Surgical Management of GERD After Sleeve Gastrectomy
Evaluation of a patient referring GERD after sleeve gastrectomy should start with a detailed history and physical examination; the presence or absence of GERD-related symptoms should be thoroughly documented as well as any prior treatments or therapy used to treat it. Obtaining preoperative and operative records is of paramount importance particularly in those patients who had their index procedure performed elsewhere. Any endoscopic findings and prior imaging available are important to determine what the best course of action would be. If the patient had preoperative and postoperative imaging such as UGI, it is useful to compare those with a recent study to look for anatomical problems that may have been not addressed at the time of the index operation or developed over time. After this information is obtained, we can classify the GERD after sleeve as:
1. De novo GERD
2. Preexisting GERD without improvement
3. Preexisting GERD with worsening/complication
Regardless of how we classify the GERD, an initial evaluation with imaging
studies such as UGI and EGD is recommended. Comparison with any prior films if available is of significant value. Based on the UGI, we can determine if the shape of the sleeve falls into one of the following categories: tubular, dilated bottom, dilated upper, or dumbbell-shaped sleeve; we will also be able to evaluate esophageal peristalsis in real time and if there is associated hiatal hernias. We believe UGI under fluoroscopy provides important physiologic and anatomic information that can help guide our management approach, and therefore we offer it to all patients. We follow the radiologic evaluation with endoscopy, and during endoscopy, we look for objective signs of reflux such as esophagitis, presence of bile in the stomach or esophagus, as well as missed or recurrent hiatal hernias. In patients with evidence of esophagitis or metaplasia, multiple biopsies are taken. During the endoscopy, subtle findings that suggest a kink or a stricture may be present. In the absence of objective signs of gastroesophageal reflux disease on both endoscopy and upper GI series, we pursue physiologic testing followed by highresolution manometry and pH monitoring. In those patients where clear reflux esophagitis is seen, this additional testing may not be necessary or may be performed in selected cases depending on what the surgical or endoscopic therapy would be.

While it is true that most sleeve-related GERD will be effectively treated with a conversion to Roux-en-Y gastric bypass, not every patient with GERD after reflux will require a bypass or would agree to have one. First key step in addressing the patient is to evaluate whether the patient was selected appropriately to have a sleeve and second is to determine the exact sleeve anatomy; are there anatomical factors that will make it more likely for this patient to experience reflux; is there dilated fundus? Is there a kink or stricture in the sleeve or is it an anatomically appropriate operation? We should pay important attention to the weight loss the patient has experienced with the sleeve. Patients who do not have adequate weight loss and have GERD symptoms should not undergo other therapies and should probably undergo a bypass; however it is our unpublished experience that patients with the association of poor weight loss after sleeve and difficult to treat GERD will correct their GERD after conversion, but their weight loss results are still marginal even with a well-constructed bypass.
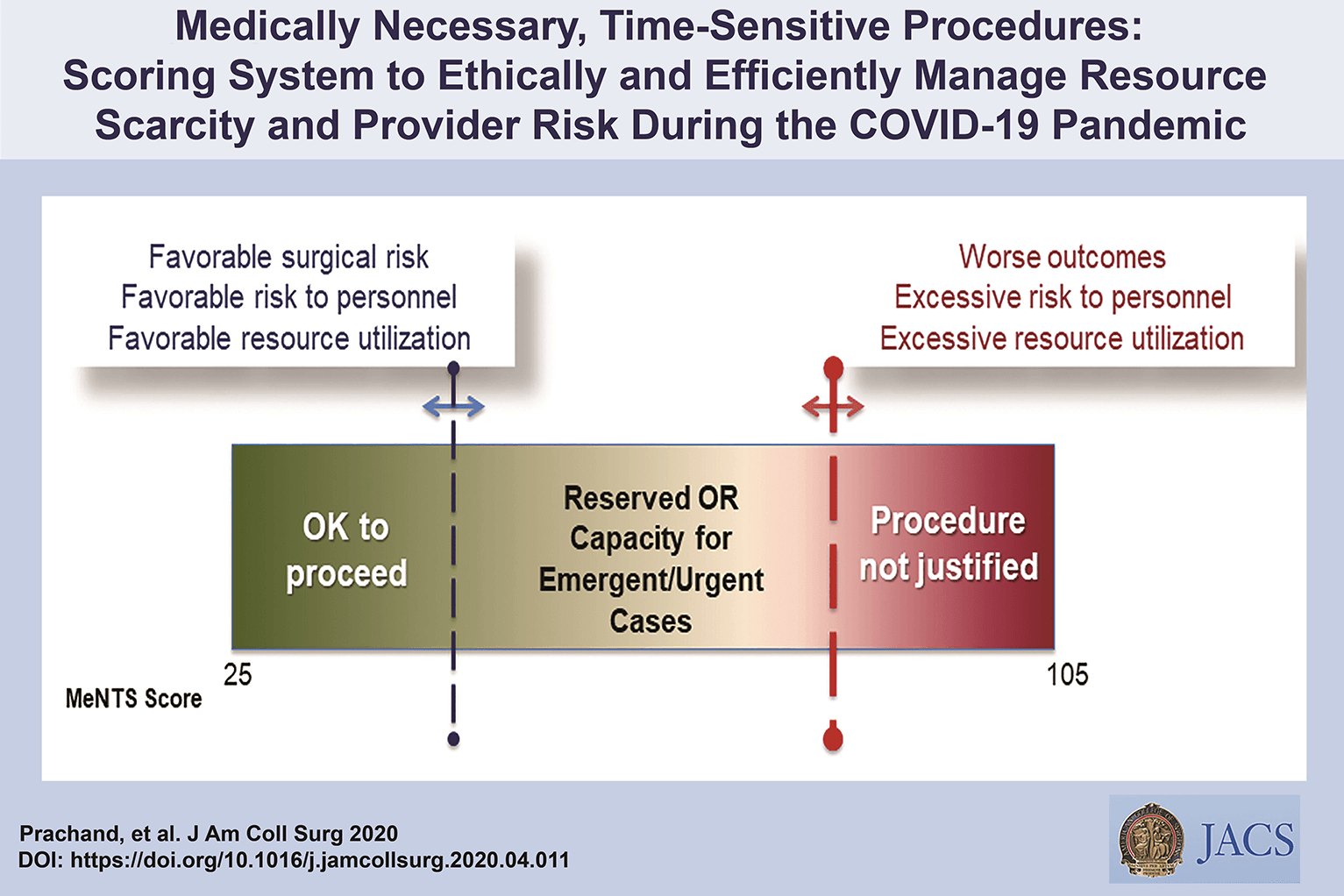
Medically-Necessary, Time Sensitive: (MeNTS) Score
Operating During The COVID-19 Coronavirus Pandemic
“At the University of Chicago, members of the Department of Surgery decided to investigate this issue more precisely. As stay-at-home restrictions in some states are easing, and as non-emergency medical care is being reconsidered, how does one possibly triage the thousands upon thousands of patients whose surgeries were postponed? Instead of the term “elective,” the University of Chicago’s Department of Surgery chose the phrase “Medically-Necessary, Time Sensitive” (MeNTS). This concept can be utilized to better assess the acuity and safety when determining which patients can get to the operating room in as high benefit/low risk manner as possible. And unlike in any recent time in history, risks to healthcare staff as well as risks to the patient from healthcare staff, are now thrown into the equation. The work was published in the April issue of the Journal of the American College of Surgeons.
On March 17, 2020, the American College of Surgeons recommended that all “elective” surgeries be canceled indefinitely. These guidelines were published, stating that only patients with “high acuity” surgical issues, which would include aggressive cancers and severely symptomatic disease, should proceed. Based on the Elective Surgery Acuity Scale (ESAS), most hospitals were strongly encouraged to cancel any surgery that was not high acuity, including slow-growing cancers, orthopedic and spine surgeries, airway surgeries, and any other surgeries for non-cancerous tumors. Heart surgeries for stable cardiac issues were also put on hold. Patients and surgeons waited. Some patients did, indeed undergo non-Covid-19-related surgeries. But most did not. Redeployment is gradually turning to re-entry.
The re-entry process for non-urgent (yet necessary) surgeries is a complicated one. Decisions and timing, based on a given hospital’s number and severity of Covid-19 patients, combined with a given city or state’s current and projected number of Covid-19 cases, how sick those patients will be, and whether or not a second surge may come, involves a fair amount of guesswork. As we have all seen, data manipulation has become a daily sparring match in many arenas. The authors of the study created an objective surgical risk scoring system, in order to help hospitals across this country, as well as others across the world, better identify appropriate timing regarding which surgeries can go ahead sooner rather than later, and why. They factored several variables into their equation, to account for the multiple potential barriers to care, including health and safety of hospital personnel. They created scoring systems based on three factors: Procedure, Disease and Patient Issues.
CALCULATE MeNTS SCORE HERE
The authors of the study created an objective surgical risk scoring system, in order to help hospitals across this country, as well as others across the world, better identify appropriate timing regarding which surgeries can go ahead sooner rather than later, and why. They factored several variables into their equation, to account for the multiple potential barriers to care, including health and safety of hospital personnel. Each patient would receive an overall conglomerate score, based on all of these factors, with the lower risks giving them more favorable scores to proceed with surgery soon, and the higher risks giving patients a higher score, or higher risk regarding proceeding with surgery, meaning it may be safest, for now, to wait.
Dr. Jeffrey Matthews, senior author of the paper, and Department Chair at the University of Chicago, stated that this model is reproducible across hospital systems, in urban, rural, and academic settings. And in the event of potential unpredictable surges of Covid-19 cases, the scoring system “helps prioritize cases not only from the procedure/disease standpoint but also from the pandemic standpoint with respect to available hospital resources such as PPE, blood, ICU beds, and [regular hospital] beds.”
The scoring system is extremely new, and the coming weeks will reveal how patients, surgeons and hospitals are faring as patients without life-and-death emergencies and/or Covid-19 complications gradually begin filling the operating rooms and hospital beds. In addition, and perhaps just as important, the study authors note that creating systems whereby healthcare resources, safety, and impact on outcomes need to be considered more carefully for each patient intervention, the larger impact of each intervention on public health will be better understood: not only for today’s pandemic, but also in future, as yet unknown, global events.”
Source: Nina Shapiro, 2020
Discover our surgical video channel and lectures associated with the surgeon blog.
Share and Join: https://linktr.ee/TheSurgeon
Covid-19 and Digestive Surgery
The current world Covid-19 pandemic has been the most discussed topic in the media and scientific journals. Fear, uncertainty, and lack of knowledge about the disease may be the significant factors that justify such reality. It has been known that the disease presents with a rapidly spreading, it is significantly more severe among the elderly, and it has a substantial global socioeconomic impact. Besides the challenges associated with the unknown, there are other factors, such as the deluge of information. In this regard, the high number of scientific publications, encompassing in vitro, case studies, observational and randomized clinical studies, and even systematic reviews add up to the uncertainty. Such a situation is even worse when considering that most healthcare professionals lack adequate knowledge to critically appraise the scientific method, something that has been previously addressed by some authors. Therefore, it is of utmost importance that expert societies supported by data provided by the World Health Organization and the National Health Department take the lead in spreading trustworthy and reliable information.










