Variações Anatômicas da Árvore Biliar Extra-Hepática no Contexto da Colecistectomia Laparoscópica
Introdução A compreensão das variações anatômicas dos ductos biliares extra-hepáticos é essencial para a realização segura da colecistectomia laparoscópica. A terminologia frequentemente utilizada para descrever essas variações inclui termos como “acessório”, “anômalo” e “aberrante”. Entretanto, essas variações são naturais e suficientemente frequentes para serem antecipadas pelo cirurgião atento. A preferência é pelo termo “duto variante”.
Marcos Anatômicos Gerais para a Orientação
Durante a colecistectomia laparoscópica, é crucial reconhecer marcos anatômicos adjacentes para evitar lesões. O ligamento falciforme situa-se entre os segmentos hepáticos 3 e 4, e o ducto hepático comum (DHC) está próximo ao plano mediano do fígado entre os segmentos 4 e 5. O sulco de Rouvière é uma fissura que contém porções do pedículo portal direito e demarca o plano ventral-dorsal do ducto biliar comum (DBC), auxiliando na orientação durante a dissecção.
Anatomia dos Ductos Hepáticos Direitos
Na configuração mais comum, o ducto hepático seccional anterior direito (segmentos 5 e 8) e o ducto hepático seccional posterior direito (segmentos 6 e 7) unem-se para formar o ducto hepático direito (DHD), que se junta ao ducto hepático esquerdo para formar o DHC. Essa anatomia ocorre em 57-72% dos indivíduos. Em 15-30% dos casos, os ductos seccionais direito anterior e posterior não se unem, cada um tendo uma junção separada com o DHC ou o ducto hepático esquerdo, aumentando o risco de lesão durante a cirurgia.

Ductos Subvesicais
Os ductos subvesicais, localizados superficialmente no leito da vesícula biliar, são a fonte mais comum de vazamento biliar pós-operatório. Observados em cerca de um terço dos espécimes humanos, esses ductos, geralmente originários do segmento 5, drenam para o ducto hepático direito, o DHD ou o DHC. A dissecção deve ser mantida fora do fígado sempre que possível para evitar lesões.
Anatomia do Ducto Cístico
O ducto cístico geralmente se junta ao DHC, com a localização da junção variando do hilo hepático à área pré-ampular. Configurações paralelas e espirais do ducto cístico são comuns e representam fatores de risco significativos para lesões durante a colecistectomia. Fusão inflamatória e contração do ducto cístico são situações de alto risco.
A variabilidade anatômica dos ductos biliares extra-hepáticos requer uma abordagem cuidadosa durante a colecistectomia laparoscópica para evitar lesões. O conhecimento detalhado das possíveis variações e a identificação precisa dos marcos anatômicos são fundamentais para o sucesso cirúrgico. As variações anatômicas dos ductos biliares são frequentes e devem ser esperadas pelos cirurgiões. A terminologia adequada e o reconhecimento dessas variações são cruciais para prevenir lesões durante a colecistectomia laparoscópica. Como afirmou Lahey: “A variação anatômica é a regra, não a exceção.”
Referências
- Michels, NA. “Every duct drains a definite segmental area of the liver.”
- Strasberg, SM. “Anatomic and historical basis of variations in bile ducts.”
- Bismuth, H. “Variations in the anatomy of the extrahepatic bile ducts.”
Diferenciação Morfológica do Ducto Cístico e do Ducto Colédoco no Contexto da Colecistectomia Laparoscópica
Introdução
Na cirurgia laparoscópica, a precisão na identificação e dissecação das estruturas anatômicas é fundamental para a prevenção de lesões iatrogênicas da via biliar. O conhecimento detalhado das variações anatômicas do ducto cístico e do ducto colédoco é essencial para evitar complicações graves. Conforme disse Lahey em 1954: “Cholecystectomy is a dangerous operation unless one realizes that variations are very common.” Assim, a terminologia anatômica deve ser correta, consistente e padronizada para evitar mal-entendidos.
Anatomia Normal
O ducto cístico conecta a vesícula biliar ao ducto hepático comum, formando o ducto colédoco. Este último é a principal via de passagem da bile do fígado para o duodeno. A correta identificação dessas estruturas é crucial durante a colecistectomia para evitar lesões.
Dimensões e Diâmetro
O ducto cístico geralmente tem um comprimento de 2-4 cm e um diâmetro de 1-5 mm. Já o ducto colédoco mede aproximadamente 6-8 cm de comprimento e tem um diâmetro que varia de 4-10 mm.
Trajeto e Topografia
O ducto cístico apresenta um trajeto sinuoso, que pode variar significativamente entre os pacientes. Ele se une ao ducto hepático comum para formar o ducto colédoco, que desce posteriormente ao duodeno até a ampola de Vater. A topografia dessas estruturas é fundamental para a correta dissecação durante a cirurgia.
Vascularização
O ducto cístico é irrigado principalmente pela artéria cística, um ramo da artéria hepática direita. O ducto colédoco, por sua vez, recebe irrigação de pequenos ramos axiais das artérias hepática direita, gástrica direita e pancreatoduodenal onde 60% é inferior e 40% é superior.
Epônimos e Terminologia Correta
Historicamente, a anatomia hepato-biliar tem sido confundida por diferentes nomenclaturas e epônimos imprecisos. O termo “triângulo de Calot”, descrito por Jean-Francois Calot em 1890, refere-se à área limitada pelo ducto cístico, o ducto hepático comum e a artéria cística. No entanto, o triângulo de Calot não é uma definição anatomicamente precisa, sendo preferível o termo “triângulo hepatocístico”, que é delimitado pelo ducto cístico e a vesícula biliar, o ducto hepático comum e a borda do fígado. Esta é uma área crítica onde ductos hepáticos direitos e a artéria hepática direita podem ser encontrados, sendo comumente obscurecida por inflamação aguda ou crônica.
Principais Variações Anatômicas e Suas Incidências
As variações anatômicas são comuns e devem ser antecipadas. Cerca de 20% dos ductos císticos seguem um trajeto paralelo ao ducto hepático comum, compartilhando uma bainha comum de tecido conjuntivo. Outros 5-10% têm um curso espiralado, cruzando o ducto hepático comum de forma ventral ou dorsal. As variações no trajeto e na união dos ductos são fatores de risco significativos para lesões durante a cirurgia.
Idiotopia em Relação ao Duodeno e Holotipia em Relação à Tríade Portal
O ducto colédoco passa diretamente atrás do duodeno, uma característica que o diferencia do ducto cístico durante a dissecção. Em relação à tríade portal, o ducto cístico e o ducto colédoco são componentes críticos, juntamente com a artéria hepática e a veia porta, sendo importantes marcos anatômicos para a orientação cirúrgica.
Sintopia Entre Eles
A relação espacial entre o ducto cístico e o ducto colédoco é complexa e varia com a inflamação e a dissecção cirúrgica. Durante a colecistectomia, a visualização clara do “triângulo hepatocístico” é fundamental para identificar corretamente o ducto cístico e evitar danos ao ducto colédoco.
Conclusão
O entendimento detalhado das variações anatômicas do ducto cístico e do ducto colédoco é crucial para a realização segura da colecistectomia laparoscópica. A aplicação do conceito da “vista crítica de segurança” ajuda a minimizar os riscos de lesões. Portanto, a terminologia precisa e o conhecimento das variações anatômicas são fundamentais para a prática cirúrgica segura.
Colecistectomia Laparoscópica Segura
Histórico
A primeira colecistectomia laparoscópica foi realizada por Mouret em Lyon, em 1988, com o primeiro relato escrito por Dubois em 1989. Reddick popularizou o procedimento nos Estados Unidos em 1990.
Indicações e Contraindicações
Indicações:
- Mesmas da colecistectomia aberta.
- O cirurgião deve estar adequadamente treinado para realizar o procedimento.
- Manifestações de cálculos biliares sintomáticos: cólica biliar, histórico de icterícia, colecistite crônica e aguda.
- Pancreatite por cálculos biliares.
- Colecistite acalculosa.
- Pólipos grandes na vesícula biliar.
Contraindicações:
- Não há contraindicações absolutas.
- Contraindicações relativas incluem cirrose, hipertensão portal, diátese hemorrágica e gravidez, podendo requerer modificações técnicas.
Investigação Pré-operatória e Preparação
- Testes de Função Hepática: Essenciais para avaliar a função hepática.
- Ultrassonografia: Tipicamente realizada para avaliar a condição da vesícula biliar.
- Estudos Nucleares: Utilizados para avaliar a função da vesícula biliar na colecistite acalculosa.
- Tomografia Computadorizada (TC): Necessária se houver suspeita de câncer na vesícula biliar ou grandes pólipos.
- CPRE (Colangiopancreatografia Retrógrada Endoscópica): Não realizada rotineiramente no pré-operatório.
- Antibióticos Profiláticos: Administrados na indução.
- Medidas Antitrombóticas: Devem ser tomadas medidas preventivas adequadas.
Variações Anatômicas
- As principais variações anatômicas envolvem o ducto biliar comum e a artéria hepática direita.
- Variações do Ducto Biliar Comum: Um ducto biliar comum muito pequeno pode ser confundido com o ducto cístico e excisado.
- Variações de Junção dos Ductos Hepáticos: Junções baixas dos ductos hepáticos ou aberturas diretas da bolsa de Hartmann podem levar à identificação e divisão incorreta dos ductos.
- Ausência de Ducto Cístico: Em alguns casos, a bolsa de Hartmann se abre diretamente no ducto hepático direito ou no ducto comum, complicando o procedimento.
Complicações Intraoperatórias
- Hemorragia: Geralmente ocorre de uma artéria cística curta ou da artéria hepática direita. A hemorragia da veia porta é rara, mas torrencial, exigindo conversão imediata para cirurgia aberta.
- Falha de Progressão: Se o procedimento não está progredindo, deve ser convertido para colecistectomia aberta.
- Lesão do Ducto Biliar: Técnicas adequadas e conversão oportuna para cirurgia aberta minimizam o risco. Consultar imediatamente um especialista em hepatobiliar se ocorrer uma lesão.
Complicações Pós-operatórias
- Fugas Biliares: A maioria é de baixo volume e resolve-se espontaneamente. Fugas de alto volume requerem CPRE para avaliação e manejo.
- Coleção Subfrênica: Pode necessitar de drenagem percutânea.
- Pneumonia: Tratada com fisioterapia e antibióticos.
- Icterícia: Indica obstrução ou lesão maior do ducto, necessitando de CPRE ou encaminhamento a um especialista.
Dicas do Cirurgião Sênior
- Hipertensão Portal e Cirrose: Considerar colecistectomia parcial para evitar hemorragias com risco de vida.
- Colecistite Aguda Severa: Descomprimir a vesícula biliar aspirando seu conteúdo para torná-la mais manejável.
- Cálculo Impactado na Bolsa de Hartmann: Empurrar o cálculo de volta para a vesícula biliar para permitir a manipulação segura do triângulo de Calot.
Técnicas Específicas
Ilustração da Técnica:
- Posicionamento dos Instrumentos: A vesícula biliar é levantada em direção cefálica com um primeiro fórceps inserido pelo portal na linha médio-clavicular, logo abaixo do rebordo costal, para segurar o pescoço da vesícula. Um segundo fórceps é inserido pelo portal na linha axilar anterior para empurrar o cólon e o duodeno para baixo, liberando o campo de visão.
- Incisão na Serosa: A incisão na serosa sobre a junção do ligamento hepatoduodenal é estendida paralelamente a uma linha a 5 mm da borda do fígado, melhorando a visualização do triângulo de Calot.

- Manobras de Tração: O pescoço da vesícula é retraído para baixo e a serosa é retraída para cima com o segundo fórceps, criando contra-tração e ampliando a visualização do triângulo de Calot. Isso também evita lesões térmicas desnecessárias na superfície do fígado.
- Dissecção e Identificação: Tecidos adiposos e bandas fibrosas são removidos até que a relação anatômica entre o ducto cístico e a artéria cística seja clara. A eletrocauterização é usada com cautela para evitar lesões térmicas no ducto biliar comum.
- Colangiografia Intraoperatória: Protagonistas da colangiografia intraoperatória sugerem que essa investigação pode minimizar o risco de lesão do trato biliar extra-hepático, fornecendo um registro anatômico preciso. No entanto, a dissecção cuidadosa e a identificação dos ductos são essenciais.
Complicações durante a Colecistectomia Laparoscópica:
- Cálculos Múltiplos e Aderências: Podem dificultar o procedimento e aumentar o risco de complicações, como lesões térmicas em órgãos adjacentes.
- Hemorragia e Fugas Biliares: A hemorragia deve ser controlada com coagulação ou clipes, e as fugas biliares são geralmente geridas com endoloop após aspiração da bile.
- Extração de Cálculos: Cálculos que escapam devem ser removidos com fórceps para prevenir abscessos intra-abdominais.
Conclusão
A colecistectomia laparoscópica é um procedimento padrão com indicações específicas. A preparação pré-operatória, conhecimento das variações anatômicas e técnicas cirúrgicas meticulosas são cruciais para o sucesso. O manejo eficaz das complicações intra e pós-operatórias garante a segurança e a recuperação do paciente.
Lesão da Via Biliar Durante a Colecistectomia
A lesão da via biliar é uma complicação significativa tanto na colecistectomia aberta quanto na laparoscópica. Na colecistectomia aberta, o risco é de aproximadamente 1 em 1000 casos. No entanto, na colecistectomia laparoscópica as taxas de lesão da via biliar comum variam entre 0,2% e 3%.
Popularidade da Colecistectomia Laparoscópica
Apesar do maior risco de lesão na colecistectomia laparoscópica, sua popularidade continua a crescer entre cirurgiões e o público em geral. Este aumento se deve aos benefícios percebidos, como menor dor pós-operatória, cicatrizes menores e recuperação mais rápida. No entanto, essas vantagens podem ser rapidamente anuladas por uma única lesão da via biliar.
Fatores de Risco e Procedimentos
Estudos, como o de Easter e Moossa, mostraram que a dissecção a laser está associada a um maior risco de lesão em comparação com o uso de eletrocautério. As lesões ocorrem frequentemente devido à dificuldade de visualização clara do campo operatório, exacerbada por inflamação, cicatrizes ou sangramento na região do triângulo de Calot.
Diferenças na Tração Durante a Cirurgia
Durante a colecistectomia aberta, as forças opostas aplicadas ao fígado e ao duodeno tendem a alinhar o ducto biliar comum de maneira a minimizar sua angulação. Em contraste, na colecistectomia laparoscópica, a tração lateral e cefálica na vesícula biliar pode fazer com que o ducto cístico e o ducto biliar distal fiquem alinhados no mesmo plano, aumentando o risco de confusão anatômica e lesão inadvertida do ducto hepático comum.
Estratégias de Prevenção
Para minimizar o risco de lesões, recomenda-se uma tração lateral do fundo da vesícula biliar e uma dissecção cuidadosa no nível do infundíbulo antes da aplicação de clipes ou divisão das estruturas no triângulo de Calot. A colangiografia intraoperatória é fundamental sempre que houver dúvida sobre a anatomia, pois pode ajudar a identificar anomalias anatômicas ou lesões antes que ocorram complicações graves.
Importância do Reconhecimento Precoce
Os sintomas pós-operatórios de anorexia, íleo, náuseas ou vômitos que não melhoram conforme esperado após uma colecistectomia laparoscópica podem indicar uma lesão ductal. A detecção precoce dessas lesões e o reparo imediato por um cirurgião experiente são essenciais para um bom prognóstico a longo prazo. Lesões não detectadas durante o procedimento inicial frequentemente resultam em complicações mais graves, como peritonite biliar e estenoses anastomóticas.
Considerações Finais
Embora a colecistectomia laparoscópica ofereça vantagens significativas, é crucial que os cirurgiões estejam cientes de seus riscos e limitações. A conscientização e o reconhecimento dos fatores de risco podem ajudar a alcançar o nível de segurança esperado na colecistectomia aberta, garantindo melhores resultados para os pacientes.
Colecistectomia Segura
A colecistectomia laparoscópica, amplamente utilizada para a remoção da vesícula biliar, oferece muitas vantagens em relação à técnica aberta tradicional. Entre os benefícios estão a redução da dor pós-operatória, menor tempo de internação hospitalar e recuperação mais rápida. No entanto, esses benefícios não devem compensar a maior incidência de lesões no ducto biliar comum associada ao procedimento laparoscópico em determinadas situações.

Riscos das Lesões no Ducto Biliar
Como enfatizado por Sackier, lesões no ducto biliar comum podem resultar em complicações graves, muitas vezes referidas como “aleijados biliares”. Essas lesões podem levar a estenoses recorrentes, necessitando de múltiplas cirurgias e aumentando o risco de cirrose biliar secundária e falência hepática. O ditado cirúrgico, “o único pecado capital na cirurgia das vias biliares é a lesão do ducto biliar comum”, reflete a gravidade dessas complicações. A morbidade e mortalidade associadas a essas lesões são altas: mais de 25% dos pacientes sofrem complicações em cirurgias de seguimento e a mortalidade pós-operatória imediata de estenoses benignas do ducto biliar é de 8,3%, com uma mortalidade a longo prazo de 13%. A principal causa de morte nesses pacientes é a falência hepática, resultante de sepse ou lesão no suprimento sanguíneo do fígado, ou desenvolvendo-se como cirrose biliar e hipertensão portal.
Incidência e Prevenção
Nos Estados Unidos, são realizadas aproximadamente 500.000 colecistectomias anualmente. Em colecistectomias abertas, o risco de lesão no ducto biliar comum é de cerca de 0,1%, ou seja, 500 pacientes por ano. Para a técnica laparoscópica, os dados variam, com estudos iniciais relatando incidências de 0 a 7%. Estudos mais recentes indicam riscos entre 0,2% e 0,3%, o que significa que cerca de 1.500 pacientes por ano podem sofrer lesões no ducto biliar comum, uma incidência duas a três vezes maior em comparação com a técnica aberta. Trabalhos mais recentes mostram atualmente uma equiparação nos índices de lesões das vias biliares.
Estratégias Preventivas
Para minimizar o risco de lesões, diversas estratégias foram desenvolvidas com base na literatura relevante e nas práticas do Columbia-Presbyterian Medical Center:
- Seleção Apropriada de Pacientes: A colecistectomia laparoscópica não deve ser a escolha para todos os pacientes. Fatores de risco como cicatrizes abdominais, inflamação aguda severa e obesidade grave devem ser consideradas no momento do planejamento cirúrgico.
- Dissecção Cuidadosa: Identificação meticulosa da anatomia é crucial, especialmente devido às limitações visuais bidimensionais da cirurgia laparoscópica.
- Uso do Laparoscópio de 30°: Este oferece uma visão mais ampla do ducto biliar comum, permitindo uma visualização mais segura.
- Retração Apropriada: A tração cefálica no fundo da vesícula biliar e tração posterior e lateral no infundíbulo são necessárias para evitar a distorção do ducto biliar comum.
- Dissecção do Junção Ducto Cístico-Vesícula Biliar: Diferenciar entre o ducto cístico entrando na vesícula e alargando-se no infundíbulo é vital.
- Identificação do Junção Ducto Cístico-Ducto Biliar Comum: A junção deve ser visualizada e o caminho do ducto biliar comum deve ser determinado.
- Relaxamento da Retração: Relaxar a retração no infundíbulo antes de clipar o ducto cístico garante que o ducto biliar comum não esteja sendo tracionado.
- Manutenção de um Remanescente Longo do Ducto Cístico: Evita lesões no ducto biliar comum.
- Evitar Procedimentos Potencialmente Lesivos Próximos à Porta Hepática: Dissecção afiada aumenta o risco de sangramento e lesão.
- Uso liberal de Colangiografia Intraoperatória: Dúvidas na anatomia e diagnosticar lesões imediatamente para reparo imediato (caso o cirurgião tenha experiência em cirurgia hepatobiliar) melhora significativamente os resultados.
- Baixo Limite para Conversão para Cirurgia Aberta: Converte-se para a técnica aberta diante de circunstâncias difíceis, em especial o sangramento, para garantir segurança.
- Curva de Aprendizado: A maioria das lesões no ducto biliar comum ocorre devido à inexperiência (<50 casos). Programas de treinamento adequados podem reduzir essas lesões.
Considerações Finais
Apesar da baixa incidência geral de lesões no ducto biliar comum durante a colecistectomia laparoscópica, a preocupação com o aumento de lesões em comparação com a técnica aberta é válida. As lesões causadas pela técnica laparoscópica são mais extensas e difíceis de reparar, frequentemente ocorrendo em pacientes jovens e saudáveis. As vantagens da colecistectomia laparoscópica não trazem benefícios se aumentarem a possibilidade de lesões graves. Essas medidas preventivas e estratégias adequadas podem tornar a colecistectomia laparoscópica tão segura quanto, ou até mais segura do que, a técnica aberta.
Does routine performance of IOC prevent common bile duct injuries?
The main goals of IOC are to identify bile duct stones, clarify biliary anatomy, and prevent bile duct injuries. Indications for IOC during laparoscopic cholecystectomy may include jaundice or a history of jaundice, a history of pancreatitis particularly related to gallstone pancreatitis, elevated liver function tests, a common bile duct larger than 5-7mm in diameter, a cystic duct larger than 3mm in diameter, multiple small gallbladder stones, unclear anatomy, common bile duct stones visualized on preoperative ultrasound, possible bile duct injury or leak, and a short cystic duct.
The SAGES guidelines for the clinical application of laparoscopic biliary tract surgery recommended that IOC may decrease the risk of bile duct injury when used routinely and can allow access to the biliary tree for therapeutic intervention (Level II evidence, grade B recommendation). In a more recent guideline from the European Association for Endoscopic Surgery (EAES) regarding the prevention and treatment of bile duct injuries during laparoscopic cholecystectomy, the authors commented that the routine use of IOC remained controversial and that routine IOC could not be recommend based on the available literature. This guideline, however, indicated that IOC allows forearly identification of bile duct injuries as long as they are correctly interpreted.
Recommendation
Surgeons should use IOC liberally, be familiar with its indications, and become facile with the technique and interpretation of cholangiogram images. While IOC may decrease the risk of bile duct injury its routine use remains controversial; further high quality evidence is needed before routine IOC can be recommended. (Quality of evidence: +++, weak)
Requisitos Fundamentais da Clínica Cirúrgica
Atul Gawande, um autor celebrado por suas perspectivas perspicazes sobre a saúde, especialmente no campo cirúrgico, ofereceu insights valiosos que ressoam com profissionais médicos. Em seu livro “Complicações: Notas de um Cirurgião sobre Desempenho,” Gawande articula três requisitos fundamentais para o sucesso na medicina:
Diligência: Enfatiza a importância da atenção meticulosa aos detalhes para prevenir erros e superar desafios.
Fazer o Certo: Reconhece que a medicina é, inerentemente, uma profissão humana, destacando o imperativo ético de priorizar o bem-estar do paciente.
Ingenuidade: Incentiva uma mentalidade de inovação, instigando os praticantes a pensarem de maneira diferente, abraçar mudanças e aprender com os fracassos.
Gawande vai além de definir esses requisitos fundamentais e oferece cinco sugestões convincentes sobre como indivíduos podem causar um impacto positivo dentro de sua cultura profissional:
Faça uma Pergunta Não Roteirizada: Defende perguntas espontâneas que podem levar a descobertas inesperadas e fomentar uma cultura de comunicação aberta.
Não Reclame: Aconselha contra reclamações improdutivas, enfatizando que isso não resolve problemas nem contribui construtivamente para discussões. Incentiva os indivíduos a estarem preparados com tópicos alternativos para discussão.
Conte Algo: Promove a prática de quantificar aspectos do próprio trabalho. Gawande sugere que contar algo de interesse pessoal leva a insights valiosos e aprendizado contínuo.
Escreva Algo: Reconhece o poder transformador de escrever ou digitar. Encoraja os profissionais a documentarem experiências, insights e reflexões, aprimorando tanto o aprendizado pessoal quanto coletivo.
Mude—Seja um Adaptador Precoce: Reconhece a necessidade de abraçar mudanças, especialmente no panorama em rápida evolução da tecnologia cirúrgica. Instiga os indivíduos a serem adaptadores precoces, mantendo-se atualizados com inovações para aprimorar o cuidado ao paciente.
As orientações de Gawande vão além dos aspectos técnicos da medicina, adentrando os domínios da comunicação, mentalidade e desenvolvimento profissional. Esses princípios fornecem um roteiro para que os profissionais médicos não apenas se destaquem em suas capacidades individuais, mas também influenciem positivamente a cultura mais ampla na qual operam.
“O sucesso na medicina é cultivado não apenas através da habilidade técnica, mas pela dedicação incessante ao aprendizado, inovação e ao compromisso com o bem-estar do paciente.”
O Legado do Dr. William Stewart Halsted: Pioneiro da Cirurgia Moderna
A história da medicina é marcada por avanços revolucionários que transformaram a prática clínica, o ensino e os cuidados aos pacientes. Entre os nomes que se destacam neste cenário, o do cirurgião norte-americano William Stewart Halsted (1852–1922) é, sem dúvidas, um dos mais influentes. Halsted não apenas elevou os padrões da cirurgia, mas também criou um modelo de treinamento que se tornou a base para a formação de cirurgiões em todo o mundo, com aplicações diretas no tratamento das doenças do aparelho digestivo.
O Início de uma Jornada Brilhante
Nascido em Nova York, Halsted iniciou sua formação acadêmica com forte ênfase em anatomia e fisiologia, que mais tarde se tornariam a base de suas contribuições à medicina. Após se formar na College of Physicians and Surgeons, em 1877, ele ampliou seus horizontes ao estudar em centros de excelência europeus, como Viena e Hamburgo, onde foi influenciado por cirurgiões renomados como Theodor Billroth e Johannes von Mikulicz.
Contribuições ao Tratamento Cirúrgico do Aparelho Digestivo
Entre os muitos campos em que Halsted deixou sua marca, destaca-se a cirurgia do aparelho digestivo. Seu estudo experimental sobre suturas intestinais, realizado no início de sua carreira em Baltimore, estabeleceu as bases para anastomoses seguras e eficazes. Ele demonstrou que a submucosa é a camada crítica para sustentação das suturas, um conceito que permanece fundamental até hoje. Outro marco foi seu pioneirismo em ressecções gastrointestinais e controle de sangramentos intra-abdominais. Sua abordagem técnica, caracterizada por dissecação cuidadosa e manuseio gentil dos tecidos, minimizou complicações como infecção e deiscências, ampliando significativamente as chances de sucesso em cirurgias de alta complexidade.
O Modelo Halstediano de Treinamento Cirúrgico
Um dos legados mais duradouros de Halsted foi seu modelo de residência médica, implementado no Hospital Johns Hopkins. Ele estabeleceu um sistema hierárquico com responsabilidades graduais, permitindo que residentes desenvolvessem habilidades progressivamente. Esse método não apenas garantiu um treinamento mais completo, mas também formou líderes que perpetuaram suas ideias. Para a cirurgia do aparelho digestivo, essa abordagem foi crucial. O treinamento intensivo em anatomia, fisiopatologia e técnicas operatórias sofisticadas possibilitou avanços significativos no manejo de doenças como cânceres gastrointestinais, doenças inflamatórias intestinais e patologias biliares.
Avanços e a Influência no Ensino Moderno
Embora o modelo Halstediano tenha sido modificado ao longo das décadas, seus princípios básicos continuam sendo a espinha dorsal da educação cirúrgica. Programas atuais incorporam avanços tecnológicos, como cirurgia robótica e simulações, mas a ética da responsabilidade progressiva e a atenção aos detalhes, promovida por Halsted, permanecem inalteradas.
Reflexão Final
O legado de William Stewart Halsted é inestimável. Suas contribuições estabeleceram os alicerces da cirurgia moderna, com implicações diretas na melhora do cuidado ao paciente e na educação médica. Para estudantes e residentes, entender sua história é compreender as origens de muitas práticas e conceitos que hoje são considerados padrão na formação e prática cirúrgica.
“A grandeza de um cirurgião não reside apenas em suas habilidades técnicas, mas na sua dedicação contínua em aprimorar a arte de curar.” – William Stewart Halsted.
Gostou ❔ Nos deixe um comentário ✍️ , compartilhe em suas redes sociais e|ou mande sua dúvida pelo 💬 Chat On-line em nossa DM do Instagram.
Hashtags:
#CirurgiaDigestiva #EducaçãoMédica #HistóriaDaCirurgia #ResidênciaMédica #WilliamHalsted
Maestria na Cirurgia Digestiva
Em seu aclamado livro “Fora de Série: Outliers – Descubra Por Que Algumas Pessoas Têm Sucesso e Outras Não”, Malcolm Gladwell explora a essência da maestria, destacando a regra das 10.000 horas popularizada pelo neurologista Daniel Levitin. Esta regra postula que são necessárias impressionantes 10.000 horas de prática dedicada para alcançar a maestria e a excelência em qualquer campo. Gladwell examina diversos campos, de compositores e jogadores de basquete a escritores de ficção e cirurgiões, encontrando o fio condutor recorrente da marca de 10.000 horas.
A Discrepância no Treinamento Cirúrgico ⏰🔍
No contexto do treinamento cirúrgico, no entanto, uma diferença marcante surge. Residentes chefes de cirurgia em formação são encarregados de documentar aproximadamente 850 casos, muito aquém do marco das 10.000 horas. Mesmo considerando uma estimativa de 2 horas por caso, as horas acumuladas ficam significativamente aquém. A ênfase do Coach Carril no trabalho em equipe, na atenção meticulosa e na importância do momento presente alinha-se com o conceito de prática deliberada. Nesses 850 casos, os residentes são incentivados a focar no aprimoramento de técnicas e a aproveitar cada oportunidade de desenvolvimento de habilidades.
Trabalho em Equipe, Fundamentos e Prática Deliberada 🤝📚
Os princípios do Coach Carril ecoam a necessidade de trabalho em equipe e concentração nos aspectos fundamentais, ressoando com as percepções de Gladwell. O princípio nº 18 de Carril, que enfatiza a importância da tarefa presente, alinha-se com a ideia de prática deliberada—imersão total na experiência de aprendizado atual. Residentes, assim como jogadores de basquete que aprimoram suas habilidades, encontram valor na prática focada e intencional para superar a lacuna de treinamento.
Cirurgia: A Tríade Satisfatória de Autonomia, Complexidade e Conexão 🌐💼💡
Gladwell ainda postula três atributos-chave que tornam o trabalho satisfatório para os indivíduos: autonomia, complexidade e uma conexão tangível entre esforço e recompensa. A cirurgia, por sua própria natureza, encapsula esses elementos. A autonomia reina na tomada de decisões e nas habilidades procedimentais, a complexidade se manifesta nos intrincados aspectos de várias cirurgias, e a conexão entre esforço e recompensa é evidente tanto para o paciente quanto para o praticante.
A Recompensa do Cirurgião: A Sobrevivência do Paciente e a Compensação Pessoal 🏥💰
No cerne da satisfação cirúrgica está a profunda conexão entre o esforço do cirurgião e o bem-estar do paciente. Navegar com sucesso por cenários complexos pode ser uma recompensa gratificante, epitomizando a essência da cirurgia. Além disso, os esforços mais amplos de um cirurgião, medidos em operações realizadas e pacientes atendidos, correlacionam-se com a compensação pessoal e o reconhecimento profissional.
À medida que o treinamento cirúrgico evolui, a delicada interação entre prática, trabalho em equipe e as recompensas intrínsecas da cirurgia permanece um alicerce. A jornada para a maestria pode não aderir estritamente à regra das 10.000 horas, mas os princípios de prática deliberada, trabalho em equipe e a natureza gratificante do trabalho cirúrgico persistem como faróis orientadores no domínio da cirurgia. 🌟🔪
“A busca pela maestria cirúrgica é um contínuo equilíbrio entre prática intencional, colaboração e a profunda satisfação de transformar vidas.”
Cirurgia: Uma Sinfonia de Habilidade e Trabalho em Equipe
No intricado domínio da cirurgia, onde anos de treinamento rigoroso moldam as mãos e mentes dos cirurgiões gerais, uma verdade profunda emerge—cirurgia não é um empreendimento solitário. A narrativa transcende a sala de operação, destacando a sinfonia de profissionais dentro do ecossistema de saúde. Enquanto o cirurgião navega pelas complexidades do cuidado ao paciente, um esforço colaborativo se desenrola, semelhante ao funcionamento harmonioso de uma equipe.
Treinamento como um Cadinho para os Fundamentos 🎓⚙️
Enfrentando a árdua jornada da faculdade de medicina e uma exigente residência cirúrgica, o arsenal de um cirurgião é forjado. Conhecimento, destreza técnica e resistência tornam-se os pilares, fortalecendo a base sobre a qual a prática cirúrgica se sustenta. No entanto, o pilar central é o trabalho em equipe, uma realização que surge para todo praticante ao ingressar na dança intricada da prestação de cuidados de saúde.
O Maestro Cirúrgico: A Sabedoria de Pete Carril 🏀📘
Buscando inspiração de uma fonte inesperada, o treinador Pete Carril, o ilustre técnico de basquete da Universidade de Princeton, torna-se um farol de sabedoria. Além da quadra de basquete, os ensinamentos de Carril encapsulam princípios universais aplicáveis à vida e, surpreendentemente, à cirurgia. No volume sucinto, “The Smart Take from the Strong”, co-escrito com Dan White e introduzido pelo venerável Bobby Knight, Carril transmite sabedoria atemporal.
25 Pequenas Coisas: Um Paradigma para a Cirurgia e a Vida 🌐📜
As “25 pequenas coisas a lembrar” do Coach Carril ecoam com relevância não apenas no basquete, mas ressoam nos corredores da cirurgia e da vida. Explorando algumas, como “cada pequena coisa conta”, “você quer ser bom naquelas coisas que acontecem muito” e “a maneira como você pensa afeta o que você vê e faz”, os paralelos com a cirurgia tornam-se surpreendentemente aparentes. A filosofia de Carril torna-se um guia para cirurgiões, enfatizando a importância da atenção aos detalhes, prática e a profunda interação entre pensamento e ação.
Além da Quadra: Cirurgia como um Esporte de Equipe 🤝🔬
Em uma sincronia reminiscente de uma equipe de basquete, o cirurgião harmoniza-se com um coro de profissionais de saúde—enfermeiros, anestesiologistas, equipe de apoio, administradores e mais. A cadência do sucesso é ditada não apenas pela habilidade individual, mas pelo esforço coletivo da equipe. Visão, antecipação e dedicação inabalável convergem, não apenas na quadra de basquete, mas também no teatro da cirurgia.
Enquanto o Coach Carril permanece um espectador silencioso nos sagrados salões de Princeton, testemunhando uma nova geração lutando pela vitória, os cirurgiões também encontram inspiração na busca coletiva pela excelência. Trabalho em equipe, um espírito indomável e um compromisso com o crescimento pessoal e coletivo emergem como os marcos do sucesso, tanto na quadra quanto na sala de operações. 🏀🌟🔪
“A verdadeira maestria cirúrgica não reside apenas nas mãos que operam, mas na harmonia da equipe que, unida, transforma vidas.”
Os Dez Princípios Cirúrgicos
A jornada da vida é um mosaico tecido com fios de orientação de pais, irmãos e mentores. Este artigo transcende o mundano, abraçando a filosofia e o testemunho pessoal na construção de uma carreira cirúrgica triunfante. Revelamos uma lista dos dez principais mandamentos que serve como uma bússola para cirurgiões aspirantes:
Os Dez Princípios Cirúrgicos do Dr. Thirlby 📜🌐
- O Treinamento é Divertido (Você Nunca Vai Esquecê-lo): Um aceno para o aprendizado contínuo, reconhecendo a metamorfose perpétua nas carreiras cirúrgicas.
- Segurança no Emprego: Cirurgiões gerais, vitais e requisitados, encontram posições em diversos cenários, desde centros urbanos movimentados até expansões rurais serenas.
- A Remuneração é Boa: Uma compensação confortável, acima das médias da sociedade, promete estabilidade financeira.
- Sua Mãe Se Orgulhará de Você: Um orgulho familiar ressoa, estendendo-se além das mães para pais, tias e um tapete de familiares.
- Cirurgiões Têm Estilo: Abraçando a personalidade cirúrgica e a cultura única que envolve os reinos cirúrgicos.
- Você Terá Heróis; Você Será um Herói: Cirurgiões, moldados por influenciadores, retribuem tornando-se faróis de esperança para pacientes gratos.
- Existe Espiritualidade, se Você Quiser: As recuperações inexplicáveis, os momentos milagrosos que desafiam as normas estatísticas.
- Você Vai Mudar a Vida dos Pacientes: Uma profunda satisfação pessoal derivada do impacto tangível no destino dos pacientes.
- Pacientes Vão Mudar Sua Vida: Lições diárias dos pacientes promovem humildade, não julgamento e uma jornada contínua para se tornar um ser humano melhor.
- Eu Amo “Dissecar”: Uma reflexão poética da alegria derivada da arte meticulosa dos procedimentos cirúrgicos, executados com precisão para o bem maior.
Os Mandamentos da Vida Cirúrgica 🌌📜
Acrescentando profundidade à narrativa, como mandamentos atemporais, o Dr. James D. Hardy contribui com uma lista que transcende milênios, gravada na versão King James da Bíblia Sagrada.
- Conheça Seu Poder Superior: Uma homenagem ao aspecto espiritual da vida e à santidade do dia de descanso.
- Respeite Suas Raízes: Um reconhecimento da importância dos pais e dos laços familiares.
- Não Faça Mal: Um ethos antigo ressoa através da proibição de ações como assassinato, adultério, roubo, mentir e cobiçar os pertences dos outros.
- Busque a Excelência: Uma busca incessante pelo crescimento pessoal e profissional, incorporando eficiência, excelência e preservação da integridade.
- Prepare-se para a Liderança: Um chamado para formar líderes, enfatizando a importância do crescimento educacional e profissional.
- Cultive Relacionamentos Profissionais: Reconhecendo o valor dos mentores, preservando a sabedoria transmitida através das gerações.
- Lembre-se de Suas Origens: Um eco dos dez mandamentos pessoais do Dr. Hardy, incentivando os indivíduos a honrar sua origem e representá-la com orgulho.
- Valorize a Família: Um lembrete gentil para passar tempo de qualidade com a família, reconhecendo o impacto profundo do amor nos filhos.
- Passe Tempo Sozinho: Defendendo momentos de solidão, promovendo o pensamento criativo e a reflexão pessoal.
- Encontre Alegria em Seu Trabalho: Uma verdade profunda encapsulada na sustentação derivada da busca diária por um trabalho significativo que se gosta genuinamente.
Nesta amalgamação dos dez principais mandamentos do Dr. Thirlby e dos mandamentos do Dr. Hardy, um roteiro se desenrola — um guia não apenas para uma carreira cirúrgica, mas para uma vida plena e com propósito. 🌈🔍🔬
“A verdadeira liderança em cirurgia é esculpida não apenas pelas mãos que operam, mas pelo coração que guia e inspira.”
Safe Cholecystectomy | Bailout Procedures : When and How
Cholecystectomy is a common surgical procedure, with over 750,000 performed annually in the United States and 200,000 in Brazil. Popularized in the early 1990s, laparoscopic cholecystectomy (LC) is now considered the gold standard for routine cases of benign gallbladder and biliary pathology. LC has clear advantages over the traditional open approach, such as lower morbidity, less pain, and faster recovery. However, it is associated with a three to five times increase in bile duct injury (BDI). Major BDI can be a catastrophic complication, significantly increasing mortality. Additionally, patients who suffer a BDI often require further interventions, have a higher risk of additional complications, and experience a reduced quality of life. BDI is a common cause of legal litigation and remains one of the most frequent reasons for monetary compensation.
Correct Anatomical Identification The “classic injury” to the bile duct occurs when the common bile duct is mistaken for the cystic duct. This typically happens in the setting of severe acute or chronic inflammation, where the gallbladder may fuse to the lateral wall of the common hepatic duct, predisposing the surgeon to misidentify the biliary anatomy. This can result in a major BDI, where a segment of the common hepatic duct and bile duct is removed. Beyond this classic injury, other injuries to the biliary system can occur, such as sectional or segmental ducts disconnected from the liver with or without bile leakage, bile leakage from the cystic duct stump, long-term strictures due to thermal or iatrogenic damage, or combined vasculobiliary injuries.
Critical View of Safety (CVS) The Critical View of Safety (CVS), introduced by Strasberg et al. in 1995, is a method of safe anatomical identification that serves as a set of criteria to ensure the proper identification of the appropriate anatomy before ductal structures are ligated. These criteria include separating the lower end of the gallbladder from the liver to expose at least the lower third of the cystic plate, cleaning all fibrous and fatty tissue within the hepatocystic triangle, and seeing only two structures entering the gallbladder. The CVS mirrors the safe identification that occurs in traditional open cholecystectomy. While there are no level 1 data to support its use (due to the large sample size required to discriminate between an injury that occurs at a relatively low incidence), there is a body of literature of over 6000 cases where CVS was achieved without any major BDI.
Culture of Safety in Cholecystectomy (COSIC) Strict adherence to CVS is crucial to reducing BDI, but it is only part of the Culture of Safety in Cholecystectomy (COSIC), which requires that safety be at the forefront. Besides achieving CVS in total cholecystectomy cases, COSIC also requires proper patient selection and evaluation, adjustment of surgical technique in non-routine cases, use of bailout procedures, and avoiding complex cases when appropriate expertise is unavailable. The American Society of Gastrointestinal and Endoscopic Surgeons (SAGES) has developed a six-step program to enhance cholecystectomy safety:
- Understanding CVS and using it for identifying the cystic duct and artery.
- Considering an intraoperative pause before clipping or cutting any structure.
- Understanding aberrant anatomy.
- Liberal use of cholangiography or other intraoperative imaging means of the biliary system.
- Recognizing when dissection is approaching a significant danger zone and terminating the operation by a safe method, other than cholecystectomy, if the conditions around the gallbladder are too dangerous.
- Seeking assistance from another surgeon when conditions are difficult.
Bailout Procedures: When and How to Opt Deciding when to stop dissection of the hepatocystic triangle and opt for a bailout procedure rather than total cholecystectomy can be challenging. To make this decision before any biliary or vascular injury occurs, the surgeon must constantly ask: “Is it possible to safely achieve CVS?” When the answer is “No” or “I am not sure,” we recommend considering a bailout procedure. Early adoption of a bailout procedure is believed to reduce the difficulty of making this decision and avoid inadvertent injuries to the biliary system while trying to dissect in difficult and obstructed planes. It is essential always to remember that this operation is performed for benign pathology.
There are three clear bailout options in difficult cases:
- Stop the Operation (Stop, Drain, and Refer): Stopping the operation may conflict with the surgeon’s goal of “solving a problem,” but it should be considered and is a viable and safe option to avoid BDI. The patient should continue with a short course of antibiotics or even undergo postoperative drain placement and/or percutaneous cholecystostomy. A second attempt at cholecystectomy can be considered in 2–3 months.
- Surgical Cholecystostomy: The gallbladder’s fundus can be opened after placing a purse-string suture, the contents are aspirated, and a drainage catheter is placed in the gallbladder lumen. This method works as a temporary measure since definitive cholecystectomy will likely be necessary in 2–3 months.
- Subtotal “Fenestrating” Cholecystectomy: Subtotal cholecystectomy has been a surgical option for over 100 years. In 2016, an attempt was made to define subtotal cholecystectomy into two distinct subtypes to allow for improved study and dissemination of the technique. When a new gallbladder remnant is created, this is called “reconstituting” subtotal cholecystectomy. When the gallbladder is left open with a remaining portion, this is called “fenestrating” subtotal cholecystectomy. Recent systematic reviews have demonstrated the safety of these procedures. Fenestrating subtotal cholecystectomy is recommended as the most definitive bailout procedure.
Once the decision is made to proceed with fenestrating subtotal cholecystectomy, the surgeon should consider their experience and either convert to an open procedure or continue laparoscopically. This procedure can be safely performed laparoscopically with minimal “advanced” laparoscopic maneuvers, but it can also be easily performed using an open technique.
Fenestrating Subtotal Cholecystectomy Procedure The first step involves incising the anterior (peritonealized) wall of the gallbladder at the fundus. By initially leaving the gallbladder body intact, its contents can be evacuated more easily. It may be advisable to place a surgical sponge or “endobag” under the gallbladder to facilitate catching any stones that might spill upon opening. The incision should continue towards the infundibulum, removing most of the anterior wall of the gallbladder. A very important consideration of this technique involves leaving a portion of the anterior infundibulum wall intact to avoid inadvertent entry into the hepatoduodenal ligament. Once most of the anterior wall is removed and the gallbladder contents, including all stones, are evacuated, the internal aspect of the gallbladder can be examined. It is essential to identify whether continuous biliary drainage from the gallbladder is present. In most “difficult” gallbladders requiring fenestrating subtotal cholecystectomy, the cystic duct is obliterated and does not require formal ligation. However, in the rare instances where the duct is patent and bile continues to drain from it, the internal orifice of the cystic duct should be closed with non-permanent sutures from the internal aspect of the gallbladder. At no point should external ligation of the cystic duct be attempted, which could potentially injure the bile duct. A drain should be left in the hepatorenal recess. No drain is needed inside the gallbladder lumen. The drain should be monitored for biliary drainage. Although generally rare, if a postoperative biliary fistula occurs, standard management should proceed. Routine postoperative endoscopic sphincterotomy is not recommended unless the biliary fistula is persistent, as most of them are self-limiting.
The main goal of laparoscopic cholecystectomy is “safety first, total cholecystectomy second.” While most laparoscopic cholecystectomies are straightforward, the surgeon must always keep this safety culture at the forefront and remain vigilant to anticipate dangerous situations. COSIC will help minimize (or eliminate) BDI and assist the surgeon in managing difficult operating conditions or clinical scenarios. Safe management of the difficult gallbladder is possible with operational adjustments and liberal use of bailout procedures, specifically fenestrating subtotal cholecystectomy.
Colecistectomia Segura: Quando e Como realizar procedimentos de Resgate | Colecistectomia Subtotal
A colecistectomia é um procedimento cirúrgico comum, com mais de 750.000 realizadas anualmente nos Estados Unidos e 200.000 no Brasil. Popularizada no início dos anos 1990, a colecistectomia laparoscópica (CL) é agora considerada o padrão-ouro para casos rotineiros de patologia benigna da vesícula biliar e biliar. A CL tem vantagens claras sobre a abordagem aberta tradicional, como menor morbidade, menos dor e recuperação mais rápida. No entanto, está associada a um aumento de três a cinco vezes na lesão do ducto biliar (LDB). A LDB maior pode ser uma complicação catastrófica, aumentando claramente a mortalidade. Além disso, pacientes que sofrem uma LDB geralmente precisam de intervenções adicionais, têm maior risco de complicações adicionais e sofrem redução na qualidade de vida. A LDB é uma causa comum de litígios legais e continua sendo uma das razões mais comuns para indenizações monetários.
Identificação Anatômica Correta
A “lesão clássica” do ducto biliar ocorre quando o ducto biliar comum é confundido com o ducto cístico. Geralmente, isso ocorre em um cenário de inflamação aguda ou crônica severa, onde a vesícula biliar pode se fundir à parede lateral do ducto hepático comum, predispondo o cirurgião a identificar erroneamente a anatomia biliar. Isso pode resultar em uma LDB maior, onde um segmento do ducto hepático comum e do ducto biliar é removido. Além dessa lesão clássica, outras lesões do sistema biliar podem ocorrer, como ductos seccionais ou segmentares desconectados do fígado com ou sem vazamento biliar, vazamento biliar do coto do ducto cístico, estenoses de longo prazo por danos térmicos ou iatrogênicos, ou lesões vasculobiliares combinadas.
Visão Crítica de Segurança (CVS)
A visão crítica de segurança (CVS), introduzida por Strasberg et al. em 1995, é um método de identificação anatômica segura que serve como um conjunto de critérios para garantir a identificação adequada da anatomia apropriada antes da ligadura de estruturas ductais. Esses critérios incluem a separação da extremidade inferior da vesícula biliar do fígado para expor pelo menos o terço inferior da placa cística, todos os tecidos fibrosos e adiposos limpos dentro do triângulo hepatocístico e apenas duas estruturas vistas entrando na vesícula biliar. A CVS imita a identificação segura que ocorre na colecistectomia aberta tradicional. Embora não existam dados de nível 1 para apoiar seu uso (devido ao grande tamanho da amostra necessário para discriminar entre uma lesão que ocorre com uma incidência relativamente baixa), há um corpo de literatura de mais de 6000 casos onde a CVS foi alcançada sem nenhuma LDB maior.
Cultura de Segurança em Colecistectomia (COSIC)
Embora a adesão estrita à CVS seja importante para diminuir a LDB, ela é apenas uma parte da Cultura de Segurança em Colecistectomia (COSIC), que exige que a segurança esteja na vanguarda. Além de alcançar a CVS em casos de colecistectomia total, a COSIC também requer seleção e avaliação adequadas do paciente, ajuste da técnica cirúrgica em casos não rotineiros, uso de procedimentos de resgate e evitar casos complexos quando a experiência apropriada não estiver disponível. A Sociedade Americana de Cirurgiões Gastrointestinais e Endoscópicos (SAGES) desenvolveu um programa de seis etapas para aumentar a segurança da colecistectomia:
- Compreender a CVS e usá-la para identificação do ducto cístico e da artéria.
- Considerar uma pausa intraoperatória antes de prender ou cortar qualquer estrutura.
- Compreender a anatomia aberrante.
- Uso liberal de colangiografia ou outros meios de imagem intraoperatória do sistema biliar.
- Reconhecer quando a dissecção está se aproximando de uma zona de risco significativo e terminar a operação por um método seguro, além da colecistectomia, se as condições ao redor da vesícula biliar forem muito perigosas.
- Buscar ajuda de outro cirurgião quando as condições forem difíceis.
Procedimentos de Resgate: Quando e Como Optar
Decidir quando interromper a dissecção do triângulo hepatocístico e optar por um procedimento de resgate em vez da colecistectomia total pode ser desafiador. Para tomar essa decisão antes que ocorra qualquer lesão biliar ou vascular, o cirurgião precisa constantemente se perguntar: “É possível alcançar a CVS com segurança?” Quando a resposta for “Não” ou “Não tenho certeza”, recomendamos considerar um procedimento de resgate. Acreditamos que a adoção precoce de um procedimento de resgate diminuirá a dificuldade de tomar essa decisão e evitará lesões inadvertidas ao sistema biliar ao tentar dissecar em planos difíceis e obstruídos. É importante sempre lembrar que esta operação é feita para patologia benigna.
Existem três opções claras de resgate em casos difíceis:
- Interromper a Operação (Parar, Drenar e Encaminhar):
- Parar a operação pode atuar em tensão com o objetivo do cirurgião de “resolver um problema”, mas deve ser considerado e é uma opção viável e segura para evitar a LDB. O paciente deve continuar com um curso curto de antibióticos ou até mesmo ser submetido à colocação de um dreno e/ou de colecistostomia percutânea pós-operatória. Uma segunda tentativa de colecistectomia pode ser considerada em 2–3 meses.
- Colecistostomia Cirúrgica:
- O fundo da vesícula biliar pode ser aberto após a colocação de uma sutura em “bolsa de tabaco”, o conteúdo é aspirado e um cateter de drenagem é colocado na luz da vesícula biliar. Este método funciona como uma medida temporária, pois a colecistectomia definitiva provavelmente será necessária em 2–3 meses.
- Colecistectomia Subtotal “Fenestrante”:
- A colecistectomia subtotal tem sido uma opção cirúrgica por mais de 100 anos. Em 2016, foi feita uma tentativa de definir a colecistectomia subtotal em dois subtipos distintos para permitir um estudo e disseminação melhorados da técnica. Quando um novo remanescente da vesícula biliar é criado, isso é chamado de colecistectomia subtotal “reconstituinte”. Quando a vesícula biliar é deixada aberta com uma porção restante, isso é chamado de colecistectomia subtotal “fenestrante”. Recentes revisões sistemáticas demonstraram a segurança desses procedimentos. Recomenda-se a colecistectomia subtotal fenestrante como o procedimento de resgate mais definitivo.
Uma vez que a decisão é tomada para proceder com a colecistectomia subtotal fenestrante, o cirurgião deve considerar sua experiência e se converter para um procedimento aberto ou continuar laparoscopicamente. Acreditamos que esse procedimento pode ser realizado com segurança laparoscopicamente com manobras laparoscópicas mínimas “avançadas”; no entanto, também pode ser realizado facilmente usando uma técnica aberta.
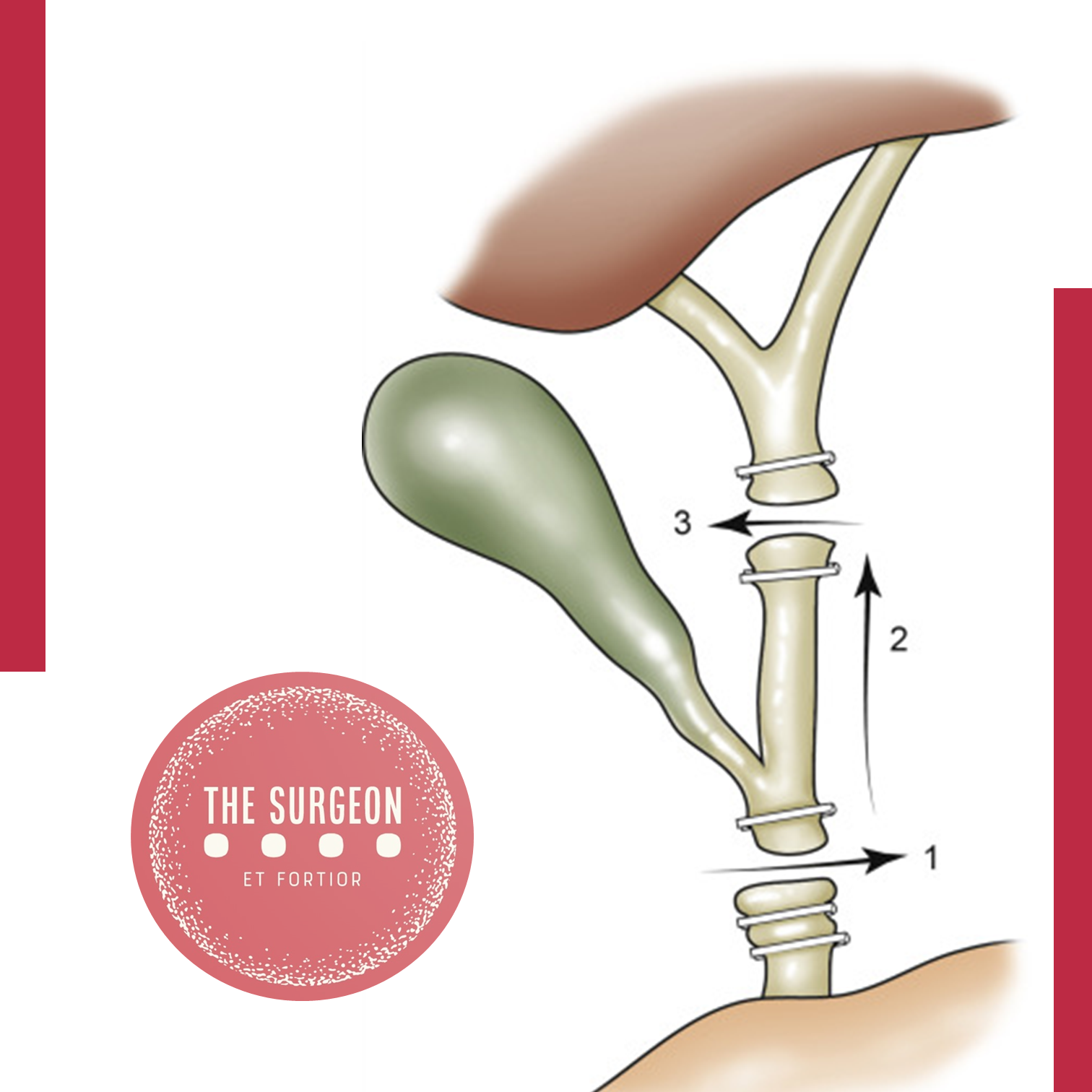
Procedimento de Colecistectomia Subtotal “Fenestrante”
O primeiro passo envolve a incisão da parede anterior (peritonealizada) da vesícula biliar no fundo. Ao deixar o corpo da vesícula biliar intacto inicialmente, o conteúdo da vesícula biliar pode ser evacuado mais facilmente. Pode ser aconselhável colocar uma esponja cirúrgica ou “endobag” sob a vesícula biliar para facilitar a captura de quaisquer pedras que possam ser derramadas ao abri-la. A incisão deve ser continuada em direção ao infundíbulo, removendo a maior parte da parede anterior da vesícula biliar. Uma consideração muito importante dessa técnica envolve deixar uma porção da parede anterior do infundíbulo intacta para evitar a entrada inadvertida no ligamento hepatoduodenal. Uma vez que a maior parte da parede anterior é removida e o conteúdo da vesícula biliar, incluindo todas as pedras, são evacuados, o aspecto interno da vesícula biliar pode ser examinado. É importante identificar se há ou não drenagem biliar contínua da vesícula biliar. Observa-se que na maioria das vesículas biliares “difíceis” que requerem colecistectomia subtotal fenestrante, o ducto cístico está obliterado e não requer ligadura formal. No entanto, nas raras instâncias em que o ducto está patente e a bile continua a drenar dele, o orifício interno do ducto cístico deve ser fechado com sutura não permanente do aspecto interno da vesícula biliar. Em nenhum momento deve ser tentada a ligadura externa do ducto cístico, o que poderia potencialmente lesionar o ducto biliar. Um dreno deve ser deixado no recessus hepatorenal. Nenhum dreno é necessário dentro da luz da vesícula biliar. O dreno deve ser monitorado para drenagem biliar. Embora geralmente rara, se ocorrer uma fístula biliar pós-operatória, o manejo padrão deve prosseguir. Não se recomenda a esfincterotomia endoscópica pós-operatória de rotina, a menos que a fístula biliar seja persistente, pois a maioria delas é autolimitada.

A meta principal da colecistectomia laparoscópica é “segurança em primeiro lugar, colecistectomia total em segundo”. Embora a maioria das colecistectomias laparoscópicas realizadas sejam diretas, o cirurgião deve sempre manter essa cultura de segurança na vanguarda e permanecer vigilante para se antecipar a situações perigosas. A COSIC ajudará a minimizar (ou eliminar) a LDB e ajudará o cirurgião a manejar condições operatórias difíceis ou cenários clínicos. O manejo seguro da vesícula biliar difícil é possível com ajustes operacionais e uso liberal de procedimentos de resgate, especificamente a colecistectomia subtotal fenestrante.
SAFE laparoscopic cholecystectomy
The CVS technique, which was first described by Strasberg et al. in 1995, was introduced to reduce the risk of bile duct injury. A recent Society of American Gastrointestinal and Endoscopic Surgeons (SAGES) expert Delphi consensus deemed the CVS as being the most important factor for overall safety.
Nowadays, the CVS technique is the gold standard to perform a safe cholecystectomy with identification of the vital structures such as the cystic duct.The reviewed literature suggests that judicious establishment of CVS could decrease bile duct injury rate, from an average 0.4% to nearly 0%.
To establish CVS, two windows need to be created during dissection of Calot’s triangle: one window between the cystic artery, cystic duct, and gallbladder, and another one between the cystic artery, gallbladder, and liver. The CVS technique is aimed especially at mobilizing the gallbladder neck from the liver in the appropriate cystic plate to obtain a circumferential identification of the cystic duct and its transition into the gallbladder.
The guiding structure for dissection should be the wall of the gallbladder. Proper retraction of the fundus cephalad and of the infundibulum posteriorly and laterally is necessary, and tenting by excessive lateral pulling on the gallbladder should be avoided. Cephalad traction on the fundus compresses Calot’s triangle, while lateral traction on Hartmann’s pouch tents up the CBD, which may then be mistaken for the cystic duct, especially when that duct is very short. The cystic duct should be dissected in a retrograde fashion, starting at gallbladder proceeding with the identification of the cystic duct–gallbladder junction on both sides and the visualization of the cystic duct–common bile duct junction prior to clipping.
Calot’s triangle should be dissected from all fibrous and fatty tissues. At the end of the dissection, only the cystic duct and artery cystica should enter the gallbladder and the bottom of the liver bed should be visible. The CBD is not necessary to be exposed. Failure to achieve the CVS is an absolute indication for conversion or additional bile duct imaging. The CVS should be described in the operative report.
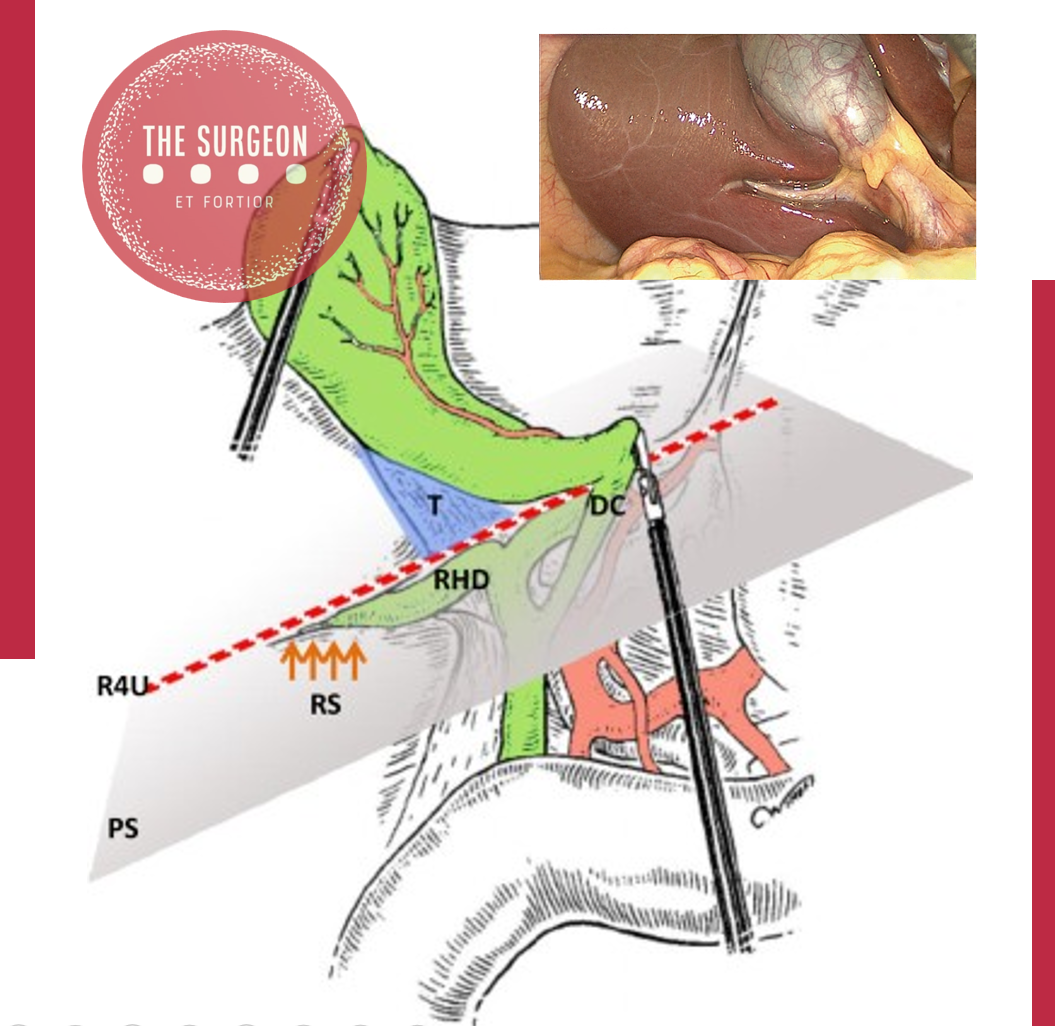
Connor et al. and Wakabayashi et al. elegantly describe five key initial steps in performing safe laparoscopic cholecystectomy: (1) retract the gallbladder laterally to a 10 o’clock position relative to the principle plane of the liver (Cantlie’s line); (2) confirm Hartmann’s pouch is retracted up and towards segment IV; (3) identify Rouviere’s sulcus which marks the level of the right posterior portal pedicle and is identifiable in >80% of the patients. An imaginary line (R4U) drawn along the sulcus and carried across to the base of segment IV shows the level ventral to which dissection is “safe” and dorsal to which it is not; (4) dissect the posterior peritoneum of the hepatobiliary or hepatocystic triangle; and (5) confirm the critical view is obtained.
Preventive strategies and safe surgery are of utmost importance to minimize BDI during laparoscopic cholecystectomy. Although many methods used in the prevention of BDI have demonstrated promising results, there is no consensus regarding a systematic reporting system of BDI. Currently, CVS seems to be the cornerstone for a safe laparoscopic cholecystectomy. In difficult cases, a sufficient attention to alternative techniques should be apprehended. In such cases, intraoperative imaging may delineate the biliary anatomy.
Prevenção de Lesão da Via Biliar durante a Colecistectomia
A colecistectomia laparoscópica tornou-se o padrão ouro para o tratamento da colelitíase sintomática e outras doenças da vesícula biliar. No entanto, a incidência de lesões da via biliar (LVB) aumentou de 0,2–0,3% na era da colecistectomia aberta convencional para 0,5–0,8% na era da colecistectomia laparoscópica. Essas lesões são frequentemente associadas a significativa morbidade e mortalidade pós-operatória, reduzida qualidade de vida a longo prazo e representam um desafio cirúrgico considerável. A prevenção dessas lesões deve ser o principal objetivo, exigindo adesão a princípios rigorosos de dissecação meticulosa e segura das estruturas identificadas.
Causas e Fatores de Risco para Lesões da Via Biliar
As lesões da via biliar podem ocorrer devido à dissecação incorreta ou incompleta do triângulo de Calot, especialmente em casos de inflamação significativa no local cirúrgico ou anatomia aberrante do ducto biliar. Outros fatores que aumentam a incidência de LVB incluem:
- Inexperiência do Cirurgião: A “curva de aprendizado” inicial contribuiu para a alta taxa de lesões biliares nos primeiros relatos.
- Inflamação e Cicatrizes: Inflamação aguda ou crônica e cicatrizes densas podem obscurecer a anatomia normal e aumentar a dificuldade do procedimento.
- Obesidade: A presença de tecido adiposo abundante ao redor do ligamento hepatoduodenal aumenta a dificuldade cirúrgica e promove lesões biliares.
- Anatomia Aberrante: Variações anatômicas, como um ducto hepático direito aberrante, podem ser erroneamente identificadas como ducto cístico e ligadas ou cortadas.
- Uso Excessivo de Energia: O uso excessivo de dispositivos de energia, como eletrocautério, pode levar a lesões térmicas e isquemia do ducto biliar.
- Fatores Adversos: Idade avançada, gênero masculino, obesidade mórbida, longa duração dos sintomas antes da cirurgia, cirurgias abdominais superiores prévias e inflamação aguda contribuem para o aumento do risco.
Princípios Técnicos para Prevenção de Lesões da Via Biliar
Para prevenir lesões durante a colecistectomia laparoscópica, os cirurgiões devem seguir princípios técnicos essenciais:
- Visão Crítica de Segurança (CVS): A técnica CVS, descrita por Strasberg et al., é fundamental para a identificação segura das estruturas vitais, como o ducto cístico. Dois espaços devem ser criados durante a dissecação do triângulo de Calot para identificar circunferencialmente o ducto cístico e sua transição para a vesícula biliar.
- Dissecação Meticulosa do Triângulo de Calot: A limpeza do triângulo hepatocístico de gordura e tecidos fibrosos, e a separação do terço inferior da vesícula biliar do fígado para expor a placa cística são passos cruciais.
- Uso Judicioso de Dispositivos de Energia: Os dispositivos de energia devem ser usados com cautela no triângulo de Calot, com configurações de baixa potência e coagulação de pequenos pedaços de tecido por vez.
- Reconhecimento de Dissecção Insegura: O cirurgião deve ser capaz de reconhecer quando a dissecção se torna insegura, com alto potencial para LVB, e estar preparado para buscar alternativas técnicas, pedir uma segunda opinião ou converter para uma colecistectomia aberta.
- Imagens Intraoperatórias: Técnicas como colangiografia intraoperatória, ultrassonografia laparoscópica e colangiografia por fluorescência de infravermelho próximo podem ser usadas para avaliar a anatomia biliar.
Procedimentos de Resgate e Conversão
Em casos onde a CVS não pode ser alcançada e as estratégias de resgate não podem ser implementadas, não hesite em converter para uma colecistectomia aberta. Procedimentos de resgate, como colecistectomia subtotal ou colecistectomia iniciada pelo fundo, podem ser necessários em casos de inflamação severa e/ou incapacidade de realizar a CVS.
Avaliação Pré-operatória e Planejamento
A avaliação pré-operatória de preditores de colecistectomia difícil é crucial. Fatores como gênero masculino, obesidade, idade avançada, histórico de ataques de cólica biliar, intervalo prolongado entre o início e a apresentação dos sintomas, cirurgias abdominais superiores prévias e cirrose devem ser identificados. A seleção cuidadosa de pacientes e a preparação para a possibilidade de conversão para cirurgia aberta são essenciais para a segurança do procedimento.
Conclusão
A prevenção de lesões da via biliar durante a colecistectomia laparoscópica exige uma abordagem meticulosa, conhecimento anatômico detalhado e a aplicação de técnicas cirúrgicas refinadas. A adesão à técnica CVS, uso cauteloso de dispositivos de energia e a prontidão para procedimentos de resgate ou conversão são fundamentais para minimizar riscos e melhorar os resultados dos pacientes. A experiência do cirurgião e a colaboração da equipe cirúrgica são fatores críticos para a execução segura desta operação comum, mas potencialmente desafiadora.
Mechanisms of Bile Duct Injury
Mechanism of Bile Duct Injury: Understanding the Risks in Laparoscopic Cholecystectomy
Introduction
Laparoscopic cholecystectomy, the “gold standard” for treating symptomatic gallbladder disease, has transformed surgical practice since its introduction in the early 1990s. Despite its widespread adoption and the improved safety profile over time, the procedure remains fraught with risks, particularly bile duct injuries (BDIs). The incidence of BDIs during laparoscopic cholecystectomy has declined from its peak, but this complication still represents a significant challenge in digestive surgery, leading to substantial morbidity, mortality, and legal consequences. In Brazil, where an estimated 300,000 cholecystectomies are performed annually, BDIs continue to be a significant concern. This article delves into the mechanisms of bile duct injuries during laparoscopic cholecystectomy, exploring the factors that contribute to these adverse events and their implications for surgical practice.
Development of the Theme
The advent of laparoscopic cholecystectomy marked a turning point in the management of gallbladder disease, offering patients reduced postoperative pain, shorter hospital stays, and faster recovery times. However, the initial enthusiasm for this minimally invasive approach was tempered by a notable increase in bile duct injuries. As surgeons adapted to the new technique, the incidence of BDIs spiked, with early reports indicating injury rates as high as 0.7%. Today, with increased experience and refined techniques, the incidence has decreased to approximately 0.1% to 0.2%. Despite these improvements, the risk remains significant, with estimates suggesting that one in three general surgeons will cause a bile duct injury at some point in their careers.

Iatrogenic bile duct injuries are most often the result of perceptual errors in identifying biliary anatomy during surgery. The most common injury involves a complete transection of the common bile duct, which is also the most difficult to manage. Typically, excessive cephalad retraction of the gallbladder fundus or insufficient lateral retraction on the infundibulum leads to an alignment of the cystic and common bile ducts, causing the common bile duct to be mistaken for the cystic duct. This misidentification results in clipping and transecting the common bile duct—a scenario that can lead to devastating outcomes if not promptly recognized and appropriately managed.
Inflammatory conditions, such as acute or chronic cholecystitis, further complicate the surgical landscape. Thickened and friable tissue, along with adhesions, can obscure normal anatomical landmarks, increasing the difficulty of the procedure. Aberrant biliary anatomy, such as a low-lying right hepatic duct, poses additional risks, as these anatomical variations can be easily overlooked during surgery, leading to unintended ductal injury.
Energy sources used for hemostasis, such as electrocautery, introduce another layer of complexity. Excessive or inappropriate use of these tools can damage the bile duct or its blood supply, resulting in stricture formation or bile leaks. Another common mechanism of injury occurs when a clip is inadvertently placed across the common bile duct, often in a hurried attempt to control bleeding from the hilum without a clear view of the anatomy.
In the context of laparoscopic cholecystectomy, BDIs are particularly perilous when the common bile duct is mistaken for the cystic duct. This classical injury pattern, first described by Davidoff and colleagues, typically involves clipping and dividing the common bile duct, with further proximal dissection leading to injury of the right hepatic artery and more proximal ductal structures, including the common hepatic duct and intrahepatic ducts. Poor visualization due to inadequate illumination, excessive smoke, or intraoperative bleeding exacerbates these risks, making meticulous surgical technique and optimal visualization crucial to avoiding these injuries.
Key Points
- Perceptual Errors: The primary mechanism of bile duct injury during laparoscopic cholecystectomy is the misidentification of biliary anatomy, particularly the confusion between the cystic and common bile ducts.
- Risk Factors: Inflammatory conditions, aberrant anatomy, and excessive use of energy devices significantly increase the risk of bile duct injuries.
- Incidence: Despite advancements in technique, bile duct injuries remain a significant concern, with a 0.1% to 0.2% incidence in laparoscopic cholecystectomy. In Brazil, the annual rate of cholecystectomies underscores the importance of vigilance in preventing these injuries.
- Complications: Bile duct injuries can lead to severe complications, including biliary stricture, leakage, infection, and even death. The financial and legal implications further highlight the need for preventive measures.
Conclusion
Understanding the mechanisms of bile duct injury during laparoscopic cholecystectomy is crucial for improving surgical outcomes and minimizing patient morbidity. Surgeons must remain vigilant in identifying biliary anatomy, particularly in the presence of risk factors such as inflammation and aberrant anatomy. Enhanced visualization techniques, careful dissection, and judicious use of energy devices are essential strategies to reduce the incidence of BDIs. As the field of minimally invasive surgery continues to evolve, ongoing education and training in these areas are paramount to ensuring patient safety and improving the quality of care.
In the words of Alexis Carrel, “There is no such thing as minor surgery, but there are many minor surgeons”. This sentiment is particularly relevant to the surgical treatment of biliary diseases, where the combination of skill, experience, and compassion is vital to patient outcomes.
Did you like it? Leave us a comment ✍️, share on your social networks, and | or send your question via 💬 Online Chat in our Instagram DM.
LaparoscopicCholecystectomy #BileDuctInjury #SurgicalComplications #DigestiveSurgery #SurgicalEducation
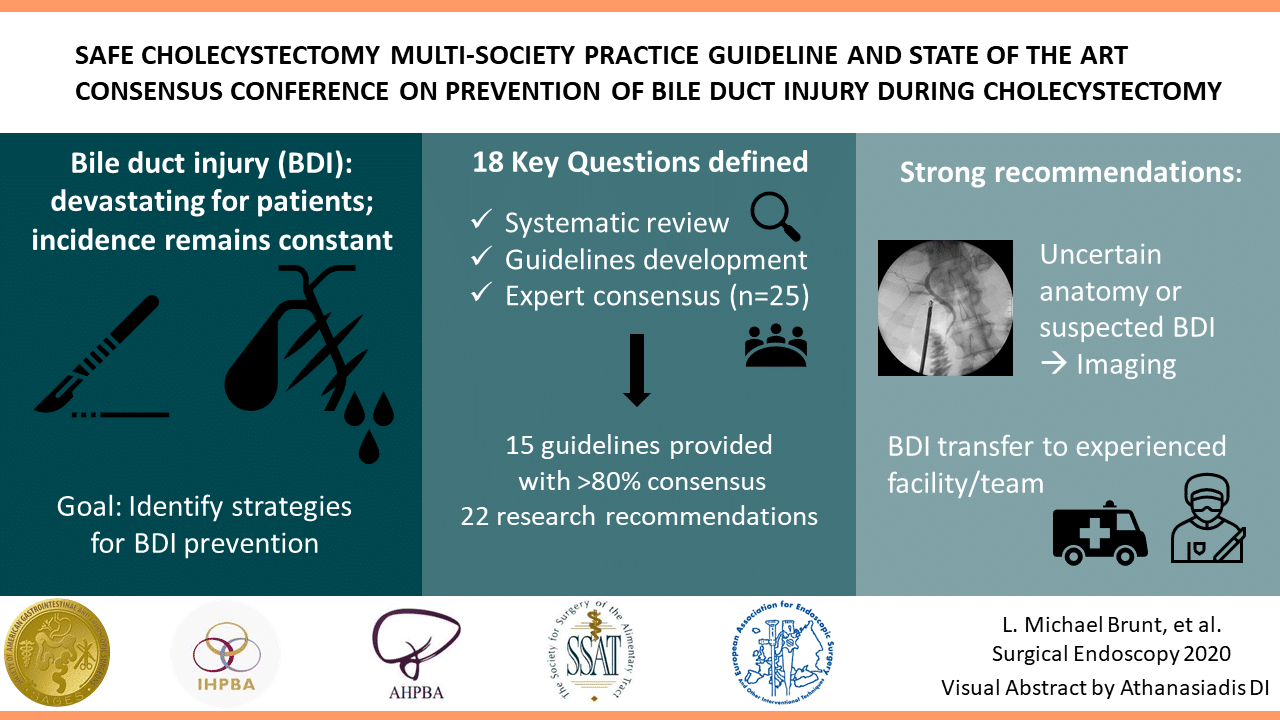
Prevention of Bile Duct Injury
Prevention of Bile Duct Injury During Laparoscopic Cholecystectomy
Introduction
Bile duct injury (BDI) during laparoscopic cholecystectomy is a significant surgical complication with profound clinical and medico-legal implications. The incidence of BDI ranges from 0.3% to 0.6%, despite advances in surgical techniques and imaging modalities. The prevalence of BDI remains concerning due to its association with high morbidity and mortality rates. Patients who suffer from BDI often face prolonged hospital stays, multiple surgeries, and long-term complications such as bile leakage, strictures, and secondary biliary cirrhosis. Medico-legally, BDI is one of the most common reasons for litigation against surgeons, often resulting in significant financial settlements and professional repercussions.
Questions and Answers
Question 1: What technique should be used to identify the anatomy during laparoscopic cholecystectomy?
Answer: The Critical View of Safety (CVS) is recommended for identifying the cystic duct and cystic artery.
Key Findings: The incidence of BDI was found to be 2 in one million cases using CVS, compared to 1.5 per 1000 cases with the infundibular technique.
Question 2: When should intraoperative cholangiography (IOC) be used?
Answer: IOC should be used in cases of anatomical uncertainty or suspicion of bile duct injury.
Key Findings: IOC aids in the prevention and immediate management of BDI by providing a precise assessment of biliary anatomy during surgery.
Question 3: What are the recommendations for managing patients with confirmed or suspected bile duct injury?
Answer: Patients with confirmed or suspected BDI should be referred to an experienced surgeon or a multidisciplinary hepatobiliary team.
Key Findings: Early referral to hepatobiliary specialists is associated with better long-term outcomes and lower complication rates.
Question 4: Should the “fundus-first” technique be used when CVS cannot be achieved?
Answer: Yes, the “fundus-first” technique is recommended when CVS cannot be achieved.
Key Findings: This technique is effective for safely dissecting the gallbladder in complex cases where anatomy is unclear.
Question 5: Should CVS be documented during laparoscopic cholecystectomy?
Answer: Yes, documenting CVS with double-static photographs is recommended.
Key Findings: Photographic documentation of CVS ensures correct anatomical identification and serves as a record for later review in case of complications.
Question 6: Should near-infrared biliary imaging be used intraoperatively?
Answer: The evidence for near-infrared biliary imaging is limited; thus, IOC is preferred.
Key Findings: IOC is more widely studied and proven effective in preventing BDI compared to near-infrared imaging.
Question 7: Should surgical risk stratification be used to mitigate the risk of BDI?
Answer: Yes, surgical risk stratification is recommended.
Key Findings: Risk stratification helps identify patients at higher risk of complications, aiding in surgical planning and decision-making.
Question 8: Should the presence of cholecystolithiasis be considered in risk stratification?
Answer: Yes, the presence of cholecystolithiasis should be considered in risk stratification.
Key Findings: Patients with cholecystolithiasis have a higher risk of complications during cholecystectomy, making it important to include this condition in risk assessments.
Question 9: Should immediate cholecystectomy be performed in cases of acute cholecystitis?
Answer: Yes, immediate cholecystectomy within 72 hours is recommended.
Key Findings: Surgery within 72 hours of the onset of acute cholecystitis symptoms is associated with lower complication rates and better patient recovery.
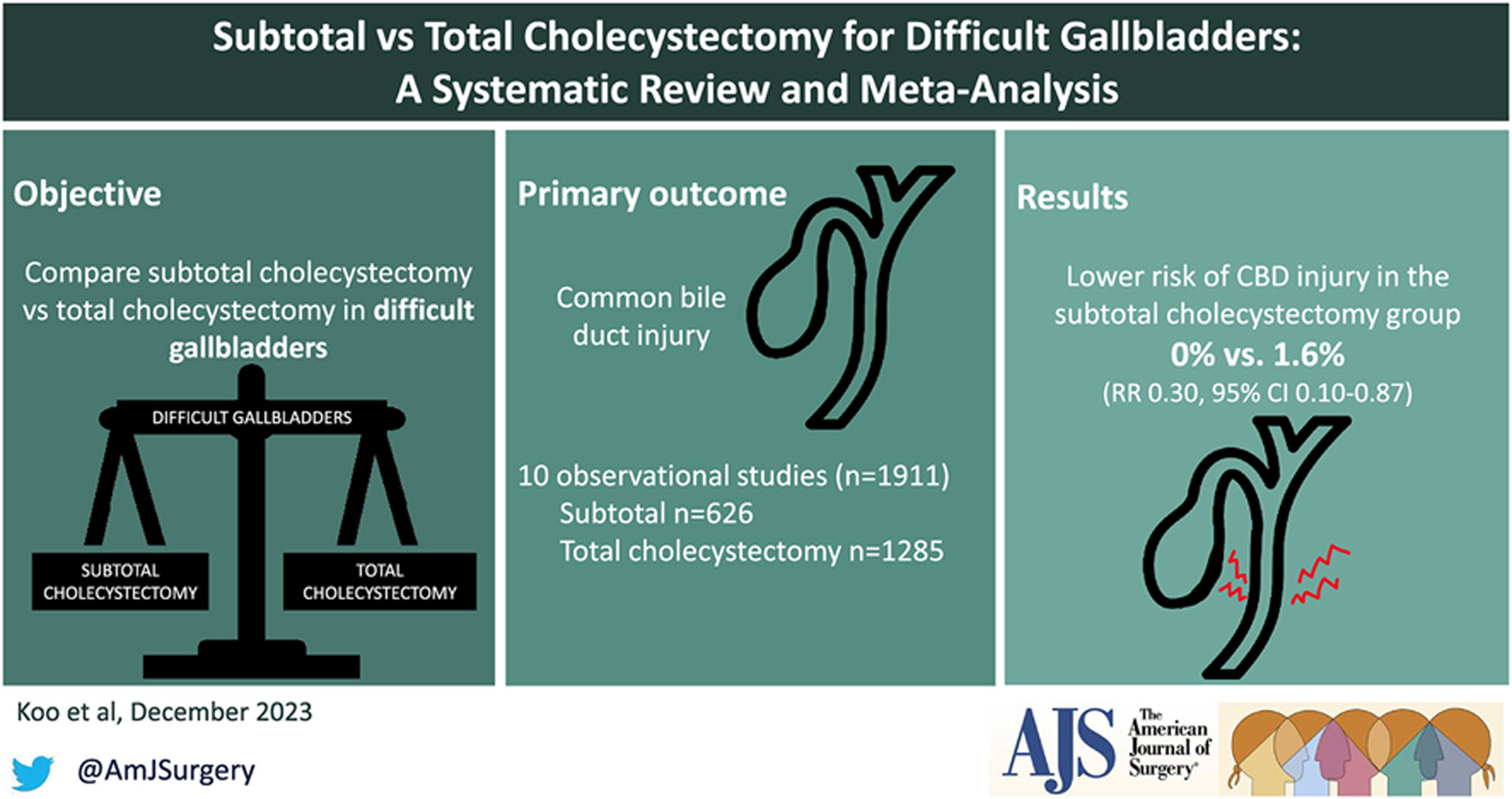
Question 10: Should subtotal cholecystectomy be performed in cases of severe inflammation?
Answer: Yes, subtotal cholecystectomy is recommended in cases of severe inflammation where CVS cannot be obtained.
Key Findings: In severe inflammation scenarios, subtotal cholecystectomy can facilitate the surgery and reduce the risk of BDI.
Question 11: Which approach is preferable, four-port laparoscopic cholecystectomy or reduced-port/single-incision?
Answer: Four-port laparoscopic cholecystectomy is recommended as the standard approach.
Key Findings: The four-port technique is the most studied, showing effectiveness and safety in performing cholecystectomies with lower complication risks.
Question 12: Should interval cholecystectomy be performed following percutaneous cholecystostomy?
Answer: Yes, interval cholecystectomy is recommended after initial stabilization with percutaneous cholecystostomy.
Key Findings: Interval cholecystectomy offers better long-term outcomes and lower risk of recurrent complications compared to no additional treatment.
Question 13: Should laparoscopic cholecystectomy be converted to open in difficult cases?
Answer: Yes, conversion to open surgery is recommended in cases of significant difficulty.
Key Findings: Conversion to open surgery can prevent BDI in situations where laparoscopic dissection is extremely difficult or risky.
Question 14: Should a waiting time be implemented to verify CVS?
Answer: Yes, a waiting time to verify CVS is recommended.
Key Findings: A waiting time allows better anatomical evaluation before proceeding with dissection, reducing the risk of BDI.
Question 15: Should two surgeons be used in complex cases?
Answer: The presence of two surgeons can be beneficial in complex cases, although strong recommendations are not made due to limited evidence.
Key Findings: Some studies suggest that collaboration between two surgeons can improve anatomical identification and reduce complications in difficult cases.
Question 16: Should surgeons receive coaching on CVS to limit the risk or severity of BDI?
Answer: Yes, surgeons should receive coaching on CVS.
Key Findings: Surgeons who receive targeted coaching on CVS show improved anatomical identification and reduced rates of BDI.
Question 17: Should simulation or video-based education be used to train surgeons?
Answer: Yes, simulation or video-based education should be used.
Key Findings: These training methods enhance technical skills, increase surgical precision, and reduce the incidence of BDI during laparoscopic cholecystectomy.
Conclusion
The consensus recommendations provide evidence-based approaches to minimize bile duct injury during laparoscopic cholecystectomy. Practices such as the critical view of safety (CVS), intraoperative cholangiography (IOC), and early referral to specialists can significantly improve surgical outcomes and reduce complications. As famously stated, “The history of surgery is the history of the control of bleeding,” a phrase that underscores the importance of meticulous surgical technique and the prevention of complications like bile duct injuries.
Liderança no Campo da Cirurgia
O campo da cirurgia está em constante evolução, exigindo não apenas habilidades técnicas de alta qualidade, mas também capacidades de liderança excepcionais. No entanto, a formação tradicional dos cirurgiões raramente inclui treinamento formal em liderança, deixando muitos profissionais despreparados para assumir posições de liderança. Este artigo explora a importância da liderança na cirurgia, os diferentes tipos de liderança, suas características e oferece recomendações para o desenvolvimento de líderes cirúrgicos.
A Importância da Liderança na Cirurgia
Historicamente, os cirurgiões eram vistos como líderes incontestáveis dentro de um modelo de treinamento de aprendizado, onde a experiência pessoal e o julgamento clínico guiavam as práticas. No entanto, a modernização da medicina, impulsionada pela tecnologia e pela disponibilidade de dados, transformou o ambiente cirúrgico em um campo mais colaborativo e complexo. A liderança eficaz agora é crucial para navegar esse ambiente volátil, incerto, complexo e ambíguo. Como disse Napoleão Bonaparte, “Um líder é um negociador de esperanças.” Na cirurgia, liderar é guiar equipes em meio a incertezas, mantendo sempre a esperança e a confiança nos melhores resultados para os pacientes.
Desenvolvimento da Liderança Cirúrgica
Apesar da importância, muitos cirurgiões recém-formados não recebem treinamento formal em liderança durante a residência. Ao contrário de outras profissões, onde a liderança é um componente central da formação, os médicos devem aprender habilidades de liderança na prática ou através da observação de líderes bem-sucedidos. Programas de desenvolvimento de liderança, semelhantes aos oferecidos a oficiais militares e executivos de negócios, poderiam beneficiar grandemente os cirurgiões. George S. Patton afirmou: “Não diga às pessoas como fazer as coisas, diga-lhes o que fazer e deixe que elas surpreendam você com seus resultados.” Essa filosofia pode ser aplicada na cirurgia, incentivando a autonomia e a inovação dentro das equipes cirúrgicas.
Tipos de Liderança em Cirurgia
Diversos estilos de liderança podem ser aplicados no campo da cirurgia, cada um com suas características únicas:
- Liderança Autoritária:
- Caracterizada por decisões centralizadas e controle rígido.
- Pode ser eficaz em situações de emergência onde decisões rápidas são necessárias.
“O verdadeiro gênio reside na capacidade de avaliar informações incertas, conflitantes, e perigosas.” Winston Churchill
- Liderança Hierárquica:
- Baseada em uma estrutura de comando clara.
- Útil em ambientes estruturados com protocolos bem definidos.
Sun Tzu, em “A Arte da Guerra”, escreveu: “Aquele que é prudente e espera por um inimigo imprudente será vitorioso.”
2. Liderança Transacional:
- Focada em recompensas e punições para alcançar resultados.
- Pode ser útil para manter a eficiência e a produtividade.
Douglas MacArthur disse: “Os soldados devem ter ganho pessoal de suas ações; isso estimula o cumprimento do dever.”
3. Liderança Transformacional:
- Inspira e motiva a equipe a alcançar metas além das expectativas.
- Promove inovação e mudanças positivas na prática cirúrgica.
“O maior líder não é necessariamente aquele que faz as maiores coisas. Ele é aquele que faz as pessoas fazerem as maiores coisas.” – Ronald Reagan
4. Liderança Adaptativa:
- Envolve a capacidade de ajustar-se a novas situações e desafios.
- Crucial em ambientes cirúrgicos dinâmicos e em constante mudança.
Dwight D. Eisenhower afirmou: “Os planos são inúteis, mas o planejamento é tudo.”
5. Liderança Situacional:
- Adapta o estilo de liderança com base nas necessidades específicas da equipe e da situação.
- Proporciona flexibilidade e resposta eficaz a diferentes cenários clínicos.
Como observou Alexander, o Grande: “Não há nada impossível para aquele que tentará.”
6. Liderança Servidora:
- Foca no bem-estar e no desenvolvimento dos membros da equipe.
- Constrói uma cultura de apoio e colaboração.
“O melhor dos líderes é aquele cujo trabalho é feito, cujas pessoas dizem: ‘Nós fizemos isso sozinhos.'” – Lao-Tzu
Características de um Líder Cirúrgico Eficaz
Um líder cirúrgico eficaz deve possuir várias qualidades essenciais, incluindo visão, flexibilidade, motivação, inteligência emocional (EI), empatia, adaptabilidade, confiança, confiabilidade, responsabilidade e habilidades de gestão. A visão permite ao líder definir e perseguir objetivos claros, enquanto a flexibilidade e a adaptabilidade são necessárias para navegar em um ambiente em rápida mudança. Napoleão Bonaparte afirmou: “A liderança é uma combinação de estratégia e caráter. Se você precisar dispensar um, dispense a estratégia.” Essa citação reflete a importância do caráter e da integridade na liderança cirúrgica. A inteligência emocional e a empatia são fundamentais para a comunicação eficaz e para a construção de relacionamentos sólidos dentro da equipe. A confiabilidade e a responsabilidade asseguram que o líder seja um exemplo a ser seguido, promovendo uma cultura de confiança e responsabilidade mútua.
Recomendações para o Desenvolvimento de Líderes Cirúrgicos
Para desenvolver habilidades de liderança, os cirurgiões devem buscar oportunidades de treinamento formal em liderança, participar de workshops e seminários, e buscar orientação de mentores experientes. A autoavaliação honesta e o feedback contínuo são essenciais para o crescimento pessoal e profissional. Além disso, a incorporação de programas de liderança nos currículos de residência cirúrgica pode preparar melhor os futuros cirurgiões para os desafios do campo. Estabelecer um ambiente que encoraje a liderança colaborativa e o desenvolvimento contínuo também é crucial para a formação de líderes eficazes.
Conclusão
A liderança no campo da cirurgia é essencial para enfrentar os desafios de um ambiente médico moderno e complexo. Desenvolver habilidades de liderança em cirurgiões pode melhorar significativamente os resultados dos pacientes e promover uma prática cirúrgica mais eficiente e colaborativa. Ao reconhecer a importância da liderança e investir em seu desenvolvimento, a comunidade cirúrgica pode assegurar um futuro mais brilhante e inovador para a medicina.
Fricção Cirúrgica: Desafios e Realidades no Centro Cirúrgico
Fricção Cirúrgica: Desafios e Realidades no Centro Cirúrgico
No universo da teoria militar, Carl von Clausewitz introduziu o conceito de “fricção” para descrever as dificuldades e imprevistos que complicam a execução dos planos de guerra. Esse conceito, no entanto, transcende o campo de batalha e encontra paralelos surpreendentes em outros cenários complexos e de alta pressão, como o centro cirúrgico. A “fricção cirúrgica” refere-se às diversas dificuldades que cirurgiões e equipes médicas enfrentam durante procedimentos, afetando a eficiência e os resultados esperados.
Imprevisibilidade e Complexidade
Assim como na guerra, a cirurgia está repleta de elementos imprevisíveis. Mesmo com um planejamento meticuloso e uma equipe altamente treinada, fatores inesperados podem surgir. Complicações anatômicas, reações adversas a medicamentos e condições pré-existentes do paciente são apenas alguns exemplos de imprevistos que podem alterar drasticamente o curso de uma operação.
“Tudo na guerra é simples, mas a coisa mais simples é difícil.” – Carl von Clausewitz
Equipamentos e Tecnologia
Embora a tecnologia moderna tenha revolucionado a medicina, ela também introduz sua própria forma de fricção. Equipamentos sofisticados podem falhar ou não funcionar conforme esperado. A calibração inadequada de máquinas, falhas de software em dispositivos médicos e até problemas de energia podem criar obstáculos significativos durante uma cirurgia. Manter e operar esses equipamentos requer um nível elevado de expertise técnica e atenção constante.
“A fricção é o único conceito que distingue amplamente a guerra real da guerra no papel.” – Carl von Clausewitz
Comunicação e Coordenação
A comunicação é crucial em um centro cirúrgico, onde cada membro da equipe desempenha um papel vital. Qualquer falha na transmissão de informações pode ter consequências sérias. Mal-entendidos entre cirurgiões, anestesistas, enfermeiros e técnicos podem levar a erros críticos. A coordenação eficaz é essencial para garantir que todos os procedimentos sejam executados sem problemas, desde a preparação do paciente até a conclusão da cirurgia.
“A mais triviais coisas, vistas no contexto de uma operação militar, parecem ir contra você.” – Carl von Clausewitz
Fatores Humanos
A fricção também emerge das variáveis humanas. Fadiga, estresse e pressão emocional podem afetar o desempenho dos profissionais de saúde. Cirurgiões e enfermeiros frequentemente trabalham em turnos longos e intensos, o que pode levar a lapsos de concentração e julgamento. A capacidade de um profissional de saúde de manter a calma e tomar decisões rápidas e precisas é testada continuamente no ambiente cirúrgico.
“A guerra é o domínio da incerteza; três quartos dos fatores sobre os quais a ação é baseada estão enfiados na névoa de maior ou menor incerteza.” – Carl von Clausewitz
Logística e Suprimentos
A logística desempenha um papel crítico no funcionamento suave de um centro cirúrgico. A disponibilidade de instrumentos estéreis, medicamentos e outros suprimentos médicos é fundamental. Qualquer atraso na entrega de suprimentos ou problemas com a esterilização de instrumentos pode interromper um procedimento e aumentar os riscos para o paciente.
“A guerra é a área da atividade humana mais suscetível à fricção.” – Carl von Clausewitz
Mitigando a Fricção Cirúrgica
Assim como os comandantes militares desenvolvem estratégias para mitigar a fricção na guerra, as equipes cirúrgicas adotam várias práticas para reduzir as dificuldades inesperadas. Treinamento rigoroso e contínuo, simulações de procedimentos complexos e protocolos claros de comunicação são essenciais. Além disso, a manutenção regular de equipamentos e a implementação de sistemas de redundância podem ajudar a minimizar falhas técnicas.
“A habilidade de um líder militar reside na manutenção de uma visão clara e objetiva apesar da fricção.” – Carl von Clausewitz
A fricção cirúrgica, como descrita por Clausewitz em um contexto militar, reflete a realidade desafiadora do centro cirúrgico. Reconhecer e preparar-se para essas dificuldades é crucial para garantir a segurança do paciente e o sucesso das operações. Em última análise, a habilidade das equipes médicas em gerenciar a fricção cirúrgica determina a eficácia e a eficiência das intervenções cirúrgicas.
Charlie Munger’s 25 Cognitive Biases Applied to Digestive Surgery
In the demanding field of digestive surgery, excellence is not just a goal but a necessity. By integrating the profound insights of Charlie Munger on cognitive biases with the motivational principles of Zig Ziglar, surgeons can achieve superior performance and enhance patient care. This comprehensive guide offers actionable recommendations and illustrative examples tailored to the unique challenges of digestive surgery, ensuring that every decision is informed, balanced, and patient-centered. Charlie Munger is a renowned investor and philosopher known for his ability to identify and avoid judgment errors, often rooted in cognitive biases. For a digestive surgeon, understanding and mitigating these biases can significantly enhance clinical decision-making and performance. This summary outlines Munger’s 25 biases and provides specific examples and recommendations for surgical practice.
The 25 Cognitive Biases
- Reward and Punishment Super-Response Tendency
- Example: Opting for procedures with higher financial incentives despite less lucrative alternatives being more appropriate for the patient.
- Recommendation: Always evaluate the long-term benefits for the patient over immediate rewards.
- Liking/Loving Tendency
- Example: Ignoring a team member’s faults because you like them, compromising care quality.
- Recommendation: Maintain objective and impartial evaluations of all team members’ performance.
- Disliking/Hating Tendency
- Example: Dismissing valuable suggestions from colleagues due to personal dislike.
- Recommendation: Prioritize the efficacy of suggestions and patient safety, regardless of who proposes them.
- Doubt-Avoidance Tendency
- Example: Sticking to familiar procedures and avoiding new techniques with better outcomes due to fear of the unknown.
- Recommendation: Stay updated with best practices and be willing to explore new, evidence-based approaches.
- Inconsistency-Avoidance Tendency
- Example: Persisting with outdated surgical techniques to remain consistent with past practices.
- Recommendation: Regularly review clinical guidelines and adapt as necessary.
- Curiosity Tendency
- Example: Spending excessive time researching rare conditions not relevant to daily practice.
- Recommendation: Focus on continuous updates in areas directly related to daily clinical work.
- Kantian Fairness Tendency
- Example: Treating all cases identically without considering individual patient needs.
- Recommendation: Personalize care to meet the unique needs of each patient.
- Envy/Jealousy Tendency
- Example: Allowing jealousy of colleagues’ success to affect the work environment.
- Recommendation: Focus on personal and collaborative professional development, celebrating others’ successes.
- Reciprocity Tendency
- Example: Rewarding personal favors with clinical decisions, like preferences for shifts or cases.
- Recommendation: Maintain professionalism and base decisions on clinical and ethical criteria.
- Simple, Pain-Avoiding Psychological Denial
- Example: Avoiding discussions about poor prognoses to evade emotional discomfort.
- Recommendation: Address all clinical situations honestly and sensitively, providing appropriate support.
- Excessive Self-Regard Tendency
- Example: Overestimating personal skills and refusing assistance or second opinions.
- Recommendation: Recognize personal limitations and seek collaboration when necessary.
- Over-Optimism Tendency
- Example: Underestimating surgical risks and failing to prepare patients for potential complications.
- Recommendation: Conduct comprehensive risk assessments and communicate realistically with patients.
- Deprival-Superreaction Tendency
- Example: Overreacting to resource shortages impulsively.
- Recommendation: Plan ahead and stay calm to find effective solutions.
- Social-Proof Tendency
- Example: Adopting practices simply because they are popular among peers without assessing their efficacy.
- Recommendation: Base clinical decisions on robust evidence and recognized medical guidelines.
- Contrast-Misreaction Tendency
- Example: Underestimating a postoperative complication because it seems minor compared to a recent severe case.
- Recommendation: Evaluate each case individually and objectively, avoiding subjective comparisons.
- Stress-Influence Tendency
- Example: Making hasty decisions under high-pressure situations.
- Recommendation: Develop stress management techniques and make decisions calmly and deliberately.
- Availability-Misweighing Tendency
- Example: Making decisions based primarily on recent experiences instead of comprehensive historical data.
- Recommendation: Maintain detailed records and review long-term data to inform decisions.
- Use-It-or-Lose-It Tendency
- Example: Assuming surgical skills remain unchanged without regular practice.
- Recommendation: Regularly participate in training and simulations to keep skills up-to-date.
- Drug-Misinfluence Tendency
- Example: Underestimating the effects of postoperative analgesics.
- Recommendation: Carefully monitor medication use and adjust as needed.
- Senescence-Misinfluence Tendency
- Example: Resisting learning new surgical techniques due to age.
- Recommendation: Engage in continuous medical education and remain open to innovation.
- Authority-Misinfluence Tendency
- Example: Blindly following a senior colleague’s outdated practices.
- Recommendation: Question and validate all practices against current evidence and standards.
- Twaddle Tendency
- Example: Engaging in irrelevant discussions during surgical planning.
- Recommendation: Focus on relevant, evidence-based information.
- Reason-Respecting Tendency
- Example: Failing to explain the rationale behind surgical decisions to patients.
- Recommendation: Always provide clear, logical explanations to patients and their families.
- Lollapalooza Tendency
- Example: Multiple biases leading to a major error in patient care.
- Recommendation: Be vigilant about recognizing and mitigating multiple biases simultaneously.
- Tendency to Overweight Recent Information
- Example: Giving undue importance to the most recent piece of information received.
- Recommendation: Balance recent information with a thorough review of all relevant data.
Just as Charlie Munger highlights the importance of avoiding cognitive biases for effective decision-making, Zig Ziglar teaches us the significance of attitude and continuous improvement. For a digestive surgeon, applying these principles can transform clinical practice, leading to exceptional performance and superior patient care. Zig Ziglar said, “You don’t have to be great to start, but you have to start to be great.” Every step taken towards overcoming cognitive biases and adopting evidence-based practices is a step towards excellence. By recognizing and mitigating these 25 cognitive biases, you position yourself for an assistive performance that not only treats but truly cares for patients.
Recommendations from Zig Ziglar for Digestive Surgeons
- Believe in Yourself: “If you can dream it, you can achieve it.” Trust in your ability to learn and grow continually.
- Set Clear Goals: “A goal properly set is halfway reached.” Define clear objectives to enhance your skills and knowledge.
- Maintain a Positive Attitude: “Your attitude, not your aptitude, will determine your altitude.” Face challenges with a positive and resilient mindset.
- Learn from Every Experience: “Failure is an event, not a person.” Use every situation, good or bad, as a learning opportunity.
- Serve Others with Excellence: “You can have everything in life you want if you will just help enough other people get what they want.” Focus on patient well-being in all decisions.
By integrating Munger’s lessons and Ziglar’s motivational wisdom, you will not only become a better surgeon but also an inspiring leader and a true advocate for excellence in medicine. Remember always: “Success is doing the best we can with what we have.” Keep evolving, seeking knowledge, and above all, serving your patients with dedication and compassion. Together, let’s transform the practice of digestive surgery, one step at a time, towards the excellence our patients deserve.
Mondino de Luzzi (1270-1326) e o surgimento do MONITOR DE ANATOMIA
Mondino, oriundo de Bolonha, nasceu e concluiu seus estudos em sua cidade natal, obtendo sua graduação por volta do ano de 1290. A partir de 1306, tornou-se membro do corpo docente da universidade local. Ele recebeu instrução de Tadeu, compartilhando a mesma época de estudo com Mondeville, e dedicou-se de maneira sistemática à Anatomia, realizando dissecações públicas do corpo humano. Mondino é reconhecido como o pioneiro na “restauração” da Anatomia. Em 1316, publicou o tratado intitulado “Anothomia”, considerado o primeiro trabalho “moderno” na área, distinguindo-se por sua abordagem prática e original, diferenciando-se de simples traduções de textos clássicos.
A obra de Mondino apresenta desafios, conforme apontado por Singer (1996), destacando-se a nomenclatura confusa e as condições peculiares da dissecação naquela época. A ausência de conservantes apropriados, apesar do conhecimento acumulado pelos egípcios em técnicas de embalsamamento, tornava a dissecação um processo extenuante, preferencialmente realizado no inverno e em até quatro dias específicos para cada região do corpo.
Apesar de imprecisões anatômicas, como apontado por Friedman e Friedman (2001), Mondino desempenhou um papel crucial na instituição da dissecação como componente essencial do estudo anatômico. Essa prática foi posteriormente integrada ao currículo médico da Universidade de Bolonha, permitindo, até o final do século XVI, que as execuções de criminosos fossem realizadas de maneira que não comprometesse o trabalho anatômico, representando um avanço no uso do corpo humano na construção do conhecimento.
A contribuição de Mondino foi duradoura, pois sua obra foi uma das principais fontes de conhecimento em Anatomia humana por mais de duzentos anos, até o advento da obra de Vesalius no século XVI. Ao assumir a cátedra da disciplina, Mondino introduziu uma nova dinâmica nas aulas de Anatomia, afastando-se da dissecação e inserindo o ostensor (aluno) e o demonstrator ou incisore (técnico) para conduzirem os procedimentos, enquanto os alunos observavam.
As técnicas predominantes, como dissecação a fresco, maceração e preparações secas ao sol, eram utilizadas por Mondino e seus contemporâneos. Apesar de suas reservas quanto à maceração, essa técnica continuou a ser praticada, como confirmado pelos textos de Guido de Vigevano em 1345, representando a persistência do uso da dissecação para fins educacionais em Bolonha.
Mondino não expandiu significativamente o conhecimento anatômico existente, mas contribuiu para a formação de anatomistas que perpetuaram a tradição da disciplina em Bolonha, Pádua e em outros países. Notáveis estudiosos, como Gabrielle de Gerbi e Alessandro Achillini, aprimoraram e ampliaram as descrições anatômicas de Mondino em suas próprias contribuições.
A anatomia permanece como alicerce fundamental para o desenvolvimento da medicina ao oferecer conhecimentos cruciais para o adequada exercício profissional. O legado de anatomistas como Mondino, que enfrentaram desafios significativos em suas dissecações pioneiras, ecoa nas salas de aula modernas. A persistência do estudo anatômico é essencial para a formação médica, e os monitores de anatomia desempenham um papel vital nesse processo educativo. Atuando como elo entre a teoria e a prática, esses monitores, herdeiros contemporâneos do ostensor de Mondino, desempenham um papel crucial ao auxiliar na orientação dos alunos nas complexidades da dissecação e na compreensão da anatomia humana. Sua contribuição atual é inseparável do legado histórico, garantindo que o conhecimento anatômico continue a florescer, moldando as futuras gerações de profissionais de saúde e consolidando a anatomia como um pilar indispensável no edifício da medicina.
ODE AOS MESTRES ANATÔMICOS
Ser mestre é perpetuar juventude, Afrontando o inexorável fio do tempo, Desdobrando-se, multiplicando-se, Nas almas dos discípulos, criando ensejo.
Escolas germinam quando a maturidade, Se entrelaça à força do nobre sentimento, O mestre, sábio, fala à mente e coração, Exemplo luminoso, toque profundo, alento.
Na odisseia do saber, mestre é guia, Navegando oceanos de experiência viva, Com luz, desbrava trilhas no pensamento.
O mestre, como sol em seu zênite, Aquece a jornada do aprendizado, Conservando-se jovem, eternamente, erudito.
Assim, na sala de aula, é o comandante, Que com alma e sabedoria encanta, O mestre, semeando luz e meta.
Small desires have a life as short as the journey of those who pursue them.
The will is the road: those who want, move forward; those who don’t, justify.
Those who want find the way; those who don’t, know the reasons.
Those who want make sacrifice meaningful.
Those who don’t want declare the barriers that ease guilt.
Those who don’t want turn restriction into prohibition, limit into decision.
Those who want decide for the outcome to be achieved.
Those who don’t want decide based on the difficulty encountered.
What is challenging for one is motivating for another.
What is sacrifice for one is commitment for the other.
The challenge, for both, changes – irritating or exciting, obstacle or opportunity. Those who want accept and persist.
Those who don’t want retreat and give up.
The drive of man is his GREAT desire.
Small desires have a life as short as the journey of those who pursue them.
O Estoicismo Cirúrgico
Aplicando Princípios Filosóficos na Prática Cirúrgica
O campo da cirurgia, especialmente no tratamento das doenças do aparelho digestivo, exige não apenas habilidades técnicas refinadas, mas também resiliência emocional e ética sólida. A prática cirúrgica, por sua natureza, envolve decisões difíceis, momentos de pressão extrema e desafios inesperados. Nesse contexto, os princípios do estoicismo, filosofia praticada por pensadores como Sêneca, Epicteto e o imperador Marco Aurélio, oferecem ferramentas valiosas para que o cirurgião enfrente a complexidade emocional e ética de sua profissão.
Neste artigo, direcionado a estudantes de medicina, residentes de cirurgia geral e pós-graduandos em cirurgia do aparelho digestivo, vamos explorar como os princípios estoicos podem ser aplicados à prática cirúrgica, promovendo não apenas a eficiência técnica, mas também a excelência ética. Abordaremos as virtudes estoicas que podem moldar o comportamento de um cirurgião, aprimorando sua capacidade de lidar com adversidades e tomar decisões sábias no centro cirúrgico.
1. Aceitação das Limitações: “Primum non nocere” em Ação
O princípio estoico de aceitar o que não pode ser mudado é fundamental para o cirurgião. Em um procedimento cirúrgico, o inesperado pode surgir a qualquer momento. O estoicismo ensina que devemos focar no que está sob nosso controle – nossas ações e reações – e aceitar com serenidade aquilo que foge ao nosso alcance, como complicações imprevistas ou resultados adversos. Essa atitude fortalece o cirurgião, permitindo-lhe manter a calma e a clareza mental em situações críticas.
“O que está no meu poder é como reajo ao que acontece. O resto está fora do meu controle.” – Marco Aurélio
2. A Virtude da Perseverança em Meio às Adversidades
A cirurgia, especialmente nas doenças do aparelho digestivo, frequentemente envolve longos procedimentos, altos níveis de complexidade e a necessidade de ajustes rápidos. O estoicismo valoriza a perseverança diante de dificuldades, uma virtude essencial para o cirurgião que deve persistir no cuidado dos pacientes, mesmo em cenários complicados. A capacidade de continuar com foco e determinação, mesmo em circunstâncias adversas, é o que distingue o cirurgião estoico.
“A adversidade é uma oportunidade para a virtude.” – Marco Aurélio
3. Disciplina e Autocontrole no Centro Cirúrgico
O autocontrole é uma das virtudes centrais do estoicismo, e no campo cirúrgico, é vital que o cirurgião mantenha o controle emocional durante procedimentos complexos. O estoicismo nos ensina a não sermos controlados por emoções passageiras, como medo ou frustração, mas sim a agir com racionalidade. No centro cirúrgico, isso se traduz em decisões conscientes e calculadas, que priorizam o bem-estar do paciente, mantendo a objetividade diante de situações estressantes.
“Não é o que acontece, mas como você reage que importa.” – Marco Aurélio
4. Justiça e a Importância de Tratar Todos os Pacientes com Equidade
Para o cirurgião, a justiça, outro pilar estoico, é essencial. Todo paciente, independentemente de sua condição socioeconômica, deve receber o mesmo nível de cuidado e atenção. A prática cirúrgica ética requer que o cirurgião trate cada paciente com equidade, aplicando os princípios da medicina de maneira justa, sem preconceitos ou favoritismos. O cirurgião estoico vê em cada paciente uma oportunidade de exercer a sua profissão com justiça e integridade.
“A justiça consiste em fazer o que é correto, não o que é popular.” – Marco Aurélio
5. Coragem e Resiliência na Tomada de Decisões Difíceis
A cirurgia muitas vezes exige coragem para tomar decisões difíceis, especialmente em situações de risco à vida do paciente. A filosofia estoica valoriza a coragem como uma virtude indispensável. Para o cirurgião, isso significa enfrentar com firmeza e clareza os dilemas éticos e clínicos, mesmo quando há incertezas. A coragem estoica permite que o cirurgião aja com confiança e serenidade, tomando decisões informadas e moralmente corretas, mesmo em momentos críticos.
“A coragem é a dignidade sob pressão.” – Marco Aurélio
Conclusão
A prática cirúrgica é muito mais do que um conjunto de habilidades técnicas; é uma arte que exige um equilíbrio entre conhecimento, ética e resiliência emocional. Ao adotar os princípios estoicos, o cirurgião pode enfrentar os desafios diários com serenidade, perseverança e justiça, sempre em busca do bem maior para seus pacientes. O estoicismo oferece uma base filosófica robusta para lidar com as pressões da vida cirúrgica, fortalecendo o profissional em sua jornada por excelência técnica e moral.
“A felicidade de sua vida depende da qualidade de seus pensamentos.” – Marco Aurélio
Gostou ❔ Nos deixe um comentário ✍️, compartilhe em suas redes sociais e|ou mande sua dúvida pelo 💬 Chat On-line em nossa DM do Instagram.
#cirurgiageral #filosofiaestoica #éticaemcirurgia #estoicismonaetica #resiliencia
The Surgical Coach (P7)
Importance of OR Etiquette and Professionalism
The NOTTS emphasizes the significance of operating room (OR) etiquette and the evolution of surgical culture towards a more respectful and collaborative environment. Key points include:
- Changing Dynamics in the OR: The historical reputation of surgeons as being arrogant or demeaning, engaging in hazing practices, or displaying disruptive behavior is no longer acceptable. Modern surgeons are expected to create an atmosphere of mutual respect, trust, and communication.
- Cultural Shift towards Respect and Safety: A culture of safety and respect in the OR correlates with improved patient outcomes. It also enhances team communication, fosters professionalism, and contributes to a positive educational experience for all involved.
- Introduction to OR Etiquette: The concept of “OR etiquette” is introduced as a code of conduct among professionals that governs how they act and work together. This is distinct from manners, which are specific behaviors reflecting attitudes toward others.
- Components of OR Etiquette: The chapter covers various aspects of OR etiquette, including communication skills, leadership and followership, giving and receiving feedback, and available programs for improving team communication and culture.
- Team Members in the OR:
- Private Practice Setting: An attending surgeon, possibly with one or more assistants, which may include a second attending surgeon, certified surgical assistant (CSA), or physician assistant (PA).
- Academic Setting: Assistants may include medical students, residents, or fellows. Fellows are fully trained surgeons undergoing additional subspecialty training.
- Learning Environment: Progressive autonomy is a crucial concept, allowing learners to take on more responsibilities based on their competency level.
- Preoperative Discussion: Clear communication between the surgeon and the team members before the operation is essential. This includes discussing roles, responsibilities, and educational goals for the case.
- Patient-Centered Approach: Team members are responsible for reviewing the patient’s case in detail, understanding medical history, current disease status, medications, and diagnostic studies. A shared mental model of the operative and postoperative plan is crucial.
- Intraoperative Focus: During the operation, the patient becomes the central focus. Each team member is expected to contribute to the progress of the operation and assist others in doing the same.
- Postoperative Care Discussion: After the operation, discussions should cover postoperative care aspects, such as pain management, dietary restrictions, venous thromboembolism prophylaxis, and prescription medications.
The series posts (The Surgical Coach) aims to guide professionals in developing a positive OR culture through adherence to etiquette, emphasizing teamwork, respect, and effective communication for improved patient outcomes and a better working environment.
The Surgical Coach (P6)
Promoting a Positive OR Environment: Manners and Etiquette
Maintaining a respectful and collaborative atmosphere in the operating room (OR) is crucial for effective teamwork and patient safety. The author outlines key manners and etiquette that contribute to a positive OR environment:
- Politeness: Being courteous and considerate in interactions with colleagues fosters a harmonious atmosphere.
- Respect: Treating everyone in the OR with respect, regardless of their role or position, is essential for teamwork.
- Humility: Remaining humble helps create a collaborative environment where everyone’s input is valued.
- Learning Names: Taking the time to learn and use the names of all team members enhances personal connections.
- Offering Help: Anticipating needs and offering assistance without being asked demonstrates a proactive and cooperative attitude.
- Asking for Help: Being willing to seek assistance when needed promotes a culture of mutual support.
- Expressing Gratitude: Thanking colleagues for their contributions acknowledges their efforts and encourages teamwork.
- Patient-Centered Focus: Keeping the patient at the center of all actions emphasizes the ultimate goal of providing quality care.
Avoiding Disruptive Behavior:
- Rude, disruptive, or disrespectful behavior is not tolerated.
- Avoid yelling, making sarcastic comments, or engaging in inappropriate jokes.
- Refrain from gossiping or denigrating others.
- When playing music, be considerate of others’ preferences, and turn it off during critical times like the initial time-out.
Social Media Etiquette in the OR:
- Stay professional when using social media in the OR.
- Avoid checking Facebook or Instagram during surgery.
- Exercise caution when posting online, as anything posted can be captured and spread.
- Refrain from posting identifiable patient information.
Effective Communication and Surgical Pause:
- Ongoing effective communication among the surgical team is crucial.
- Emphasizes the importance of the surgical pause or “time-out” to establish a shared mental model.
- Recommends using a structured checklist, such as the World Health Organization Surgical Safety Checklist, during the surgical pause.
- Highlights the checklist’s positive impact on reducing mortality, complications, and hospital length of stay.
- Encourages active engagement of all team members during the checklist process.
Customizing the Checklist:
- The surgical safety checklist can be modified by hospitals or services to include relevant items specific to their patient population.
- Designated leaders should review and discuss each item, ensuring that all team members are introduced and empowered to speak up if they identify potential safety concerns.
- Customization may include a debriefing section at the end of the case to address additional items relevant to the team’s specific practices.
In summary, promoting positive manners and etiquette, avoiding disruptive behavior, and utilizing effective communication tools contribute to a culture of safety and collaboration in the OR. The surgical safety checklist serves as a valuable tool when implemented with commitment and engagement from all team members.
The Surgical Coach (P5)
The Surgery Success Pyramid: Insights from Coach Wooden
Drawing inspiration from the legendary basketball coach John Wooden and his “pyramid of success,” the author has adapted the concept to create the “surgery success pyramid.” This modified pyramid is tailored to the field of surgery, emphasizing key elements for professional and personal success.
Foundational (1st Tier) Elements:
- Industriousness: Hard work and diligence remain foundational to success in surgery.
- Friendship: Emphasizes the importance of teamwork, collaboration, and camaraderie within the surgical profession.
- Loyalty: Stresses the significance of loyalty to colleagues, patients, and the profession.
- Cooperation: Highlights the need for effective collaboration and cooperation among members of the surgical team.
- Enthusiasm: Encourages a positive and passionate approach to the practice of surgery.
2nd Tier Elements:
- Self-Control: The ability to maintain composure and discipline in challenging situations.
- Alertness: Staying vigilant and aware of the evolving surgical environment.
- Initiative: Taking proactive steps to address challenges and improve surgical practices.
- Intentness: Maintaining a focused and determined mindset toward achieving surgical goals.
While the foundational and second-tier elements retain Wooden’s original principles, modifications have been made to better reflect the nuances of the surgical profession.
Take-Home Points for Success in Surgery:
The author concludes with practical advice for success at different stages of a surgical career:
- Medical Student Success:
- Study or practice for an average of 4 hours per day.
- Write at least one paper for the literature per year.
- Engage in lab work and aim for a minimum of three papers per year.
- Read medical journals regularly.
- Strive for academic excellence, including achieving membership in one surgical association.
- Keep a journal or log of patient encounters and lessons learned.
- Prioritize physical fitness.
- Resident Success:
- Dedicate at least 2 hours a day to deliberate practice and study.
- Write one paper per clinical year and a minimum of three papers per year during lab experience.
- Be a positive deviant by identifying and improving inefficient processes.
- Keep a journal or log of valuable clinical insights.
- Maintain physical fitness and well-being.
- Fulfill all residency requirements promptly.
- Junior Faculty Success :
- Focus on mastering surgical practice.
- Seek mentorship and engage in a mentor-mentee relationship.
- Embrace new challenges in education, research, and administration.
- Plan for a full career by considering long-term well-being and financial planning.
- Prioritize life outside the hospital, spending time with family and friends.
- Contribute to the literature and engage in teaching.
- Value colleagues and foster a sense of community within the surgical field.
The author underscores the fulfillment derived from a life dedicated to surgery, emphasizing the value of hard work, continuous learning, and contributions to the field.
The Surgical Coach (P4)
Atul Gawande’s Insights: Navigating Medicine’s Core Requirements
Atul Gawande, a celebrated author known for his insightful perspectives on healthcare, especially in the surgical realm, has provided valuable insights that resonate with medical professionals. In his book “Better: A Surgeon’s Notes on Performance,” Gawande articulates three fundamental requirements for success in medicine:
- Diligence:
- Emphasizes the importance of meticulous attention to detail to prevent errors and overcome challenges.
- Do Right:
- Acknowledges that medicine is inherently a human profession, highlighting the ethical imperative to prioritize patient well-being.
- Ingenuity:
- Encourages a mindset of innovation, urging practitioners to think differently, embrace change, and learn from failures.
Gawande goes beyond defining these core requirements and offers five compelling suggestions on how individuals can make a positive impact within their professional culture:
- Ask an Unscripted Question:
- Advocates for spontaneous inquiries that can lead to unexpected discoveries and foster a culture of open communication.
- Don’t Complain:
- Advises against unproductive complaining, emphasizing that it neither solves problems nor contributes constructively to discussions. Encourages individuals to be prepared with alternative topics for discussion.
- Count Something:
- Promotes the practice of quantifying aspects of one’s work. Gawande suggests that counting something of personal interest leads to valuable insights and continuous learning.
- Write Something:
- Recognizes the transformative power of writing or typing. Encourages professionals to document experiences, insights, and reflections, enhancing both personal and collective learning.
- Change—Be an Early Adopter:
- Acknowledges the necessity of embracing change, especially in the rapidly advancing landscape of surgical technology. Urges individuals to be early adopters, staying abreast of innovations to enhance patient care.
Gawande’s guidance extends beyond the technical aspects of medicine, delving into the realms of communication, mindset, and professional development. These principles provide a roadmap for medical professionals to not only excel in their individual capacities but also positively influence the broader culture within which they operate.
The Surgical Coach (P3)
Legacy of Dr. William Stewart Halsted: Pioneer of Modern Surgery
In the annals of American surgery, the towering figure of Dr. William Stewart Halsted looms large, leaving an indelible mark on the field. Born in 1852 and educated at Andover and Yale, Halsted earned his medical degree from the College of Physicians and Surgeons in New York City in 1878. His illustrious career unfolded against the backdrop of transformative contributions to surgery, earning him the title of the “father of modern surgery.”
Innovations and Contributions 🌟💡
Halsted’s impact reverberated across various realms of surgery. He played a pivotal role in introducing cocaine’s use as a topical anesthetic, revolutionizing the management of pain during surgical procedures. His contributions to the “radical cure” of inguinal hernia, deployment of Listerian principles to reduce wound infections significantly, and groundbreaking surgeries for conditions like gallbladder disease, thyroid disease, periampullary cancer, aneurysm, and breast cancer underscore his multifaceted brilliance.
Halsted Residency Program 🏥👨⚕️
Central to his legacy is the renowned Halsted residency program, which yielded 17 chief residents within 33 years. Dr. Gerald Imber’s biography, “Genius on the Edge: The Bizarre Double Life of Dr. William Stewart Halsted,” encapsulates the complexity of Halsted’s character—rigid yet nurturing, compulsive yet negligent, and always devoted to advancing surgical science.
Halsted’s Reflections and Critique 📜🤔
In a reflective address at Yale in 1904, Halsted acknowledged the transformative strides made in surgery, with pain, hemorrhage, and infection no longer posing insurmountable challenges. However, he voiced concerns about the state of medical education in the United States, advocating for a system that produces surgeons of the highest caliber. His critique emphasized the need for reforms unburdened by tradition, offering ample opportunities for comprehensive training.
Legacy Through Teaching and Training 👩⚕️📚
Following Halsted’s passing in 1922, Dr. Rudolph Matas extolled his greatness as a clinician, scientist, and founder of a surgical school that stood unparalleled in scholarship and achievement. Matas highlighted Halsted’s unique ability to select and nurture a cadre of surgeons who would carry forth his teachings and principles.
The Goal of Training the Next Generation 🌱👩⚕️
Matas, in emphasizing Halsted’s enduring impact, touched upon a lofty aspiration—to train the next generation of surgeons for excellence. Indeed, an active surgeon’s noble pursuit involves imparting knowledge, skills, and a commitment to advancing surgical science to successors.
There Are No Time-Outs: Surgeon’s Lifelong Commitment ⏰💪
The training of a surgeon spans a lengthy, intricate, and challenging path, yet it is undeniably rewarding. Dr. Thirlby’s sentiments, expressed in his Top Ten list, echo the pride associated with surgical accomplishments. The narrative takes a turn toward addressing the often-unspoken topics of work-life balance and burnout. Dr. Thirlby reflects on the countless instances where a surgeon, even when “off duty,” is called upon to employ medical skills and surgical expertise, underscoring the ever-present nature of a surgeon’s commitment to patient care.
In the world of surgery, the white coat symbolizes an unwavering commitment. Driven by a sense of duty, surgeons find themselves intervening in various settings—restaurants, airplanes, theaters, sports fields—always ready to respond. The poignant illustration, “Once you put on the white coat, there are no substitutions, there are no time outs,” encapsulates the profound truth that defines a surgeon’s lifelong dedication to healing and serving others. 🩺👨⚕️🌐
The Surgical Coach (P2)
Mastery in Surgery: The 10,000-Hour Rule
In his acclaimed book “Outliers: The Story of Success,” Malcolm Gladwell delves into the essence of mastery, drawing attention to the 10,000-hour rule popularized by neurologist Daniel Levitin. This rule posits that a staggering 10,000 hours of dedicated practice are requisite for achieving mastery and excellence in any domain. Gladwell surveys diverse fields, from composers and basketball players to fiction writers and surgeons, finding the recurrent thread of the 10,000-hour benchmark.
The Discrepancy in Surgical Training ⏰🔍
However, in the context of surgical training, a stark contrast emerges. Graduating surgical chief residents are tasked with documenting approximately 850 cases, far from the 10,000-hour milestone. Even when considering an estimated 2 hours per case, the cumulative hours fall significantly short. Coach Carril’s emphasis on teamwork, meticulous attention, and the importance of the present moment aligns with the concept of deliberate practice. In those 850 cases, residents are encouraged to focus on refining techniques and embracing each opportunity for skill development.
Teamwork, Basics, and Deliberate Practice 🤝📚
Coach Carril’s principles echo the necessity for teamwork and concentration on fundamental aspects, resonating with Gladwell’s insights. Carril’s principle #18, emphasizing the significance of the present task, aligns with the idea of deliberate practice—immersing oneself fully in the current learning experience. Residents, akin to basketball players honing their skills, find value in focused and intentional practice to bridge the training gap.
Surgery: The Satisfying Triad of Autonomy, Complexity, and Connection 🌐💼💡
Gladwell further posits three key attributes that render work satisfying for individuals: autonomy, complexity, and a tangible connection between effort and reward. Surgery, by its very nature, encapsulates these elements. Autonomy reigns in decision-making and procedural skills, complexity manifests in the intricate facets of various surgeries, and the connection between effort and reward is evident at both the patient and practitioner levels.
The Surgeon’s Reward: A Patient’s Survival and Personal Compensation 🏥💰
At the heart of surgical satisfaction lies the profound connection between the surgeon’s effort and the patient’s well-being. Successfully navigating complex scenarios can be a gratifying reward, epitomizing the essence of surgery. Moreover, the broader efforts of a surgeon, measured in operations performed and patients attended to, correlate with personal compensation and professional recognition.
As surgical training evolves, the delicate interplay between practice, teamwork, and the intrinsic rewards of surgery remains a cornerstone. The journey to mastery may not strictly adhere to the 10,000-hour rule, but the principles of deliberate practice, teamwork, and the fulfilling nature of surgical work persist as guiding beacons in the realm of surgery. 🌟🔪
The Surgical Coach (P1)
Surgery: A Symphony of Skill and Teamwork
In the intricate realm of surgery, where years of rigorous training shape the hands and minds of general surgeons, a profound truth emerges—surgery is not a solitary endeavor. The narrative transcends beyond the operating room, highlighting the symphony of professionals within the healthcare ecosystem. As the surgeon navigates the complexities of patient care, a collaborative effort ensues, akin to the harmonious workings of a team.
Training as a Crucible for Fundamentals 🎓⚙️
Enduring the arduous journey of medical school and a demanding surgical residency, a surgeon’s arsenal is forged. Knowledge, technical prowess, and stamina become the pillars, fortifying the foundation upon which surgical practice rests. Yet, the linchpin is teamwork, a realization that dawns upon every practitioner as they step into the intricate dance of healthcare delivery.
The Surgical Maestro: Pete Carril’s Wisdom 🏀📘
Drawing inspiration from an unexpected quarter, Coach Pete Carril, the luminary basketball coach at Princeton University, becomes a beacon of wisdom. Beyond the basketball court, Carril’s teachings encapsulate universal principles applicable to life and, surprisingly, surgery. In the succinct volume, “The Smart Take from the Strong,” co-authored with Dan White and introduced by the venerable Bobby Knight, Carril imparts timeless wisdom.
25 Little Things: A Paragon for Surgery and Life 🌐📜
Coach Carril’s “25 little things to remember” echo with relevance not just in the realm of basketball but resonate in the corridors of surgery and life. Delving into a few, such as “every little thing counts,” “you want to be good at those things that happen a lot,” and “the way you think affects what you see and do,” the parallels with surgery become strikingly apparent. Carril’s philosophy becomes a guide for surgeons, emphasizing the importance of attention to detail, practice, and the profound interplay between thought and action.
Beyond the Hardwood: Surgery as a Team Sport 🤝🔬
In a synchrony reminiscent of a basketball team, the surgeon harmonizes with a chorus of healthcare professionals—nurses, anesthesiologists, support staff, administrators, and more. The cadence of success is dictated not just by individual skill but by the collective effort of the team. Vision, anticipation, and unwavering dedication converge, not only on the basketball court but also in the theater of surgery.
As Coach Carril remains a silent spectator in the hallowed halls of Princeton, witnessing a new generation striving for victory, surgeons too find inspiration in the collective pursuit of excellence. Teamwork, an indomitable spirit, and a commitment to personal and collective growth emerge as the hallmarks of success, both on the hardwood and in the operating room. 🏀🌟🔪
The Surgical Coach
Surgical Wisdom Unveiled: A Top Ten List and Commandments
Reflections on a Surgical Journey 🌟
Life’s journey is a mosaic woven with threads of guidance from parents, siblings, and mentors. This chapter transcends the mundane, embracing philosophy and personal testimony on sculpting a triumphant surgical career. Dr. Richard C. Thirlby, in the spirit of David Letterman, unfurls a top ten list that serves as a compass for aspiring surgeons.
Dr. Thirlby’s Top Ten Surgical Tenets 📜🌐
- Training is Fun (You’ll Never Forget It): A nod to lifelong learning, acknowledging the perpetual metamorphosis in surgical careers.
- Job Security: General surgeons, vital and in demand, find positions across diverse landscapes, from bustling urban centers to the serene rural expanses.
- The Pay is Not Bad: Comfortable compensation, soaring above societal averages, promises financial stability.
- Your Mother Will Be Proud of You: A familial pride resonates, extending beyond mothers to fathers, aunts, and a tapestry of family members.
- Surgeons Have Panache: Embracing the surgical personality and the unique culture that envelopes surgical realms.
- You Will Have Heroes; You Will Be a Hero: Surgeons, sculpted by influencers, reciprocate by becoming beacons of hope for grateful patients.
- There is Spirituality if You Want It: The inexplicable recoveries, the miraculous moments that defy statistical norms.
- You Will Change Patients’ Lives: A profound personal satisfaction derived from the tangible impact on patients’ destinies.
- Patients Will Change Your Life: Daily lessons from patients foster humility, nonjudgmentalism, and a continuous journey towards becoming a better human being.
- I Love to Cut: A poetic reflection of the joy derived from the meticulous artistry of surgical procedures, executed with precision for the greater good.
The Commandments of Surgical Living 🌌📜
Adding depth to the narrative, akin to timeless commandments, Dr. James D. Hardy contributes a list transcending millennia, etched in the New King James Version of the Holy Bible.
- Know Your Higher Power: An homage to the spiritual facet of life and the sanctity of the Sabbath day.
- Respect Your Roots: An acknowledgment of the significance of parents and the importance of familial bonds.
- Do No Harm: An ancient ethos resonates through the prohibition of actions such as murder, adultery, theft, lying, and coveting others’ belongings.
- Strive for Excellence: An unending pursuit of personal and professional growth, embodying efficiency, excellence, and the preservation of integrity.
- Prepare for Leadership: A call to groom leaders, emphasizing the importance of educational and professional growth.
- Nourish Professional Relationships: Recognizing the value of mentors, preserving the wisdom passed down through generations.
- Remember Your Roots: An echo from Dr. Hardy’s personal ten commandments, urging individuals to honor their origin and represent it with pride.
- Cherish Family: A gentle reminder to spend quality time with family, recognizing the profound impact of love on children.
- Spend Time Alone: Advocating for moments of solitude, fostering creative thinking and personal reflection.
- Find Joy in Your Work: A profound truth encapsulated in the sustenance derived from the daily pursuit of meaningful work one genuinely enjoys.
In this amalgamation of Dr. Thirlby’s top ten and Dr. Hardy’s commandments, a roadmap unfolds — a guide not just for a surgical career but for a fulfilling and purpose-driven life. 🌈🔍🔬
Gastrointestinal Anastomosis
Navigating the Gastrointestinal Anastomosis: A Surgical Odyssey
Unveiling the Historical Tapestry 🕰️
The creation of gastrointestinal anastomoses, an art in general surgery, has evolved over centuries. In delving into this surgical saga, fundamental principles stand tall, guiding the surgeon’s hands. This chapter unfolds the historical nuances, general tenets for successful anastomosis creation, and delves into pivotal technical considerations amidst current controversies.
The Dance of Healing and Anatomy 🩹🔍
Understanding the physiological waltz of gastrointestinal wound healing and the intricacies of intestinal wall anatomy sets the stage. An enterotomy’s inception triggers a symphony of vasoconstriction, vasodilation, and capillary changes, orchestrating the ballet of tissue healing. Granulation tissue emerges, heralding the proliferative phase, where collagen undergoes a dance of lysis and synthesis.
Layers of the Gastrointestinal Tapestry 🧵
The intestinal wall, a multilayered tapestry, unravels its secrets. The serosa, a connective tissue cloak veiled by mesothelial lining, demands precise apposition to thwart leakage risks. The submucosa, the stronghold of tensile strength, anchors the sutures knitting the anastomosis. Intestinal mucosa seals the deal, driven by epithelial cell migration and hyperplasia, crafting a watertight barrier.
Local Factors: Paving the Path to Healing ⚒️🩹
The local factors influencing this symphony include intrinsic blood supply and tension management. Adequate blood supply, a lifeline for tissue oxygenation, hinges on meticulous surgical technique. Tension, a delicate partner in this dance, demands finesse; too much jeopardizes perfusion, too little invites inflammatory infiltrates. The colon, in particular, demands a surgeon’s nuanced touch.
Systemic Harmony: The Ripples of Patient Factors 🔄🌊
Systemic factors contribute their ripples to this surgical pond. Hypotension, hypovolemia, and sepsis compose a dissonant note affecting blood flow and oxygen delivery. Patient-specific variables — malnutrition, immunosuppression, and medication use (hello, steroids and NSAIDs) — compose a subplot, influencing the narrative of wound healing.
As the surgeon steps into this intricate ballet of anastomosis creation, history, physiology, and patient-specific factors converge. Each suture, each decision, shapes the narrative of healing. The gastrointestinal odyssey continues, blending tradition with innovation, as surgeons embark on the timeless quest for successful anastomoses. 🌐🔍🩺
Pre Surgical Evaluation of BLEEDING
Unraveling Bleeding Risks: A Surgical Odyssey
In the realm of surgical care, meticulous assessment of bleeding risk is paramount. The age of onset of bleeding and the specific sites affected offer crucial clues, helping differentiate between inherited and acquired bleeding disorders. Inherited disorders, often manifesting in childhood, may lurk beneath the surface, surfacing during surgical trauma in adulthood.
Decoding the History 🕰️
Interrogating the patient’s history unveils key insights. Medication usage, both prescription and over-the-counter, unfurls potential contributors to bleeding events. Family history provides a roadmap for inheritance patterns, crucial in diagnosing disorders like hemophilia. The severity of past bleeding incidents serves as a yardstick, guiding expectations during surgical challenges. Comorbidities, especially liver and kidney dysfunction, loom large in magnifying bleeding risks.
The Physical Symphony 🩺🎶
While the physical exam plays a supportive role, it may hint at platelet disorders through findings like petechiae and ecchymoses. Platelet function issues or deficiencies may manifest similarly, emphasizing the importance of a comprehensive history. Single-site bleeding tends to be non-indicative of a bleeding disorder, while multisite bleeding raises red flags.
Laboratory Pilgrimage 🧪
A pilgrimage through laboratory tests offers a comprehensive snapshot of hemostatic competence. Assessing platelet count, complete blood count (CBC), platelet function, aPTT, PT, and fibrinogen levels becomes the map for surgical decisions.
Unmasking Causes of Excessive Surgical Bleeding 🚩
Most patients enter the operating room with normal hemostasis. However, certain surgeries, like liver transplants or trauma interventions, may trigger consumptive coagulopathy. Preexisting hemostatic defects, especially congenital bleeding disorders like hemophilia and von Willebrand disease, require keen suspicion.
Hunting the Culprit: Acquired Bleeding Disorders 🎯
Liver disease emerges as a common instigator of coagulation abnormalities, while anticoagulant therapies like Coumadin and heparin cast shadows on surgical hemostasis. Acquired thrombocytopenia, often linked to splenomegaly or medications, and platelet function disorders, especially induced by aspirin and clopidogrel, populate the landscape of surgical challenges.
Navigating Intraoperative Waters ⚓🔍
Intraoperative bleeding may cascade from shock, massive transfusions, or acute hemolytic reactions. Hemostatic agents, from gelatin sponge to topical thrombin, stand as stalwart navigators through these turbulent waters.
Postoperative Chessboard: A Risky Endgame ♟️🩹
Postoperative bleeding, often stemming from inadequate hemostasis, unveils additional players. Residual heparin, altered liver function, and acquired clotting factor deficiencies post-hepatectomy amplify the stakes. Fibrinolysis disorders may also cast shadows post-surgery.
Dancing with Disseminated Intravascular Coagulation (DIC) 🩸🎭
DIC, a theatrical presentation of intravascular coagulation gone awry, demands a spot on the stage. Prompt recognition and addressing precipitating factors are pivotal, with cryoprecipitate and platelet transfusions standing as protagonists.
Fibrinolytic Fantasia: When Clotting Goes Amiss 🌪️🩹
Primary and secondary fibrinolysis emerge as culprits in postsurgical bleeding, often linked to lytic therapy, severe liver failure, or DIC. Managing fibrinolytic storms necessitates tailored interventions.
Hypercoagulable Waltz in Surgical Limelight 💃🕺
A careful dance with thromboembolism risks follows, accentuating the importance of patient history in unraveling congenital and acquired hypercoagulable states. A familial narrative often unravels the genetic predispositions steering this intricate choreography.
In the surgical arena, every patient’s hemostatic tale unfolds uniquely. Through history, examination, and laboratory revelations, surgeons navigate the delicate balance between bleeding and clotting, ensuring a symphony of healing amidst the surgical odyssey. 🌐🔍🩺
Nutritional Surgical Care
Navigating the Nutritional Maze in Surgical Care 🌐🔍
Surgeons bear the responsibility of caring for patients whose nutritional status may be compromised, influencing their ability to heal optimally. The challenges encompass an array of issues, including anorexia, inanition, gluconeogenesis acceleration, hyperglycemia, insulin resistance, and electrolyte and hormonal imbalances. These factors intricately impact surgical responses and a patient’s healing capacity. Let’s delve into the complex world of digestive tract, esophageal, gastric, intestinal, and other surgeries, exploring how they interplay with nutritional considerations.
Digestive Tract Surgery 🍽️
The digestive tract, a bustling center of metabolic activity, plays a pivotal role in nutrient digestion, absorption, and metabolism. Surgical interventions involving the gastrointestinal (GI) tract can lead to malabsorption and maldigestion, causing nutritional deficiencies. Understanding the site of nutrient absorption aids in identifying potential postoperative deficiencies. Enhancing nutritional status before surgery becomes crucial for a smoother postoperative recovery.
Esophageal Surgery 🥄
Various conditions affecting the esophagus, from corrosive injuries to obstruction, necessitate surgical intervention. Procedures involve replacing the esophagus with the stomach or intestine, each carrying unique considerations. Nutritional support, including nasoenteric feeding tubes or parenteral nutrition (PN), may be necessary preoperatively for obstructed esophagi, with additional intraoperative measures for optimal postoperative outcomes.
Gastric Surgery 🥢
Gastric surgical procedures, while addressing specific issues, can potentially lead to malnutrition. Patients may experience dumping syndrome, requiring dietary modifications and cautious fluid intake. Anemia and metabolic bone diseases are common consequences, demanding periodic injections and calcium-vitamin D supplementation. Understanding postgastrectomy dietary modifications and careful fluid management becomes paramount.
Intestinal Surgery 🍴
Resection of excessive lengths of the intestine, especially in short bowel syndrome, can result in severe malabsorption and malnutrition. Long-term PN might be necessary to maintain nutritional balance. Pancreaticoduodenectomy, a complex surgery, requires postoperative monitoring for complications like delayed gastric emptying, diabetes mellitus, and malabsorption, influencing nutrient guidelines.
Ileostomy and Colostomy 🚽
Procedures like ileostomy or colostomy, creating artificial anuses, are employed for various intestinal issues. Patients with ostomies generally follow regular diets, with adjustments based on stoma output. High-output ostomies necessitate specific dietary precautions to manage fluid levels. Nutritional assessment’s crucial role in surgical outcomes emphasizes the growing interest in tailored preoperative nutritional support and the potential resurgence of parenteral nutrition.
Conclusion 🩺💡
Understanding the intricate dance between surgical interventions and nutritional considerations is paramount for surgeons and medical practitioners. As regulatory scrutiny intensifies, the role of nutrition in preventing complications and improving outcomes will likely take center stage, emphasizing the importance of personalized nutritional strategies in the surgical journey. 🌟💪
Tubes and Drains
Unlocking the World of Tubes and Drains in Medical Practice 🩹
Understanding the diverse array of tubes and drains is crucial for any medical practitioner, and it all begins with appreciating the French size system, where the outer diameter of a catheter is denoted. A quick calculation (French size multiplied by 0.33) reveals the catheter’s outer diameter in millimeters.
Gastrointestinal Tract Tubes 🍽️
Starting with nasogastric tubes designed to evacuate gastric contents, these are frequently employed in patients facing ileus or obstruction. Modern nasogastric tubes often incorporate a sump function, preventing suction locks and enhancing efficiency. Nonsump tubes, though less common, may be used for intermittent suction. Nasogastric tubes also serve in feeding, with soft, fine-bore tubes being preferred for this purpose. Nasoenteric tubes, intended for feeding, require careful attention to safety during instillation.
Nasobiliary tubes, often placed endoscopically, aid in biliary drainage in cases of obstruction or fistula. T-tubes within the common bile duct ensure closed gravity drainage. Gastrostomy tubes, placed surgically or via percutaneous endoscopic gastrostomy (PEG), find utility in drainage or feeding. Jejunostomy tubes, inserted surgically or endoscopically, are vital for long-term nutritional access.
Respiratory Tract Tubes 🫁
Chest tubes play a pivotal role in pleural cavity drainage, addressing issues like pneumothorax, hemothorax, or effusion. The three-bottle system facilitates constant suction, drainage, and prevention of air entry, crucial for maintaining a water seal.
Endotracheal tubes, cuffed for a secure tracheal seal, cater to short-term mechanical ventilation needs in adults. Tracheotomy tubes, directly inserted into the trachea through the neck, become essential for prolonged mechanical ventilation or when maintaining a patent airway is challenging.
Urinary Tract Tubes 🚰
Bladder catheters, commonly known as “Foley” catheters, serve to straight drain urine. Nephrostomy tubes, placed in the renal pelvis, drain urine above obstructions or delicate ureteral anastomoses. Percutaneously placed tubes, often pigtail catheters, assist in draining abscesses, typically guided by interventional radiologists.
Surgical Drains 🌡️
Closed suction drains, such as Jackson-Pratt and Hemovac, prove invaluable for evacuating fluid collections during surgery. Sump suction drains, like Davol drains, are larger and designed for continuous suction in scenarios with thick or particulate drainage. Passive tubes, exemplified by Penrose drains, offer a pathway for fluid without applied suction, serving as a two-way conduit for bacteria. Understanding these various tubes and drains is pivotal for medical practitioners navigating complex clinical scenarios. 💉💊
The Geriatric Patient
Navigating Surgical Challenges in an Aging Population: A Delicate Balance 🌐
The ongoing aging process within the American population brings forth a set of unique challenges that surgeons must adeptly navigate for decades to come. Elderly individuals, compared to their younger counterparts, often exhibit diminished physiological reserves. Their health is frequently influenced by medications that can alter normal physiological responses, such as β-blockers, or impact surgical outcomes, like warfarin or platelet aggregation–inhibiting agents. Additionally, baseline impairments, ranging from sensory issues to difficulties in ambulation or dementia, may complicate their ability to engage in everyday activities.
One perplexing dilemma faced by surgeons when caring for elderly patients revolves around the decision to pursue an aggressive intervention plan. Transparent communication between the patient and physician is paramount in determining the appropriate level of aggressiveness in the patient’s best interest. This conversation takes on heightened significance in the elderly population. Engaging in repeated discussions with patients and their families, starting before surgery and extending into the postoperative phase, is crucial. Generally, patients express a desire for aggressive medical care as long as there remains a reasonable chance for meaningful survival.
While these discussions may be uncomfortable, they are as integral to the patient’s care as any aspect of their medical history. It is imperative to recognize that surgical care is provided by individuals who genuinely care about the patient’s overall well-being. In certain situations, medical care may prioritize alleviating pain over prolonging life. Ideally, these conversations should occur in a serene and comfortable setting, free from distractions.
Moreover, it is essential to underscore that discussions about end-of-life matters are not legal proceedings. No forms need to be signed. These discussions are akin to any other conversation between a doctor and a patient regarding their care. The dialogue involves a careful consideration of the strengths and weaknesses of different approaches until a collaborative plan of action is determined. The only distinction lies in the profound nature of end-of-life discussions, offering patients the best opportunity to shape their destinies. Consequently, these discussions should be approached with the utmost reverence, acknowledging the gravity of the subject matter. 🤝💙
Estabelecendo Conexões Essenciais 💬
Técnicas de Entrevista na Medicina: Estabelecendo Conexões Essenciais 💬
A relação médico-paciente é uma parte vital do cuidado cirúrgico. O vínculo entre o cirurgião e o paciente deve ser construído, mantido e valorizado. Boas técnicas de entrevista são fundamentais para estabelecer essa relação. O alicerce para uma boa entrevista advém de uma preocupação genuína com as pessoas. Embora existam habilidades de entrevista que podem ser aprendidas, a qualidade da interação pode ser aprimorada. Estudantes de medicina devem reconhecer seu papel especial no cuidado do paciente, não se envergonhando de sua posição e compreendendo que são membros eficazes da equipe. Pacientes frequentemente veem os estudantes de medicina como acessíveis, compartilhando detalhes que poderiam ocultar de membros mais seniores da equipe. O papel do estudante é descobrir as queixas médicas principais do paciente, realizar uma história e exame físico focalizados e apresentar os achados à equipe. Uma entrevista eficaz requer a comunicação sobre quem você é e como se encaixa na equipe. 🏥
Desafios da Entrevista na Medicina: Adaptando-se a Diferentes Ambientes 🌐
Entrevistar bem pode ser desafiador devido à variedade de ambientes, como sala de cirurgia, unidade de terapia intensiva, consultório particular, leito hospitalar, sala de emergência e ambulatório. Cada ambiente apresenta desafios únicos à comunicação eficaz. Para construir boas relações médico-paciente, cirurgiões ajustam seus estilos a cada ambiente e à personalidade e necessidades de cada paciente. Algumas regras básicas são comuns a todas as entrevistas profissionais. A primeira regra é deixar claro ao paciente que, durante a história e o exame, nada além de uma emergência de vida ou morte terá maior importância do que a interação entre o cirurgião e o paciente naquele momento. Este é o primeiro e melhor momento para conectar-se com o paciente. É crucial que o paciente compreenda que um cirurgião cuidadoso, conhecedor e dedicado será seu parceiro na jornada pelo tratamento de doenças cirúrgicas. O cirurgião deve observar outras regras, incluindo dar atenção adequada à aparência pessoal para transmitir uma imagem profissional que inspire confiança, estabelecer contato visual, comunicar interesse, calor e compreensão, ouvir de forma não julgadora, aceitar o paciente como pessoa, ouvir a descrição do problema do paciente e ajudar o paciente a se sentir confortável na comunicação. 👩⚕️👨⚕️
Primeiros Minutos: Estabelecendo uma Base Sólida 🤝
Ao receber o paciente em um ambiente ambulatorial, os primeiros minutos são dedicados a cumprimentar o paciente pelo nome formal, apertar as mãos, se apresentar e explicar o papel do cirurgião. A atenção à privacidade do paciente, ajustando o estilo de conversação e o vocabulário às necessidades do paciente, descobrindo a atitude do paciente em relação à clínica, conhecendo a ocupação do paciente e entendendo o que o paciente sabe sobre sua condição são passos fundamentais. A seguir, ocorre a exploração do problema, movendo-se de perguntas abertas para perguntas fechadas. Técnicas importantes incluem o uso de transições, fazer perguntas específicas e claras e reformular o problema para verificação. É crucial determinar se o paciente tem alguma pergunta. No final da entrevista, o cirurgião explica quais serão os próximos passos e que realizará um exame no paciente. Por fim, verifica-se se o paciente está confortável. 🌟
Diferenças nos Ambientes de Atendimento: Adaptação e Compreensão 🏨
As técnicas utilizadas em ambientes ambulatoriais são igualmente adequadas para encontros em ambientes hospitalares e de pronto-socorro. Geralmente, mais tempo é dedicado ao paciente nas entrevistas iniciais e subsequentes do que em um ambiente ambulatorial. Na entrevista inicial, os pacientes podem estar com dor, preocupados com problemas financeiros e ansiosos com a falta de privacidade ou dietas desagradáveis. Eles também podem ter dificuldade para dormir, sentir medo do tratamento ou se sentir impotentes. É importante comunicar gentil e confiantemente o propósito da entrevista e quanto tempo levará. O paciente não apenas escuta, mas também observa o comportamento e a vestimenta do médico. O ambiente também afeta a entrevista. Por exemplo, um ambiente apertado, barulhento e lotado pode afetar a qualidade da comunicação. Pacientes podem ter sentimentos negativos devido a insensibilidades por parte do médico ou de outras pessoas. É fundamental evitar falar com o paciente na entrada do quarto, dar ou receber informações pessoais em um ambiente lotado, falar sobre um paciente em um elevador ou em outro espaço público, ou falar com um paciente sem fechar a cortina em uma enfermaria. 🌆
Conclusão: Construindo Relações de Confiança na Medicina 🌐
Em resumo, dominar as técnicas de entrevista na medicina é essencial para construir relações sólidas entre médico e paciente. Os cirurgiões habilmente ajustam suas abordagens a diferentes ambientes e personalidades dos pacientes, aplicando regras básicas universais. Os primeiros minutos são cruciais para estabelecer uma base sólida, enquanto a exploração cuidadosa do problema requer uma transição de perguntas abertas para fechadas. Adaptações ao ambiente e compreensão das preocupações do paciente são vitais para uma comunicação eficaz. Ao incorporar essas técnicas, os médicos podem garantir que a interação médico-paciente seja centrada no paciente, transmitindo confiança e dedicação à jornada conjunta pelo tratamento. 👨⚕️🤝👩⚕️
Navigating Your Clinical Experience in Surgery
Transitioning to the Role as a Junior Member of the Surgical Health Care Team: Navigating Your Clinical Experience in Surgery
Embarking on your surgical clerkship is an immersive clinical journey that extends beyond aspiring surgeons. This experience is a valuable opportunity to refine essential clinical skills applicable to any medical specialty. As you progress in your medical career, encounters with patients requiring surgical intervention will be inevitable. The insights gained during your surgery clerkship will empower you to identify surgical diseases, understand the need for surgical consultations, and develop empathy for the emotional, physiological, and logistical aspects patients and their families may face during operations or consultations.
Approaching Your Role: A Shift in Learning Dynamics
As a seasoned learner in medical school, your entry into the health care team during your 3rd year marks a profound transition. The focus is no longer solely on memorization; it now involves understanding patients’ complaints and diseases. Balancing voluminous information, time constraints, and determining the depth of knowledge required for patient care present unique challenges. Successful clinical performance is influenced by various factors:
- Preparatory Coursework and Experience: Constructing new knowledge relies on existing foundations. Deep knowledge, especially in anatomy, facilitates a seamless connection between new information and prior understanding.
- Quality of Study Methods: Active learning demands taking responsibility for your education. Maintaining a disciplined study plan aligned with your learning style is essential.
- Organizational Skills: Successful learners adeptly manage time and priorities to avoid last-minute cramming, reducing stress.
- Motivation and Emotion: Enthusiasm and positive feelings toward content, team, and environment significantly impact the clerkship experience and how you are perceived by patients and the team.
- Physical Health: The link between physical well-being and effective learning underscores the importance of attending to personal health needs.
- Distractibility and Concentration Skills: Active engagement in learning, whether through reading or listening, is crucial for processing and translating information into meaningful knowledge.
Maximizing Your Learning: Strategies for Success
1. Prepare, Practice, and Review:
- Preparation: Activate prior knowledge by pre-reading about upcoming topics, enhancing comprehension, and fostering long-term memory.
- Practice: Actively engage in learning, take notes, and generate questions. Studies show that self-generated notes enhance retention.
- Review: Ongoing review, coupled with self-assessment using test questions, patient management problems, and creating personal tests, reinforces information.
2. Organize Your Knowledge:
- Get the Big Picture: Familiarize yourself with learning objectives, chapter headings, and subheadings before reading. Listing questions beforehand guides focused reading.
- Review Charts and Diagrams: Key information in charts and diagrams aids study. Testing yourself on missing information enhances understanding.
- Emphasize Integration: Relate new information to patient encounters, lectures, or images. Create mind maps to organize information and identify patterns.
3. Know Expectations and Thyself:
- Clarify your role and responsibilities by reviewing syllabus materials and seeking guidance from experienced peers, residents, or faculty.
- Define personal learning goals and learning style, being proactive in your approach to studying.
4. Ask! Ask! Ask!:
- Be persistent and assertive in seeking clarification, feedback, or assistance.
- Utilize the wealth of expertise within the surgical team, including nurses, physician assistants, pharmacists, social workers, and technicians.
Maximizing Your Emotional Intelligence: Strategies for Well-Being
1. Focus Forward with a Positive Attitude:
- Make decisions with a positive end in mind, maintaining situational awareness in varied scenarios.
- Cultivate open-mindedness, positive energy, and enthusiasm to contribute constructively to patient care and the team.
2. Set Goals and Celebrate Successes:
- Define short- and long-range goals, including personal, financial, and relationship goals.
- Document achievements, reinforcing a sense of accomplishment and self-confidence.
3. Promote a Supportive Learning Environment:
- Take responsibility for mistakes, learn from them, and foster trust within the team.
- Avoid negativity by steering clear of individuals with persistent negative attitudes or behaviors.
In conclusion, approach your surgery clerkship with a proactive mindset. Maximize both your intellectual capabilities and emotional intelligence to derive the utmost benefit from this transformative experience. Keep in mind the wisdom of John Wooden, emphasizing the importance of being the best version of yourself. This principle not only ensures success in your surgery clerkship but resonates throughout your medical journey.
REVISIONAL BARIATRIC SURGERY
- INTRODUCTION
Morbid obesity is a global chronic disease affecting 13% of people worldwide. Weight loss surgery has been proven to be effective in addressing this chronic disease and its associated comorbidities. In 2016, over 200,000 procedures were performed in the United States, and the volume continues to grow. Cases analyzed between 2015 and 2018 indicate an overall growth rate of 21.9%. The most common surgeries performed in the United States are Roux-en-Y gastric bypass (RYGB), sleeve gastrectomy (SG), and biliopancreatic diversion with duodenal switch (BPD/DS). Estimated mean weight loss is 33% of the initial body weight. Unfortunately, it is estimated that up to 25% of patients will have weight regain after primary surgery. Weight regains or recidivism has emerged as a clinical entity and important public health issue given its association with re-emergence of obesity related comorbidities, worsening quality of life, and increased healthcare costs. With the increased number of primary bariatric surgery performed worldwide, revisional surgery has also increased, and it has been shown to be the fastest-growing category of bariatric procedures, currently representing 7 to 15% of all bariatric operations and long-term rates of revisional surgery have been estimated to be as high as 56%.
2. CAUSES
Weight regain is estimated in up to 25% of patients following primary bariatric surgery. In addition, it is estimated that more than 80% of the weight regain happens within the first 6 years following primary surgery. A major factor contributing to weight regain is lack of adherence to recommended followup visits, observed in approximately 60% of patients 4 years after primary surgery. The etiology of weight regain has been attributed to:
• Noncompliance with dietary recommendations.
• Hormonal/metabolic imbalance.
• Mental health.
• Physical inactivity.
• Anatomic/surgical factors.
• Medications.
3. PREOPERATIVE EVALUATION
A multidisciplinary evaluation is essential prior to recommending revisional surgery to patients presenting with weight gain. As with primary surgery, a nutritional evaluation, behavioral/psychological assessment, and endoscopic and contrast series studies should be obtained. The latter will not only aid in establishing an anatomic etiology for weight regain if present, but it will also aid in choosing the type of revisional surgery.
4. SELECTING THE TYPE OF REVISIONAL SURGERY
There are several revisional procedures following primary bariatric surgery. The choice of revisional surgery is tailored according to initial surgery, cause of failure, and surgeon’s experience. Multiple revisional surgeries have been described for all primary bariatric surgeries, but no standardized guidelines have been established. In June 2019, 70 experts from 27 countries formed a committee and created the first consensus on revisional bariatric surgery. An agreement of 70% or more was considered consensus. Consensus was achieved in several points including but not limited to:
(1) RBS is justified in some patients;
(2) RBS is more technically challenging than the respective primary bariatric surgery;
(3) second or third RBS can be justified in some patients;
(4) candidates should undergo a nutritional assessment, psychological evaluation, endoscopy, and a contrast series;
(5) RYGB, one anastomosis gastric bypass (OAGB), and SADI-S are options after gastric banding; and
(6) OAGB, BPD/DS, and SADI-S are options after sleeve gastrectomy. Regarding revision for primary RYGB, the only consensus obtained was lengthening of the biliopancreatic limb as RBS option for RYGB or OAGB.
Roux-En-Y Gastric Bypass
Roux-en-Y gastric bypass is one of the most common weight loss procedures performed worldwide and is considered by many to be the gold standard. Unfortunately, approximately 10–34% of patients experience inadequate weight loss or weight gain and may ultimately require revision. The most common etiology of weight regain is pouch dilation. Other reported etiologies include enlarged gastric pouch greater than 5 cm in diameter, wide gastro-jejunal anastomosis (GJA), anastomosis greater than 1 cm, GJA > 1.5 cm in diameter, dilated GJA greater than or equal to 2 cm, pouch >30 mL, pouch dilation >120 mL, weight recidivism with or without gastric fistula, gastric fistula, short-limb bypass, and hyperphagic behavior. Multiple revisional surgeries have been described. In a recent systemic review and meta-analysis, distal Roux-en-Y gastric bypass (DRGB) alone showed the highest decrease in BMI at 1-year follow-up versus biliopancreatic diversion with duodenal switch (BPD/DS) or single anastomosis duodeno-ileal bypass and sleeve gastrectomy (SADI-S) at 3-year follow-up. Overall, they found maximal BMI decrease in DRGB alone, followed by BPD/DS or SADI-S, laparoscopic pouch and/or GJA resizing, and endoscopic pouch and/or GJA resizing.
Sleeve Gastrectomy
Sleeve gastrectomy (SG) is currently the most commonly performed bariatric procedure worldwide. Its relatively simple technique and low complication rate contribute to it being preferred over some other procedures. Revision is estimated in up to 30% of cases for multiple etiologies, including weight regain. Loss of restriction is one of the main anatomic factors contributing to weight regain. Although revision to RYGB or DS has been recommended as the standard of care, some studies have described revision with re-sleeve for dilation of the residual stomach as the cause. The overall %EWL following re-sleeve can be up to 57% at 12 months and up to 60% at 20 months. A retrospective study analyzed conversion from SG to either RYGB or SADI for insufficient weight loss or weight regain. Out of 140 patients, 66 patients underwent SG to SADI, and 74 patients underwent SG to RYGB. SADI was found to achieve 8.7%, 12.4%, and 19.4% more total body weight loss at 6, 12, and 24 months compared to RYGB for weight regain alone. RYGB is preferred when symptoms of reflux accompany weight regain. For patients with super morbid obesity and weight regain after SG, in the absence of reflux symptoms, conversion to biliopancreatic diversion with duodenal switch (BPD/DS) is recommended for maximal weight loss, with %EWL ranging from 70 to 80% at 2 years.
5. WEIGHT LOSS FOLLOWING REVISIONAL SURGERY
Weight loss after revisional bariatric surgery leads to significant weight loss in the long term, rates varying per procedure performed. A single-center retrospective study for patients who underwent revisional surgery for weight regain (52.4%) S. Ardila et al. analyzed weight loss at 3-, 6-, 9-, and 12-month intervals. Patients with a primary restrictive procedure and reflux symptoms underwent conversion to either RYGB or BPD/DS and experienced 50–65.3%EWL at 3 months and 50.1–79.1%EWL at 12 months. Patients with initial RYGB underwent GJ revision for pouch or GJ abnormalities. For those without anatomic abnormalities, they underwent conversion to distal bypass. At 3 months, %EWL was 36.6 for GJ revision and 37.5% for distal revision.
6. Complications of Revisional Surgery
Revisional bariatric surgery is complex, is technically demanding, and is therefore associated with higher morbidity and mortality. Compared to primary surgery, revisional surgery has been associated with higher rates of postoperative complications, longer operative times, longer hospital stay, conversion to open surgery, readmission, and unplanned admission to the critical care unit. In comparing primary versus revisional RYGB, revisional surgery was associated with higher rates of leak, hemorrhage, wound infection, stricture, ulcer, perforation, and hernia. A single-center retrospective study analyzed complications after revisional surgeries performed at their center for weight regain between 2012 and 2015. Of 84 patients, 43 presented for weight regain (52.4%). Complications included incarcerated ventral hernia following AGB conversion to SG, anastomotic leak and recurrent intussusception following gastro-jejunostomy revision, and stricture and marginal ulcer following AGB conversion to RYGB . In summary, reported complications of revisional bariatric surgery are:
• Hernia.
• Anastomotic leak.
• Stricture.
• Marginal ulcer.
• Wound infection.
• Hemorrhage.
• Perforation.
• Obstruction.
Conclusion
Weight regain after primary bariatric surgery is multifactorial. It is imperative to establish guidelines for classifying weight gain in order to guide subsequent intervention and thus to aid bariatric teams internationally in the management of this clinical entity. Revisional surgery has been shown to be a successful treatment option for patients presenting with weight gain, with rates of weight loss nearing those seen after primary surgery. Furthermore, the importance of revisional surgery lies in its ability to readdress many of the obesity-related comorbidities which prompted the primary procedure. When indicated, it is important to tailor the type of revisional surgery to each patient. Although Roux-en-Y gastric bypass remains the most common type of revisional surgery after primary surgery of any type, duodenal switch is emerging as the revision procedure of choice for superobese patients and patients with failed sleeve gastrectomy secondary to weight regain in the absence of reflux symptoms.
Revisional Surgery for Weight Regain
- Introduction
Revisional bariatric surgery is a weight loss surgery for people who have not lost enough weight or have regained weight after their first bariatric surgery. It is a complex and technically demanding procedure, but it can be a successful treatment option for patients with weight regain.
- Causes of Weight Regain
There are many factors that can contribute to weight regain after bariatric surgery, including:
* Lack of adherence to dietary recommendations
* Hormonal/metabolic imbalance
* Mental health
* Physical inactivity
* Anatomic/surgical factors
* Medications
- Preoperative Evaluation
Before revisional surgery, patients will undergo a thorough evaluation to determine if they are eligible for the procedure. This evaluation will include a medical history and physical exam, as well as blood tests, imaging studies, and a psychological evaluation.
- Selecting the Type of Revisional Surgery
The type of revisional surgery that is best for a patient will depend on a number of factors, including the type of primary surgery they had, the cause of their weight regain, and their overall health. Some of the most common types of revisional surgery include:
* Roux-en-Y gastric bypass (RYGB)
* Sleeve gastrectomy (SG)
* Biliopancreatic diversion with duodenal switch (BPD/DS)
* Single anastomosis gastric bypass (OAGB)
* Sleeve gastrectomy with duodenal switch (SADI-S)
- Weight Loss Following Revisional Surgery
Weight loss after revisional surgery can be significant. In one study, patients who underwent revisional surgery for weight regain lost an average of 50–65.3% of their excess weight after 3 months and 50.1–79.1% of their excess weight after 12 months.
- Complications of Revisional Surgery
Revisional surgery is more complex and technically demanding than primary bariatric surgery, and therefore carries a higher risk of complications. Some of the most common complications of revisional surgery include:
* Hernia
* Anastomotic leak
* Stricture
* Marginal ulcer
* Wound infection
* Hemorrhage
* Perforation
* Obstruction
- Conclusion
Revisional bariatric surgery can be a successful treatment option for patients with weight regain. However, it is important to carefully consider the risks and benefits of the procedure before making a decision. Patients should also work closely with their healthcare team to choose the best type of revisional surgery for them and to prepare for the procedure and its aftermath. Revisional bariatric surgery is a complex and technically demanding procedure, but it can be a successful treatment option for patients with weight regain. It is important to work closely with your healthcare team to determine if you are eligible for the procedure and to choose the best type of surgery for you.
The Stoic Surgeon: Drawing Inspiration from Marcus Aurelius in Medical Practice
Introduction
The practice of medicine and surgery, while profoundly rewarding, can also be challenging and emotionally demanding. In these moments, many professionals seek guidance and inspiration to navigate the inherent difficulties in human healthcare. A rich source of timeless wisdom can be found in the words of the philosopher-emperor Marcus Aurelius, whose Stoic teachings resonate powerfully in the context of contemporary medicine. Let’s explore how Marcus Aurelius’s ideas can illuminate and fortify medical and surgical practice.
Development
- “What we control is what we calmly accept.” – In moments of uncertainty and pressure in the operating room, the serene acceptance of circumstances is crucial for maintaining composure and focus.
- “Do not expect the doctors to do everything for you.” – Marcus Aurelius reminds us of the importance of recognizing our own limitations. Collaboration between doctor and patient is essential for effective treatment.
- “Pain is inevitable. Suffering is optional.” – When dealing with patients in painful situations, it’s vital to remember that our role extends beyond physical treatment to emotional support and alleviating suffering.
- “Doing what needs to be done when it needs to be done, to the best of our ability, is already enough.” – In a profession as demanding as medicine, it’s vital to remember that every effort dedicated to patient care is valuable and meaningful.
- “What is morally right is more important than what is legally right.” – In some situations, it may be necessary to make decisions that go beyond protocol, aiming for the best interest of the patient.
- “To wait is harmful. Not to wait is necessary.” – Readiness and agility in making medical decisions can be crucial in emergency situations.
- “Time is a river, and facts are currents; we cannot escape, we cannot choose where we will go, nor when, nor how.” – This reflection reminds us of life’s impermanence and the importance of cherishing every moment in medical practice.
- “Man’s health is our treasure.” – Marcus Aurelius emphasizes the valuable responsibility doctors have in preserving and restoring individuals’ health.
- “Every day that dawns brings some evil, which we must accept, for no day will be without it.” – Recognizing that challenges are part of the medical journey allows professionals to face them with courage and determination.
- “Where is the good, if not in doing good to those in need?” – The practice of medicine is a living testament to compassion and altruism. Through it, doctors have the opportunity to demonstrate the true essence of human kindness.
Conclusion
Just as Marcus Aurelius faced the challenges of the Roman Empire with serenity and wisdom, the modern surgeon finds in his words a guide to practicing medicine with virtue and humanity. By uniting technical skill with Stoic philosophy, the surgeon becomes not only a master of their craft but also an example of Stoic activity for the entire medical community. May each operating room be a temple of virtue and care, where the legacy of Marcus Aurelius lives on through the hands of Stoic surgeons.

The Art of Healing: Wisdom from Opus Dei for Medical Professionals
1. “Work is a path to holiness.” – Just as in Opus Dei, where work is considered a means to grow closer to God, in the field of medicine, every interaction with a patient, every diagnosis, and every surgery is an opportunity to serve and make a positive impact.
2. “In your daily work, offer up small sacrifices for your patients.” – Much like Opus Dei encourages offering up small sacrifices for spiritual growth, in medicine, dedicating extra time, attention, or effort for a patient’s well-being can be a powerful form of compassion.
3. “Strive for excellence in your field; it is a reflection of your dedication to your patients.” – Opus Dei emphasizes the pursuit of excellence in one’s profession as a form of service to God. Similarly, in medicine, continuous learning and improvement directly benefit the quality of care provided to patients.
4. “Treat each patient with dignity, respect, and kindness.” – This fundamental principle aligns with Opus Dei’s emphasis on valuing every individual. In medicine, showing compassion and empathy is as important as clinical expertise.
5. “Pray for guidance in making difficult decisions.” – Just as Opus Dei encourages seeking spiritual guidance in challenging situations, in medicine, turning to one’s faith for moral and ethical dilemmas can provide clarity and a sense of purpose.

6. “Foster a culture of trust and collaboration among colleagues.” – Opus Dei emphasizes unity and mutual support among its members. Similarly, in the medical field, teamwork and open communication are vital for providing the best possible care for patients.
7. “Never underestimate the power of a kind word or gesture.” – Small acts of kindness, like those encouraged in Opus Dei, can have a profound impact on a patient’s experience and recovery in the medical setting.
8. “Cultivate a spirit of gratitude for the opportunity to serve others.” – Recognizing the privilege of being able to heal and alleviate suffering is a perspective shared by Opus Dei and medical professionals alike.
9. “Strive for balance between professional and personal life.” – Opus Dei emphasizes the importance of a balanced life. In medicine, maintaining a healthy work-life balance is crucial for sustaining a long and fulfilling career.
10. “Embrace the challenges of medicine as opportunities for growth and service.” – Opus Dei encourages embracing life’s challenges as a means of spiritual growth. Likewise, in medicine, facing the complexities and difficulties of healthcare with dedication and compassion can lead to profound personal and professional development.
Incorporating these principles from Opus Dei into the practice of medicine can not only enhance the quality of care provided but also contribute to a more compassionate and fulfilling healthcare experience for both practitioners and patients alike.
Wasteland in the Operating Room: Reflections on Medical Practice
“April is the cruellest month” – This T.S. Eliot verse may, in a way, resonate in the hallways of hospitals. April, for many, signifies the onset of spring, but in the operating room, it can symbolize the start of intense challenges.
“Mixing memory and desire” – As surgeons, we are constantly challenged to balance past experiences with future aspirations. The memory of previous cases shapes our desire to refine techniques and achieve better outcomes for our patients.
“Spring is dead, buried is hope” – Post-operative desolation often mirrors this verse. Surgery is at times a painful and grueling process, but it is in these moments that our hope for recovery and healing remains steadfast.
“Here is no water but only rock” – The operating room, with its sterile white surfaces, may seem devoid of life. Yet, it is here that life is preserved and restored, where the line between mortality and survival is drawn with surgical precision.
“Shaking the bitter foam of past experience” – As healthcare professionals, we are compelled to learn from each procedure. Every case is an opportunity for refinement, a chance to perfect our skills and grasp the intricacies of medicine.
“I cannot help but think/ This that we believe to be the end is only the beginning” – When the scalpel glides, when the sutures are closed, it is crucial to remember that the conclusion of a surgery is just the start of the patient’s recovery process. Hope is renewed in the promise of a healthier tomorrow.
“In the waiting room, gazing at the sky” – Even in moments of pre-operative anxiety, we look to the future with optimism. We know that medicine is a journey of challenges and triumphs, and each patient is a star in the sky of our professional experience.
“Here we are, contemplating the horizon” – In our medical careers, we face each day with determination and resilience. We are always keeping an eye on the horizon, seeking new techniques, advancements, and opportunities to enhance patient care.
“Shantih shantih shantih” – At the end of each procedure, when silence fills the operating room, it is a tranquil reminder that, even amidst complexity and challenges, medicine is ultimately an act of compassion and healing.
Just as in T.S. Eliot’s “The Waste Land,” in medicine and surgery, desolation and hope intertwine. Each procedure is an opportunity for learning and renewal. Through dedication and a commitment to patient well-being, we find our “shantih,” the peace we seek throughout this medical journey.

Liderança Inspiradora de Lord Nelson: Lições para Cirurgiões Contemporâneos
A história nos presenteou com inúmeros líderes notáveis, cujas habilidades e características têm inspirado gerações ao longo dos séculos. Um desses ícones é Lord Nelson, o lendário almirante britânico do século XVIII, conhecido por sua coragem e maestria tática nas batalhas navais. Surpreendentemente, as características de liderança de Lord Nelson têm aplicações valiosas mesmo na prática contemporânea da cirurgia. Neste artigo, exploraremos algumas dessas qualidades e como nós cirurgiões podemos aplicá-las para alcançar o sucesso em nossas batalhas cirúrgicas.
“Eu sou inabalável em minha determinação, como nunca estive em minha vida, desde que coloquei o pé no convés de um navio.”
1. Determinação Inabalável: Lord Nelson era conhecido por sua determinação inabalável em alcançar seus objetivos. Ele enfrentou inúmeras adversidades e desafios durante suas batalhas navais, mas nunca desistiu diante das dificuldades. Os cirurgiões contemporâneos podemos aprender com essa qualidade, mantendo-se resilientes diante de obstáculos, buscando soluções mesmo nas situações mais desafiadoras e garantindo o melhor atendimento possível para nossos pacientes. Durante a Batalha do Nilo, em 1798, Nelson enfrentou condições adversas quando a frota britânica ficou encalhada em bancos de areia. Enfrentando uma situação aparentemente desesperadora, ele permaneceu determinado a superar os obstáculos para alcançar a vitória. Com habilidades táticas brilhantes, Nelson conseguiu finalmente manobrar sua frota para fora dos bancos de areia e alcançar uma vitória decisiva sobre a frota francesa.
“Eu sempre fui um covarde em tudo, exceto nesta profissão.”
2. Coragem sob Pressão: Durante a Batalha de Copenhague, em 1801, Nelson foi ordenado a se retirar pelo comandante em chefe, mas ele ignorou a ordem e ergueu o telescópio em seu olho cego para afirmar que não conseguia ver o sinal. Ele então liderou seu esquadrão em um ataque corajoso, superando uma poderosa defesa dinamarquesa. Sua determinação e coragem sob pressão foram fundamentais para a vitória britânica. Em meio ao caos e perigo das batalhas navais, Lord Nelson demonstrou coragem excepcional. Seu exemplo inspirador pode nos lembrar da importância de permanecermos calmos e focados, mesmo durante procedimentos complexos ou emergências médicas. A coragem para tomar decisões rápidas e precisas pode fazer a diferença entre a vida e a morte em uma sala de cirurgia.
“A vontade não pode ser chamada de coragem, mas dever, o resultado da força da mente; e qualquer um que possua esse poder, quando chega a hora de agir, encontrará a coragem que necessita.”
3. Liderança Carismática: Lord Nelson conquistou o respeito e a admiração de sua tripulação com sua liderança carismática. Durante a Batalha do Nilo, quando o perigo era iminente e a tripulação estava nervosa, Nelson subiu ao convés e enfrentou corajosamente o inimigo, encorajando seus marinheiros a seguirem seu exemplo. Sua presença inspiradora foi fundamental para manter o moral elevado e motivar sua equipe a lutar com determinação. Lord Nelson era conhecido por sua liderança carismática e inspiradora. Ele conquistou o respeito e a lealdade de sua tripulação com sua empatia e capacidade de se conectar emocionalmente com seus marinheiros. Os cirurgiões contemporâneos também podem se beneficiar ao desenvolver uma liderança que inspire confiança e motivação em suas equipes médicas, promovendo um ambiente colaborativo e eficiente.
“Eu planejo que cada homem atue de acordo com o que vê melhor, mas qualquer homem que venha entre as duas frotas, não pode ser errado, portanto, não pode ser chamado de insubordinação, mas uma obediência em que cada oficial julga por si mesmo o que é melhor a ser feito.”
4. Capacidade de Adaptação: Durante a Batalha de Trafalgar, a estratégia inicial de Nelson era enfrentar a frota inimiga de maneira mais tradicional. No entanto, quando percebeu que a formação inimiga era mais forte do que o esperado, ele rapidamente adaptou sua tática e implementou a “manobra de Nelson”, cortando a linha inimiga e concentrando seu poder de fogo para alcançar a vitória. Durante suas batalhas, Lord Nelson enfrentou situações imprevistas e mudanças de planos. Sua capacidade de adaptação e flexibilidade permitiu-lhe ajustar suas estratégias conforme necessário. Na cirurgia contemporânea, os profissionais também devem ser ágeis e adaptáveis, prontos para responder a mudanças repentinas durante procedimentos cirúrgicos complexos ou emergências médicas.
“Seja qual for a estação em que você estiver, carregue consigo o pensamento de que todos os olhos estão voltados para você. Comande a si mesmo sempre que for o exemplo de todos os outros.”
5. Comunicação Efetiva: Lord Nelson era conhecido por sua habilidade de comunicação clara e direta com sua equipe. Antes da Batalha do Nilo, ele escreveu uma carta aos marinheiros enfatizando a importância da vitória e oferecendo palavras de encorajamento. Sua mensagem sincera e motivadora demonstrava sua preocupação com o bem-estar de sua tripulação e ajudou a criar um senso de propósito comum entre seus homens. A comunicação efetiva era uma das principais características de liderança de Lord Nelson. Ele sabia como transmitir suas ordens com clareza e também valorizava o feedback de sua equipe. Cirurgiões contemporâneos podem seguir esse exemplo, enfatizando a comunicação transparente com seus colegas e pacientes para garantir que todos estejam alinhados quanto aos procedimentos e tratamentos.
Em suma, a história de Lord Nelson nos ensina que as características de liderança transcendem as épocas e têm aplicação valiosa em diversas áreas, incluindo a medicina. Ao incorporar a determinação, coragem, carisma, adaptação e comunicação efetiva de Lord Nelson, podemos nos inspirar e tornar líderes excepcionais em nossas práticas médicas, promovendo um atendimento de qualidade e impactando positivamente a vida dos pacientes. A frase ‘A Inglaterra espera que cada um faça sua parte’ tornou-se um lema inspirador e atemporal, capturando a essência da liderança de Lord Nelson na Batalha de Trafalgar. Essas palavras ecoam através dos séculos, lembrando-nos da importância da responsabilidade individual e do trabalho em equipe para alcançar o sucesso em qualquer empreendimento. Assim como os marinheiros da frota britânica foram impulsionados por esse chamado à ação, também podemos aplicar essa mensagem em nossas próprias vidas e carreiras. Como cirurgiões, somos lembrados da nossa obrigação de desempenhar cada procedimento com diligência e dedicação, e ao mesmo tempo, liderar nossas equipes com empatia e coragem. A mensagem de Lord Nelson nos inspira a superar desafios, enfrentar pressões e trabalhar juntos para alcançar os melhores resultados possíveis em nossas práticas médicas. Ao seguir esse exemplo atemporal de liderança podemos oferecer o melhor atendimento possível aos nossos pacientes e à sociedade.
Ortodoxia Cirúrgica
Embora “Ortodoxia” seja uma obra filosófica e teológica escrita por G.K. Chesterton, suas ideias podem ter algumas aplicações interessantes e reflexivas no cotidiano da cirurgia. Claro que a relação direta pode não ser evidente, mas certos princípios filosóficos podem fornecer perspectivas valiosas para os cirurgiões. Aqui estão algumas maneiras pelas quais as ideias de “Ortodoxia” podem ser aplicadas no contexto cirúrgico:
- Valorizar o pensamento paradoxal: A cirurgia é uma disciplina complexa e muitas vezes ambígua, onde os médicos devem tomar decisões cruciais em situações desafiadoras. Valorizar o pensamento paradoxal pode ajudar os cirurgiões a considerar opções diversas e até opostas antes de tomar decisões importantes.
- Reconhecimento da complexidade humana: Chesterton destaca a importância de compreender a natureza complexa da realidade. No contexto cirúrgico, isso se traduz em tratar cada paciente como um indivíduo único, com suas próprias circunstâncias médicas, emocionais e sociais. Isso pode ajudar os cirurgiões a abordar cada caso com uma mente aberta e livre de preconceitos.
- Equilíbrio entre tradição e inovação: Assim como Chesterton valoriza a tradição cultural, os cirurgiões podem se beneficiar de uma abordagem equilibrada entre as técnicas tradicionais e as inovações médicas. Combinar o conhecimento estabelecido com as mais recentes pesquisas e tecnologias pode levar a melhores resultados para os pacientes.
- Enfrentar a incerteza: A cirurgia pode ser imprevisível, e os resultados nem sempre são garantidos. A ortodoxia de Chesterton nos encoraja a aceitar a incerteza e a enfrentar os desafios com coragem e confiança. Essa mentalidade pode nos ajudar a enfrentar situações complicadas e se adaptar a cenários imprevistos.
- Importância da ética e moralidade: Chesterton enfatiza a importância da moralidade e da virtude. Na cirurgia, esses princípios são essenciais para garantir a melhor qualidade de atendimento ao paciente, respeitando sempre a dignidade e os direitos humanos.
- Valorizar a imaginação: A imaginação é uma parte essencial do trabalho cirúrgico, permitindo aos médicos visualizar procedimentos, simular situações e pensar em soluções criativas. A capacidade de imaginar possibilidades pode ajudar os cirurgiões a planejar cuidadosamente cada intervenção.
Embora “Ortodoxia” não tenha sido escrito com o objetivo específico de se aplicar à cirurgia, as ideias e princípios contidos na obra podem inspirar uma reflexão mais profunda e nos guiar de forma mais consciente, sensível e equilibrada.
As virtudes cardinais cirúrgicas
A prática cirúrgica é uma forma de arte que exige habilidade técnica e precisão, mas vai além disso. Os cirurgiões não apenas dominam as técnicas e procedimentos, mas também são desafiados a aplicar virtudes cardinais em cada etapa do ato operatório. A diérese, exérese, hemostasia e síntese, as quatro fases cruciais da cirurgia, podem ser vistas como um reflexo das virtudes cardinais: prudência, justiça, fortaleza e temperança. Vamos explorar como essas virtudes se manifestam na rotina de um cirurgião comprometido com o bem-estar dos pacientes.
Diérese (A Prudência como Guia) : A primeira etapa da cirurgia, a diérese, é o momento em que o cirurgião realiza uma incisão precisa para acessar o local a ser tratado. A prudência, virtude da sabedoria prática, entra em cena através do domínio da anatomia. O cirurgião deve avaliar cuidadosamente cada caso, analisar os riscos e tomar decisões fundamentadas. A prudência orienta a escolha das melhores abordagens cirúrgicas, levando em consideração a saúde geral do paciente, suas necessidades individuais e o objetivo final da intervenção.
Exérese (A Justiça na Busca pelo Equilíbrio): Na fase de exérese, o cirurgião remove tecidos ou estruturas comprometidas pela doença. Aqui, a justiça desempenha um papel essencial. O cirurgião deve agir com equidade, buscando remover apenas o que é necessário, sem excessos ou negligências. A justiça implica em tratar cada paciente com equidade, respeito e imparcialidade, levando em consideração os melhores interesses do indivíduo e buscando o bem comum. É um compromisso em garantir que o procedimento cirúrgico seja realizado com integridade e sempre em benefício do paciente.
Hemostasia (A Fortaleza para Enfrentar Desafios) : Durante a fase de hemostasia, o cirurgião aplica técnicas para controlar o sangramento e garantir um campo cirúrgico claro. Nesse momento, a fortaleza se faz presente. A cirurgia pode apresentar situações imprevistas, complicações ou momentos de grande pressão. A fortaleza permite ao cirurgião manter-se firme, agir com coragem diante de adversidades e tomar decisões rápidas, mas sábias, para proteger a vida e o bem-estar do paciente. A fortaleza é a virtude que impulsiona o cirurgião a enfrentar desafios com firmeza e superar obstáculos através de uma alma inabalável, mantendo durante todo o procedimento uma determinação com o melhor prognóstico do paciente.
Síntese (A Temperança na Busca do Equilíbrio Final) : A última etapa, a síntese, envolve a restauração da integridade do tecido por meio de suturas ou outros meios. Nesse momento, a temperança se revela. A temperança é a virtude que permite ao cirurgião exercer controle e moderação, evitando excessos e buscando a harmonia. A escolha adequada do material de sutura, a técnica precisa e o cuidado meticuloso são fundamentais. A temperança assegura que a finalização do ato operatório seja feita com prudência, justiça e fortaleza, considerando o bem-estar a longo prazo do paciente.
Logo, podemos concluir que a prática da cirurgia transcende a habilidade técnica e exige o cultivo das virtudes cardinais. A prudência, a justiça, a fortaleza e a temperança tornam-se guias éticos para o cirurgião comprometido com o cuidado ao paciente. A diérese, exérese, hemostasia e síntese, cada uma refletindo uma virtude cardinal, são etapas cruciais em busca da excelência médica. Quando o cirurgião incorpora essas virtudes em sua rotina, ele se torna não apenas um técnico habilidoso, mas um verdadeiro médico que busca o bem-estar e a cura integral do paciente. A arte da cirurgia, assim, se revela não apenas como uma expressão de destreza manual, mas como uma expressão do cuidado compassivo e virtuoso que o médico oferece ao paciente.
10 Anatomical Aspects for Prevention the Bile Duct Injury
Essential aspects to visualize and interpret the anatomy during a cholecystectomy:
1. Have the necessary instruments for the procedure, with adequate positioning of the trocars and a 30-degree optic.
2. Cephalic traction of the gallbladder fundus and lateral traction (pointing to the patient’s right shoulder), to reduce redundancy of the infundibulum.
3. Puncture and evacuation of the gallbladder to improve its retraction, in cases where traction cannot be performed easily (acute cholecystitis).
4. Lateral and caudal traction of the infundibulum, for correct exposure of Calot’s triangle, exposing the CD and artery.
5. “Critical view of Safety” to avoid misidentification of the bile ducts, ensuring that only two structures (CD and artery) are attached to the gallbladder. For this, they must be dissected separately, and the proximal third of the gallbladder must be moved from its fossa, to ensure that there is no anatomical variant there.
6. Systematic use of intraoperative cholangiography. Ideally by transcystic route or possibly by a puncture of the gallbladder.
7. Ligation of the cystic duct with knots (“endoloop”) to prevent migration of metallic clips that could condition a postoperative leak.
8. In case of severe inflammation of the gallbladder pedicle, with its retraction or lack of recognition of cystic structures, a subtotal cholecystectomy might be indicated.
9. In case of hemorrhage, avoid indiscriminate clip placement and or blind cautery. Opt for compressive maneuvers and, once the bleeding site has been identified, evaluate the best method of hemostasis.
10. If the surgeon is not able to resolve the injury caused, it is always better to ask for help from a colleague, and if necessary, to refer the patient to a specialized center.
#SafetyFirst
The main goal in the postoperative management of BDI is to control sepsis in the first instance and to convert an uncontrolled biliary leak into a controlled external biliary fistula to achieve optimal local and systemic control. Definitive treatment to re-establish biliary continuity will be deferred once this primary goal is achieved and should not be obsessively pursued in the acute phase. The factors that will determine the initial presentation of a patient with a BDI in the postoperative stage are related to the time elapsed since the primary surgery, the type of injury, the mechanism of injury, and the overall general condition of the patient.
Sobre o FUTURO
Aos cinco anos, o que você queria ser quando crescesse?
Médico.
Tudo começou quando eu tinha por volta de 4 – 5 anos e após um acidente domiciliar, precisei passar por uma cirurgia na mão. A forma como aquele profissional que nos atendeu acalmou a angústia dos meus pais e tratou com habilidade o ferimento me marcou profundamente. Apesar de não ter ideia do que isso significaria na minha jornada futura, aquele sentimento de ação e resolução se tornou uma paixão que me acompanha até hoje.

Anatomia Cirúrgica da REGIÃO INGUINAL
A hérnia inguinal é uma condição comum que ocorre quando um órgão abdominal protraí através de uma fraqueza na parede abdominal na região abdominal. O orifício miopectineal é a principal área de fraqueza na parede abdominal onde a hérnia inguinal pode se desenvolver. O conhecimento da anatomia da parede abdominal é importante para entender a patofisiologia da hérnia inguinal e para ajudar no diagnóstico e tratamento dessa condição médica comum.
GASTROSTOMY: INDICATIONS, TECHNICAL DETAILS AND POSTOPERATIVE CARE.
Ozimo Pereira Gama Filho
Adjunct Professor at the Federal University of Maranhão
No conflict of interest
- INTRODUCTION
- HISTORICAL ASPECTS
- ANATOMICAL FUNDAMENTALS
- INDICATIONS
- TYPES & TECHNIQUES
- ADVERSE EVENTS
- CUSTO RATIO x EFFECTIVENESS
- CONCLUSIONS
SUMMARY
In the last decade, the use of gastrostomies has been widely indicated as the preferred form of access to the gastrointestinal tract for feeding in chronic conditions and during recovery from acute conditions such as trauma. Together with this increase in indications, new techniques have been developed that have made gastrostomies simpler and less risky. From the classical technique of Stamm performed by laparotomy, two new alternatives that do not require laparotomy emerged: percutaneous endoscopic gastrostomy (PEG) and fluoroscopy gastrostomy. Its main benefit is to avoid a laparotomy, with less associated postoperative pain and earlier return of gastrointestinal function. Although peg is currently widely accepted as the insertion technique of choice due to its simplicity and efficacy, there are patients who are not candidates for an endoscopic approach. In this article we seek to clarify the indications, technical aspects and perioperative care of patients undergoing gastrostomy.
Keywords: Surgical Procedures; Ostomies; Gastrostomy.
Area of Knowledge: General Surgery
- INTRODUCTION
The main indication for enteral or parenteral feeding in the perioperative period is the provision of nutritional support to supply the metabolism of patients with inadequate oral intake. Enteral feeding is the preferred method in relation to parenteral feeding in patients with gastrointestinal dysfunction in the perioperative period due to the inherent risks associated with parenteral nutritional support, such as: infectious complications of the access routes, higher operational cost, and the inability to parenteral nutrition to provide adequate enteral stimulation and subsequent involvement of the intestinal defense barrier [1,2]. In addition, enteral feeding may decrease the risk of bacterial translocation and corresponding bacteremia [3]. Gastric nutritional support is the most common type used. Access to insert the gastrostomy probe can be achieved using endoscopy, interventional radiologia, or surgical techniques (open or laparoscopic). However, since its description in the 1980s [4], percutaneous endoscopic gastrostomy (PEG) is currently considered the method of choice for medium and long-term enteral support.
1.1 Objective: This article reviews the current knowledge about GOSTROSTOMIA in the medical literature, emphasizing the technical and perioperative aspects.
- HISTORICAL ASPECTS
In 876, Verneoil [5] successfully made the first gastrostomy in humans. Since then, several technical modifications have been suggested, such as witzel’s technique in 1891, in which a subseroso tunnel is made on the probe [6]. Stamm, in 1894 [7], described one of the most performed techniques today and in the history of surgical gastrostomy, which consists in the making of suture in a pouch to invaginate the probe inserted into the stomach [8]. In 1980, percutaneous endoscopic gastrostomy was described by Gauderer et al. [4] , which transformed the technique of making gastrostomy.
- ANATOMICAL FUNDAMENTALS
The stomach is a J-shaped dilated cylindrical organ that rests in the left epigastric and hypochodrial region of the abdomen at the level of the first lumbar vertebra. It is previously limited by the left hemidiaphragm, the left lobe of the liver and a triangular portion of the anterior abdominal wall. Subsequently, the pancreas, left kidney and adrenal delimit the stomach. The spleen is posterolaterally and the transverse colon is inferior. It is fixed at two points of continuity: gastroesophageal, superiorly and the duodenal, retroperitoneally. Its ligament attachments also help you in fixation to adjacent organs: gastrophemic (diaphragm), hepatogastric or minor omentum (liver), gastrosplenic or gastrolienal (spleen), and gastrocholic or omentum major (transverse colon). The anatomical regions of the stomach can be distinguished as this: começa superiorly in the continuity of the abdominal part of the esophagus and dthe gastroesophageal junction, the cardiac part of the stomach. Soon below this portion, lies the bottom of the stomach that expands to the left extending above thegastroesophageal junction, forming an acute angle with the distal esophagus known as cardiac notches. The body s andextends as a distensible reservoir and forms a medial edge called the smallest curvature to the right and a side edge called the largest curvature on the left. The gastric den of the stomach is not anatomically distinguishable, but it is estimated to be a region of the angular isis along the distal minor curvature to a point along a lower line to the distal major curvature. It thus ends bymouthing r into the pyloric canal limited by the pyloric sphincter, a palpable thickened ring of muscle that is continuous with the first part of the duodenum.
- INDICATIONS
Gastrostomy is used in the following situations:
- Gastric decompression: can be obtained by means of temporary gastrostomy, occasionally recommended, as a complement to large abdominal operations for which gastric stems, prolonged “adynamic ileus” and digestive fistulas are foreshadowed.
- Nutritional Support: b.1 Temporary; indicated when access to the digestive tract is temporarily impaired for recovery and maintenance of nutritional status (E.g. CEsophageal EC); b.2 Definitive; as palliative therapy in patients with unresectable malignant neoplasia of the head and neck, as wellas n degenerative neurological diseases that lead to irreversible disorders of deglutition.
However, the decision to perform a gastrostomy, as well as its route (surgical, radiological or endoscopic) should be individualizedaccording to the needs, diagnosis, life expectancy of the patient and the available hospital logistics. The objective is not only to optimize perioperative recovery, to improve survival and nutritional status of the patient, but also to promote quality of life, which is not necessarily correlated with nutritional improvement only [9]. Therefore, the appropriate indication, like any other surgical intervention, must be clearly establishedand informed before it is performed. Some of the absolute contraindications of gastrostomy are summarized in Table 1. In addition to absolute contraindication conditions, other situations such as the presence of non-obstructive oromyctological oresophageal malignancy, hepatomegaly, splenomegaly, peritoneal dialysis, portal hypertension with gastric varicose veins, and a history of partial gastrectomy are also considered relative contraindications.
| ABSOLUTE CONTRA – INDICATIONS |
| Coagulopatia Severa (INR > 5, Plaquetas < 50.000 e TPT > 50s) |
| Hemodynamic Instability |
| Septic Shock |
| Refractory Ascites |
| Peritonitis |
| Dermatological infection in the upper abdomen |
| Carcinomatose Peritoneal |
| Interposition of organs that prevent gastric access |
| History of Total Gastrectomy |
| Stenosis or Pyloric Obstruction |
| Severe gastroparesis, in cases of indication for nutritional support |
| Absence of Informed Consent |
- TYPES & TECHNIQUES
Currently there are three techniques for performing gastrostomy: radiological, through percutaneous gastrostomy by fluoroscopy, percutaneous endoscopic gastrostomy (PEG) and surgical gastrostomy. Due to the didactic characteristics of this material, we will focus on endoscopic and surgical gastrostomy , which becomes the main option in the following situations: 1) when the patient will already undergo a laparotomy due to some abdominal condition ; 2) impossibility of performing gastroscopy to perform gastrostomy endoscopic percutaneous (PEG) ; 3) in case of peg technical failure; 4) unavailability of resources for the preparation of PEG or percutaneous gastrostomy by fluoroscopy.
- ENDOSCOPIC PERCUTANEOUS GASTROSTOMY
The informed consent form must be obtained from patients or their legal representatives. Patients should fast for a minimum of 8 hours and receive prophylactic antibiotics one hour before proceeding and intravenous administration of 1-2 g of cefazolin is recommended. The technique introduced by Gauderer et al [4] is the most used technique to insert the PEG gastrostomy probe. In this method, a guide wire is used, inserted in the distal gastric chamber through a needle puncture n to the anterior abdominal wall. This guide wire is then seized endoscopically with a handle and then removed through the esophagus and mouth. Subsequently, the guide wire is fixed to the end of the gastrostomy probe and then pulled from the mouth to the esophagus, stomach and then out to the abdominal wall, where it will be fixed.
- SURGICAL GASTROSTOMY
Surgical gastrostomy can be performed in two ways: 1) via laparotomy – the predominant form; and 2) laparoscopic approach. The preparations are the same as the endoscopic pathway.
5.2.1. GASTROSTOMIA At STAMM
After adequate asepsis and antisepsis, with the patient under anesthesia and in horizontal dorsal decubitus, the technical steps are as follows: 1. Median laparotomy (supraumbilical median incision); 2. Identification of the gastric body; 3. Stomach hold with Babcock tweezers (to evaluate the approach of the stomach to the peritoneum); 4. Suture in pouch (circular area of 2cm) – atraumatic absorbable thread; 5. Section of the stomach wall (0.5cm) – (incision with scalpel or Electrocautery in the center of the suture, of sufficient size, for the placement of a probe with 20 to 26 French); 6. Placement of the Gastrostomy probe in the extension of 5-6 cm, followed by suture closure in a pouch); 7. Tie the suture threads in a pouch around the probe; 8. Apply a second suture in a pouch 1cm above the first (seromuscular stitches); 9. Externalization of the probe by counter opening on the left flank; 10. Fix the stomach wall to the abdominal wall in 4 cardinal points (external ration with the two Kocher tweezers used for grip of the alba line and against traction by means of the index fingers of the wall of the left hipochondrio to approach the parietal peritoneum of the gastric wall); 11. Fixation of the probe to the skin (point with nonabsorbable wire); 12. Closure of the abdominal wall (synthesis of the wall with approximation of the alba thread by continuous suture with monofilament thread 1-0 or 2-0 and of the skin with separate points of nylon 3-0); 13. Dressing.
5.2.1 GASTROSTOMIA EM WITZEL
The initial technical steps from gastrostomy to Witzel are like those of gastrostomy to Stamm, including fixation of the probe to the stomach by a pouch suture. Then, the probe is placed on the gastric wall and a tunnel of 8-10 cm is made by seromuscular suture (continuous or with separate points of absorbable or nonabsorbable thread) covering it and externalization is performed by counteropening.
- ADVERSE EVENTS
According to the literature, the rate of complications for different procedures varies due to the heterogeneity of the samples evaluated. For surgical gastrostomy, the reported complication rates are between 1% and 35%, while for percutaneous radiological gastrostomy it is 3% to 11%, and for percutaneous endoscopic, 17%–32%, the main related adverse event is surgical site infection [10, 11]. Although considered a basic procedure, gastrostomy is associated with an extensive list of related technical complications, care and use of the probe. Serious problems related to the technique include separation of the stomach from the abdominal wall (leading to peritonitis), separation of wounds, hemorrhage, infection, lesion of the posterior gastric wall or other organs, and placement of the tube in an inappropriate place of gastric position. Separation of the stomach from the abdominal wall usually occurs due to inadvertent and premature displacement of the tube, particularly with balloon-like devices, or a rupture during a catheter change. It requires immediate attention, being treated with laparotomy, although in selected cases laparoscopic correction is possible. Most complications can be avoided with the careful choice of the type of procedure, from the appropriate ostomy device, considering it an important intervention and using meticulous technique with the proper approximation of the stomach to the abdominal wall and outflow of the probe through a counter-incision (in conventional procedures), thus avoiding probes in the midline or awfully close to the costal edge.
- COST VS. EFFECTIVENESS
A recent study [12] compared the cost associated with the different gastrostomy techniques, and the results of the evaluation showed variable the benefits of each of the individual percutaneous procedures, indicating that surgical gastrostomy was the onerous mais of the three modalities due to higher costs, complications, and recovery time, as well as the endoscopic technique presenting the cost effectiveness ratio.
- CONCLUSIONS
Despite the technique employed, the decision to performa gastrostomy is not based only on the patient’s survival expectancy, because the adequate indication provides a better quality of life even when the survival of the patient after the procedure is severely limited. Therefore, understanding of techniques, indications, complication rates is essential to guide the surgical team in the scope of multidisciplinary care, as well as the education of patients and their caregivers is vital to ensure the correct maintenance of the devices, thus ensuring adequate nutritional intake of the patient and minimizes complication rates.
References
1 Alverdy J, Chi HS, Sheldon GF. The effect of parenteral nutrition in gastrointestinal immunity. The importance of de estimulação enteral. Ann Surg, 1985; 202: 681-684 [PMID:3935061]
2 Deitch EA, Ma WJ, Ma L, Berg RD, Specian RD. Protein malnutrition predisposes to inflammation-induced intestinal origin septic states. Ann Surg, 1990; 211: 560-567; discussion 560-567 [PMID: 2111125]
3 Deitch EA, Winterton J, Li M, Berg R. The intestine as a portal of entry to bacteremia. Role of protein malnutrition. Ann Surg 1987; 205: 681-692 [PMID: 3592811]
4 Gauderer MW, Ponsky JL, Izant RJ. Gastrostomia sem laparotomy: percutaneous endoscopic technique. J Pediatrician Surg, 1980; 15: 872-875 [PMID: 6780678]
5 Anselmo CB, Tercioti Júnior V, Lopes LR, Coelho Neto JS, Andreollo NA. Surgical gastrostomy: current indications and complications in patients of a university hospital. Rev Col Bras Cir. [Internet journal] 2013;40(6). Available in URL: http://www.scielo.br/rcbc
6 Witzel O. For gastric fistula technique. Chir Zbl. 1891;18:601-4.
7 Stamm M. Gastrostomy: a new method. Med News. 1894;65:324.
8 JP grant. Comparison of percutaneous endoscopic gastrostomy com gastrostomia strain. Ann Surg. 1988;207(5):598-603
9 Bannerman E, Pendlebury J, Phillips F, Ghosh S. Cross-sectional and longitudinal study of health-related quality of life after percutaneous gastrostomy. Eur J Gastroenterol Hepatol 2000; 12: 1101-1109 [PMID: 11057455]
10 Möller P, Lindberg CG, Zilling T. Gastrostomy by various techniques: evaluation of indications, outcome and complications. Scand J Gastroenterol. 1999;34(10):1050-4.
11 Clarke E, Pitts N, Latchford A, Lewis S. A major prospective audit of morbidity and mortality associated with food gastrostomies in the community. Clin Nutr. 2017 Apr;36(2):485-490. DOI: 10.1016/j.clnu.2016.01.008. EPub 2016 January 21. PMID: 26874913.
12 Wollman B, D’Agostino HB, Walus-Wigle JR, Easter DW, Beale A (1995) Radiological, endoscopic and surgical gastrostomy: an institutional evaluation and meta-analysis of the literature. Radiology 197: 699–704.