NOTTS: The Operating Room Team

Introduction
“Analysis of medical errors has shown that more than two-thirds involve issues of team communication, and these are contributed to by issues of institutional and team culture. These errors can include missed communication, inaccurate communication, or inability or unwillingness of team members to speak up—all of which can be related to the culture of a team or institution and which are dramatically affected based on the tone and climate set by surgeon leaders, both in and out of the operating room. Every team and institution have a “safety culture”—the attitudes, behaviors, and expectations that affect patient outcomes for good or for ill. There is increasing evidence that this safety culture directly affects both morbidity and mortality. For example, in a study of 31 hospitals in South Carolina, institutional safety culture was directly related to patient death. For every 1-point change (on a 7-point scale) in the hospital-level scores for respect, clinical leadership, and assertiveness, 30-day mortality after surgery decreased from 29% to 14%. In another example, measures of safety culture across 22 hospitals in Michigan directly predicted patient outcomes after bariatric surgery. In that study, when nurses rated coordination of OR teams as acceptable, rather than excellent, serious complications were 22% more likely.
The Operating Room Team
The act of surgery is inherently team-based. Each operation requires the surgeon to work closely and effectively with their assistants, anesthesia providers, nursing staff, surgical technologists, and ancillary staff members to make the OR function. Team members frequently move in and out of the OR, with change of shift or for breaks, and additional team members may be required for specialty or emergency care. The key is to remember that the patient is at the center of the team, thus the phrase “patient-centered care.” Always keep in mind that patient safety and well-being are at the heart of all our efforts. It is especially important that all members of the team have a “shared mental model”—a common understanding of the issues, both medical and logistical, which might affect the course of an operation. This allows for improved efficiency, better situational awareness, and better ability to recognize and respond to issues. Here we describe the individuals commonly encountered in the operating room.
The Surgeons
Every surgical team will consist of an attending surgeon, usually accompanied by one or more assistants. In the learning environment, it is important for the surgeons to discuss roles and responsibilities as well as educational goals for the case, which may vary depending on the level of training and experience of the team members. An important concept in surgical education is “progressive autonomy,” in which learners are allowed to take on more and more responsibility in an operation based on their level of competency. A preoperative discussion between the surgeon and the resident is critical to clear understanding of which parts of the operation the learner can be expected to perform and when the attending might need to take control of the case. It is the responsibility of every member of the surgeon’s team to review the patient’s case in detail to understand their past medical and surgical history, their current disease and how it has been managed to date, relevant medications, and review of all diagnostic studies to anticipate difficulties that may be encountered during the operation. Secondarily, it is incumbent on each member to discuss the case with other members of the team to ensure that all individuals have a shared mental model of the operative plan, the postoperative plan, and any anticipated difficulties. During the operation, the patient is the focus of the team. Each individual is expected to do their part to advance the operation while helping other team members to do the same. Following the operation, it is important to discuss postoperative care such as pain management, dietary restrictions, venous thromboembolism prophylaxis, and the need for new or existing prescription medications.
Scrub Nurse and Circulator
Working closely with every surgical team is the surgical technologist or scrub nurse, often referred to as the “scrub.” This individual will have various levels of training depending on their background—he or she may be a certified surgical technician or a nurse with extra training. The scrub is an integral part of the team as they are responsible for ensuring that all necessary equipment is open or readily available prior to the case starting, anticipating the needs of the surgeon to maximize efficiency, and troubleshooting when there are equipment problems or failures. Depending on the scope of practice as defined by state law and regulations, the scrub may or may not be authorized to assist with limited surgical tasks. It is the responsibility of the surgeon (or surgical resident in their place) to meet with the scrub ahead of time, confirm that all necessary equipment is available, and confirm this during the surgical pause or “time-out.” Doing so will foster a collegial environment while also helping the case run more smoothly. The circulator is typically a nurse by training who is responsible for maintaining the flow of the OR, while the surgeons are sterilely gowned and gloved. It is important (especially for new residents) to introduce yourself to the circulator to open the flow of communication for the day and to give them a baseline understanding of your skill level so that they can assist you as necessary. For example, the circulator may pay extra close attention to the medical student as they don their sterile gown and glove to ensure that they do not break the sterile field. Throughout the case, the circulator works to maintain the flow of the OR. As such, the circulator is not always available to assist in tasks not related to the direct care of the patient.
The Anesthesia Team
Without the anesthesia team, the surgeon cannot operate. The anesthesia team consists of either an attending anesthesiologist who is present for the duration of the case or an anesthesia resident or certified registered nurse anesthetist (CRNA) who is supervised by an attending anesthesiologist who may be overseeing several operations at once. In some states, depending on state law, a CRNA can also practice independently. The anesthesia provider is often helped by an anesthesia technician, much like the surgeon is helped by a surgical technician. The anesthesia team is responsible for providing pain control and sedation, managing the airway, medical and fluid management throughout the case, and monitoring the patient for any physiologic derangements that may or may not be related to the operation at hand. They should meet the patient ahead of time to evaluate for any risk factors such as underlying cardiovascular or pulmonary disease. Communication with the anesthesia team is critical for maintaining the safety and well-being of the patient. One of the most important tools to promote this communication is the surgical pause or “time-out”. Throughout the case, the surgical team must also alert the anesthesia team if they anticipate significant hemodynamic changes for the patient. This can range from events as common as insufflation of pneumoperitoneum during a laparoscopic operation to more uncommon events such as unexpected, significant hemorrhage. Conversely, it is imperative that the anesthesia team communicates with the surgeon about any significant changes in hemodynamic status or about other issues that may impact patient care. Finally, it is important to debrief with anesthesia at the end of the case, to ensure that all members of the team have the same situational awareness and understanding of the patient’s intraoperative course and postoperative plan. This includes issues such as fluid and electrolyte management, expected or potential postoperative issues, and a plan for pain management.
NON-TECHNICAL SKILLS FOR SURGEONS (NOTTS)

“NON-TECHNICAL SKILLS FOR SURGEONS (NOTTS) was developed by a team in Scotland at the University of Aberdeen and funded by the Royal College of Surgeons of Edinburgh and NHS Education for Scotland; lead investigator Steven Yule, PhD, was a part of this team and now brings his experience and expertise to the United States with the Non-Technical Skills Lab at Brigham and Women’s Hospital and Harvard Medical School. NOTSS was developed from the bottom up with a panel of subject matter experts (consultant/attending surgeons/psychologists) in place of adapting an existing framework employed by other industries. The aim of the NOTSS project was to develop and test an educational system for assessment and training based on observable behavioral skills in the intraoperative phase of surgery (Yule et al. Surg Clin N Am 2012;92:37-50).
THE NOTSS SYSTEM
was written in surgical language for trained surgeons to observe, rate, and provide feedback on non-technical skills in a structured manner (Yule et al. Surg Clin N Am 2012;92:37-50). The NOTSS taxonomy is broken down into four distinct categories of non-technical skill: Situation Awareness, Decision Making, Communication and Teamwork, and Leadership (Yule et al. World J Surg 2008;32:548-556), each with associated elements. Good and poor behaviors were carefully written for each element. The Royal College of Surgeons of Edinburgh also provide resources for training non-technical skills. Click Here!“
| Fundamentals of Acceptable Behavior in the Operating Room |
“As much as the culture and practice of surgery have changed and evolved over the last several hundred years, it remains true that the operating room (OR) can be an intimating place for medical students or junior residents. In the past, surgeons have often had the reputation of being arrogant or demeaning, with frequent stories akin to hazing of junior residents in the OR, or of impulsive, disruptive behavior aimed at team members such as nursing staff, anesthesia team, and support personnel. In fact, this type of “old-school” behavior is no longer acceptable, for many reasons. The OR is a special place, but it is still in the end a workplace, and workplace norms of mutual respect and polite behavior must apply. In the modern era, it is clear that surgeons must work in a respectful and collaborative fashion with all members of the patient care team. It is incumbent on the surgeon to create an atmosphere of mutual respect, trust, and communication. This is often called “OR etiquette,” as etiquette is defined as a code of conduct among a group or professionals that should dictate how we act and work with others. This is related to but distinct from manners—which are behaviors (good or bad) that reflect our attitude toward others. Etiquette, therefore, creates the structure within which manners exist.”
Surgeons and Performance
SURGEONS ARE HIGH PERFORMANCE ATHLETES
In a 2011 New Yorker article, Dr. Atul Gawande explored the idea that surgeons should consider a performance coach. Like athletes, he reasons, surgeons rely on complex physical movements to achieve their goals. Guidance and refinement by a trained eye could improve their performance.
Surgical coaching is a controversial topic (one which colleagues and I are actively investigating). But in the years following Dr. Gawande’s article, this idea opened the door to a broader concept: the “surgeon athlete.” An “athlete” is one whose performance depends on a carefully choreographed interplay between mind and body: heightened focus and anticipation along with quick decision-making and coordination. Combined with the reliance on teamwork and requisite stamina, this is wholly within the job description of a surgeon. Many surgeons are likely to find this concept silly. But our profession has imprudently encouraged surgical trainees to disregard the critical fine-tuning of their minds and bodies. We demand perfection, stamina, and encyclopedic knowledge, while discouraging the healthy habits that improve performance. Ironically, the sports world is more advanced in applying science to their training. And by ignoring this indisputable science, we are really hurting our patients. Because in order to best take care of them, we need to first take care of ourselves.
A especialização e a busca pela excelência

“Onde quer que a arte de curar é amada, também há um amor pela humanidade.” — Hipócrates
A especialização em órgãos e o volume de casos têm sido temas centrais nos últimos anos, revelando uma relação direta entre alto volume de procedimentos e melhores desfechos, conforme evidenciado pela literatura recente. Estudos mostram que a concentração de procedimentos de alto risco, como esofagectomias, pancreatectomias e ressecções hepáticas, em centros especializados pode reduzir significativamente a mortalidade pós-operatória anual. Embora procedimentos como tireoidectomias e ressecções do cólon mostrem um efeito semelhante, mas em menor escala, a redução da mortalidade pós-operatória em 5% pode ser tão eficaz quanto tratamentos adjuvantes tóxicos e deve ser uma prioridade na busca pela mais alta qualidade em cirurgia oncológica e digestiva. Além da redução da morbidade e mortalidade, há evidências de que a especialização pode levar a melhores resultados funcionais e financeiros. Às vezes, a atenção excessiva aos números anuais obscurece o fato de que hospitais menores, com equipes dedicadas, também podem alcançar bons resultados. É provável que não apenas o volume, mas também o treinamento e a especialização resultem em melhores desfechos. Definir um número absoluto de casos pode ser improdutivo e desviar a atenção de fatores essenciais, como reuniões multidisciplinares organizadas, infraestrutura adequada e disponibilidade de técnicas modernas.
O Foco na Otimização do Processo
O foco deve ser direcionado para a análise e otimização de todo o processo de diagnóstico e tratamento, já que este processo pode colocar o paciente em grave risco, especialmente durante o período hospitalar. A prevenção de erros tem recebido atenção significativa, levando ao surgimento do conceito de segurança do paciente. Desde a publicação do relatório To Err Is Human pelo Institute of Medicine, a abordagem para erros mudou drasticamente.
Em vez de focar exclusivamente no indivíduo, a abordagem sistêmica considera as condições em que as pessoas trabalham e tenta construir defesas para mitigar os efeitos dos erros. O modelo de queijo suíço ilustra bem essa abordagem: várias camadas de defesa, cada uma com suas falhas, são colocadas em torno de um procedimento. As falhas ativas e condições latentes criam buracos em cada camada. Em vez de apenas fechar os buracos na última camada de defesa, redesenhar o processo e fechar um buraco em uma camada anterior pode ser mais eficaz.
A análise de causa raiz é essencial para identificar pontos fracos no procedimento. Um exemplo é a colocação incorreta de uma colostomia após uma resseção abdominoperineal. Em vez de culpar o residente por não selecionar a posição correta durante a cirurgia ou marcar o ponto errado no dia anterior, uma solução mais eficaz seria o treinamento adequado do junior ou a marcação do ponto certo por um terapeuta de estomas durante a clínica ambulatorial.
A marcação do local correto no corpo tornou-se uma medida de segurança e o paciente deve ser instruído a exigir essa prática para sua própria segurança. É crucial eliminar a cultura de ‘culpa e vergonha’ e promover um ambiente mais aberto, onde erros e quase erros possam ser relatados. O clima de segurança em um departamento cirúrgico pode ser medido de forma validada e é um elemento essencial para uma cultura onde a segurança do paciente possa prosperar.
O Cuidado com os Detalhes e a Otimização de Resultados
A atenção meticulosa a cada detalhe durante o período pré-operatório e clínico pode reduzir eventos adversos. O que é chamado de “primeira vez em risco” deve ser considerado. Há também exemplos de ações para otimizar resultados que são mais específicas para o câncer. Por exemplo, o uso de técnicas que estimulam a cicatrização de feridas após uma resseção abdominoperineal, como a omentoplastia ou o retal abdominal flap, pode evitar atrasos no tratamento adjuvante para câncer retal.
A atenção cuidadosa à cicatrização de feridas em sarcoma pode evitar o adiamento da necessária radioterapia adjuvante. Omissão de uma tomografia computadorizada com contraste contendo iodo no diagnóstico de câncer de tireoide pode possibilitar um tratamento radioativo com iodo mais precoce, resultando em possíveis melhores resultados. A coleta de um número suficiente de linfonodos em câncer de cólon pode evitar discussões sobre a indicação de quimioterapia adjuvante.
A maioria dos exemplos de segurança do paciente no período clínico está relacionada ao uso ótimo de tratamento multimodal ou aos efeitos gerais da cirurgia. Às vezes, é necessário equilibrar o risco de aceitar um procedimento cirúrgico mais extenso, com uma morbidade mais alta, para alcançar um melhor resultado a longo prazo. O oposto também é possível, quando um bom resultado de curto prazo de uma excisão local em câncer retal deve ser equilibrado com uma maior taxa de recorrência local. A garantia de qualidade para todas as disciplinas participantes (diagnósticas e terapêuticas) é um elemento chave na configuração de ensaios clínicos prospectivos e randomizados.
“A prática é a maior professora, e o mais sábio cirurgião é aquele que aprende a valorizar o conhecimento não apenas pela sua acumulação, mas pela sua aplicação.” — William Osler
Pringle Maneuver
After the first major hepatic resection, a left hepatic resection, carried out in 1888 by Carl Langenbuch, it took another 20 years before the first right hepatectomy was described by Walter Wendel in 1911. Three years before, in 1908, Hogarth Pringle provided the first description of a technique of vascular control, the portal triad clamping, nowadays known as the Pringle maneuver. Liver surgery has progressed rapidly since then. Modern surgical concepts and techniques, together with advances in anesthesiological care, intensive care medicine, perioperative imaging, and interventional radiology, together with multimodal oncological concepts, have resulted in fundamental changes. Perioperative outcome has improved significantly, and even major hepatic resections can be performed with morbidity and mortality rates of less than 45% and 4% respectively in highvolume liver surgery centers. Many liver surgeries performed routinely in specialized centers today were considered to be high-risk or nonresectable by most surgeons less than 1–2 decades ago.Interestingly, operative blood loss remains the most important predictor of postoperative morbidity and mortality, and therefore vascular control remains one of the most important aspects in liver surgery.
“Bleeding control is achieved by vascular control and optimized and careful parenchymal transection during liver surgery, and these two concepts are cross-linked.”
First described by Pringle in 1908, it has proven effective in decreasing haemorrhage during the resection of the liver tissue. It is frequently used, and it consists in temporarily occluding the hepatic artery and the portal vein, thus limiting the flow of blood into the liver, although this also results in an increased venous pressure in the mesenteric territory. Hemodynamic repercussion during the PM is rare because it only diminishes the venous return in 15% of cases. The cardiovascular system slightly increases the systemic vascular resistance as a compensatory response, thereby limiting the drop in the arterial pressure. Through the administration of crystalloids, it is possible to maintain hemodynamic stability.

In the 1990s, the PM was used continuously for 45 min and even up to an hour because the depth of the potential damage that could occur due to hepatic ischemia was not yet known. During the PM, the lack of oxygen affects all liver cells, especially Kupffer cells which represent the largest fixed macrophage mass. When these cells are deprived of oxygen, they are an endless source of production of the tumour necrosis factor (TNF) and interleukins 1, 6, 8 and 10. IL 6 has been described as the cytokine that best correlates to postoperative complications. In order to mitigate the effects of continuous PM, intermittent clamping of the portal pedicle has been developed. This consists of occluding the pedicle for 15 min, removing the clamps for 5 min, and then starting the manoeuvre again. This intermittent passage of the hepatic tissue through ischemia and reperfusion shows the development of hepatic tolerance to the lack of oxygen with decreased cell damage. Greater ischemic tolerance to this intermittent manoeuvre increases the total time it can be used.
The century of THE SURGEONS
Surgery is a profession defined by its authority to cure by means of bodily invasion. The brutality and risks of opening a living person’s body have long been apparent, the benefits only slowly and haltingly worked out. Nonetheless, over the past two centuries, surgery has become radically more effective, and its violence substantially reduced — changes that have proved central to the development of mankind’s abilities to heal the sick.
Consider, for instance, amputation of the leg.
The procedure had long been recognized as lifesaving, in particular for compound fractures and other wounds prone to sepsis, and at the same time horrific. Before the discovery of anesthesia, orderlies pinned the patient down while an assistant exerted pressure on the femoral artery or applied a tourniquet on the upper thigh.
Surgeons using the circular method proceeded through the limb in layers, taking a long curved knife in a circle through the skin first, then, a few inches higher up, through the muscle, and finally, with the assistant retracting the muscle to expose the bone a few inches higher still, taking an amputation saw smoothly through the bone so as not to leave splintered protrusions. Surgeons using the flap method, popularized by the British surgeon Robert Liston, stabbed through the skin and muscle close to the bone and cut swiftly through at an oblique angle on one side so as to leave a flap covering the stump.
The limits of patients’ tolerance for pain forced surgeons to choose slashing speed over precision. With either the flap method or the circular method, amputation could be accomplished in less than a minute, though the subsequent ligation of the severed blood vessels and suturing of the muscle and skin over the stump sometimes required 20 or 30 minutes when performed by less experienced surgeons.
No matter how swiftly the amputation was performed, however, the suffering that patients experienced was terrible. Few were able to put it into words. Among those who did was Professor George Wilson. In 1843, he underwent a Syme amputation — ankle disarticulation — performed by the great surgeon James Syme himself. Four years later, when opponents of anesthetic agents attempted to dismiss them as “needless luxuries,” Wilson felt obliged to pen a description of his experience:
“The horror of great darkness, and the sense of desertion by God and man, bordering close on despair, which swept through my mind and overwhelmed my heart, I can never forget, however gladly I would do so. During the operation, in spite of the pain it occasioned, my senses were preternaturally acute, as I have been told they generally are in patients in such circumstances. I still recall with unwelcome vividness the spreading out of the instruments: the twisting of the tourniquet: the first incision: the fingering of the sawed bone: the sponge pressed on the flap: the tying of the blood-vessels: the stitching of the skin: the bloody dismembered limb lying on the floor.”
It would take a little while for surgeons to discover that the use of anesthesia allowed them time to be meticulous. Despite the advantages of anesthesia, Liston, like many other surgeons, proceeded in his usual lightning-quick and bloody way. Spectators in the operating-theater gallery would still get out their pocket watches to time him. The butler’s operation, for instance, took an astonishing 25 seconds from incision to wound closure. (Liston operated so fast that he once accidentally amputated an assistant’s fingers along with a patient’s leg, according to Hollingham. The patient and the assistant both died of sepsis, and a spectator reportedly died of shock, resulting in the only known procedure with a 300% mortality.)
The “GOOD” Surgeon
Surgery is an extremely enjoyable, intellectually demanding and satisfying career, and many more people apply to become surgeons each year than there are available places.
Those who are successful have to be ready not just to learn a great deal, but have the right kind of personality for the job.
Is a surgical career right for you?
Read the link…
THE GOOD SURGEON

O TEMPLO DO CIRURGIÃO.

BLOCO CIRÚRGICO: O TEMPLO DO CIRURGIÃO.
Templo (do latim templum, “local sagrado”) é uma estrutura arquitetônica dedicada ao serviço religioso. O termo também pode ser usado em sentido figurado. Neste sentido, é o reflexo do mundo divino, a habitação de Deus sobre a terra, o lugar da Presença Real. É o resumo do macrocosmo e também a imagem do microcosmo: ‘o corpo é o templo do Espírito Santo’ (I, Coríntios, 6, 19).
Dos locais especiais, O corpo humano (morada da alma), a Cavidade Peritoneal e o Bloco Cirúrgico, se bem analisados, são muito semelhantes e merecem atitudes e comportamentos respeitáveis. O Templo, em todos os credos, induz à meditação, absoluto silêncio tentando ouvir o Ser Supremo. A cavidade peritoneal | abdominal , espaço imaculado da homeostase, quando injuriada, reage gritando em dor, implorando uma precoce e efetiva ação terapêutica.
O Bloco Cirúrgico, abrigo momentâneo do indivíduo solitário, que mudo e quase morto de medo, recorre à prece implorando a troca do acidente, da complicação, da recorrência, da seqüela, da mutilação, da iatrogenia e do risco de óbito pela agressiva e controlada intervenção que lhe restaure a saúde, patrimônio magno de todo ser vivo.
O Bloco Cirúrgico clama por respeito ao paciente cirúrgico, antes mesmo de ser tomado por local banal, misturando condutas vulgares, atitudes menores, desvio de comportamento e propósitos secundários. Trabalhar no Bloco Cirúrgico significa buscar a perfeição técnica, revivendo os ensinamentos de William Stewart Halsted , precursor da arte de operar, dissecando para facilitar, pinçando e ligando um vaso sangüíneo, removendo tecido macerado, evitando corpos estranhos e reduzindo espaço vazio, numa síntese feita com a ansiedade e vontade da primeira e a necessidade e experiência da última.
Mas, se a cirurgia e o cirurgião vêm sofrendo grande evolução, técnica a primeira e científica o segundo, desde o início do século, a imagem que todo doente faz persiste numa simbiose entre mitos e verdades. A cirurgia significa enfrentar ambiente desconhecido chamado “sala de cirurgia” onde a fobia ganha espaço rumo ao infinito. O medo ainda prepondera em muitos.
A confiança neste momento além de um reconhecimento é um troféu que o cirurgião recebe dos pacientes e seus familiares. Tanto a CONFIANÇA quanto a SEGURANÇA têm que ser preservadas a qualquer custo. Não podem correr o risco de serem corroídas por palavras e atitudes de qualquer membro da equipe cirúrgica. Não foi tarefa fácil transformar, para a população, o ato cirúrgico numa atividade científica, indispensável, útil e por demais segura. Da conquista da cirurgia, como excelente arma terapêutica para a manutenção de um alto padrão de qualidade técnica, resta a responsabilidade dos cirurgiões, os herdeiros do suor e sangue, que se iniciou com o trabalho desenvolvido por Billroth, Lister, Halsted, Moyniham, Kocher e uma legião de figuras humanas dignas do maior respeito, admiração e gratidão universal.
No ato operatório os pacientes SÃO TODOS SEMELHANTES EM SUAS DIFERENÇAS, desde a afecção, ao prognóstico, ao caráter da cirurgia e especialmente sua relação com o ato operatório. Logo, o cirurgião tem por dever de ofício entrar no bloco cirúrgico com esperança e não deve sair com dúvida. Nosso trabalho é de equipe, cada um contribui com uma parcela, maior ou menor, para a concretização do todo, do ato cirúrgico por completo, com muita dedicação, profissionalismo e sabedoria. Toda tarefa, da limpeza do chão ao ato de operar, num crescendo, se faz em função de cada um e em benefício da maioria, o mais perfeito possível e de uma só vez, quase sempre sem oportunidade de repetição e previsão de término.
O trabalho do CIRURGIÃO é feito com carinho, muita dignidade, humildade e executado em função da alegria do resultado obtido aliado a dimensão ética do dever cumprido que transcende a sua existência. A vida do cirurgião se materializa no ato operatório e o bloco cirúrgico, palco do nosso trabalho não tolera e jamais permite atitudes menores, inferiores, ambas prejudiciais a todos os pacientes e a cada cirurgião. Como ambiente de trabalho de uma equipe diversificada, precisamos manter, a todo custo, o controle de qualidade, eficiência, eficácia e efetividade técnina associados aos mais altos valores ético, pois lidamos com o que há de mais precioso da criação divina na Terra: O SER HUMANO.
“Tem presença de Deus, como já a tens. Ontem estive com um doente, um doente a quem quero com todo o meu coração de Pai, e compreendo o grande trabalho sacerdotal que os médicos levam a cabo. Mas não se ponham orgulhosos, porque todas as almas são sacerdotais. Devem pôr em prática esse sacerdócio! Ao lavares as mãos, ao vestires a bata, ao calçares as luvas, pensa em Deus, e pensa nesse sacerdócio real de que fala São Pedro, e então não se te meterá a rotina: farás bem aos corpos e às almas” São Josemaria Escriva
A “PROFISSÃO” CIRÚRGICA
 “A arte de curar vem do coração e da mente mais do que das mãos.” – Hipócrates
“A arte de curar vem do coração e da mente mais do que das mãos.” – Hipócrates
Na complexa tapeçaria da sociedade moderna, as profissões desempenham papéis fundamentais na organização dos serviços necessários ao bem-estar coletivo. Definida pelo American College of Surgeons, uma profissão é um campo onde a maestria de um corpo complexo de conhecimento e habilidades é essencial. É uma vocação em que o conhecimento científico ou a prática de uma arte, fundamentada nesse conhecimento, é empregada em benefício dos outros. O compromisso com a competência, a integridade e a moralidade forma a base de um contrato social entre a profissão e a sociedade, que concede à profissão um monopólio sobre o uso de seu conhecimento, considerável autonomia na prática e o privilégio da auto-regulação. Em troca, a profissão deve prestar contas a quem serve e à sociedade como um todo.
Os Elementos Essenciais da Profissão
No cerne de toda profissão estão quatro elementos fundamentais:
- Monopólio do Conhecimento Especializado: Profissionais detêm o direito exclusivo de utilizar conhecimentos e habilidades especializados, o que lhes confere uma posição única na sociedade.
- Autonomia e Auto-Regulação: Em troca deste monopólio, profissionais desfrutam de uma relativa autonomia na prática e são responsáveis pela sua própria regulação.
- Serviço Altruísta: A profissão deve servir tanto indivíduos quanto a sociedade de forma altruísta, colocando o bem-estar do paciente acima de outros interesses.
- Responsabilidade pela Manutenção e Expansão do Conhecimento: Profissionais são responsáveis por atualizar e expandir continuamente seu conhecimento e habilidades.
O Que é Profissionalismo?
Profissionalismo descreve as qualidades cognitivas, morais e colegiais de um profissional. É o conjunto de razões pelas quais um pai se orgulha de dizer que seu filho é um médico e cirurgião. Profissionalismo é mais do que apenas conhecimento técnico; é uma combinação de ética, respeito e dedicação ao ofício e ao paciente.
Por Que Precisamos de um Código de Conduta Profissional?
A confiança é o alicerce da prática cirúrgica. O Código de Conduta Profissional esclarece a relação entre a profissão cirúrgica e a sociedade que serve, frequentemente referido como contrato social. Para os pacientes, o código cristaliza o compromisso da comunidade cirúrgica em relação aos indivíduos e suas comunidades. A confiança é construída, tijolo por tijolo.
O Código de Conduta Profissional
O Código de Conduta Profissional aplica os princípios gerais do profissionalismo à prática cirúrgica e serve como a fundação sobre a qual os privilégios profissionais e a confiança dos pacientes e do público são conquistados. Durante o cuidado pré-operatório, intraoperatório e pós-operatório, os cirurgiões têm a responsabilidade de:
- Advogar Eficazmente pelos interesses dos pacientes.
- Divulgar Opções Terapêuticas incluindo seus riscos e benefícios.
- Divulgar e Resolver Conflitos de Interesse que possam influenciar as decisões de cuidado.
- Ser Sensível e Respeitoso com os pacientes, compreendendo sua vulnerabilidade durante o período perioperatório.
- Divulgar Completamente Eventos Adversos e Erros Médicos.
- Reconhecer Necessidades Psicológicas, Sociais, Culturais e Espirituais dos pacientes.
- Incorporar Cuidados Especiais para Pacientes Terminais.
- Reconhecer e Apoiar as Necessidades das Famílias dos Pacientes.
- Respeitar o Conhecimento, Dignidade e Perspectiva de outros profissionais de saúde.
A Necessidade do Código de Profissionalismo para Cirurgiões
Procedimentos cirúrgicos são experiências extremas que impactam os pacientes fisiológica, psicológica e socialmente. Quando os pacientes se submetem a uma experiência cirúrgica, devem confiar que o cirurgião colocará seu bem-estar acima de todas as outras considerações. O código escrito ajuda a reforçar esses valores, garantindo que a confiança e o compromisso sejam mantidos.
Princípios Fundamentais do Código de Conduta Profissional
- Primazia do Bem-Estar do Paciente: Os interesses do paciente sempre devem vir em primeiro lugar. O altruísmo é central para esse conceito, e é o altruísmo do cirurgião que fomenta a confiança na relação médico-paciente.
- Autonomia do Paciente: Pacientes devem entender e tomar suas próprias decisões informadas sobre o tratamento. Os médicos devem ser honestos para que os pacientes façam escolhas educadas, garantindo que essas decisões estejam alinhadas com práticas éticas.
- Justiça Social: Como médicos, devemos advogar pelos pacientes individuais enquanto promovemos a saúde do sistema de saúde como um todo. Precisamos equilibrar as necessidades dos pacientes (autonomia) sem desviar recursos escassos que beneficiariam a sociedade (justiça social).
“Não há maior coisa a ser conquistada do que a confiança dos pacientes e da sociedade, pois ela é a base sobre a qual construímos nossas práticas e nossa profissão.” – William Osler
GOSSIPIBOMA
O Inimigo Oculto no Bloco Operatório e o Desafio Médico-Legal na Cirurgia Digestiva
Autor: Prof. Dr. Ozimo Gama (Tempo de Leitura: 11 minutos)
Introdução
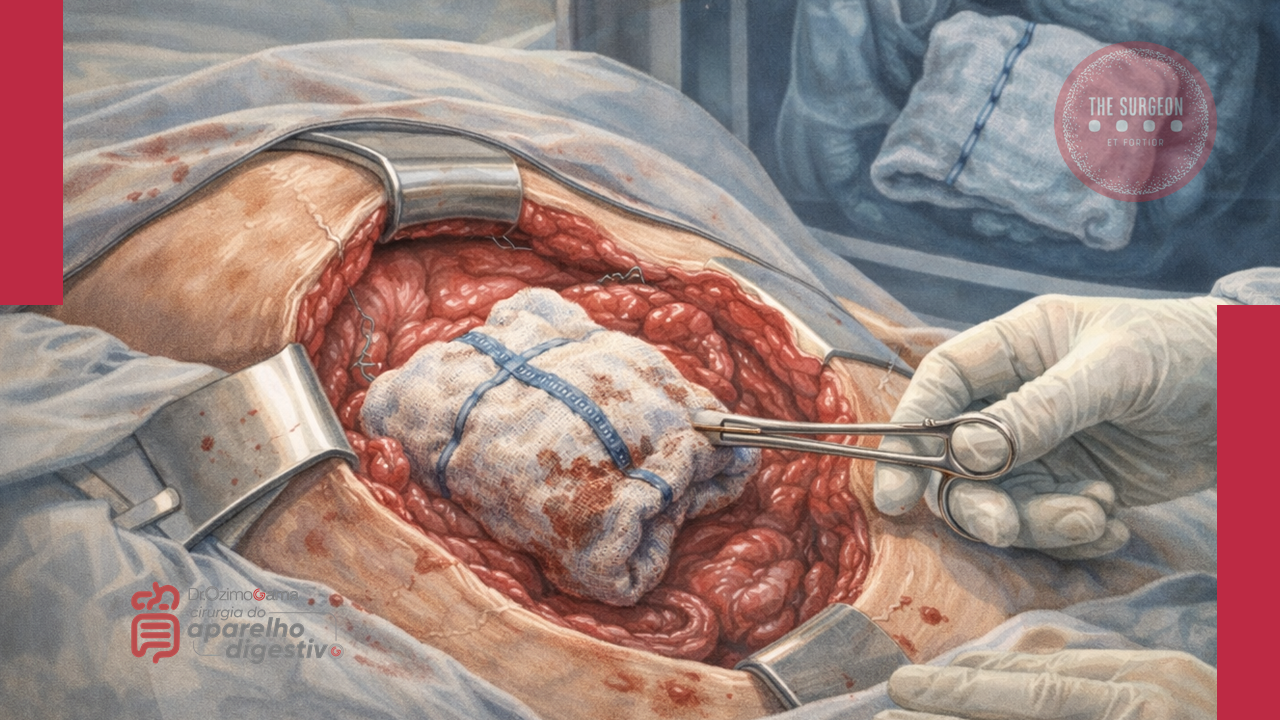
No vasto e complexo universo da cirurgia do aparelho digestivo, poucos eventos adversos geram tanta perplexidade clínica e devastação médico-legal quanto o “gossipiboma”. O termo deriva do latim Gossypium (algodão) e do swahili boma (esconderijo), designando uma matriz de matéria têxtil envolvida por uma reação de corpo estranho. Também apelidado de “textiloma”, o seu primeiro caso foi descrito por Wilson em 1884. Embora gazes e compressas sejam as ferramentas mais básicas de qualquer laparotomia, o seu esquecimento no interior da cavidade abdominal transforma um material de hemostase num tumor iatrogénico. A incidência real dos gossipibomas é subnotificada — primariamente devido ao estigma e às pesadas implicações legais da sua deteção —, mas representa uma falha catastrófica nos protocolos de segurança do bloco operatório. Para o cirurgião e para toda a equipa, compreender a fisiopatologia, os fatores de risco e, sobretudo, os métodos de prevenção desta entidade é um dever ético inegociável.
Epidemiologia e Fatores de Risco
Estima-se que a retenção de material têxtil ocorra numa frequência de 1 a cada 1.000 a 1.500 operações intra-abdominais. A cavidade abdominal e pélvica é, de longe, o “esconderijo” mais comum devido à sua vasta anatomia e aos recessos profundos.
O gossipiboma não é um mero fruto do acaso; ele prospera no caos. A literatura científica identifica fatores predisponentes cruciais:
- Cirurgia de Emergência: A incidência é nove vezes maior nestes cenários.
- Mudança de Tática Intraoperatória: Alterações não planeadas no decorrer da intervenção elevam o risco em quatro vezes.
- Fatores do Doente e do Ambiente: Doentes com obesidade mórbida, perdas hemáticas maciças que exigem tamponamento rápido, tempo operatório prolongado e, criticamente, a troca de turnos do pessoal médico e de enfermagem (instrumentistas e circulantes) durante o ato cirúrgico.
Fisiopatologia e Evolução Clínica
O relógio biológico do gossipiboma é imprevisível. O tempo entre a operação primária e as manifestações clínicas pode variar de meros 10 dias a várias décadas. A patologia manifesta-se essencialmente através de duas reações orgânicas distintas:
- Resposta Assética Fibrinosa (Crónica): O material têxtil, se permanecer estéril, induz a produção de fibrina, originando aderências e o encapsulamento do corpo estranho (granuloma). O doente pode permanecer completamente assintomático durante anos, ou apresentar queixas inespecíficas e uma massa abdominal palpável que mimetiza uma neoplasia.
- Resposta Exsudativa (Aguda): Ocorre uma infeção secundária severa, culminando na formação de abcessos e fístulas. O material retido tenta encontrar uma via de exteriorização, podendo fistulizar para órgãos internos (estômago, intestino, cólon, bexiga) ou formar uma fístula externa na parede abdominal. Nestes casos, o doente apresenta um quadro florido: dor abdominal, náuseas, vómitos, febre, sépsis, hemorragia digestiva crómica ou síndrome de má absorção.
Diagnóstico, Tratamento e Prognóstico
A ausência de sintomas precoces ou a sua inespecificidade tornam o diagnóstico um autêntico desafio. O cirurgião deve manter um elevado índice de suspeição perante qualquer massa abdominal num doente com história de laparotomia prévia.
- O Padrão-Ouro Diagnóstico: A Tomografia Computorizada (TC) de abdómen é o exame de eleição. A imagem clássica revela uma lesão cística de aspeto “espongiforme” (padrão em miolo de pão), uma cápsula hiperdensa em camadas concêntricas e, ocasionalmente, calcificações murais. A presença de gás no interior da lesão sem evidência de perfuração intestinal é altamente sugestiva.
- Tratamento: A remoção cirúrgica (seja por via laparoscópica em casos altamente selecionados ou laparotomia) é o único tratamento curativo.
- Prognóstico: A excisão atempada é vital para evitar complicações que elevam a taxa de mortalidade para valores inaceitáveis de 11% a 35%. Se a retenção for crónica, a severidade das aderências pode exigir ressecções intestinais extensas e complexas.
Implicações Médico-Legais e Procedimentos Preventivos
O gossipiboma é indiscutivelmente uma falha grave na prestação de cuidados de saúde (malpractice). Do ponto de vista médico-legal, a responsabilidade é frequentemente partilhada entre o cirurgião principal — o “capitão do navio” — e a equipa de enfermagem responsável pela contagem.
A abordagem definitiva é, e sempre será, a Prevenção. A adoção de protocolos rígidos no bloco operatório salva vidas e carreiras:
- Contagem Meticulosa Universal: São mandatárias quatro contagens rigorosas do material cirúrgico: na montagem da mesa, imediatamente antes da incisão, no início do encerramento da aponevrose e durante a síntese da pele.
- Material Radiopaco: O uso exclusivo de compressas e gazes equipadas com filamentos radiopacos é obrigatório.
- Exploração Ativa: Autores como Dhillon e Park reforçam a necessidade primária da exploração manual e visual dos quatro quadrantes abdominais pelo cirurgião no final do procedimento, independentemente de uma contagem de compressas declarada “correta”.
- Conduta Perante Falha na Contagem: Se a contagem final for divergente, a síntese da cavidade não deve ser concluída até que o material seja localizado (a menos que haja instabilidade hemodinâmica crítica). A realização de uma radiografia intraoperatória imediata é mandatária.
Conclusões Aplicadas
O gossipiboma não é uma complicação inerente e aceitável do ato cirúrgico; é uma falha de sistema e de liderança. O aumento aparente da sua incidência exige que os métodos, a comunicação e a disciplina no interior do bloco operatório sejam revistos e aperfeiçoados. Para os jovens cirurgiões e residentes, a mensagem é clara: a cirurgia de excelência não termina na anastomose perfeita, mas sim na verificação obsessiva e no respeito incondicional pelos protocolos de segurança. A verdadeira destreza cirúrgica repousa na humildade de nunca presumir que a cavidade está vazia sem antes a inspecionar exaustivamente.
“A confiança é um sentimento nobre, mas no bloco operatório, a dupla verificação é a única garantia de segurança. Um erro de omissão pode ensombrar o mais brilhante dos procedimentos cirúrgicos.” — Aforismo da Segurança do Doente Cirúrgico.
Gostou ❔Deixe-nos um comentário ✍️ , partilhe nas suas redes sociais e|ou envie a sua dúvida pelo 💬 Chat On-line na nossa DM do Instagram.
10 Princípios da interação PACIENTE – CIRURGIÃO
Comunicação, Ética e Segurança na Prática Cirúrgica
Autor: Prof. Dr. Ozimo Gama (Tempo de Leitura: 11 minutos)
Introdução
Quando a perspectiva de uma intervenção cirúrgica se impõe — seja para a ressecção de uma neoplasia gástrica, a correção de uma hérnia complexa ou o tratamento metabólico da obesidade —, o medo, a apreensão e a sensação de perda de controle são reações viscerais e universais do ser humano. A visão da dor, o fantasma das complicações e a entrega do próprio corpo ao bisturi de outrem geram uma ansiedade que a mais avançada tecnologia robótica não é capaz de aplacar. No Brasil, onde realizamos milhões de procedimentos cirúrgicos anualmente pelo Sistema Único de Saúde (SUS) e pela Saúde Suplementar, estatísticas dos Conselhos Regionais de Medicina (CRMs) revelam um dado alarmante: mais de 70% das denúncias e processos ético-profissionais por suposto “erro médico” não nascem de falhas técnicas grosseiras, mas da quebra, deterioração ou inexistência de uma relação médico-paciente sólida e transparente. Para o estudante de medicina e o residente de cirurgia, compreender que a destreza manual deve ser precedida pela empatia relacional é o primeiro passo para a maestria.
Os 10 Princípios da Prática Cirúrgica Ética
Para enfrentar os desafios do perioperatório de forma eficaz e blindar a relação terapêutica contra ruídos e frustrações, estruturamos os 10 princípios fundamentais que regem a interação entre o cirurgião e o paciente:
1. Construção da Confiança Mútua
A cirurgia não é um ato comercial; é um pacto de confiança. O cirurgião deve dedicar tempo qualitativo na consulta, evitando o modelo impessoal e apressado (“medicina de linha de montagem”). Um relacionamento humanizado evita que insucessos terapêuticos se transformem em acusações injustas.
2. Clareza e Transparência na Informação
O consentimento deve ser genuinamente esclarecido, não apenas assinado. É imperativo banir o jargão técnico excessivo. Traduzir a fisiopatologia e o plano cirúrgico para uma linguagem acessível reduz o medo do desconhecido e prepara o paciente e seus familiares para o desdobramento natural do pós-operatório.
3. Alinhamento de Expectativas Realistas
Muitas frustrações cirúrgicas nascem do hiato entre a expectativa do paciente e a realidade biológica. É vital discutir os limites da medicina. Prometer “cura absoluta” ou “risco zero” é uma falácia ética.
4. Avaliação Abrangente de Riscos
O Risco Cirúrgico transcende a avaliação cardiológica (Escore de Goldman ou Lee). A avaliação pré-operatória moderna exige uma visão holística: o estado nutricional, a fragilidade (especialmente em idosos), a sarcopenia e, crucialmente, a saúde mental do paciente devem ser exaustivamente investigados.
5. O Papel Estratégico do Anestesiologista
O ato cirúrgico é indissociável do ato anestésico. A escolha da técnica anestésica (bloqueios, anestesia geral, monitorização multimodal) é uma decisão compartilhada. O cirurgião deve fomentar o encontro pré-operatório entre o paciente e a equipe de anestesiologia para dirimir receios e garantir as melhores práticas.
6. Preparação para Mudanças de Rota (O Imprevisto)
O paciente deve entrar no centro cirúrgico ciente de que a tática operatória pode ser alterada. O consentimento para uma laparoscopia deve invariavelmente incluir a possibilidade de conversão para via aberta. Surpresas intraoperatórias (como invasões tumorais insuspeitas) alteram o prognóstico, o tempo de internação e as necessidades de reabilitação.
7. Documentação Exaustiva e Irretocável
O prontuário médico é a testemunha ocular do cuidado. Detalhes das consultas preliminares, opções terapêuticas recusadas pelo paciente e as orientações fornecidas devem estar meticulosamente registrados. Como já abordamos em nosso artigo sobre o método S.O.A.P., documentação é proteção mútua.
8. Descrição Cirúrgica e Rastreabilidade
A descrição do ato operatório deve ser um relato literário da técnica executada. Além disso, a gestão de peças cirúrgicas (envio para exame anatomopatológico) exige rigor logístico. A falha na identificação ou a perda de uma biópsia é uma tragédia diagnóstica inaceitável.
9. Pós-Operatório: Presença e Cuidado Contínuo
O ato cirúrgico não termina no fechamento da pele. O acompanhamento pós-operatório (na UTI, na enfermaria e no ambulatório) exige a presença física e atenciosa do cirurgião principal. Delegar todo o pós-operatório a terceiros é uma das maiores fontes de ressentimento por parte dos pacientes.
10. Atenção ao Estado Emocional
A instabilidade emocional predispõe a uma resposta inflamatória exacerbada e a uma percepção amplificada da dor. Pacientes com ansiedade severa ou depressão pré-existente exigem suporte psicológico ou psiquiátrico adjuvante para garantir resiliência durante a convalescença.
Aplicação na Cirurgia Digestiva
Na cirurgia do aparelho digestivo, estes princípios encontram aplicação diária e visceral:
- Na Cirurgia Bariátrica: O alinhamento de expectativas (Princípio 3) é o alicerce do sucesso. O paciente deve compreender que o bisturi altera a anatomia (Restrição/Incretinas), mas não opera a mente. O reganho de peso é uma possibilidade real se não houver adesão multidisciplinar (Princípio 10).
- Na Cirurgia Oncológica: Informar um paciente sobre a possível necessidade de um estoma (colostomia ou ileostomia) definitivo ou temporário (Princípio 6) exige tato excepcional (Princípio 2). Esconder essa possibilidade para “evitar o sofrimento prévio” destrói a confiança se o paciente acordar com uma bolsa coletora no abdome.
- Na Cirurgia Biliar e Pancreática: Complicações temidas, como a fístula biliar ou pancreática, devem ser discutidas com transparência empática. Quando a complicação ocorre, a presença diária e incansável do cirurgião à beira do leito (Princípio 9) é o que diferencia o abandono do amparo.
Pontos-Chave para a Prática Diária
- Comunicação é Procedimento: Trate a conversa com o paciente e a família com o mesmo rigor técnico que você trata a dissecção de um hilo hepático.
- A Verdade Suportável: Nunca minta, mas adeque a entrega da informação à capacidade de absorção do paciente naquele momento.
- Consentimento Individualizado: Termos de consentimento (TCLE) padronizados e genéricos não possuem força legal. O TCLE deve espelhar as peculiaridades anatômicas e biológicas do paciente específico.
Conclusões Aplicadas
A ética na cirurgia moderna vai imensuravelmente além da destreza técnica, dos nós bem atados e da ausência de complicações infecciosas. Trata-se do respeito à autonomia daquele que se submete à lâmina. A prática cirúrgica de excelência exige que sejamos peritos em fisiologia e mestres em humanidade. O cirurgião do aparelho digestivo que domina estes 10 princípios navega pelas tempestades de uma fístula anastomótica não como um réu diante de um juiz (o paciente), mas como um comandante ao lado de seu companheiro de naufrágio, trabalhando juntos para alcançar a margem segura da cura.
“O bom cirurgião opera com a mão; o cirurgião brilhante opera com o cérebro; mas o cirurgião extraordinário opera com o coração. O bisturi corta tecidos, mas é a compaixão que cicatriza as feridas da alma.” — Adaptado dos princípios humanitários de Sir William Osler, pai da medicina moderna.
Gostou ❔Nos deixe um comentário ✍️ , compartilhe em suas redes sociais e|ou mande sua dúvida pelo 💬 Chat On-line em nossa DM do Instagram.
The General Surgery Job Market

There is a current shortage of general surgeons nationwide. A growing elderly population and ongoing trends toward increased health care use have contributed to a higher demand for surgical services, without a corresponding increase in the supply of surgeons. The number of general surgeons per 100,000 people in the United States declined by 26% from the 1980s to 2005. Cumulative growth in demand for general surgery is projected to exceed 25% by 2025. The Association of American Medical Colleges has projected a shortage of 41,000 general surgeons by 2025. General surgeons make up 33% of the total projected physician shortage, the second highest after primary care physicians, who make up 37% of the total shortage. Despite the demand for general surgeons, the percentage of general surgery trainees going directly into practice is decreasing while the percentage of trainees pursuing subspecialty training is increasing. A recent study reported that graduating residents who lacked confidence in their skills to operate independently were more likely to pursue subspecialty training. This suggests that some graduating residents are motivated to obtain subspecialty training to gain more experience rather than narrow their clinical scope of practice. Given the projected shortage of general surgeons, this will be a crucial distinction when reforming surgical education. General surgery trainees interested in career planning would benefit from understanding the demand for general and/or specialty skills in a job market heavily influenced by a constant stream of new graduates. However, little is currently known about the demand for subspecialty vs general surgical skills in the current job market. The goal of this study was to describe the current job market for general surgeons in the United States, using Oregon and Wisconsin as surrogates. Furthermore, we sought to compare the skills required by the job market with those of graduating trainees with the goal of gaining insight that might assist in workforce planning and surgical education reform.
Survival Guide for SURGERY ROUND

SURGERY ROUND
Medical students are often attached to the various services. They can provide a significant contribution to patient care. However, their work requires supervision by the surgical intern/resident who takes primary clinical responsibility. Subinterns are senior medical students who are seeking additional clinical experience. Their assistance is needed and appreciated, but again, close supervision of their clinical responsibilities by the intern/resident is mandatory.Outside reading is recommended, including textbooks, reference sources, and monthly journals.Eating is prohibited in patient care areas.Maintain patient confidentiality at all times.At conferences use only patient initials in presentations; and speak carefully and respectfully on work rounds.
PRINCIPLES
1. Always be punctual (this includes ward rounds, operating room, clinics, conferences, morbidity and mortality). Personal appearance is very important. Maintain a high standard including clean shirt and tie (or equivalent) and a clean white coat. The day begins early. Be ready with all the data to start rounds with the senior resident or chief resident. Be sure to provide enough time each morning to examine your patients before rounds.
ABOUT NOTES
2.Aim to get all of your chart notes written as soon as possible; this will greatly increase your effi ciency during the day. Sign and print your name, and include your beeper number, date, and time. Progress notes on patients are required daily. Surgical progress notes should be succinct and accurate, briefl y summarizing the patient’s clinical status and plan of management. Someone unfamiliar with the case should be able to get a good understanding of the patient’s condition from one or two notes. Operative consent is obtained after admitting the patient, performing the history and physical examination, discussing the risks, benefi ts, and alternatives of the procedure(s), and having the patient’s nurse sign the consent with the patient. If you are unaware of the risks and benefi ts of a procedure, discuss this with the service chief resident. Blood transfusion attestation forms need to be signed by the counseling physician before each surgical procedure.
OPERATING ROOM
3. Arrive in the operating room with the patient and before the attending physician or chief resident. Make sure that the charts and all of the relevant x-rays are in the operating room. Make sure that the x-rays are on the x-ray view box prior to the commencement of the case. The intern or resident performing the case should be familiar with the patient’s history and physical exam, current medications, and comorbidities, and be familiar with the principles of the operation prior to arriving in the operating room. Make it a habit to introduce yourself to the patient before the operation. It is mandatory that the surgical resident involved with a case in the operating room attend the start of the case punctually. Scheduled operative cases do not necessarily occur at the listed time. For this reason, it is necessary to check with the operating room front desk frequently. Do not rely on being paged. Conduct in the operating room includes assisting with the preoperative positioning and preparation of the patient; this includes shaving, catheterization, protection of pressure points, and thromboembolism protection. The resident should escort the patient from the operating room to the intensive care unit (ICU) or the postanesthetic care unit with the anesthesiologists. The operating surgeon is responsible for dictating the case. The resident must record all cases performed. For cases admitted to the surgery ICU, a hand-over to the surgery ICU resident is mandatory.This includes discussing all the preoperative assessment, operative details, and postoperative management of the case with the ICU resident.
ROUNDS
4. Signing out to cross-cover services must be performed in a meticulous and careful fashion. All patients should be discussed between the surgical intern and the cross-covering intern to cover all potential problems. A sign-out list containing all the patients, patient locations, and the responsible attendings should be given personally to the cross-cover intern. Any investigations performed at night (e.g., lab studies, chest x-ray, electrocardiogram [ECG]) should be checked that night by the covering intern. No test order should go unchecked. Abnormal lab values should be reviewed and discussed with the senior resident or the attending staff, especially on preoperative patients. Starting antibiotics should be a decision left to the senior resident or attending staff. If consultants are asked to see patients, their recommendations mustbe discussed with your senior resident or attending priorto initiating any new plans. Independent thought is good; independent action is bad.
SUPERVISION
5. Document all procedures performed on patients—including arterial lines, chest tubes, and central lines—with a short procedure note in the chart. Every patient contact should be documented in the patient record.If you see a patient in the middle of the night, write a short note to describe your assessment and plan. Remember, if there is no documentation, then nobody responded to the patient’s complaint or needs. Obtain appropriate supervision for procedures. There are always more senior residents available if your chief is not. Protect yourself; practice universal precautions! Wash your hands before and after examining a patient. Wear gloves. All wounds should be inspected every day by the surgical intern as part of the clinical examination. Please re-dress them; the nursing staff is not always immediately available to do so. There should never be any surprises in the morning.
RESIDENTS
Your senior resident is responsible for the service and should be kept aware of any problems, regardless of the time of day. If the senior resident is not available, the attending staff should be contacted directly. There are always senior residents in the hospital who are available to be used as resources for emergencies. Always be aware of who is in-house (i.e., consult resident, ICU resident, trauma chief). A surgery resident’s days are long. They start early and they fi nish late. Always remember the three A’s to being a successful resident: Affable, Available, and Able. Be prepared to maintain a flexible daily schedule depending on the workload of the service and the requirement for additional manpower.
“COMO PODEMOS CURAR A MEDICINA?”
“Nos últimos anos percebemos que estávamos na mais profunda crise da existência da medicina, devido a algo sobre o que você normalmente não pensa quando você é um médico preocupado em fazer o bem para as pessoas, que é o custo do tratamento de saúde. Não há um país no mundo que não esteja perguntando agora se podemos custear o que médicos fazem. A luta política que desenvolvemos tornou-se aquela sobre se o governo é o problema ou se as companhias de seguro são o problema. E a resposta é sim e não; é mais profundo que tudo isso. A causa de nossos problemas é, na verdade, a complexidade que a ciência nos deu. E para entender isso, voltarei algumas gerações…”
“CIRURGIA: PASSADO, PRESENTE e FUTURO ROBÓTICO”
A cirurgiã e inventora Catherine Mohr nos guia pela história da cirurgia (e seu passado pré-anestesia e pré-antissepsia), e depois demonstra algumas das mais novas ferramentas para cirurgias realizadas através de pequenas incisões, usando ágeis mãos robóticas.
Prontuário Médico
Evolução Cirúrgica S.O.A.P.
A Engenharia do Prontuário Médico, Ética, LGPD e Defesa Profissional
Autor: Prof. Dr. Ozimo Gama (Tempo de Leitura: 12 minutos)

Introdução
O prontuário médico transcende a simples formalidade administrativa; ele é o repositório sagrado do segredo médico, o espelho da qualidade assistencial e a testemunha silenciosa de cada decisão clínica tomada na beira do leito. No ambiente de alta complexidade da cirurgia do aparelho digestivo, onde o limiar entre a recuperação fisiológica e a complicação catastrófica é estreito, a evolução médica diária exige uma precisão quase matemática. A prática de preencher o prontuário é uma obrigação legal e uma responsabilidade intransferível do médico assistente. Em hospitais de ensino — o berço da formação cirúrgica —, acadêmicos de medicina e médicos residentes (especializandos) realizam as anotações sob a estrita supervisão, correção e responsabilidade solidária de seus preceptores ou médicos do staff. É uma prática antiética, ilegal e frontalmente condenável delegar o preenchimento da evolução clínica a qualquer profissional que não seja um médico habilitado perante o Conselho Regional de Medicina (CRM) ou um acadêmico em treinamento devidamente supervisionado. Historicamente e na atualidade, o prontuário médico corretamente preenchido tem sido a principal, e muitas vezes a única, peça de defesa do cirurgião em casos de denúncias por suposto mau atendimento, imperícia, imprudência ou negligência. Quando a polícia, o Poder Judiciário ou as Câmaras Técnicas do CRM são acionados, o prontuário é o primeiro documento requisitado. Se a sua técnica cirúrgica no bloco operatório for irretocável, mas a sua evolução na enfermaria for omissa, perante a lei, o cuidado não existiu.
Aspectos Históricos e a Gênese do Modelo S.O.A.P.
Até meados do século XX, os prontuários médicos eram estruturados de forma cronológica e narrativa, assemelhando-se a um diário confuso, onde informações vitais perdiam-se num mar de textos desorganizados. A revolução ocorreu na década de 1960, quando o Dr. Lawrence L. Weed publicou o artigo seminal “Medical records that guide and teach” (N Engl J Med; 1968). Weed propôs uma inversão de paradigma: o Problem-Oriented Medical Record (Prontuário Médico Orientado por Problemas). No Brasil, este modelo foi amplamente adotado e adaptado sob a sigla POPE (Prontuário Orientado por Problemas e Evidências), destacando a necessidade de fundamentar cada passo clínico em evidências científicas sólidas. A espinha dorsal deste modelo é a nota de evolução estruturada no formato S.O.A.P., que divide o raciocínio médico em quatro quadrantes fundamentais: Subjetivo, Objetivo, Avaliação e Plano. Esta sistematização traz objetividade, clareza, facilidade de auditoria e, principalmente, permite que qualquer membro da equipe multidisciplinar (enfermagem, fisioterapia, nutrição) compreenda imediatamente o estado clínico e as metas terapêuticas do paciente cirúrgico.
A Estrutura do S.O.A.P. Cirúrgico
Na rotina da enfermaria de cirurgia digestiva, a evolução deve seguir um rigor técnico absoluto. O cabeçalho deve, obrigatoriamente, conter a identificação completa do paciente (Nome, Idade, Registro Hospitalar), a Enfermaria/Leito, o Diagnóstico Principal, o Nome da Cirurgia Realizada, o Dia de Pós-Operatório (ex: PO2 de Gastrectomia Total) e o Horário exato do atendimento.
Abaixo, detalhamos como cada componente da sigla S.O.A.P. deve ser preenchido sob a ótica cirúrgica:
1. “S” – Dados Subjetivos (A Voz do Paciente)
Compreende as queixas do paciente, sua percepção sobre a evolução e informações fornecidas por acompanhantes. Em cirurgia, não basta escrever “passou bem”. É imperativo interrogar ativamente sobre:
- Dor: Utilizar escalas validadas (ex: Escala Visual Analógica – EVA de 0 a 10). A dor é em cólica? É contínua? Piora à mobilização?
- Trato Gastrointestinal: Houve náuseas ou episódios de êmese? Houve eliminação de flatos (sinal crucial de retorno do trânsito intestinal)? Houve evacuação? Como foi a aceitação da dieta oferecida?
- Mobilização: O paciente deambulou? Conseguiu sentar na poltrona? (Dados vitais para a profilaxia de trombose venosa profunda e atelectasia).
- Exemplo: “Paciente refere dor incisional leve (EVA 2/10), com boa aceitação de dieta líquida. Nega náuseas. Refere eliminação de flatos durante a madrugada. Deambulou no corredor hoje cedo.”
2. “O” – Dados Objetivos (A Visão do Cirurgião)
Inclui os dados vitais irrefutáveis, o exame físico focado e os resultados de exames complementares laboratoriais ou de imagem. Este é o terreno da evidência mensurável.
- Sinais Vitais: Frequência Cardíaca (FC), Pressão Arterial (PA), Frequência Respiratória (FR), Temperatura (T) e Saturação de O2. A taquicardia inexplicada no pós-operatório de uma anastomose intestinal é o primeiro grito de socorro de uma fístula, antes mesmo da febre ou da dor peritonítica.
- Exame Físico Específico: * Abdome: Globoso? Flácido? Ruídos hidroaéreos presentes? Dor à palpação (diferenciar dor incisional de irritação peritoneal)?
- Ferida Operatória (FO): Limpa e seca? Hiperemiada? Presença de secreção (serosa, purulenta, hemática)?
- Drenos: Tipo de dreno (ex: Jackson-Pratt, Blake, Penrose). Qual o aspecto do débito (seroso, sero-hemático, bilioso, entérico, fecaloide)? Qual o volume em 24 horas?
- Estomas: Colostomia/Ileostomia com mucosa rósea (vitalidade)? Edemaciada? Isquêmica? Estoma funcionante (presença de fezes na bolsa)?
- Exemplo: “PA: 120×70 mmHg; FC: 88 bpm; FR: 16 irpm; T: 36,8ºC. Abdome: flácido, RHA+, indolor à palpação profunda. FO: sem hiperemia, curativo limpo. Dreno de Blake em FIE: débito de 30ml sero-hemático em 24h. Labs (05/10): Hb 11.2, Leucócitos 8.500 (sem desvio), PCR 12 (em queda).”
3. “A” – Avaliação (O Raciocínio Clínico)
A Avaliação é a síntese. É o momento em que o cirurgião processa os dados Subjetivos e Objetivos para emitir o seu juízo de valor sobre o estado do paciente. Não é a repetição dos diagnósticos da internação, mas a avaliação do momento atual.
- O paciente está evoluindo conforme o esperado para o dia de pós-operatório?
- Há suspeita de complicações (íleo paralítico prolongado, infecção de sítio cirúrgico, fístula anastomótica, sangramento, pneumonia)?
- Exemplo: “Paciente no 2º PO de Colectomia Direita Videolaparoscópica por Adenocarcinoma. Evolução clínica e laboratorial amplamente favorável. Trânsito intestinal restabelecido. Sem sinais de complicações infecciosas ou hemorrágicas no momento.”
4. “P” – Plano (A Conduta e o Futuro)
O Plano define as ações imediatas e de médio prazo. É a conduta terapêutica e diagnóstica fundamentada na avaliação recém-feita.
- Terapêutica: Progressão ou regressão de dieta? Transição de analgesia venosa para via oral? Suspensão de fluidos intravenosos? Descalonamento ou suspensão de antibioticoterapia profilática/terapêutica?
- Procedimentos: Retirada de dreno? Troca de curativo? Retirada de Sonda Vesical de Demora (SVD)?
- Diagnóstico: Solicitação de novos exames laboratoriais ou tomografia de abdome (se suspeita de complicação)?
- Educação/Alta: Orientações ao paciente e preparo para alta hospitalar.
- Exemplo: “1. Progredir para dieta pastosa; 2. Suspender hidratação venosa e manter acesso salinizado; 3. Trocar analgesia para via oral; 4. Retirar dreno de Blake hoje; 5. Programar alta hospitalar para amanhã, caso mantenha tolerância à dieta.”
Aspectos Éticos, Legais e Atualizações Normativas
A prática médica contemporânea exige que a evolução cirúrgica esteja blindada contra vulnerabilidades legais. A doutrina da “medicina de defesa” tem dado lugar à Prevenção Jurídica Ativa, onde o prontuário é o escudo. Segundo o Código de Ética Médica (Resolução CFM nº 2.217/2018), em seu Capítulo X, é vedado ao médico negar acesso ao prontuário ao paciente, bem como é infração ética grave deixar de elaborar prontuário legível para cada paciente.
O Código Penal e a Falsidade Ideológica
As anotações devem refletir a estrita verdade temporal e clínica. O Artigo 299 do Código Penal Brasileiro é taxativo quanto ao crime de falsidade ideológica: “Omitir, em documento público ou particular, declaração que dele devia constar, ou nele inserir ou fazer inserir declaração falsa ou diversa da que devia ser escrita…”. A pena varia de 1 a 5 anos de reclusão. Evoluções “clonadas” (o infame “copiar e colar” do dia anterior no prontuário eletrônico sem verificar o paciente) que não relatam a mudança do estado clínico (ex: o paciente apresentou febre à noite, mas a evolução matinal diz “afebril” por cópia da véspera) podem caracterizar este crime, além de negligência médica. No papel, rasuras anulam o valor probatório; deve-se usar a expressão “digo” ou “em tempo” para retificações.
O Prontuário Eletrônico do Paciente (PEP) e a Certificação Digital
A Resolução CFM nº 1.638/2002 tornou obrigatória a legibilidade do prontuário em papel (o fim definitivo da “letra de médico” ilegível). Contudo, a grande revolução normativa reside no Prontuário Eletrônico. De acordo com a Resolução CFM nº 1.821/2007 (e suas atualizações, como a Resolução 2.299/2021), para que um documento médico eletrônico tenha validade legal e elimine a necessidade do papel, ele deve utilizar sistema de segurança com Nível de Garantia de Segurança 2 (NGS2), que exige a Assinatura Digital com certificado ICP-Brasil (Infraestrutura de Chaves Públicas Brasileira). Sem o token ou certificado digital em nuvem assinado pelo médico, a evolução digitada não tem presunção de veracidade jurídica plena. A senha do sistema do hospital não substitui a assinatura digital. A prática de fornecer seu login e token para que o residente ou interno assine por você é falta ética gravíssima, equiparada à quebra de sigilo e falsidade ideológica.
A Lei Geral de Proteção de Dados (LGPD – Lei 13.709/2018)
O prontuário cirúrgico contém dados sensíveis (informações sobre saúde). A implementação da LGPD obriga as instituições e os médicos a garantirem o acesso restrito a essas informações. A evolução clínica SOAP não pode ser fotografada pelo celular do médico e enviada em grupos de mensagens (como WhatsApp) sem a desidentificação completa do paciente ou consentimento expresso. Vazamentos de dados contidos no prontuário geram pesadas multas pela Autoridade Nacional de Proteção de Dados (ANPD) e processos civis por dano moral.
Pontos-Chave para a Prática Diária do Residente
- Tempo é Documento: A data e a hora do atendimento são cruciais. A evolução médica reflete o paciente naquele minuto exato. A cronologia dos eventos salva ou condena o cirurgião em uma sindicância.
- O Perigo do Copiar/Colar: No prontuário eletrônico, o recurso de copiar a evolução do dia anterior induz ao erro, perpetuando dados vitais antigos ou ignorando exames recentes. Cada dia exige uma avaliação autêntica e original.
- Assinatura e Carimbo: No papel, carimbo e assinatura legível com CRM. No eletrônico, Assinatura Digital (ICP-Brasil). A validação de quem prescreve ou evolui é intransferível.
- Comunicação Multidisciplinar: A evolução SOAP não é escrita apenas para o juiz ou para o CRM; ela é lida pelo enfermeiro que administrará o antibiótico, pelo fisioterapeuta que mobilizará o paciente e pelo nutrólogo que ajustará a dieta. Clareza é respeito pela equipe e segurança para o doente.
Conclusões Aplicadas à Prática do Cirurgião Digestivo
A evolução cirúrgica é a radiografia do intelecto do médico. O método S.O.A.P. obriga o cirurgião do aparelho digestivo a estruturar seu pensamento científico de maneira cartesiana, garantindo que nenhum dreno, ostomia ou sintoma de alarme passe despercebido na enfermaria. Em uma era dominada pela alta tecnologia robótica e laparoscópica no centro cirúrgico, é na beira do leito e na frente da tela do Prontuário Eletrônico que o pós-operatório é vencido. Compreender as legislações vigentes, a obrigatoriedade da certificação digital e a rigidez da LGPD protege o patrimônio e a carreira do profissional, permitindo que ele exerça a arte da cirurgia com paz de espírito, sabendo que sua conduta está não apenas eticamente correta, mas juridicamente blindada.
“O prontuário não é apenas um registro de doenças, mas sim o livro de memórias de uma batalha travada em conjunto pelo médico e pelo paciente. Uma palavra mal escrita ou omitida pode ser tão letal quanto um bisturi mal empunhado na sala de operações.” — Aforismo da Educação Médica Cirúrgica.
Gostou ❔Nos deixe um comentário ✍️ , compartilhe em suas redes sociais e|ou mande sua dúvida pelo 💬 Chat On-line em nossa DM do Instagram.
LIFE AS A SURGEON
Life as a Surgeon
Surgical careers begin long before one is known as a surgeon. Medicine in general, and surgery in particular, is competitive from the start. As the competition begins, in college or earlier, students are confronted with choices of doing what interests them and what they may truly enjoy vs doing what is required to get to the next step. It is easy to get caught up in the routine of what is required and to lose track of why one wanted to become a doctor, much less a surgeon, in the first place. The professions of medicine and surgery are vocations that require extensive knowledge and skill. They also require a high level of discretion and trustworthiness. The social contract between the medical profession and the public holds professionals to very high standards of competence and moral responsibility. Tom Krizek goes on to explain that a profession is a declaration of a way of life ‘‘in which expert knowledge is used not primarily for personal gain, but for the benefit of those who need that knowledge.’’
For physicians, part of professionalism requires that when confronted with a choice between what is good for the physician and what is good for the patient, they choose the latter. This occurs and is expected sometimes to the detriment of personal good and that of physicians’ families. Tom Krizek even goes so far as to question whether surgery is an ‘‘impairing profession.’’ This forces one to consider the anticipated lifestyle. In sorting this out, it is neither an ethical breach nor a sign of weakness to allocate high priority to families and to personal well-being. When trying to explain why surgery may be an impairing profession, Krizek expands with a cynical description of the selection process. Medical schools seek applicants with high intelligence; responsible behavior; a studious, hard-working nature; a logical and scientific approach to life and academics; and concern for living creatures. He goes further to explain that in addition to these characteristics, medical schools also look for intensity and drive, but are often unable to make distinctions among those who are too intense, have too much drive, or are too ingratiating.
Medical School
There are many ethical challenges confronting medical students. As they start, medical students often have altruistic intentions, and at the same time are concerned with financial security. The cost of medical education is significant. This can encourage graduates to choose specialty training according to what will provide them the most expedient means of repaying their debt. This can have a significant, and deleterious, impact on the health care system in that the majority of medical graduates choose to pursue specialty training, leaving a gap in the availability of primary care providers. As medical students move into their clinical training, they begin interacting with patients. One concern during this time is how medical students should respond and carry on once they believe that a mistake on their part has resulted in the injury or death of another human being. In addition, the demands of studying for tests, giving presentations, writing notes, and seeing patients can be overwhelming. The humanistic and altruistic values that medical students have when they enter medical school can be lost as they take on so much responsibility. They can start to see patient interactions as obstacles that get in the way of their other work requirements. During their clinical years, medical students decide what field they will ultimately pursue. For students to make an informed decision about a career in surgery, they need to know what surgeons do, why they do it, and how surgery differs from other branches of medicine. It is important for them to be aware of what the life of a surgeon entails and whether it is possible for them to balance a surgical career with a rewarding family life.
Surgical Residency
Beginning residents are confronted with a seemingly unbearable workload, and they experience exhaustion to the point where the patient may seem like ‘‘the enemy.’’ At the same time, they must learn how to establish strong trusting relationships with patients. For the first time, they face the challenge of accepting morbidity and death that may have resulted directly from their own actions. It is important that residents learn ways to communicate their experience to friends and family, who may not understand the details of a surgeon’s work but can provide valuable support. The mid-level resident confronts the ethical management of ascending levels of responsibility and risks, along with increasing emphasis on technical knowledge and skills. It is at this level that the surgical education process is challenged to deal with the resident who does not display the ability to gain the skills required to complete training as a surgeon. Residents at this level also must deal with the increasing level of responsibility to the more junior residents and medical students who are dependent on them as teacher, organizer, and role model. All of this increasing responsibility comes at a time when the resident must read extensively, maintain a family life, and begin to put long-range plans into practice in preparation for the last rotation into the chosen final career path. The senior surgical resident should have acquired the basics of surgical technique and patient management, accepting nearly independent responsibility for patient care. The resident at this level must efficiently and fairly coordinate the functioning team, engage in teaching activities, and work closely with all complements of the staff. As far as ethics education is concerned, residents at this stage should be able to teach leadership, teamwork, and decision-making. They should be prepared to take on the value judgments that guide the financial and political aspects of the medical and surgical practice.
The Complete Surgeon
The trained surgeon must be aware of the need to differentiate between the business incentives of medical care and doing what is right for a sick individual. As financial and professional pressures become more intense, the challenge increases to appropriately prioritize and balance the demands of patient care, family, education, teaching, and research. For example, how does the surgeon deal with the choice between attending a child’s graduation or operating on an old patient who requests him rather than an extremely well-trained associate who is on call? How many times do surgeons make poor choices with respect to the balance of family vs work commitments? Someone else can
competently care for patients, but only parents can be uniquely present in the lives of their children. Time flies, and surgeons must often remind themselves that their lives and the lives of their family members are not just a dress rehearsal.
Knowing When to Quit
A 65-year-old surgeon who maintains a full operating and office schedule, is active in community and medical organizations, and has trained most of her surgical colleagues is considering where to go next with her career. Recently, her hospital acquired the equipment to allow robotic dissection in the area where she does her most complicated procedures. She has just signed up to learn this new technology, but is beginning to reflect on the advisability of doing this. How long should she continue at this pace, and how does she know when to slow down and eventually quit operating and taking the responsibility of caring for patients? Murray Brennan summarizes the dilemma of the senior surgeon well. The senior surgeon is old enough and experienced enough to do what he does well. He yearns for the less complicated days where he works and is rewarded for his endeavors. He becomes frustrated by restrictive legislation, the tyranny of compliance, and the loss of autonomy. Now regulated, restricted, and burdened with compliance, with every medical decision questioned by an algorithm or guideline, he watches his autonomy of care be ever eroded. Frustrated at not being able to provide the care, the education, and the role model for his juniors, he abandons the challenge.
Finishing with Grace
Each surgeon should continuously map a career pathway that integrates personal and professional goals with the outcome of maintaining value, balance, and personal satisfaction throughout his or her professional career. He or she should cultivate habits of personal renewal, emotional self-awareness, and connection with colleagues and support systems, and must find genuine meaning in work to combat the many challenges. Surgeons also need to set an example of good health for their patients. Maintaining these values and healthy habits is the work of a lifetime. Rothenberger describes the master surgeon as a person who not only knows when rules apply, recognizes patterns, and has the experience to know what to do, but also knows when rules do not apply, when they must be altered to fit the specifics of an individual case, and when inaction is the best course of action. Every occasion is used to learn more, to gain perspective and nuance. In surgery, this is the rare individual who puts it all together, combining the cognitive abilities, the technical skills, and the individualized decision-making needed to tailor care to a specific patient’s illness, needs, and preferences despite incomplete and conflicting data. The master surgeon has an intuitive grasp of clinical situations and recognizes potential difficulties before they become major problems. He prioritizes and focuses on real problems. He possesses insight and finds creative ways to manage unusual and complex situations. He is realistic, self-critical, and humble. He understands his limitations and is willing to seek help without hesitation. He adjusts his plans to fit the specifics of the situation. He worries about his decisions, but is emotionally stable.
Ethics in Surgery : R.I.S.K.
Renewed public attention is being paid to ethics today. There are governmental ethics commissions, research ethics boards, and corporate ethics committees. Some of these institutional entities are little more than window dressing, whereas others are investigative bodies called into being, for example, on suspicion that financial records have been altered or data have been presented in a deceptive manner. However, many of these groups do important work, and the fact that they have been established at all suggests that we are not as certain as we once were, or thought we were, about where the moral boundaries are and how we would know if we overstepped them. In search of insight and guidance, we turn to ethics. In the professions, which are largely self-regulating, and especially in the medical profession, whose primary purpose is to be responsive to people in need, ethics is at the heart of the enterprise.
Responsibility to the patient in contemporary clinical ethics entails maximal patient participation, as permitted by the patient’s condition, in decisions regarding the course of care. For the surgeon, this means arriving at an accurate diagnosis of the patient’s complaint, making a treatment recommendation based on the best knowledge available, and then talking with the patient about the merits and drawbacks of the recommended course in light of the patient’s life values. For the patient, maximal participation in decision making means having a conversation with the surgeon about the recommendation, why it seems reasonable and desirable, what the alternatives are, if any, and what the probable risks are of accepting the recommendation or pursuing an alternative course.
This view of ethically sound clinical care has evolved over the latter half of the 20th century from a doctor-knows-best ethic that worked reasonably well for both patients and physicians at a time when medical knowledge was limited and most of what medicine could do for patients could be carried in the doctor’s black bag or handled in a small, uncluttered office or operating room. What practical steps can be taken by clinicians to evaluate patient attitudes and behavior relative to the patient’s cultural context so that the physician and patient together can reach mutually desired goals of care? Marjorie Kagawa-Singer and her colleagues at the University of California, Los Angeles, developed a useful tool for ascertaining patients’ levels of cultural influence. It goes by the acronym RISK:
Resources: On what tangible resources can the patient draw, and how readily available are they?
Individual identity and acculturation: What is the context of the patient’s personal circumstances and her degree of integration within her community?
Skills: What skills are available to the patient that allow him to adapt to the demands of the condition?
Knowledge: What can be discerned from a conversation with the patient about the beliefs and customs prevalent in her community and relevant to illness and health, including attitudes about decision making and other issues that may affect the physician-patient relationship.
Leadership in SURGICAL TEAM

Leadership is a process of social influence in which one person can enlist the aid and support of others in the accomplishment of a common task. Successful leaders can predict the future and set the most suitable goals for organizations. Effective leadership among medical professionals is crucial for the efficient performance of a healthcare system. Recently, as a result of various events and reports such as the ‘Bristol Inquiry’, and ‘To Err is Human’ by the Institute of Medicine, the healthcare organizations across different regions have emphasized the need for effective leadership at all levels within clinical and academic fields. Traditionally, leadership in clinical disciplines needed to display excellence in three areas: patient care, research and education.
Within the field of surgery, the last decade has seen various transformations such as technology innovation, changes to training requirements, redistribution of working roles, multi-disciplinary collaboration and financial challenges. Therefore, the current concept of leadership demands to set up agendas in line with the changing healthcare scenario. This entails identifying the needs and initiating changes to allow substantive development and implementation of up-to-date evidence. This article delineates the definition and concept of leadership in surgery. We identify the leadership attributes of surgeons and consider leadership training and assessment. We also consider future challenges and recommendations for the role of leadership in surgery.
PRINCIPLES OF LEADERSHIP FOR GENERAL SURGEONS
“Not only SURGEONS…”

“… We need a system… which will produce not only surgeons but surgeons of the highest type,…men to study surgery and to devote their energy and their lives to raising the standard of surgical science…”
WS Halsted – Bull Johns Hopkins Hosp 15: 267, 1904.
A cirurgia é uma forma de terapia para as doenças que é motivada pelo CORAÇÃO, planejada na CABEÇA e executada pelas MÃOS.
“A cirurgia é uma forma de terapia para as doenças que é motivada pelo CORAÇÃO, planejada na CABEÇA e executada pelas MÃOS.”
Prof . Phd. Tom DeMeester
DEFINIÇÃO DE CIRURGIA (By Tom DeMeester / Gastrão 2012)
O RELATO CIRÚRGICO
A Arte e a Ciência da Documentação no Bloco Operatório
Autor: Prof. Dr. Ozimo Gama (Tempo de Leitura: 10 minutos)
Introdução
Na prática da cirurgia do aparelho digestivo, existe um aforismo não escrito, mas implacável: a cirurgia não termina quando o último ponto é dado na pele, mas sim quando o relato cirúrgico é assinado. O relato (ou descrição) cirúrgico é o documento médico-legal mais importante do perioperatório. Ele é o testemunho definitivo e detalhado de tudo o que ocorreu dentro das portas cerradas do centro cirúrgico. Infelizmente, é comum observarmos descrições feitas de forma apressada, “oficiosa” ou sumariíssima. O uso de frases genéricas como “cirurgia realizada pela técnica habitual” deve ser criticado com veemência e banido da nossa prática. Tais descrições padronizadas omitidas não apenas empobrecem a ciência cirúrgica, perdendo valiosos detalhes para consultas e pesquisas, mas também representam um verdadeiro suicídio jurídico em caso de litígio. O ato cirúrgico exige uma dissertação minuciosa e fiel à realidade biológica e técnica enfrentada.
A Anatomia de um Relato Perfeito
A elaboração da descrição cirúrgica não deve ser um fardo burocrático, mas um exercício de reflexão. Pela sua importância, este relatório pode e deve ser redigido em um momento de calma, propício à clareza mental e ao zelo pela legibilidade. Para garantir a eficácia documental, científica e legal, o relato cirúrgico deve obrigatoriamente conter a seguinte estrutura:
1. Cabeçalho e Identificação Exaustiva
- Identificação do Paciente: Nome completo, idade, número de prontuário (registro hospitalar) e leito.
- Equipe Cirúrgica: Nome do cirurgião principal, 1º e 2º auxiliares, instrumentador(a) e equipe de anestesiologia. A omissão de membros da equipe é uma falha ética grave.
- Procedimento e Diagnóstico: Nome técnico claro e completo da cirurgia proposta e da cirurgia efetivamente realizada. Registro da condição patológica que motivou a intervenção, bem como afecções concomitantes encontradas.
- Cronometria: Hora exata do início da incisão e hora do término da operação (fechamento cutâneo).
2. O Cenário e o Acesso
O relato deve descrever como o paciente foi preparado:
- Posição e Preparo: Posição do paciente na mesa (ex: decúbito dorsal, posição de Lloyd-Davies), uso de coxins de proteção (vital para evitar alegações de lesões de nervos periféricos), e os produtos utilizados para a antissepsia da pele.
- Via de Acesso: Descrição detalhada da incisão (ex: mediana supraumbilical, incisão de Mercedes) ou do posicionamento exato dos trocartes na cirurgia laparoscópica/robótica.
3. A Dissertação Técnica (O Ato em Si)
É aqui que a “técnica habitual” deve dar lugar à precisão milimétrica:
- Achados e Aspecto da Afecção: Descrever o grau de inflamação, fibrose, disseminação tumoral, presença de ascite ou aderências. O que os seus olhos viram ao abrir a cavidade?
- Tática e Técnica Operatória: Descrever o passo a passo. Como os ligamentos foram seccionados? Onde a artéria foi ligada? Houve uso de eletrocautério (monopolar/bipolar) ou energia ultrassônica?
- Fios e Suturas: Especificar os tipos de fios (ex: Polidioxanona 3-0, Polipropileno 1), o tipo de sutura (contínua, separada, invaginante) e o uso de grampeadores mecânicos (marca e cor da carga).
Aplicação na Cirurgia Digestiva: Prevenção e Rastreabilidade
No contexto das operações do aparelho digestivo, frequentemente lidamos com ressecções de órgãos, anastomoses e potencial de contaminação.
- Exames Transoperatórios: Relatar a realização de Colangiografia Intraoperatória (descrevendo seus achados: “ausência de falhas de enchimento, passagem livre de contraste para o duodeno”) ou de ultrassonografia intraoperatória.
- Gestão de Peças e Biópsias: Deve constar explicitamente o envio de peças cirúrgicas, linfonodos ou secreções colhidas para exame histopatológico e/ou cultura.
- Controle de Gaze e Instrumental: É mandatório registrar que a equipe de enfermagem (circulante/instrumentador) realizou e confirmou a contagem dupla de todas as compressas, gazes e instrumentais antes do fechamento da cavidade. Isso isenta a equipe nos tristes casos de corpos estranhos retidos (gossipiboma).
- Intercorrências e Acidentes: Qualquer lesão inadvertida (ex: lesão esplênica ao tracionar o estômago), sangramentos acima do esperado ou instabilidade hemodinâmica devem ser relatados com transparência, bem como as medidas táticas adotadas para a sua resolução.
Pontos-Chave para a Prática Diária
- Fuja do “Control C + Control V”: O relato padrão pré-descrito é injustificável em qualquer caso. Cada ser humano possui uma anatomia única; cada cirurgia é um evento singular.
- Medicina Legal e Traumas: Em lesões por arma branca ou de fogo, o relato deve descrever rigorosamente os trajetos internos. Projéteis ou objetos extraídos devem ser descritos, rotulados e entregues à autoridade policial/instituto médico-legal com protocolo de recebimento assinado.
- Desenhos Esquemáticos: Sempre que possível ou quando o sistema do prontuário permitir, a inclusão de esquemas anatómicos desenhados pelo cirurgião eleva imensamente o valor elucidativo do documento.
Conclusões Aplicadas
A descrição cirúrgica bem executada é um pilar da credibilidade profissional do cirurgião. É ela que justifica a complexidade do ato perante o faturamento hospitalar e os planos de saúde. É ela que orienta o oncologista sobre o estadiamento patológico. E, acima de tudo, é ela o escudo protetor da equipe em caso de demandas judiciais ou sindicâncias ético-profissionais. Criticar as descrições sumárias e incentivar a literatura cirúrgica detalhada nos prontuários é um dever de todos os preceptores de residência médica. Um relato rico e minucioso reflete não apenas o rigor técnico, mas o respeito sagrado do cirurgião pela história daquele paciente.
“Ex nihilo nihil fit.” (Do nada, nada surge). — Princípio filosófico. Na cirurgia moderna, aquilo que não foi detalhadamente escrito, juridicamente e cientificamente, nunca aconteceu.
Gostou ❔Nos deixe um comentário ✍️ , compartilhe em suas redes sociais e|ou mande sua dúvida pelo 💬 Chat On-line em nossa DM do Instagram.
VALORES ÉTICOS DOS ESTAGIÁRIOS DA CLÍNICA CIRÚRGICA
EXCELÊNCIA
Nunca baixar os seus padrões pessoais e profissionais. Fazer sempre o melhor, NÃO SOMENTE O POSSÍVEL.
Fazer sempre a coisa certa, mesmo quando ninguém está olhando.
RESPONSABILIDADE
Cumprir rigorosamente as atribuições em relação aos cuidados com os pacientes do serviço.
Ser uma força positiva com comprometimento na melhor assistência ao paciente.
DISCIPLINA
É a construção diária do seu objetivo.
O sucesso vem um pequeno passo de cada vez. O amanhã começa agora.

Turma 02 de RM Cirurgia Geral (HTLF)

Dr Antonio Filho (UEMA)
Dr Arimatéia Morales (UESPI)
Dra Livia Andrade (UFMA)
Dra Maura Calazeiras (UNICEUMA – APROVADA EM COLOPROCTOLOGIA NA UFCE)
Dr Igor Neiva (UNICEUMA – APROVADO EM ONCOLOGIA CIRÚRGICA NO INCA – RJ)
A todos os ex-residentes desejamos boa sorte e muitas realizações nesta nova etapa profissional.
Surgical Rotation: 5 PRINCIPLES

1.Getting along with the nurses.
The nurses do know more than the rest of us about the codes, routines, and rituals of making the wards run smoothly. They may not know as much about pheochromocytomas and intermediate filaments, but about the stuff that matters, they know a lot. Acknowledge that, and they will take you under their wings and teach you a ton!
2. Helping out.
If your residents look busy, they probably are. So, if you ask how you can help and they are too busy even to answer, asking again probably would not yield much. Always leap at the opportunity to shag x-rays, track down lab results, and retrieve a bag of blood from the bank. The team will recognize your enthusiasm and reward your contributions.
3. Getting scutted.
We all would like a secretary, but one is not going to be provided on this rotation. Your residents do a lot of their own scut work without you even knowing about it. So if you feel like scut work is beneath you, perhaps you should think about another profession.
4. Working hard.
This rotation is an apprenticeship. If you work hard, you will get a realistic idea of what it means to be a resident (and even a practicing doctor) in this specialty. (This has big advantages when you are selecting a type of internship. Staying in the loop. In the beginning, you may feel like you are not a real part of the team. If you are persistent and reliable, however, soon your residents will trust you with more important jobs. Educating yourself, and then educating your patients. Here is one of the rewarding places (as indicated in question 1) where you can soar to the top of the team. Talk to your patients about everything (including their disease and therapy), and they will love you for it.
5. Maintaining a positive attitude.
As a medical student, you may feel that you are not a crucial part of the team. Even if you are incredibly smart, you are unlikely to be making the crucial management decisions. So what does that leave: attitude. If you are enthusiastic and interested, your residents will enjoy having you around, and they will work to keep you involved and satisfied. A dazzlingly intelligent but morose complainer is better suited for a rotation in the morgue. Remember, your resident is likely following 15 sick patients, gets paid less than $2 an hour, and hasn’t slept more than 5 hours in the last 3 days. Simple things such as smiling and saying thank you (when someone teaches you) go an incredibly long way and are rewarded on all clinical rotations with experience and good grades.
Having fun! This is the most exciting, gratifying, rewarding, and fun profession and is light years better than whatever is second best (this is not just our opinion).
By: Alden H. Harken MDProfessor and Chair, Department of Surgery, University of California, San Francisco–East Bay, Oakland, California, Chief of Surgery, Department of Surgery, Alameda County Medical Center, Oakland, California
AVALIAÇÃO PRÉ-OPERATÓRIA
MEDICINA BASEADA EM EVIDÊNCIA_AVALIAÇÃO PRÉ_OPERATÓRIA

O médico CIRURGIÃO realiza a avaliação pré-operatória e define a necessidade de avaliação complementar, considerando a otimização das condições clínicas do paciente e a realização de exames complementares. Pacientes hígidos, com idade inferior a 40 anos, sem fatores de risco detectados na anamnese e no exame físico, a serem submetidos a cirurgias de pequeno porte, após a avaliação clínica básica poderão ser encaminhados à cirurgia após avaliação do Anestesiologista. Porém, nos casos em que o paciente tenha alguma comorbidade, idade maior de 60 anos, estado físico ASA II ou acima, obesidade, dependência funcional ou cirurgia de médio ou grande porte, estará indicado avaliação pré-operatória mais pormenorizada .
“poderosos além de qualquer medida…”

Nosso medo mais profundo não é o de sermos inadequados. Nosso medo mais profundo é que somos poderosos além de qualquer medida. É a nossa luz, não nossa escuridão, que mais nos assusta. Nós nos perguntamos: Quem sou eu para ser brilhante, maravilhoso, talentoso e fabuloso? Na verdade, quem não quer que você seja? Você é um filho de Deus. Seu papel pequeno não serve ao mundo. Não há nada de iluminado em se encolher, para que outras pessoas não se sintam inseguros ao seu redor. Estamos todos feitos para brilhar, como as crianças. Nascemos para manifestar a glória de Deus que está dentro de nós. Não é apenas em alguns de nós, está em todos. E conforme deixamos nossa própria luz brilhar, inconscientemente damos às outras pessoas permissão para fazer o mesmo. Como estamos libertamos do nosso medo, nossa presença, automaticamente, libera os outros.
Esse texto é atribuído a Marianne Williamson, uma autora e palestrante americana. A passagem faz parte de seu livro “A Return to Love: Reflections on the Principles of A Course in Miracles” (1992). Williamson explora temas de autoaceitação, potencial humano e espiritualidade, incentivando as pessoas a reconhecerem e expressarem sua luz interior. A citação destaca a ideia de que o verdadeiro medo não está em nossa inadequação, mas no poder e potencial que temos para impactar positivamente o mundo ao nosso redor.
Safe Surgery Save Lives

Evento Adverso (EA) é definido de acordo com a International Classification for Patient Safety proposta pela World Alliance for Patient Safety da Organização Mundial de Saúde (OMS) como incidente que resulta em dano (harm) ao paciente. Incidente definido como evento ou circunstância que poderia ter causado ou que resultou desnecessariamente em dano ao paciente e evento como algo que acontece com ou envolve o paciente. Os eventos adversos (EAs) têm estimativa de ocorrência em 4 a 16% de todos os pacientes hospitalizados, sendo que mais de metade nos cuidados cirúrgicos, dos quais acima de 50% são evitáveis. A ocorrência de EAs é considerada um problemade importância internacional sendo crescente o envolvimento de pesquisadores,profissionais de saúde e gestores de saúde na avaliação de EAs e inúmeras as instituições,redes de relacionamento e websites referentes ao tema.
Em 2004, expressando a preocupação mundial com a segurança de pacientes, foi criada pela OMS a World Alliance for Patient Safety tendo como elemento central a formulação do Global Patient Safety Challenge, que engloba temas representativos dos principais aspectos dos riscos relacionados com a assistência à saúde, considerados relevantes para os países membros da OMS. O primeiro tema selecionado foi infecção associada à prestação de serviço em saúde, seguido de segurança dos cuidados cirúrgicos,tendo como objetivo prevenir erros, evitar danos e salvar vidas. O número de cirurgias de maior porte realizadas anualmente no mundo foi estimado pela OMS em 234 milhões, o que corresponde a uma cirurgia para cada 25 pessoas.
Cirurgia de maior porte inclui qualquer procedimento realizado na sala de cirurgia envolvendo incisão, excisão, manipulação, ou sutura de tecido que geralmente requer anestesia geral ou regional, ou sedação profunda para controlar a dor. Em países industrializados complicações ocorrem em 3 – 16% dos procedimentos cirúrgicos realizados em pacientes internados, com taxa de mortalidade de 0,4 – 0,8%. Estudos realizados em países em desenvolvimento estimam uma taxa de mortalidade de 5 a 10% em pacientes submetidos à cirurgia de maior porte. A segurança em cirurgia emerge como importante preocupação para a saúde pública global. Cirurgia é um dos mais complexos e caros serviços prestados pelos sistemas de saúde.
Nos países em desenvolvimento , o mau estado da infraestrutura e dos equipamentos; os problemas quanto ao suprimento e à qualidade de medicamentos e de material médico-cirúrgico; as falhas na gestão da organização e no controle de infecção; o desempenho insatisfatório dos profissionais devido à baixa motivação ou à deficiência na capacitação técnica; as falhas no correto diagnóstico pré-operatório; as deficiências na consulta pré-anestésica, e o subfinanciamento dos custos operacionais dos serviços de saúde, tornam a probabilidade de ocorrência de eventos adversos muito maior do que em países industrializados.
Veja alguns dados:
§4% pacientes sofrem algum tipo de dano no Hospital
§70% dos eventos adversos provocam uma incapacidade temporal
§14% dos incidentes são mortais
§60% são evitáveis
World Alliance for Patient Safety : forward programme. World Health Organization 2004, apud: Harvard Medical Practice Study in 1991
Eventos Adversos na Clínica Cirúrgica
EVENTOS ADVERSOS # COMPLICAÇÕES

Introdução
O termo “Evento Adverso (EA)” cirúrgico é relativamente novo, mas o conceito de monitoramento dos resultados cirúrgicos, incluindo complicações pós-operatórias, é muito antigo. Desde 1732, existem referências a sistemas de coleta de informações hospitalares. Na Grã-Bretanha, estatísticas vitais datam de 1838, e já em 1850, a associação entre higiene das mãos e a transmissão de infecções foi estabelecida. Em 1854, os riscos de má higiene nos hospitais foram destacados, e em 1910, Ernest Codman defendeu a avaliação rotineira dos resultados negativos em cirurgias para melhorar a qualidade da assistência. Nos anos 1990, o interesse em erros e danos relacionados à saúde cresceu, mudando o foco das pesquisas para estratégias de enfrentamento e uma abordagem sistêmica ou organizacional.
Epidemiologia
Os EAs cirúrgicos contribuem significativamente para a morbidade pós-operatória, e sua avaliação e monitoramento frequentemente são imprecisos. Com a redução do tempo de permanência hospitalar e o aumento do uso de técnicas cirúrgicas inovadoras, especialmente minimamente invasivas e endoscópicas, a eficiência no monitoramento dos eventos adversos torna-se crucial. Revisões recentes identificaram que os EAs são desfavoráveis, indesejáveis, prejudiciais, impactam o paciente e estão associados ao processo de assistência à saúde, mais do que a um processo natural de doenças. A análise dos EAs é complexa devido à variabilidade dos sistemas de registro e às diversas definições na literatura científica para complicações pós-operatórias.
Custo e Efeitos de Medicina Legal
As complicações pós-operatórias resultam da interação de fatores dependentes do paciente, sua enfermidade e a atenção à saúde recebida. O estudo dos EAs cirúrgicos é relevante pela sua frequência, impacto considerável sobre a saúde dos pacientes e repercussão econômica no gasto social e sanitário. Além disso, os EAs servem como instrumento de avaliação da qualidade da assistência. Eventos adversos evitáveis, suscetíveis a intervenções de prevenção, são de maior interesse para a saúde pública. EAs cirúrgicos estão relacionados a acidentes intra-operatórios, complicações pós-operatórias imediatas ou tardias e ao fracasso da intervenção cirúrgica.
Nos Estados Unidos, um estudo em hospitais de Colorado e Utah calculou uma taxa de incidência de 1,9% para pacientes internados, e 3,0% para pacientes submetidos a cirurgia ou parto, com 54% dos EAs considerados evitáveis. Em 5,6% dos casos, os EAs resultaram em óbito. Na Austrália, a prevalência de internações cirúrgicas associadas a um EA foi de 21,9%, com 47,6% dos EAs classificados como altamente evitáveis. Na Espanha, um estudo em cirurgias de parede abdominal encontrou complicações em 16,32% dos pacientes.
Diferença entre Complicação e Evento Adverso
Complicações pós-operatórias surgem da interação entre fatores do paciente, da doença e da atenção recebida. Eventos Adversos, por outro lado, são desfavoráveis, indesejáveis e prejudiciais, resultantes do processo de assistência à saúde. Embora ambos afetem a recuperação, os EAs são frequentemente evitáveis com intervenções preventivas.
Conclusão
A segurança em cirurgia no Brasil é preocupante. Em 2003, 52,5% dos hospitais inspecionados pelo Conselho Regional de Medicina de São Paulo apresentaram condições físicas inadequadas. Hospitais de pequeno porte, que representam 62% dos estabelecimentos, enfrentam desafios significativos em termos de complexidade e densidade tecnológica.
Como Ernest Codman sabiamente afirmou: “A melhoria na assistência médica só pode ser alcançada com a análise sistemática dos resultados”. Esta frase histórica ressoa ainda hoje, destacando a importância da avaliação e monitoramento dos EAs cirúrgicos para a melhoria contínua da qualidade e segurança na assistência à saúde.
World’s Greatest Surgeon
 On July 12, 2008, the world lost an incredible talent. A renegade physician, a pioneer, the father of open-heart surgery, and perhaps the best surgeon who ever lived, Dr. Michael DeBakey died of natural causes at 99. Because of his groundbreaking research, cutting-edge medical devices and maverick approach to cardiac surgery, DeBakey literally changed the rules of the game and thousands of lives are saved each day.
On July 12, 2008, the world lost an incredible talent. A renegade physician, a pioneer, the father of open-heart surgery, and perhaps the best surgeon who ever lived, Dr. Michael DeBakey died of natural causes at 99. Because of his groundbreaking research, cutting-edge medical devices and maverick approach to cardiac surgery, DeBakey literally changed the rules of the game and thousands of lives are saved each day.
What can we learn from Michael DeBakey’s life and career?
1. Build your brand.
With a career that spanned more than 70 years, DeBakey built a reputation for being indispensable. His patients included everyone from the ordinary person next door and people with no means to a list of Who’s Who among world leaders. Presidents Kennedy, Johnson and Nixon, President Boris Yeltsin, King Hussein of Jordan, the Shah of Iran, Turkish President Turgut Ozal, just to name a few, engaged DeBakey because they knew he was the best. The Journal of the American Medical Association said in 2005, “Many consider Michael E. DeBakey to be the greatest surgeon ever.” Is your personal brand strong enough that if you left your company, colleagues and customers would have a difficult time getting along without you?
2. Be a guru, thought leader, industry expert.
Dr. DeBakey published more than 1,000 medical reports, research papers, chapters and books on topics related to cardiovascular medicine. He helped establish the National Library of Medicine, the world’s largest and most prestigious repository of medical archives. DeBakey played a key role in organizing a specialized medical center system to treat soldiers returning from the war. This system is now the Veterans’ Administration Medical Center System. For his numerous contributions Dr. DeBakey was awarded the Presidential Medal of Freedom, the Congressional Gold Medal, Congress’ highest civilian honor, the National Medal of Science, the country’s highest scientific award, and The United Nations Lifetime Achievement Award. Do people see you as a guru in your field? How distinctive is your knowledge base? How well do you garner, contribute and leverage knowledge?
3. Never quit learning.
As a child, DeBakey was required to borrow a book from the library each week and read it. He read the entire Encyclopedia Britannica before entering high school. Overseeing cases, consulting with colleagues and mentoring younger surgeons, he made his mark on the world right up to the end. DeBakey performed his last surgery at age 90 and continued to travel the globe giving lectures. Perhaps you’re thinking, “Who would want a 90-year-old surgeon operating on them?” The answer could be, “Someone who’s performed more than 60,000 cardiovascular procedures in his career.” Do you have a reputation for lifelong learning, for continually adding value? When we stop bringing something new to the game, the game is over.
4. Risk more, gain more.
DeBakey took risks others weren’t willing to take to advance medicine. Tubing, clamps, pumps, protocols all bear the mark of DeBakey’s passion for innovation. Yet, product and process innovations often pull people out of their comfort zones and some of DeBakey’s early breakthroughs weren’t accepted initially—in fact they were ridiculed. For example, in 1939, when Drs. DeBakey and Alton Ochsner linked cigarette smoking to lung cancer, many in the medical community derided it. Then in 1964, the Surgeon General confirmed their findings and documented the cause and effect. There was also skepticism when DeBakey discovered that he could substitute parts of diseased arteries with synthetic (Dacron) grafts—a procedure that enables surgeons to repair aortic aneurysms in the chest and abdomen. He initially figured out how to stitch synthetic blood vessels on his wife’s sewing machine. Now the procedure is widely used. DeBakey was also the first to perform bypass surgery and the first to perform a successful removal of a blockage of the carotid (main) artery of the neck, a procedure that has become the standard protocol for treating stroke. The world is not changed by those who are unwilling to take risks. Is your passion for advancing your field by taking a risk bigger than your fear of rejection or making a mistake?
5. Refuse to sell out on your dream.
DeBakey developed an interest in medicine in his father’s pharmacy where he listened to physicians talk shop. The vision to become a doctor was clear, the question was, “what kind?” In 1932, there simply wasn’t anything you could do for heart disease, if a patient had a heart attack the long-term prognosis wasn’t good. While he was still in school in 1932, DeBakey invented the roller pump—a critical part of the heart-lung machine that takes over the functions of the heart and lungs during open-heart surgery. This not only created the era of open-heart surgery, it cemented DeBakey’s passion to make a mark in the world of cardiovascular medicine. Engagement is about pouring your heart, mind and soul into a dream that causes you to fire on all cylinders. Does your career fulfill your desires? Or, have you sacrificed a dream that could make you come alive for a life of duty and routine that simply “works”?
6. Play to your genius.
DeBakey said, “I like my work, very much. I like it so much that I don’t want to do anything else.” Most people who are happy in life spend time doing what they love. This usually makes them extremely good at what they do. Dr. DeBakey exemplified the power of what can happen when our work requires what we are good at and passionate about. Playing to your genius is about using your gifts and talents to pursue a passion that makes a significant contribution to the people and the world you serve. Playing to your genius also promotes autonomy and self-direction, cultivates commitment, stimulates personal growth and makes work fun. Are you engaged in work you’re good at and passionate about—work that makes a contribution and needs to be done? Or are you just biding time?
7. Balance passion with discipline and focus.
With regard to his patients, the indefatigable DeBakey had an uncompromising dedication to perfection. He was known as a taskmaster who set very high standards, yet he never demanded more from others than he demanded from himself. Heart surgeons who trained under DeBakey say he was hard to keep up with when making patient rounds. They joked that he was from another world because he could maintain his focus and intensity for hours. In a world of competing priorities and information overload it’s easy to lose focus and get distracted. But, if you are playing to your genius and doing what you love, it’s easier to be disciplined and maintain a maniacal focus. Are you disciplined? Do you have a maniacal focus? Would your customers (internal and external) say you are relentless when it comes to pursuing perfection?
8. Find a void and figure out how to fill it.
Michael DeBakey’s innovations are on par with the likes of Thomas Edison, Alexander Graham Bell, Jonas Salk, Henry Ford and Alfred Nobel. During World War II, he helped establish the mobile army surgical hospitals or MASH units. He was a key player in the development of artificial hearts, artificial arteries and bypass pumps that help keep patients alive who are waiting for transplants. He was among the first to recognize the importance of blood banks and transfusions. He also helped create more than 70 surgical instruments that made procedures easier and clinical outcomes more effective. If something couldn’t be done, DeBakey found a way to do it. In 1967, Dr. Christiaan Barnard performed the first human heart transplant in South Africa. Dr. DeBakey was among the first to begin doing the procedure in the United States. The problem was that recipients’ bodies rejected the new organs and death rates were high. In the 1980s cyclosporine, a new anti-rejection drug paved the way for organ transplants. Again, DeBakey was among the first to develop new protocols and advance the field of heart transplants. Where are the gaps in your organization or industry? What would happen if you developed a reputation for filling these voids?
9. Show people that their work matters.
Michael DeBakey is known not only for his prolific contributions to the medical field, but also as a symbol of hope and encouragement to his colleagues. Many years ago a colleague of ours shadowed Dr. DeBakey for a day at The Methodist Hospital in Houston, Texas. He was struck by DeBakey’s capacity to affirm each person he saw in the course of the day. In one particular encounter, DeBakey began chatting with an elderly janitor who was sweeping the floor. DeBakey asked the man about his wife and children. He told the older man, obviously not for the first time, that the hospital couldn’t function without the janitor because germs would spread, increasing the chances of infection in the hospital. Later in the day, our colleague tracked down the janitor and asked him, “What exactly do you do? Tell me about your job.” With pride, the janitor replied: “Dr. DeBakey and I? We save lives together.” He’s right. After all, consider what would happen to our healthcare systems if the cleaning crews went on strike. DeBakey understood that showing the janitor exactly how he contributes to a larger, more heroic cause is crucial. This creates a powerful dynamic. Realizing that he is working toward a worthy goal, the janitor’s perceptions about his work changed. It had new meaning and his enthusiasm for the job was rejuvenated. Great leaders make time to help people see how their work is connected to something bigger. For a surgeon like DeBakey, those five or ten minutes each day were costly, unless, of course, you consider the productivity generated by a janitor whose work has been transformed. Right now, how many people in your organization are engaged in work that five years from today no one will give a rip about? Can you make the link between what you do and a noble or heroic cause? Can you make this link for others?
10. Be generative—inspire others to pursue the cause.
Generativity is the care and concern for the development of future generations through teaching, mentoring, and other creative contributions. It’s about leaving a positive legacy. All great leaders are generative and Michael DeBakey was no exception. He inspired many medical students to pursue careers in cardiovascular surgery. His reputation brought many people to Baylor College of Medicine and helped transform it into one of the premier medical institutions in the world. DeBakey trained and mentored almost 1,000 surgeons and physicians. In 1976, his students founded the Michael E. DeBakey International Surgical Society. Many of his residents went on to serve as chairpersons and directors of their own successful academic surgical programs in the United States and around the world. Are the people you’ve touched in your career learning, growing and making a difference as a result of your influence? Have they been inspired to build a better world than the world they inherited? Michael DeBakey applied his problem-solving skills to many parts of medicine that have changed our way of life. Timothy Gardner, M.D., president of the American Heart Association said it well, “DeBakey’s legacy will live on in so many ways—through the thousands of patients he treated directly and through his creation of a generation of physician educators, who will carry his legacy far into the future. His advances will continue to be the building blocks for new treatments and surgical procedures for years to come.”
Michael DeBakey’s life and legacy proves that one person who chooses to play to their genius can change the world and make it a better place for all. What legacy will you leave behind?

O CIRURGIÃO (POEMA)
O CIRURGIÃO
Um corpo inerte aguarda sobre a mesa
Naquele palco despido de alegria.
O artista das obras efêmeras se apresenta.
A opereta começa, ausente de melodia
E o mascarado mudo trabalha com presteza.
Sempre começa com esperança e só términa com certeza.
Se uma vida prolonga, a outra vai-se escapando.
E nem sempre do mundo o aplauso conquistando
Assim segue o artista da obra traiçoeira e conquistas passageiras.
Há muito não espera do mundo os louros da vitória
Estudar, trabalhar é sua história, e a tua maior glória
Hás de encontrar na paz do dever cumprido.
Quando a vivência teus cabelos prateando
E o teu sábio bisturi, num canto repousando
Uma vez que sua missão vai terminando
Espera do bom Deus por tudo, a ti, seja piedoso.
SOIS VÓS INSTRUMENTO DA TUA OBRA.
.
Qual o momento certo? AGORA.
“So live your life that the fear of death can never enter your heart. Trouble no one about their religion; respect others in their view, and demand that they respect yours. Love your life, perfect your life, beautify all things in your life. Seek to make your life long and its purpose in the service of your people. Prepare a noble death song for the day when you go over the great divide. Always give a word or a sign of salute when meeting or passing a friend, even a stranger, when in a lonely place. Show respect to all people and grovel to none. When you arise in the morning give thanks for the food and for the joy of living. If you see no reason for giving thanks, the fault lies only in yourself. Abuse no one and no thing, for abuse turns the wise ones to fools and robs the spirit of its vision. When it comes your time to die, be not like those whose hearts are filled with the fear of death, so that when their time comes they weep and pray for a little more time to live their lives over again in a different way. Sing your death song and die like a hero going home.”

~ Chief Tecumseh (Poem from Act of Valor the Movie)
The Qualities of a GOOD SURGEON

Following is a list of Dr. Ephraim McDowell’s personal qualities described as “C” words along with evidence corroborating each of the characteristics.
Courageous: When he agreed to attempt an operation that his teachers had stated was doomed to result in death, he, as well as his patient, showed great courage.
Compassionate: He was concerned for his patient and responded to Mrs. Crawford’s pleas for help.
Communicative: He explained to his patient the details of her condition and her chances of survival so that she could make an informed choice.
Committed: He promised his patient that if she traveled to Danville, he would do the operation. He made a commitment to her care.
Confident: He assured the patient that he would do his best, and she expressed confidence in him by traveling 60 miles by horseback to his home.
Competent: Although lacking a formal medical degree, he had served an apprenticeship in medicine for 2 years in Staunton, Virginia, and he had spent 2 years in the study of medicine at the University of Edinburgh, an excellent medical school. In addition, he had taken private lessons from John Bell, one of the best surgeons in Europe. By 1809 he was an experienced surgeon.
Carefull: Despite the fact that 2 physicians had pronounced Mrs. Crawford as pregnant, he did a careful physical examination and diagnosed that she was not pregnant but had an ovarian tumor. He also carefully planned each operative procedure with a review of the pertinent anatomic details. As a devout Presbyterian, he wrote special prayers for especially difficult cases and performed many of these operations on Sundays.
Courteous: He was humble and courteous in his dealings with others. Even when he was publicly and privately criticized after the publication of his case reports, he did not react with vitriol. The qualities of character demonstrated by Dr. Ephraim McDowell 200 years ago are still essential for surgeons today.
Dr. Ephraim McDowell exemplified the essential qualities that define a great surgeon. His courage was evident when he accepted to perform an operation deemed fatal by his mentors, facing the unknown with determination. His compassion shone through in his genuine concern for the well-being of his patients, responding to cries for help with sensitivity and empathy. He was communicative, ensuring that his patients were well-informed about their conditions and the risks involved, enabling decisions based on knowledge. Additionally, Dr. McDowell demonstrated unwavering commitment to his patients, keeping promises and ensuring that each received the best possible care.
His confidence in his abilities, even without a formal degree, was supported by a robust education and a continuous dedication to learning. Dr. McDowell was competent, the result of years of study and practice, conducting meticulous physical examinations and planning each procedure with precision. His courtesy and humility in interactions, even in the face of criticism, showed a character that valued respect and integrity. These qualities, demonstrated two centuries ago, are timeless and continue to define ethical practice in modern surgery. As William Osler aptly stated, “The practice of medicine is an art, not a trade; a calling, not a business; a calling in which your heart will be exercised equally with your head.”
Etiqueta Médica : Postura Cirúrgica na U.T.I.
 A etiqueta no ambiente hospitalar vai além das regras de boa convivência. Ela oferece recursos para que os profissionais construam relacionamentos sólidos, além de ensiná-los a lidar com os “sabotadores da carreira”, como indiscrição e a falta de educação. Logo as atitudes no trabalho devem ser pautadas pelo bom senso, pelo bom gosto e pelo equilíbrio. Esses três fatores têm um único objetivo: fazer-nos pessoas melhores na convivência com os demais. Certamente, pensar muito antes de agir nos protege de escolhas equivocadas de comportamentos. As relações de trabalho e os ambientes hospitalares mudaram muito nos últimos anos, assim como as regras de convivência e as competências relacionais. Hoje, muitas empresas adotam estações de trabalho em que todos compartilham o mesmo espaço. Tudo o que se fala pode ser ouvido. A privacidade é muito menor, o que exige discrição. As atribuições das lideranças também evoluíram: em vez de mandar, os líderes devem convencer as suas equipes para serem respeitados. Outro desafio é promover a boa convivência entre gerações diferentes nas empresas. Os avanços tecnológicos exigem muito mais dos relacionamentos com colegas de todos os níveis. Portanto, o uso de emails, redes sociais e mensagens instantâneas, entre outros recursos, deve preservar sempre a cortesia, o respeito e a devida atenção ao outro. Sendo a “regra de platina” das relações humanas: trate os outros melhor do que você gostaria de ser tratado!
A etiqueta no ambiente hospitalar vai além das regras de boa convivência. Ela oferece recursos para que os profissionais construam relacionamentos sólidos, além de ensiná-los a lidar com os “sabotadores da carreira”, como indiscrição e a falta de educação. Logo as atitudes no trabalho devem ser pautadas pelo bom senso, pelo bom gosto e pelo equilíbrio. Esses três fatores têm um único objetivo: fazer-nos pessoas melhores na convivência com os demais. Certamente, pensar muito antes de agir nos protege de escolhas equivocadas de comportamentos. As relações de trabalho e os ambientes hospitalares mudaram muito nos últimos anos, assim como as regras de convivência e as competências relacionais. Hoje, muitas empresas adotam estações de trabalho em que todos compartilham o mesmo espaço. Tudo o que se fala pode ser ouvido. A privacidade é muito menor, o que exige discrição. As atribuições das lideranças também evoluíram: em vez de mandar, os líderes devem convencer as suas equipes para serem respeitados. Outro desafio é promover a boa convivência entre gerações diferentes nas empresas. Os avanços tecnológicos exigem muito mais dos relacionamentos com colegas de todos os níveis. Portanto, o uso de emails, redes sociais e mensagens instantâneas, entre outros recursos, deve preservar sempre a cortesia, o respeito e a devida atenção ao outro. Sendo a “regra de platina” das relações humanas: trate os outros melhor do que você gostaria de ser tratado!
Ao encaminhar o paciente no pós-operatório para U.T.I. o Cirurgião legalmente mantém sua responsabilidade sob os cuidados cirúrgicos deste paciente, sendo a partir daí um dos profissionais que participará na orientação das condutas clínicas relacionadas ao procedimento cirúrgico do paciente. Desta forma deve ficar á livre disposição dos INTENSIVISTAS para dirimir qualquer dúvida ou prestar orientações quanto a evolução cirúrgica do paciente em questão.
Alguns cuidados são importantes para serem lembrados nesta relação CIRURGIÃO e o Corpo Clínico das Unidades de TERAPIA INTENSIVA…
- Ao executar um procedimento cirúrgico, lembre-se que se algum evento adverso pode ocorrer, este um dia irá acontecer (Lei de Murphy). Prepara-se o pior possível. Se pensas que após uma complicação cirúrgica as coisas não podem piorar, acredite que podem. E serão justamente esta equipe de Especialistas que nos ajudaram a conduzir melhor o caso.
- Nada na Medicina permanece constante, em especial no pós-operatório, e nenhum órgão falha isoladamente.
- Cuidado com a Lei da Especialização: se fores um martelo, o resto do mundo é um prego. Aquele que pensa que sabe tudo, não sabe nada.
- Um “abdómen agudo cirúrgico” é diagnosticado após o exame físico por parte de um cirurgião EXPERIENTE e COMPROMETIDO, podendo ou não ser ratificado pelos exames complementares. Não existe nenhum teste complementar isolado para isso.
- Antes de solicitarmos um exame complementar, precisamos planejar o que faremos se for positivo ou negativo. Se as respostas forem iguais, não o solicitaremos. Corolário: Se o teste não altera a nossa estratégia, não solicitaremos.
- Não existe nenhum efeito adverso que não possa ser causado por um determinado fármaco. Se o fármaco não é essencial no tratamento, não usaremos.
- Geralmente a qualidade do cuidado prestado ao paciente é inversamente proporcional ao número de especialidades (consultores) envolvidos nesse caso particular. Todo paciente cirúrgico possui um único cirurgião responsável pelo procedimento em questão.
- Se as orientações médicas forem passíveis de má interpretação pela equipe multidisciplinar, elas certamente serão mal interpretadas. Portanto precisamos sempre nos perguntar: “Eu fui claro nas minhas orientações?”.
- Nunca ignore uma chamada de atenção de um dos membros da equipe Multidisciplinar, em especial do corpo de enfermagem. É função destes colegas nos informar. A nossa função é decidir. Seja cordial e serás retribuído da mesma maneira. Se fores desagradável, terás uma vida miserável. Jamais confunda o carteiro com a mensagem da carta.
- Se não sabes o que fazer, não faças nada e pede ajuda. Fazer mal não é melhor que não fazer nada. Pede e insiste na ajuda se tiveres dúvidas ou complicações que você nunca conduziu. Erros de inexperiência em doentes críticos podem ter consequências catastróficas.
Deixe nos comentários a sua contribuição.
BOM PLANTÃO.
Prof. Dr. Henrique Walter Pinotti (Gastrão 2009)

“A cirurgia lida com a VIDA, logo não existe cirurgia banal.”
A cirurgia do aparelho digestivo deve ser conceituada como ciência e arte que, através do progresso técnico e da melhor organização das sociedades, expandiu seus horizontes. Hoje, essa especialidade médica se aproxima cada vez mais do indivíduo, compreendendo suas enfermidades, emoções e função na sociedade. Ao cirurgião digestivo, protagonista dessa especialidade, cabe o papel não só de tratar eficientemente, mas também de conhecer as causas das doenças e criar atitudes preventivas. Além disso, deve considerar os ônus sociais e econômicos das enfermidades cirúrgicas e adotar uma visão bio-psico-social do paciente.
O fundamento Filosófico da Cirurgia Digestiva
Hipócrates, o Pai da Medicina, já havia estabelecido os elos entre medicina e filosofia. Ele afirmava: “O médico que é, ao mesmo tempo, filósofo assemelha-se aos deuses. Não há grande diferença entre a medicina e a filosofia, porque todas as qualidades do bom filósofo devem ser encontradas no médico: desinteresse, zelo, pudor, dignidade, seriedade, tranquilidade de julgamento, serenidade, decisão, pureza de vida, conhecimento do que é útil e necessário na vida, reprovação do que é mau, alma livre de suspeitas e devoção à divindade.” Claudius Galenus, conhecido como Galeno, complementou essa visão com sua vasta produção literária, afirmando que “o ótimo médico necessita ser também ótimo filósofo”. Para ele, a prática da medicina exigia um profundo conhecimento filosófico.
A Filosofia da Cirurgia
A filosofia como ciência lida com o saber racional, sendo uma reflexão crítica sobre os fundamentos do conhecimento e seus valores normativos: lógica, ética e estética. A Filosofia da Cirurgia é uma ciência cujos conhecimentos e objetivos transcendem os de outras filosofias, pois lida diretamente com a vida humana e toda a complexidade que sua prática requer. Conduzida sob o signo da ética, visa gerar felicidade para o operado e seus dependentes. Essa filosofia é robustecida tanto na direção individual quanto na missão social, especialmente quando o profissional possui grande sensibilidade humana e uma ampla formação técnica e ética. Enquanto no Direito existe o princípio de “tratar de maneira distinta os desiguais”, a Cirurgia, embora recomende procedimentos diferentes conforme a doença e o estado do paciente, trata igualmente os socialmente desiguais. Na doença, todos são iguais; o paciente anestesiado pertence ao mundo dos iguais.
Doutrina Filosófica da Cirurgia Digestiva
A doutrina da Filosofia da Cirurgia tem finalidades elevadas, superando as de muitas outras profissões, pois coloca as necessidades do paciente acima dos interesses pessoais. A prática cirúrgica, conduzida com ética e conhecimento profundo, busca não apenas a cura, mas o bem-estar e a felicidade do paciente e de seus familiares. A cirurgia é uma especialidade médica dedicada ao tratamento de doenças, traumas e complicações de saúde por meio de intervenções manuais e instrumentais realizadas por médicos especializados. No contexto da cirurgia digestiva, essas intervenções são focadas no sistema digestivo, englobando uma série de órgãos essenciais para a digestão, absorção de nutrientes e eliminação de resíduos do corpo.
O Sistema Digestivo e Suas Funções
O sistema digestivo começa na boca e se estende até o ânus, incluindo órgãos como intestino grosso e delgado, estômago, duodeno, faringe e fígado. Esses órgãos são responsáveis não apenas pela digestão dos alimentos, mas também pela absorção de nutrientes e eliminação de substâncias desnecessárias ao organismo. Todo o processo digestivo é regulado pelo sistema nervoso e por hormônios, com o cérebro desempenhando um papel crucial na percepção da fome e no início da digestão.
A Importância de Escolher um Especialista em Cirurgia do Aparelho Digestivo
Qualquer procedimento cirúrgico é delicado, exigindo uma combinação de conhecimentos técnicos, éticos e humanísticos. No campo da cirurgia do aparelho digestivo, essa responsabilidade é ainda maior devido à complexidade das doenças tratadas e à precisão exigida nas intervenções. Portanto, é fundamental que o cirurgião responsável tenha a formação e a experiência necessárias para oferecer o melhor cuidado possível aos pacientes.
Formação e Qualificação do Cirurgião do Aparelho Digestivo
Um cirurgião do aparelho digestivo é um profissional altamente capacitado, com pelo menos 10 anos de estudos obrigatórios, que envolvem:
- 6 anos de graduação em Medicina;
- 2 anos de Residência Médica em Cirurgia Geral;
- 2 anos de Residência Médica em Cirurgia do Aparelho Digestivo, regulamentada pelo Ministério da Educação (MEC) e pelo Conselho Federal de Medicina (CFM).
Esse período de treinamento permite ao cirurgião não apenas adquirir o conhecimento teórico, mas também desenvolver as habilidades práticas necessárias para realizar procedimentos complexos com segurança e eficiência. Além disso, o cirurgião do aparelho digestivo está habilitado a utilizar tanto técnicas convencionais quanto métodos minimamente invasivos, como a cirurgia laparoscópica e endoscopia diagnóstica, que resultam em menor tempo de recuperação e menos dor para o paciente.
Áreas de Atuação e Doenças Tratadas
Os cirurgiões do aparelho digestivo são especializados em diagnosticar, tratar e prevenir uma ampla gama de doenças que afetam os órgãos abdominais. Entre os principais tratamentos realizados por esses especialistas estão as cirurgias de câncer do estômago, esôfago, intestinos, reto, pâncreas, fígado, vesícula biliar e vias biliares. Esses profissionais não apenas realizam os procedimentos cirúrgicos para tratar esses tipos de câncer, mas também atuam na prevenção, oferecendo aconselhamento e exames regulares aos pacientes em risco.
Além disso, o cirurgião do aparelho digestivo trata diversas outras condições comuns, como:
- Refluxo gastroesofágico e esofagite;
- Hérnia de hiato e da parede abdominal;
- Obesidade mórbida (cirurgia bariátrica);
- Gastrite e úlcera gástrica/duodenal;
- Tumores malignos do aparelho digestivo;
- Transplante de Órgãos do Aparelho Digestivo;
- Pancreatite e cálculos biliares;
- Doença diverticular (diverticulite);
- Retocolite ulcerativa e doença de Crohn;
- Hemorróidas, fístulas e fissuras anais;
- Hérnias da parede abdominal, entre outras condições.
Escolhendo o Cirurgião
Antes de se submeter a qualquer procedimento cirúrgico, é crucial que o paciente verifique a formação e as qualificações do médico responsável. Aqui estão alguns pontos importantes a serem considerados:
- Formação Acadêmica: Certifique-se de que o médico possui os requisitos de formação necessários, incluindo residência em cirurgia do aparelho digestivo.
- Afiliado a Entidades Científicas: Verifique se o cirurgião é membro de alguma sociedade científica representativa, como o Colégio Brasileiro de Cirurgia Digestiva (CBCD) ou a Sociedade Brasileira de Cirurgia Bariátrica e Metabólica (SBCBM).
- Atualização Constante: O campo da medicina está sempre evoluindo, e é essencial que o cirurgião mantenha-se atualizado com os últimos avanços em sua área.
- Feedback de Pacientes: Converse com pacientes que já foram operados pelo médico para conhecer suas experiências e opiniões sobre o profissional.
Considerações Finais
A decisão de se submeter a uma cirurgia é sempre delicada, e a escolha do cirurgião é um passo fundamental para garantir o sucesso do procedimento. Procurar um especialista em cirurgia do aparelho digestivo, com a devida formação e experiência, pode fazer toda a diferença no resultado final. Além disso, é recomendável sempre buscar uma segunda opinião médica para garantir que o diagnóstico e o tratamento proposto sejam os mais adequados para sua condição de saúde.
Lembre-se: procure sempre um médico especialista e informe-se adequadamente antes de qualquer procedimento.
Gostou? ✍️ Deixe seu comentário, compartilhe em suas redes sociais ou envie suas dúvidas pelo 💬 Chat On-line em nossa DM do Instagram.