Critical View Of Safety

“The concept of the critical view was described in 1992 but the term CVS was introduced in 1995 in an analytical review of the emerging problem of biliary injury in laparoscopic cholecystectomy. CVS was conceived not as a way to do laparoscopic cholecystectomy but as a way to avoid biliary injury. To achieve this, what was needed was a secure method of identifying the two tubular structures that are divided in a cholecystectomy, i.e., the cystic duct and the cystic artery. CVS is an adoption of a technique of secure identification in open cholecystectomy in which both cystic structures are putatively identified after which the gallbladder is taken off the cystic plate so that it is hanging free and just attached by the two cystic structures. In laparoscopic surgery complete separation of the body of the gallbladder from the cystic plate makes clipping of the cystic structures difficult so for laparoscopy the requirement was that only the lower part of the gallbladder (about one-third) had to be separated from the cystic plate. The other two requirements are that the hepatocystic triangle is cleared of fat and fibrous tissue and that there are two and only two structures attached to the gallbladder and the latter requirements were the same as in the open technique. Not until all three elements of CVS are attained may the cystic structures be clipped and divided. Intraoperatively CVS should be confirmed in a “time-out” in which the 3 elements of CVS are demonstrated. Note again that CVS is not a method of dissection but a method of target identification akin to concepts used in safe hunting procedures. Several years after the CVS was introduced there did not seem to be a lessening of biliary injuries.
Operative notes of biliary injuries were collected and studied in an attempt to determine if CVS was failing to prevent injury. We found that the method of target identification that was failing was not CVS but the infundibular technique in which the cystic duct is identified by exposing the funnel shape where the infundibulum of the gallbladder joins the cystic duct. This seemed to occur most frequently under conditions of severe acute or chronic inflammation. Inflammatory fusion and contraction may cause juxtaposition or adherence of the common hepatic duct to the side of the gallbladder. When the infundibular technique of identification is used under these conditions a compelling visual deception that the common bile duct is the cystic duct may occur. CVS is much less susceptible to this deception because more exposure is needed to achieve CVS, and either the CVS is attained, by which time the anatomic situation is clarified, or operative conditions prevent attainment of CVS and one of several important “bail-out” strategies is used thus avoiding bile duct injury.
CVS must be considered as part of an overall schema of a culture of safety in cholecystectomy. When CVS cannot be attained there are several bailout strategies such a cholecystostomy or in the case of very severe inflammation discontinuation of the procedure and referral to a tertiary center for care. The most satisfactory bailout procedure is subtotal cholecystectomy of which there are two kinds. Subtotal fenestrating cholecystectomy removes the free wall of the gallbladder and ablates the mucosa but does not close the gallbladder remnant. Subtotal reconstituting cholecystectomy closes the gallbladder making a new smaller gallbladder. Such a gallbladder remnant is undesirable since it may become the site of new gallstone formation and recurrent symptoms . Both types may be done laparoscopically.”

Strasberg SM, Hertl M, Soper NJ. An analysis of the problem of biliary injury during laparoscopic cholecystectomy. J Am Coll Surg 1995;180:101-25.
Síndrome de Mirizzi

Abordagem Multimodal e Estratificação Tática no Manejo da Síndrome de Mirizzi
Autor: Prof. Dr. Ozimo Gama
Categoria: Cirurgia Hepatobilipancreática / Emergências Cirúrgicas / Anatomia Aplicada
Tempo de Leitura: 13 minutos
Introdução
A Síndrome de Mirizzi, descrita originalmente por Pablo Luis Mirizzi em 1948 como um “síndrome hepático funcional”, constitui uma das complicações mais complexas e desafiadoras da colelitíase crônica. Inicialmente atribuída a um espasmo fisiológico do ducto hepático, sua fisiopatologia é hoje claramente compreendida como uma obstrução mecânica extrínseca do ducto hepático comum ou do colédoco, secundária ao impacto crônico de cálculos no infundíbulo da vesícula biliar (difundido como bolsa de Hartmann) ou no ducto cístico. Trata-se de uma entidade nosológica incomum, acometendo entre 0,05% e 5,7% dos pacientes submetidos a procedimentos cirúrgicos biliares no Ocidente. O grande desafio reside na intensa reação inflamatória local que oblitera os planos de clivagem anatômicos, culminando, frequentemente, em erosão parietal e formação de fístula biliobiliárea (colecistobiliar). Além disso, a estase biliar crônica associa esta síndrome ao carcinoma de vesícula biliar em até 28% dos casos. O objetivo desta revisão é estabelecer um algoritmo operacional reprodutível para o manejo terapêutico da Síndrome de Mirizzi, correlacionando a estratificação anatômica de Csendes às abordagens cirúrgicas e endoscópicas contemporâneas.
Classificação de Csendes e Propedêutica Armada
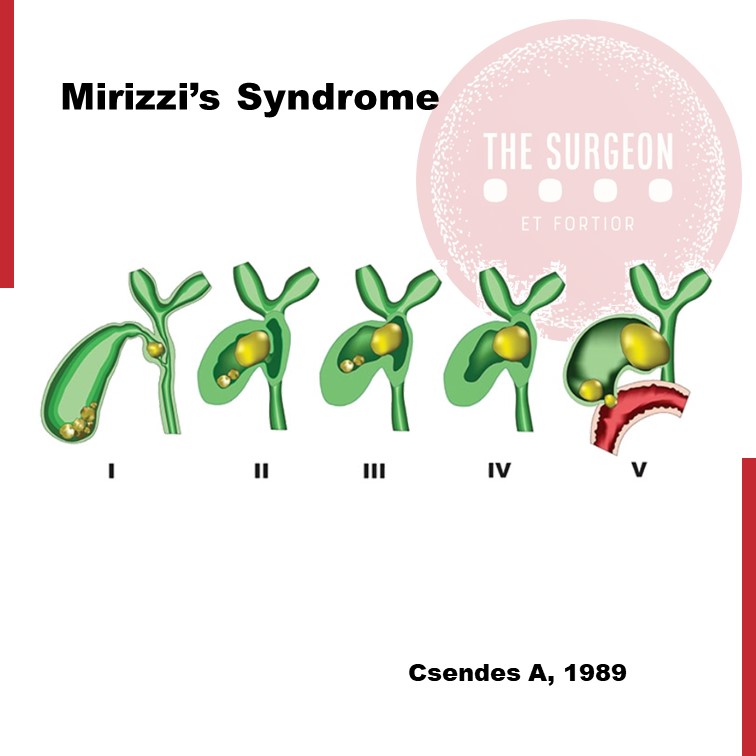
O manejo seguro e a prevenção de lesões iatrogênicas da via biliar principal exigem o estrito mapeamento da destruição tecidual. A classificação de Csendes organiza a apresentação da doença em cinco tipos anatômicos e dita a escalada terapêutica:
Classificação Temática de Csendes para Orientação Tática
| Tipo | Alteração Anatômica Estrutural | Abordagem Terapêutica de Escolha |
| Tipo I | Compressão extrínseca do ducto hepático comum por cálculo impactado, sem fístula. | Colecistectomia total (clássica) ou subtotal, via fundus-first. |
| Tipo II | Presença de fístula colecistobiliar envolvendo menos de 1/3 da circunferência da via biliar. | Colecistectomia subtotal + coledocoplastia com retalho da vesícula ou fechamento sobre tubo em T. |
| Tipo III | Fístula colecistobiliar que compromete entre 1/3 e 2/3 da circunferência do ducto. | Coledocoplastia com remanescente vesicular ou anastomose bilioentérica (Roux-en-Y). |
| Tipo IV | Destruição completa da parede da via biliar principal (> 2/3 da circunferência). | Reconstrução biliar definitiva por Hepático-jejunostomia em Y de Roux. |
| Tipo V | Qualquer tipo (I a IV) associado à presença de fístula colecistoentérica (ex: colecistoduodenal). | Correção da fístula entérica + tratamento do componente biliar correspondente. |
Diagnóstico Semiológico e a Tríade de Imagem
O quadro clínico sobrepõe-se ao de outras afecções hepatobiliares, caracterizado por icterícia obstrutiva, dor em hipocôndrio direito, náuseas e episódios de febre (sinalizando colangite). Laboratorialmente, observa-se padrão colestático proeminente, com elevação acentuada de bilirrubinas e fosfatase alcalina. Havendo suspeita clínica em pacientes idosos com níveis expressivos de CA 19-9, o diagnóstico diferencial com colangiocarcinoma ou neoplasia de vesícula deve ser prontamente conduzido.
A arquitetura radiológica diagnóstica assenta-se em uma tríade clássica observada em exames de imagem, como a Colangiorressonância (CPRM) — método não invasivo de maior acurácia:
- Dilatação do sistema biliar a montante (acima do nível do infundíbulo vesicular).
- Presença de cálculo calcificado e fixo impactado no colo gástrico ou ducto cístico.
- Estreitamento abrupto e retorno ao calibre normal da via biliar abaixo do nível do cálculo.
Estratégias de Exposição e Intervenção
1. O Papel da Endoscopia de Alta Resolução
A Colangiopancreatografia Retrógrada Endoscópica (CPRE) desempenha uma função dual. Inicialmente, funciona como ferramenta de descompressão biliar tática através do posicionamento de próteses (stents) biliares, minimizando a colangite e limpando o “terreno” para o ato cirúrgico. Em doentes de alto risco cirúrgico ou extrema fragilidade, a colangioscopia direta associada à litotripsia eletrohidráulica ou a laser atinge taxas de sucesso de 90% a 100% na fragmentação do cálculo, atuando como tratamento definitivo.
2. Tática Cirúrgica Operacional: A Linha de Defesa contra a Iatrogenia
A cirurgia para a Síndrome de Mirizzi exige o abandono da dissecção habitual do triângulo de Calot. A intensa fibrose impede a obtenção da Critical View of Safety (CVS) de Strasberg por via anterógrada, elevando o risco de trsecção inadvertida do colédoco.
- Manobra Dome-Down / Fundus-First: A dissecção da vesícula biliar deve ser realizada de forma retrógrada, do fundo em direção ao infundíbulo. Ao atingir a transição vesicular, o órgão deve ser aberto longitudinalmente para a evacuação de todos os cálculos.
- Manejo do Coto e Coledocoplastia: Nos casos de Tipo I, se o cístico estiver obliterado, a colecistectomia subtotal com fechamento do remanescente mucoso em bolsa é segura. Nos casos Tipo II, a parede residual da vesícula biliar não deve ser totalmente ressecada; ela é utilizada como um retalho biológico vascularizado para recobrir a fístula sobre um dreno de Kahr (tubo em T), reduzindo o risco de estenose biliar tardia. Nos tipos III e IV, a destruição biliar impede o reparo primário, impondo a realização de uma anastomose hepático-jejunal em Y de Roux ipsilateral, preferencialmente conduzida por cirurgião hepatobiliar experiente.
Pontos-Chave
- Estratificação por Csendes: O planejamento operatório é rigidamente atrelado ao grau de acometimento da parede do colédoco.
- Dissecção Retrógrada (Fundus-First): Abordagem obrigatória para evitar lesões catastróficas da via biliar principal diante da distorção anatômica local.
- Rastreador de Malignidade: Alta correlação com o adenocarcinoma de vesícula; biópsias de congelação perioperatórias devem ser consideradas em áreas suspeitas.
- Racionalização da Laparoscopia: Embora viável no Tipo I em mãos habilitadas, a cirurgia apresenta taxas de conversão elevadas (8% a 76%), não devendo o cirurgião postergar a conversão em caso de dúvida anatômica.
- Descompressão Precoce: A CRE pré-operatória com colocação de stent reduz a fricção cirúrgica ao delimitar a via biliar principal durante a dissecção.
Conclusões Aplicadas à Prática
A Síndrome de Mirizzi permanece como um dos cenários mais complexos da cirurgia do aparelho digestivo, testando os limites do julgamento clínico e da destreza técnica. Esta revisão demonstra que o sucesso terapêutico não decorre do imediatismo operatório, mas de uma abordagem diagnóstica precisa e integrada. O cirurgião moderno deve despir-se do dogma da colecistectomia laparoscópica total sistemática frente a uma anatomia congelada. A adoção da colecistectomia subtotal e o uso estratégico de retalhos vesiculares ou derivações biliodigestivas em Y de Roux constituem medidas de prudência científica que protegem o paciente contra disfunções hepáticas crônicas. Em suma, o manejo da Síndrome de Mirizzi corrobora que a segurança operatória fundamenta-se na simbiose entre o respeito à anatomia patológica e a flexibilidade tática da equipe cirúrgica.
“A anatomia biliar na Síndrome de Mirizzi é um labirinto onde a pressa e a autoconfiança excessiva operam como aliadas do desastre; a paciência tática e a dissecação retrógrada são as únicas vias seguras de retorno.” — Adaptado dos ensinamentos clássicos da Cirurgia Hepatobiliar.
Gostou ❔Nos deixe um comentário ✍️ , compartilhe em suas redes sociais e|ou mande sua dúvida pelo 💬 Chat On-line em nossa DM do Instagram.
Hashtags:
#SindromeDeMirizzi #CirurgiaHepatobiliar #ViaBiliar #CirurgiaDigestiva #SegurancaDoPaciente










