Tumor Markers in HPB Cancers

The “ideal” tumor marker is economical, easy to estimate in easily accessible body fluids like blood or urine, has high sensitivity and specificity, can be used to screen for a cancer, has prognostic and predictive value at diagnosis, and is reliable during treatment and follow-up. It does not exist as of now. Commonly used tumor markers in gastrointestinal, liver, biliary tract, and pancreatic cancers are alpha fetoprotein (AFP), CA19.9, carcinoembryonic antigen (CEA), and chromogranin A (CgA).
Alpha Fetoprotein (AFP)
Alpha fetoprotein (AFP) is a glycoprotein that is produced in the yolk sac and the fetal liver. It is the most commonly used tumor marker for hepatocellular carcinoma (HCC). AFP may be raised in gonadal tumors, gastric cancer, and benign states like pregnancy, viral hepatitis, and cirrhosis caused by hepatitis C. The normal range is 10–20 ng/ml. Values above 400 ng/ml or a steady rise in serial estimation (even if lower than 400 ng/ml) is highly suggestive of HCC in a patient at risk of developing HCC. Persistent elevation of AFP is more significant than fluctuating levels. AFP levels are usually normal in the fibrolamellar variety of HCC. AFP is a heterogeneous molecule with respect to the carbohydrate moiety. Different AFP glycoforms can be separated and characterized by their affinity for lectins. Lectins are carbohydrate-binding proteins.

AFP level >500 ng/ml predicts high recurrence rate after transplantation, and such patients are not listed in the USA. Rise of AFP while on the wait list is also a poor prognostic factor. AFP >1000 ng/ml appears to be related to poor prognostic factors like microvascular invasion, portal vein invasion, bile duct invasion, and intrahepatic metastasis. In 2012 a French paper reported a model that added AFP to Milan criteria which improved prediction of recurrence and survival after liver transplantation for HCC.
CA 19-9
CA 19-9 is the abbreviation for carbohydrate antigen or cancer antigen 19-9. This tumor marker belongs to the family of mucinous markers. These have a transmembrane protein skeleton and an extracellular side that has glycosylated oligosaccharides. It is a sialylated Lewis blood group antigen. Mucus glands in the pancreas, biliary tree, salivary glands, stomach, colon, and endometrium physiologically secrete CA 19-9, and this is present in small quantities in serum. Higher levels are observed in inflammatory conditions of the pancreas and biliary tree like acute pancreatitis, biliary obstruction, and cholangitis. Overall mean sensitivity and specificity of serum CA 19-9 for diagnosis of pancreatic cancer are 81% and 90% according to one recent review. This study reported these results using 37 KU/l as cutoff of CA 19-9. Serum CA 19-9 seems to fare very poorly and is unsuitable as a screening modality for pancreatic cancer.
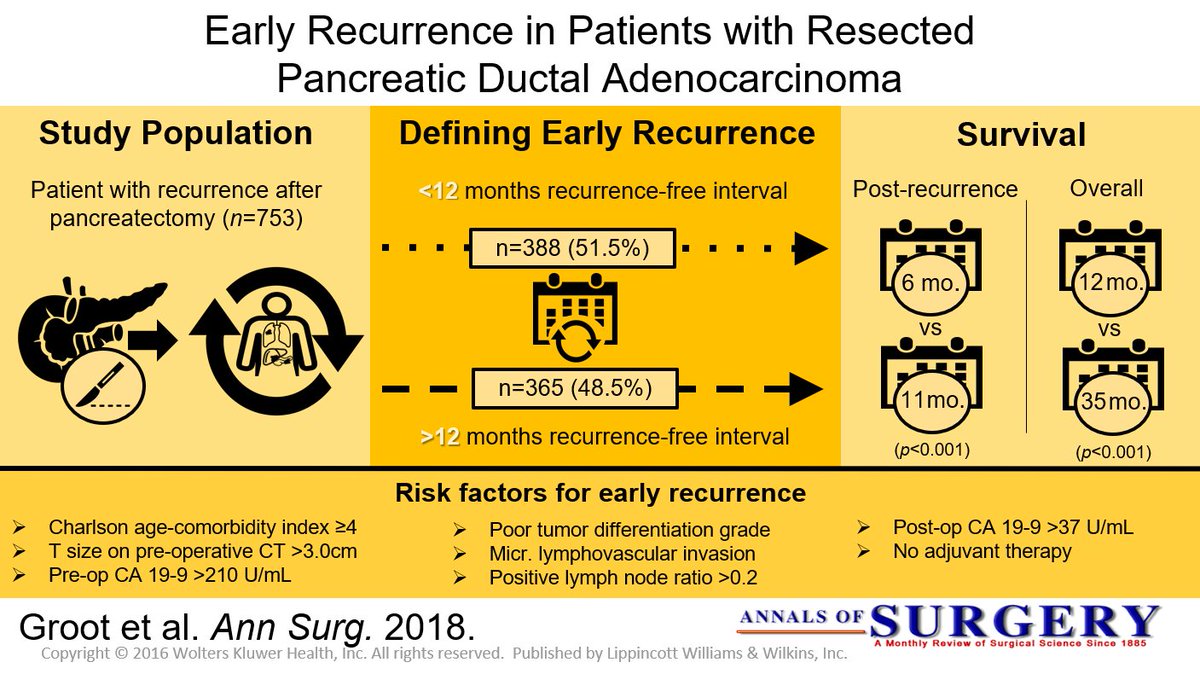
In one of the largest reviews of data, positive predictive value for diagnosis of pancreatic cancer was only 0.9%. Another study from Mumbai used CA 19-9 to predict operability in 49 patients with pancreatic cancer. When CA 19-9 was more than twice the normal (37 U/l), 88% were unresectable. Out of the 29 patients considered resectable after contrast-enhanced CT scan of abdomen, 5 patients were found unresectable at operation due to subcentimeter liver or peritoneal metastasis. All these five patients had CA 19-9 level more than three times the normal limit. These investigators suggest that diagnostic/ staging laparoscopy should be used to avoid a non-therapeutic laparotomy if CA 19-9 is more than thrice the normal limit.
Chromogranin A (CgA)
CgA is an acidic glycoprotein that is ubiquitously present in almost all endocrine and neuroendocrine cells of the human body. They are synthesized in these cells, stored along with other hormones /neurotransmitters in vesicles and released from the cells by exocytosis along with other hormones. The granin family consists of eight different substances of which chromogranin A is the best known and the one in clinical use for several decades now. CgA is thus a universal marker for neuroendocrine cell differentiation and activity. Testing its serum level is a marker of neuroendocrine secretory activity in the body. There are numerous limitations for the use of serum chromogranin A for diagnosis or follow-up of gastroenteropancreatic neuroendocrine tumors (GEP-NETs). However, it still remains the preferred tumor marker in these conditions, as it is widely available and less cumbersome to perform and retains a reasonable sensitivity and specificity provided the clinician applies all necessary recommended precautions in performance of the test and interpretation of the results.

Highest levels of CgA in GEP-NETs are obtained in midgut neuroendocrine tumors, previously termed as “carcinoid tumors.” In ileal carcinoids with liver metastasis, level as high as 200 times upper normal limit is reported. GEP-NETs in MEN-1 syndrome could result in chromogranin A values of about 150 times the upper normal limit. CgA levels in pancreatic NETs are about 60–80 times upper normal limit. CgA is elevated in 100% of gastrinomas and 70% of pancreatic NETs. In gastrinoma, very high levels are reported even in the absence of liver metastasis. CgA level of more than 5000 μg/l was found to be an independent prognostic factor for midgut NETs. Median survival was 33 and 57 months below and above the 5000 μg/l cutoff, respectively. This interpretation of CgA level cannot be generalized to all GEP-NETs. Typical exception of high level without any metastatic disease is gastrinoma as mentioned earlier. CgA level does not correlate with the degree of differentiation of GEP-NETs. Diagnostic accuracy of CgA was 73% in well-differentiated NETs and 50% in poorly differentiated NETs. This is probably related to loss of secretory function of poorly differentiated NETs, where this tumor marker is less reliable. CgA level has been reported to fall after all forms of therapy for GEP-NETs. This could be resection of the tumor, liver transplantation for metastatic disease, radionuclide therapy, or treatment with receptor blockade like everolimus.
Perioperative Fluid Management

In the setting of a normal ejection fraction, fluid is only administered when the expectation is that cardiac output will increase, and vasopressors are utilized if the aforementioned devices show fluid will not increase cardiac output. Excess fluid in certain general surgical cases can cause ileus and bowel edema, and in cardiac cases, it can cause hemodilution. Patients randomized to restricted and liberal fluid resuscitation strategies found a clear linear relationship between total fluids administered (and weight gain) and complications following colorectal surgery including pulmonary edema and tissue-healing complications. Further multiple studies exist demonstrating fewer complications with normovolemia than with liberal strategies of fluid resuscitation.
It must be understood that goal-directed therapy does, in no way, mean reduction in fluid administration. For some procedures, it may be necessary to administer more than anticipated fluid volumes (orthopedics), while for others, the opposite may be true (abdominal). Normovolemia is important to maintain perfusion without volume overload. Thus, the idea behind goaldirected therapy is to maintain zero fluid balance coupled with minimal weight gain or loss. Hypovolemia is associated with reduced circulating blood volume, decreased renal perfusion, altered coagulation, microcirculation compromise, and endothelial dysfunction, among other processes. Hypervolemia is associated with splanchnic edema, decreased pulmonary gas exchange secondary to pulmonary edema, impaired wound healing, anastomotic dehiscence, decreased mobility, altered coagulation, and endothelial dysfunction, amidst others processes.
Classroom: Perioperative Medicine
From a recent Cochrane review, there is no evidence that colloids are superior to crystalloid for resuscitation in patients. Therefore, crystalloid fluids should generally be the primary intravenous fluid during the perioperative course. In cardiac surgery, the utilization of 0.9% normal saline solution was associated with hyperchloremia and poor postoperative outcomes, including higher length of stay and increased mortality.118 Further, a more balanced crystalloid, such as Plasma-Lyte, was associated with improved outcomes in 22,851 surgical patients. In this study, there was a 2.05 odds ratio predictor of mortality with normal saline. Other complications such as acute kidney injury, gastrointestinal complications, major hemorrhage, and major infection were also increased in the group of
patients that were hyperchloremic after normal saline administration. Based on such evidence, it would seem prudent to proceed with a more balanced solution, such as PlasmaLyte, to reduce complications.
Internal Hernia after Laparoscopic Gastric Bypass
The purpose of this review is to evaluate the incidence and management of internal hernias (with or without SBO) after LGBP.
INTRODUCTION
Laparoscopic Roux-en-Y gastric bypass (LGBP) has been shown to be an effective treatment for morbid obesity, both in terms of weight loss and improvement in multiple comorbidities. While the laparoscopic approach offers many advantages to the patient in terms of fewer wound complications, decreased length of hospital stay, and decreased postoperative pain, certain complications of this operation continue to pose difficult clinical problems as the number of procedures performed increases. One such complication is internal hernia through one of the mesenteric defects, which can result in small bowel obstruction, ischemia, or infarction and often requires reoperation.
An internal hernia is defined as a protrusion of intestine through a defect within the peritoneal cavity, as opposed to an external (or incisional) hernia that protrudes through all layers of the abdominal wall. Internal hernias almost always occur through iatrogenic defects created surgically.

Incisional hernias occur at a higher incidence after open gastric bypass (GBP) at a rate of about 20 percent. LGBP has a lower rate of incisional hernias. A recent study by Rosenthal, et al., showed a 0.2-percent rate of port site hernias in 849 patients using blunt-tip trocars at 3,744 port sites. Internal hernias, on the other hand, occur more frequently in LGBP than in the open procedure. This is a significant clinical problem, since internal hernia is the most common cause of small bowel obstruction (SBO) after LGBP. Retrospective reviews have found the incidence of SBO after LGBP to be between 1.8 and 9.7 percent. The incidence of internal hernia after LGBP is between 0.2 and 8.6 percent based on multiple studies.
This incidence is higher than that seen with open GBP, and this is presumably due to decreased adhesion formation after laparoscopic surgery compared to open surgery. The creation of potential space as a result of weight loss may also be a contributing factor in the etiology of internal hernias, which often present in a delayed fashion. In addition, the particular case of pregnancy— with the mass effect of an enlarging uterus—may predispose to this condition, as there have been three case reports in the literature of internal hernia during pregnancy, one of which resulted in intestinal ischemia and fetal demise. Due to the increasing scope of this problem and its potentially devastating consequences, surgeons should have a high clinical suspicion for internal hernia after LGBP.
An internal hernia can potentially occur through either two or three defects, depending on whether a retrocolic or antecolic technique is used for the Roux limb. Petersen’s defect is defined as the space between the Roux limb and the transverse mesocolon. A defect is also present between the biliopancreatic and Roux limbs at the jejunojejunostomy. If a retrocolic approach is used, a third defect in the transverse mesocolon is created. This is the most common site of internal hernia in most reports, which has prompted many surgeons to adopt an antecolic technique in order to eliminate this defect. Higa’s study of 2,000 patients showed an internal hernia distribution of 67 percent mesocolic, 21 percent jejunal, and 7.5 percent Petersen. However, some centers experience a higher rate of hernia in the jejunal or Petersen’s defects, despite the use of a retrocolic approach.
PRESENTATION
Patients with internal hernia most commonly present with abdominal pain, and may also have symptoms of small bowel obstruction. The time of presentation varies greatly and may occur within one week of the initial operation or up to three years postoperatively. However, the majority of cases occur between 6 and 24 months postoperative. Radiographic diagnosis of internal hernia presents a challenge since the characteristic findings on computed tomography (CT) scan are often missed.
Features suggestive of an internal hernia include small bowel loops in the upper quadrants; evidence of small bowel mesentery crossing the transverse mesocolon; presence of the jejunojejunostomy superior to the transverse colon; signs of small bowel obstruction; or twisting, swirling, crowding, stretching, or engorgement of the main mesenteric trunk and according to one study, the sensitivity and specificity of CT is 63 percent and 76 percent, respectively.
Another study showed that although the diagnosis was only made prospectively by CT scan in 64 percent of cases, a retrospective review of the images showed that diagnostic abnormalities were present in 97 percent of cases. A report of five cases of internal hernia by Onopchenko found that only one was diagnosed preoperatively by radiological reading, even though all five had findings suggestive of internal hernia to the bariatric surgeon. These findings emphasize the need for communication with the radiologist, careful attention to patient history, and high clinical suspicion for internal hernias. In rare cases, closed loop obstruction and extensive bowel ischemia and infarction can occur. This dreaded complication underscores the necessity of making a rapid diagnosis. If the patient has significant symptoms but radiologic studies are negative, a diagnostic laparoscopy is warranted to rule out internal hernia.
PREVENTION AND TREATMENT
Given the prevalence of internal hernias and the increasing popularity of bariatric surgery, it is important to prevent or minimize this complication at the time of the initial operation. Although there have been no randomized, controlled trials comparing different techniques of LGBP, some authors have anecdotally reported lower rates of internal hernia after modifying their technique from a retrocolic to antecolic approach. Champion and Williams reported a significant decrease in small bowel obstruction after changing to an antecolic position, and Felsher and colleagues found no internal hernias in their study after adopting the antecolic approach.
However, other studies support careful defect closure as the most important factor in reducing hernia rates. Dresel and colleagues report no internal hernias after modifying their technique to include closure of Petersen’s defect. Carmody and colleagues report a decreased hernia incidence when closing all defects, even with a retrocolic approach. DeMaria’s study reports anecdotal improvement after closing mesenteric defects in two layers, on the medial and lateral aspects of the defect.
The majority of internal hernias can be successfully treated laparoscopically, with reduction and defect closure. The laparoscopic approach is usually successful; however, because of the lack of adhesion formation after laparoscopy, Capella, et al., suggest laparotomy for patients who experience a second episode of bowel obstruction due to recurrent internal hernia after laparoscopic repair. The greater adhesion formation after laparotomy may help prevent future internal hernia formation.
CONCLUSION
One of the benefits of laparoscopy, decreased adhesion formation, is likely also responsible for the increasing prevalence of internal hernia as a complication following laparoscopic gastric bypass. Although it has not been borne out in randomized clinical trials, anecdotal evidence and expert opinion suggest that Roux limb position and mesenteric defect closure at the time of initial operation are important factors in ultimate rates of hernia formation. Careful attention must be paid to individual surgical techniques in order to prevent this potentially devastating complication. The benefits of LGBP are maximized when there is a low incidence of postoperative hernias and resultant obstruction.
Surgical management of gastrointestinal bleeding
Severe gastrointestinal bleeding has historically been a clinical problem primarily under the purview of the general surgeon. Diagnostic advances made as the result of newer technologies, such as fiberoptic and video endoscopy, selective visceral arteriography, and nuclear scintigraphy, have permitted more accurate and targeted operations. More importantly, they have led to safe, effective nonoperative therapeutic interventions that have obviated the need for surgery in many patients. Today, most gastrointestinal bleeding episodes are initially managed by endoscopic or angiographic control measures. Such interventions are often definitive in obtaining hemostasis. Even temporary cessation or attenuation of massive bleeding in an unstable patient permits a safer, more controlled operative procedure by allowing an adequate period of preoperative resuscitation. Despite the less frequent need for surgical intervention, traditional operative approaches, such as suture ligation, lesion or organ excision, vagotomy, portasystemic anastomosis, and devascularization procedures, continue to be life-saving in many instances. The proliferation of laparoscopic surgery has fostered the application of minimally invasive techniques to highly selected patients with gastrointestinal bleeding. Intraoperative endoscopy has greatly facilitated the accuracy of laparoscopic surgery by endoscopic localization of bleeding lesions requiring excision. It is anticipated that the evolving technologies pertinent to the diagnosis and management of gastrointestinal bleeding will continue to promote collaboration and cooperation between gastroenterologists, radiologists, and surgeons.
Surgical Management
The role of surgery in acute peptic ulcer bleeding has markedly changed over the past two decades. The widespread use of endoscopic treatment has reduced the number of patients requiring surgery. Therefore, the need for routine early surgical consultation in all patients presenting with acute UGIB is now obviated (Gralnek et al., 2008). Emergency surgery should not be delayed, even if the patient is in haemodynamic shock, as this may lead to mortality (Schoenberg, 2001). Failure to stop bleeding with endoscopic haemostasis and/or interventional radiology is the most important and definite indication. The surgical procedures under these circumstances should be limited to achieve haemostasis. The widespread use of PPIs obviated further surgical procedures to reduce acid secretion. Rebleeding tends to necessitate emergency surgery in approximately 60% of cases with an increase in morbidity and mortality (Schoenberg et al.; 2001). The reported mortality rates after emergency surgery range from 2 – 36%. Whether to consider endoscopic retreatment or surgery for bleeding after initial endoscopic control is controversial (Cheung et al., 2009). A second attempt at endoscopic haemostasis is often effective (Cheung et al., 2009), with fewer complications avoiding some surgery without increasing mortality (Lau et al., 1999). Therefore, most patients with evidence of rebleeding can be offered a second attempt at endoscopic haemostasis. This is often effective, may result in fewer complications than surgery, and is the current recommended management approach. Available data suggest that early elective surgery for selected high-risk patients with bleeding peptic ulcer might decrease the overall mortality rate. It is a reasonable approach in ulcers measuring ≥2 cm or patients with hypotension at rebleeding that independently predicts endoscopic retreatment failure (Lau et al., 1999). Early elective surgery in patients presenting with arterial bleeding or a visible vessel of ≥2 mm is superior to endoscopic retreatment and has a relatively low overall mortality rate of 5% (Imhof et al., 1998 & 2003). Additional indications for early elective surgery include age >65 years, previous admission for ulcer plication, blood transfusion of more than 6 units in the first 24 hours and rebleeding within 48 hours (Bender et al., 1994; Mueller et al., 1994). This approach is associated with a low 30–day mortality rate as low as 7%.










