressão de poderosa caridade universal;
- O cadáver que dissecado, desmembrado, simboliza outra forma de crucificação para o bem comum e marca o sentido profundamente humano da Medicina;
Portanto o nosso material de estudo transcende pois ao simples valor de meio e objeto de aprendizado; e nos fala em linguagem universal que nos educa na humildade da limitação humana. Eis porque na austeridade do ambiente do Laboratório de Anatomia a atitude física, mental e verbal do aluno deve ser de sobriedade, respeito, meditação e elevada compostura, manuseando as peças anatômicas com o mais profundo sentimento de respeito e carinho.
Nulla Medicina Sine Anatomia
“Ao curvar-te sobre o cadáver desconhecido…
lembra-te que este corpo nasceu do amor de duas almas; cresceu embalado pela fé e esperança daquela que em seu seio o agasalhou, sorriu e fitou os mesmos sonhos das crianças e dos jovens; por certo amou, foi amado e também acalentou um amanhã feliz. Seu nome só Deus o sabe e agora nesta fria lousa, o destino inexorável deu-lhe o poder e a grandeza de servir a humanidade numa última missão, ENSINAR.
Ó irmão ignoto que tivestes a morada do espirito, o seu corpo, perturbado em seu repouso imutável por nossas mãos ávidas de saber, apresentamos a ti o nosso respeito permanente e infindo AGRADECIMENTO.”
*Adaptação do texto original “Aula Inaugural”
Professor Renato Locchi (1896-1978) / Emérito de Anatomia Humana da Escola Paulista de Medicina.
História da Anatomia Humana
Atualmente, o conhecimento da anatomia se junta a um universo de outros conhecimentos que, não menos importantes, vão se somando e contribuindo de forma muito rápida para o desenvolvimento científico, para a melhoria da qualidade de vida e para a maior longevidade do ser humano. A anatomia e a medicina são ciências distintas, porém não há como separar a história de ambas. Estão ligadas intimamente e por muito tempo sendo que, na antiguidade, foram tratadas como uma só história. Ana, em partes; tome, cortar. O termo anatomia, de origem grega, significa “cortar em partes”. Antigamente referia-se ao ato de explorar as estruturas do corpo humano por uso de instrumentos cortantes como anatomizar, hoje substituído pela palavra dissecar. E foi a dissecção de cadáveres humanos que serviu como método de estudo para o entendimento da estrutura e função do corpo humano durante vários séculos. Devido ao incessante trabalho de centenas de anatomistas dedicados ao aprendizado e evolução do conhecimento acerca do corpo humano, e suas de funções, é que hoje nós, estudantes, podemos aprender e familiarizar com os termos anatômicos utilizados para designar cada estrutura dessa engenhosa “máquina” que é o ser humano. Grande parte dos termos que compõe a linguagem anatômica é de procedência grega ou latina. Latim era a língua do império romano, época em que o interesse nas descrições científicas foi cultivado. No passado, a anatomia humana era acadêmica, ciência puramente descritiva, interessada principalmente em identificar e dar nomes às estruturas do corpo. Embora a dissecção e descrição formem a base da anatomia, a importância desta, hoje, está em sua abordagem funcional e nas aplicações clínicas, de forma a entender o desempenho físico e a saúde do corpo.
Aprendendo a Aprender
As oportunidades de aprendizado nos são oferecidas a cada momento, o tempo todo. Aprendemos toda vez que nos damos ao trabalho de pensar sobre o que determinado momento nos trouxe, o que nos ensinou que ainda não sabíamos, o que nos mostrou a respeito dos outros e de nós mesmos, e que antes ignorávamos. E esse processo é tão longo quanto a vida.
O caminho mais curto e certo para a estagnação é perder a disposição de aprender, seja pela arrogância de achar que já sabe tudo, seja pela enganosa convicção de que é cedo demais para adquirir tal conhecimento. A acomodação é outra inimiga do aprendizado, pois paralisa o segundo requisito necessário para que ele ocorra: o esforço. É preciso esforçar-se para manter a mente aberta ao novo, para não se deixar limitar pelos preconceitos e opiniões preconcebidas. E também é preciso esforço para ampliar as oportunidades de aprendizado, reservando tempo para as leituras, para as conversas e atividades instrutivas, para se atualizar e aprofundar seu conhecimento.
Não refiro apenas ao conhecimento necessário à sua profissão, mas a todos os aspectos de sua vida, por exemplo, conhecer mais a fundo sua família – acreditar que já sabemos tudo sobre nossos familiares é um erro fatal em qualquer tipo de relacionamento. Outro equívoco é negligenciar o autoconhecimento: uma série de frustrações, angústias e motivações. Conhecê-las também é um aprendizado constante, talvez o mais árduo de todos.
“Todas me pareceram tão cheias de si”, contou Sócrates, “tão seguras de suas verdades e certezas que, se sou de fato mais sábio do que elas, é pela simples razão de que sei de que não sei aquilo que elas acham que sabem”. Como nos sugere o filósofo com toda a sua perspicácia e sabedoria, a admissão de que ainda temos muito a aprender é o primeiro passo para transformarmos nossa vida em um constante aprendizado. A consciência desse fato enriquece nossas vidas, ampara nossas escolhas e direciona nossas ações. A importância de aprender sempre é tamanha que Stephen R. Covey, autor do best-seller Os 7 Hábitos das Pessoas Altamente Eficazes e 8° Hábito, a coloca entre as quatro necessidades básicas do ser humano – as demais serão afetadas.
O aprendizado, porém, está presente em todas: aprendemos a viver, a amar, a deixar um legado e, até mesmo, aprendemos a aprender.
NOTTS: OR Etiquette

If OR etiquette represents a code of conduct—respect, communication, shared mental model, and teamwork—then manners represent the behaviors that embody this code of behavior. These seem like simple rules that should have been learned at an early age, but a few pointers will go a long way toward integrating junior residents and students into the OR team.
1. Be polite.
2. Be respectful.
3. Be humble.
4. Learn everyone’s name.
5. Offer help without being asked.
6. Ask for help when needed.
7. Thank your colleagues.
8. Keep the patient at the center of all you do.
Rude, disruptive, or disrespectful behavior is not tolerated. Do not yell or make sarcastic comments. Do not make jokes with sexual or racial themes. Do not gossip or denigrate others. Many surgeons enjoy listening to music in the operating room, but in choosing a playlist, be aware that some music may have offensive lyrics that should not be played in the workplace. It is most polite to ask before playing music and to check in with music preferences, as not everyone in the OR may appreciate loud death metal. Music should be turned off during critical times such as the initial time-out. Surgeons use social media like many others, but the OR is not the place to check Facebook or Instagram. When posting to social media, be professional—anything posted to the Internet can be screen captured and spread, no matter what privacy settings you may have turned on. A recent study of publicly accessible Facebook posts showed 14.1% of surgery residents had posted potentially unprofessional content, and 12.2% had clearly unprofessional content, with violations of patient privacy being one of the most common problems, along with description of binge drinking and racially or sexually offensive material. Specific to the OR, be aware that social media postings with potentially identified patient information are absolutely forbidden. This does not need to include a name of a patient to be identifiable information—a few details of a particularly unique case and a timestamped posting can be enough to cause trouble.
NOTTS: Giving and Receiving Feedback

Feedback has gained an increasingly important role in surgical education. Feedback may be summative and/or formative. Summative feedback is often given at discrete time points such as the end of a rotation and is a culmination of observations of performance. Formative feedback involves an ongoing assessment of skills or knowledge and may be given throughout an education experience. There is an often misunderstood distinction between teaching and feedback. As an example, teaching is when the attending surgeon corrects the resident’s needle angle during a bowel anastomosis. Feedback is when the attending surgeon and resident meet after the case and discuss performance—either technical or nontechnical. For example, a feedback session might discuss room setup, efficiency, technical maneuvers, and communication. Giving and receiving feedback are distinct skills that require both parties to be attentive and open. To facilitate this process, several methods have been described that turn feedback into an active process for both parties. Ideally, the mentor and the trainee have a briefing prior to the case in order to set learning objectives and then formally debrief after the case to discuss how well the learning objectives were met as well as ways to improve this in the future. In the press of clinical concerns and the drive toward efficiency, the debrief session is often skipped or missed. It is incumbent on the learner, therefore, to specifically seek out and ask the attending surgeon for feedback and if necessary to schedule formal meeting times. It is also important for feedback to flow both ways, and the attending surgeon should ask for feedback from the residents as well. A good methodology for providing feedback is to ask an open-ended question such as “How did you think that operation went?” Which can be followed with “What went well?” and “What could have gone better?” This allows the person providing feedback with a baseline to start from and allow for self-reflection on the part of the learner. This can be followed with specific feedback about one to two actionable items, preferably relating back to the goals stated during the initial briefing.
NOTTS: Leadership and Followership

Although the OR may seem like a highly regimented environment, each member of the surgical team will serve as both a “leader” and a “follower” at different points during the operation. This includes everyone from the most senior attending surgeon to the most junior medical student. Within the OR, the surgical attending has ultimate responsibility for the patient. However, surgical residents will often act as leaders to junior residents and medical students. In the setting of “progressive autonomy” for surgical trainees, the attending surgeon may also formally or informally cede control of the case to the resident or fellow and may take a follower role him or herself. In fact, more often than not, the surgical attending will assist a senior resident through a case, rather than perform the operation with the resident’s assistance. In the OR, the team leader is responsible for setting the tone. It is up to the leader to make sure that all team members have a shared understanding of how the day will proceed as well as any potential problems that may arise. In many cases, the surgical attending does not arrive to the OR until the patient has arrived, been intubated, and prepped and draped. In this case, it is up to the senior-most resident to lead the team. A resident who arrives early, completes the surgical timeout in a thorough but efficient manner, and moves the room forward is much more effective than one who arrives late or is not familiar with the patient or the case. While an extensive discussion of successful leadership traits is outside of the realm of this chapter, in general a good leader is one who outlines a clear vision of the work that needs to be accomplished while also empowering those around them to take ownership over their individual work. While leadership is a commonly discussed topic, what is less commonly discussed is the importance of “followership.” While there are several different descriptions of the various types of “followers” on any given team, many focus on a spectrum from passive to active and from dependent, uncritical thinking to independent, critical thinking. Compared to the field of leadership, the study of followership is relatively new, but it is generally agreed that effective followers are those who are paying attention to what is going on around them, taking an active interest in the process, and questioning or challenging leadership or the status quo when necessary. This last point is especially critical. In the OR, being a good follower is a crucial component to maintaining patient safety as it is incumbent upon the followers (including residents, medical students, nursing staff, and all other participants) to speak up if they notice that something is going wrong or that the environment has become unsafe. Especially for more junior members of the team, it can be intimidating to alert the attending that he or she may be making a mistake or misjudging the situation. However, it is important to remember that such actions, when carried out with tact and respect, are in the best interest of the patient and may actually prevent serious harm from occurring.