Complications of HEMORROIDH SURGERY

Symptomatic hemorrhoids require a number of therapeutic interventions each of which has its own complications. Office-based therapy such as rubber band ligation carries the risk of pain and bleeding, which are self-limited, but also carries the risk of rare complications such as sepsis, which may be life threatening. Operative treatment of hemorrhoids includes conventional hemorrhoidectomy, stapled hemorrhoidectomy, and the use of energy devices. Complications of pain and bleeding are common but self-limited. Late complications such as stenosis and fecal incontinence are rare. Recurrent disease is related to the initial grade and therapeutic approach. Treatment of recurrent hemorrhoids should be individualized based on previous treatments and the grade of disease. Anesthetic complications, especially urinary retention, are common and related to the anesthetic technique. Practitioners should council their patients as to the risks of the various approaches to treating symptomatic hemorrhoids.
Intra Abdominal Infections
With intra-abdominal infection being one of the most common reasons for surgical consultation, understanding the evaluation and management of these processes becomes paramount in the day- to-day practice of the surgeon. The very broad nature of who is affected coupled with the interplay of patient comorbidities and their medications make dealing with intra-abdominal infections a challenge. As with most complex problems in medicine, it is often useful to break them down into simpler and smaller parts. One useful way to categorize intra-abdominal infections is to divide them into those originating from previous abdominal trauma or operations and those presenting in a “virgin” abdomen.
The latter group most commonly includes those patients presenting with specific organ-based infectious processes such as appendicitis, cholecystitis, or diverticulitis. These individual diseases are covered extensively in other chapters and are discussed only superficially in this chapter. The former are those patients who have sustained intra-abdominal trauma or have undergone previous abdominal interventions and are not recovering in the usual expected course. It is this group that taxes diagnostic and clinical skills and may require the most complex medical decision making.
Several factors should come into play once suspicion for an intra-abdominal infection is entertained. These include resuscitation, antibiotic usage, and source control itself. Patients who present with either a suspected or diagnosed intra-abdominal infection should have some form of volume resuscitation. Even without hypotension, there are several reasons why these patients might be volume depleted. These include nausea and vomiting, fluid sequestration within the abdominal cavity or lumen of the bowel, and poor oral intake. As the process progresses, the patient may develop tachypnea, which results in an evaporative fluid loss. By this time, one can often elicit orthostatic hypotension in most patients.
Fluid resuscitation should begin with the administration of isotonic crystalloid and in general be guided by evidence of end organ perfusion (adequate mental status, urine output, correction of acidosis). There is no utility-using colloid such as albumin or hetastarch in these circumstances, and some data suggest a worse outcome. Should the patient present with hypotension or evidence of poor perfusion, a more aggressive approach to volume resuscitation should be employed. Our recommendation is to follow the current surviving sepsis guidelines, which include fluid challenges, monitoring/assessment of filling pressures, and the potential use of pressors and steroids.
KIDNEY INJURY on perioperative period

ACUTE KIDNEY FAILURE_REVIEW ARTICLE
Alterations in renal function are common after surgical emergencies, trauma, and major operations. In these settings, successful recovery of renal function is dependent on prompt diagnosis and protective management strategies. Acute kidney injury (AKI) is characterized by an acute decrease in glomerular filtration rate (GFR). The true incidence of AKI and acute renal failure (ARF) has been difficult to define, given the broad and various definitions used to quantify and study altered renal function. Relatively recent introduction of consensus definitions, such as RIFLE (risk, failure, loss, and end-stage renal failure) criteria and AKIN (Acute Kidney Injury Network) staging, have provided standard definitions to facilitate more uniform outcome reporting. With use of these definitions, recent studies suggest that AKI occurs in up to two thirds of patients in the intensive care unit (ICU). Moreover, increasing severity of AKI is associated with increasing mortality. AKI is also associated with increased morbidity, such as increased hospital length of stay and cost of care, and has been linked to other in-hospital complications, such as increased difficulty in weaning from mechanical ventilation. Preoperative risk factors for development of AKI include older age, emergent surgery, hepatic disease, obesity, high-risk surgery, vascular disease, and chronic obstructive pulmonary disease (COPD). Prompt recognition of AKI facilitates effective treatment. Although the incidence rate of AKI appears to be rising, overall outcomes from AKI are gradually improving.
The reported mortality rate of AKI is 30% to 60%. If RRT is necessary, reported mortality rates are over 50%. The reason for such high mortality is that AKI now usually occurs as part of a spectrum of multiple organ failure, most often associated with severe sepsis or septic shock. The mortality in this setting is often determined by the underlying septic syndrome, rather than by complications of individual organ failure. Of surviving patients of AKI, a significant number have development of chronic renal insufficiency, which necessitates chronic dialysis. The precise rate of development of chronic renal failure varies greatly in the literature, depending on the patient populations. A recent review of AKI estimates that overall, the risk of necessary chronic dialysis is approximately 12%.
Laparoscopic Surgery for Morbid Obesity
The morbid obesity epidemic continues to spread throughout industrialized nations. It is a condition with a heterogeneous etiology, including genetic, psychosocial, and environmental factors. Prevention methods have currently been unable to halt the further spread of this disease. Obesity has been linked to increased healthcare costs, common physiologic derangements, reduced quality of life, and increased overall mortality. More than one third of adults and almost 17% of children in the United States are obese.
Medical therapy that can cause sustained significant weight loss may be years away. Bariatric surgery, when combined with a multidisciplinary team, continues to be the only proven method to achieve sustained weight loss in most patients. Bariatric procedures modify gastrointestinal anatomy and, in some cases, enteric hormone release to reduce caloric intake, reduce absorption, and alter metabolism to achieve weight loss. Currently, the three most common bariatric operations in the United States are Roux-en-Y gastric bypass, adjustable gastric band, and the vertical sleeve gastrectomy.
GOSSIPIBOMA
O Inimigo Oculto no Bloco Operatório e o Desafio Médico-Legal na Cirurgia Digestiva
Autor: Prof. Dr. Ozimo Gama (Tempo de Leitura: 11 minutos)
Introdução
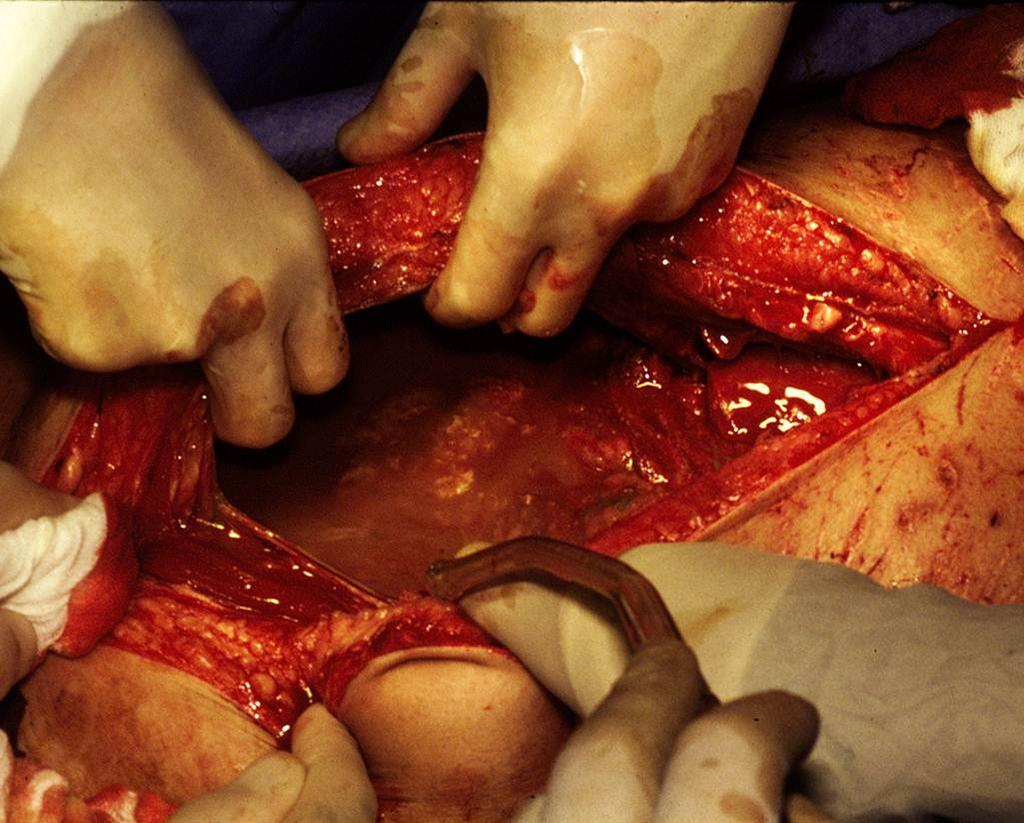
No vasto e complexo universo da cirurgia do aparelho digestivo, poucos eventos adversos geram tanta perplexidade clínica e devastação médico-legal quanto o “gossipiboma”. O termo deriva do latim Gossypium (algodão) e do swahili boma (esconderijo), designando uma matriz de matéria têxtil envolvida por uma reação de corpo estranho. Também apelidado de “textiloma”, o seu primeiro caso foi descrito por Wilson em 1884. Embora gazes e compressas sejam as ferramentas mais básicas de qualquer laparotomia, o seu esquecimento no interior da cavidade abdominal transforma um material de hemostase num tumor iatrogénico. A incidência real dos gossipibomas é subnotificada — primariamente devido ao estigma e às pesadas implicações legais da sua deteção —, mas representa uma falha catastrófica nos protocolos de segurança do bloco operatório. Para o cirurgião e para toda a equipa, compreender a fisiopatologia, os fatores de risco e, sobretudo, os métodos de prevenção desta entidade é um dever ético inegociável.
Epidemiologia e Fatores de Risco
Estima-se que a retenção de material têxtil ocorra numa frequência de 1 a cada 1.000 a 1.500 operações intra-abdominais. A cavidade abdominal e pélvica é, de longe, o “esconderijo” mais comum devido à sua vasta anatomia e aos recessos profundos.
O gossipiboma não é um mero fruto do acaso; ele prospera no caos. A literatura científica identifica fatores predisponentes cruciais:
- Cirurgia de Emergência: A incidência é nove vezes maior nestes cenários.
- Mudança de Tática Intraoperatória: Alterações não planeadas no decorrer da intervenção elevam o risco em quatro vezes.
- Fatores do Doente e do Ambiente: Doentes com obesidade mórbida, perdas hemáticas maciças que exigem tamponamento rápido, tempo operatório prolongado e, criticamente, a troca de turnos do pessoal médico e de enfermagem (instrumentistas e circulantes) durante o ato cirúrgico.
Fisiopatologia e Evolução Clínica
O relógio biológico do gossipiboma é imprevisível. O tempo entre a operação primária e as manifestações clínicas pode variar de meros 10 dias a várias décadas. A patologia manifesta-se essencialmente através de duas reações orgânicas distintas:
- Resposta Assética Fibrinosa (Crónica): O material têxtil, se permanecer estéril, induz a produção de fibrina, originando aderências e o encapsulamento do corpo estranho (granuloma). O doente pode permanecer completamente assintomático durante anos, ou apresentar queixas inespecíficas e uma massa abdominal palpável que mimetiza uma neoplasia.
- Resposta Exsudativa (Aguda): Ocorre uma infeção secundária severa, culminando na formação de abcessos e fístulas. O material retido tenta encontrar uma via de exteriorização, podendo fistulizar para órgãos internos (estômago, intestino, cólon, bexiga) ou formar uma fístula externa na parede abdominal. Nestes casos, o doente apresenta um quadro florido: dor abdominal, náuseas, vómitos, febre, sépsis, hemorragia digestiva crómica ou síndrome de má absorção.
Diagnóstico, Tratamento e Prognóstico
A ausência de sintomas precoces ou a sua inespecificidade tornam o diagnóstico um autêntico desafio. O cirurgião deve manter um elevado índice de suspeição perante qualquer massa abdominal num doente com história de laparotomia prévia.
- O Padrão-Ouro Diagnóstico: A Tomografia Computorizada (TC) de abdómen é o exame de eleição. A imagem clássica revela uma lesão cística de aspeto “espongiforme” (padrão em miolo de pão), uma cápsula hiperdensa em camadas concêntricas e, ocasionalmente, calcificações murais. A presença de gás no interior da lesão sem evidência de perfuração intestinal é altamente sugestiva.
- Tratamento: A remoção cirúrgica (seja por via laparoscópica em casos altamente selecionados ou laparotomia) é o único tratamento curativo.
- Prognóstico: A excisão atempada é vital para evitar complicações que elevam a taxa de mortalidade para valores inaceitáveis de 11% a 35%. Se a retenção for crónica, a severidade das aderências pode exigir ressecções intestinais extensas e complexas.
Implicações Médico-Legais e Procedimentos Preventivos
O gossipiboma é indiscutivelmente uma falha grave na prestação de cuidados de saúde (malpractice). Do ponto de vista médico-legal, a responsabilidade é frequentemente partilhada entre o cirurgião principal — o “capitão do navio” — e a equipa de enfermagem responsável pela contagem.
A abordagem definitiva é, e sempre será, a Prevenção. A adoção de protocolos rígidos no bloco operatório salva vidas e carreiras:
- Contagem Meticulosa Universal: São mandatárias quatro contagens rigorosas do material cirúrgico: na montagem da mesa, imediatamente antes da incisão, no início do encerramento da aponevrose e durante a síntese da pele.
- Material Radiopaco: O uso exclusivo de compressas e gazes equipadas com filamentos radiopacos é obrigatório.
- Exploração Ativa: Autores como Dhillon e Park reforçam a necessidade primária da exploração manual e visual dos quatro quadrantes abdominais pelo cirurgião no final do procedimento, independentemente de uma contagem de compressas declarada “correta”.
- Conduta Perante Falha na Contagem: Se a contagem final for divergente, a síntese da cavidade não deve ser concluída até que o material seja localizado (a menos que haja instabilidade hemodinâmica crítica). A realização de uma radiografia intraoperatória imediata é mandatária.
Conclusões Aplicadas
O gossipiboma não é uma complicação inerente e aceitável do ato cirúrgico; é uma falha de sistema e de liderança. O aumento aparente da sua incidência exige que os métodos, a comunicação e a disciplina no interior do bloco operatório sejam revistos e aperfeiçoados. Para os jovens cirurgiões e residentes, a mensagem é clara: a cirurgia de excelência não termina na anastomose perfeita, mas sim na verificação obsessiva e no respeito incondicional pelos protocolos de segurança. A verdadeira destreza cirúrgica repousa na humildade de nunca presumir que a cavidade está vazia sem antes a inspecionar exaustivamente.
“A confiança é um sentimento nobre, mas no bloco operatório, a dupla verificação é a única garantia de segurança. Um erro de omissão pode ensombrar o mais brilhante dos procedimentos cirúrgicos.” — Aforismo da Segurança do Doente Cirúrgico.
Gostou ❔Deixe-nos um comentário ✍️ , partilhe nas suas redes sociais e|ou envie a sua dúvida pelo 💬 Chat On-line na nossa DM do Instagram.
Abdominal Hernia Surgical EMERGENCIES

A hernia is a weakness or disruption of the fibromuscular tissues through which an internal organ (or part of the organ) protrudes or slides through. Collectively, inguinal and femoral hernias are often lumped together into groin hernias. Surgery remains the only effective treatment, but the optimal timing and method of repair remain controversial. Although strangulation rates of 3% at 3 months have been reported by some investigators, the largest prospective randomized trial of (watchful waiting) men with minimally symptomatic inguinal hernias showed that watchful waiting is safe. Frequency of strangulation was only 2.4% in patients followed up for as long as 11.5 years. Long-term follow-up shows that more than two-thirds of men using a strategy of watchful waiting cross over to surgical repair, with pain being the most common reasons. This risk of crossover is higher in patients older than 65 years. Once an inguinal hernia becomes symptomatic, surgical repair is clearly indicated. Femoral hernias are more likely to present with strangulation and require emergency surgery and are thus repaired even when asymptomatic. Because this article focuses on incarcerated hernias, nonoperative options are not discussed.










