“Not Only SURGEONS…”
SURGERY, A NOBLE PROFESSION
Surgery is, indeed, one of the noblest of professions. Here is how Dictionary defines the word noble: 1) possessing outstanding qualities such as eminence, dignity; 2) having power of transmitting by inheritance; 3) indicating superiority or commanding excellence of mind, character, or high ideals or morals. These three attributes befit the profession of surgery. Over centuries, the surgical profession has set the standards of ethical and humane practice. Surgeons have made magnificent contributions in education, clinical care, and science. Their landmark accomplishments in surgical science and innovations in operative technique have revolutionized surgical care, saved countless lives, and significantly improved longevity and the quality of human life. Generations of surgeons have developed their craft and passed it on to succeeding generations, as they have to me and to each one of you, to take into the future.
Beyond its scientific and technical contributions, surgery is uniquely fulfilling as a profession. It has disciplined itself over the centuries and dedicated its practice to the best welfare of all human beings. In return, it has been accorded the respect of society, of other professions, and of policy makers. Its conservative stance has served it well and has been the reason for its constancy and consistency. At the beginning of the 21st century, however, profound changes are taking place at all levels and at a dizzying pace, providing both challenges and opportunities to the surgical profession. These changes are occurring on a global level, on the national level, in science and technology, in healthcare, and in surgical education and practice.
To retain its leadership position in innovation and its attractiveness as a career choice for students, surgery must evolve with the times. It is my belief that surgery needs to introduce changes to create new priorities in clinical practice, education, and research; to increase the morale and prestige of surgeons; and to preserve general surgery as a profession. I am reminded of a Chinese aphorism that says, “You cannot prevent the birds of unhappiness from flying over your head, but you can prevent them from building a nest in your hair.”
ADVANCES IN SCIENCE
The coalescence of major advances in science and technology made the end of the 20th century unique in human history. Notable among the achievements are the development of microchips and miniaturization, which fueled the explosion in information technology. The structure of the human genome is nearly completely elucidated, ushering in the genomic era in which genetic information will be used to predict, on an individual basis, susceptibility to disease and responsiveness to drug therapy. The field of nanotechnology allows scientists to work at a resolution of less than one nanometer, the size of the atom. By comparison, the DNA molecule is 2.5 nanometers.
In the last 50 years, biomedical research became increasingly reductionist, turning physiologists and anatomists into molecular biologists. As a result, two basic science fields—integrative physiology and gross anatomy—now have a lower standing in medical education and surgical science than they once did. Surgery and surgical departments can and possibly should claim these fields, but the window of opportunity is narrow. Research is now moving back from discipline-based reductionist science to multidisciplinary science of complexity, in which biomedical scientists work side by side with engineers, mathematicians, and bioinformatists. The ability of high-speed computers to quickly process tens of millions of pieces of data now allows for data-driven rather than hypothesis-based research. This collaboration among different disciplines has already been successful.
TRANSFORMATION OF HEALTHCARE SYSTEM
During the past 75 years, we have seen the entire healthcare system undergo a profound transformation. In the 1930s and for a considerable period thereafter, medical practice was fee-for-service, the doctor–patient relationship was strong, and the physician perceived himself or herself as being responsible nearly exclusively to his or her individual patients. The texture of medical practice started to change when the federal government became involved in the provision of healthcare in 1965. The committee on “Crossing the Quality Chasm” identified six key attributes of the 21st-century healthcare system. It must be:
- Safe, avoiding injuries to patients;
- Effective, providing services based on scientific knowledge;
- Patient-oriented, respectful of and responsive to individual patients’ needs, values, and preferences;
- Timely, reducing waits, eliminating harmful delays for both care receiver and caregiver;
- Efficient, avoiding wasted equipment, supplies, ideas, and energy;
- Equitable, providing equal care across genders, ethnicities, geographic locations, and socioeconomic strata;
No one knows at present what this 21st-century healthcare system will look like. While care in the old system was reactive, in the new system it will be proactive. The “find it, fix it” approach of the old system will be replaced by a “predict it, prevent it, and if you cannot prevent it, fix it” approach. Sporadic intervention, provided only when patients present with illness, will give way to a system in which physicians and other healthcare providers plan 1-, 5-, and 10-year care programs for each patient. Care will be more interactive, with patients taking a more important role in their own care. The technology-oriented system will become a system that provides graded intervention. Delivery systems will not be fractionated but integrated. Even more importantly, care will not be based simply on experience and clinical impression but on evidence of proven outcome measures. If the old system was cost-insensitive, the new system will be cost-sensitive.
SURGICAL PRACTICE
There are many reasons for the declining interest in general surgery, some of which parallel reasons for the drop in medical school applicants in general. One problem specific to surgery is that medical students are given less and less exposure to surgery, due to the shortening of required surgical rotations. Most important, however, is their perception that the life of the surgical resident is stressful, the work hours too long, and the time for personal and family needs inadequate. The workload of the surgical resident over the years has increased significantly both in amount and intensity, without concomitant increase in the number of residents and at a time when hospitals have significantly reduced the support personnel on the surgical ward and in the operating rooms. Students graduating with debts close to $100,000 simply find the years of training in surgery too long, followed by uncertain practice income after graduation.
From several recent studies, lifestyle is the critical and most pressing issue in surgical residency. Some studies have also shown that the best students tend to select specialties that provide controllable lifestyles, such as radiology, dermatology, and ophthalmology. We have a problem not only in the declining number of students applying for surgical training but also in the declining quality of those who do apply. In a preliminary survey of 153 responding general surgery programs, we found that attrition (i.e., categorical residents leaving the training programs) occurred at a rate of 13% to 19% in the last 5 years. In 2001, 46% of those leaving general surgery training programs cited lifestyle as the major reason.
Unless these trends are reversed, general surgery as a specialty is threatened, and a future shortage of general surgeons is inevitable. I know that the Council of the American Surgical Association is most concerned about the crisis in general surgery. We must do a better job of communicating to students and residents that the practice of surgery is as rewarding as ever and full of opportunities in this new era. Innovations in minimal access and computer-assisted surgery and simulation technology provide exciting new possibilities in surgical training. We must also look very carefully at the demands of surgical residency and improve the life of residents without compromising their surgical experience. Unless we deal with work hours and quality of life issues, we are likely to see continuing decline in the interest of medical students in surgical training.
CONCLUSIONS
In conclusion, the noble profession of surgery must rise to meet numerous challenges as the world in which it operates continues to undergo profound change. These challenges represent opportunities for the profession to develop an international perspective and a global outreach and to address the growing needs of an aging population undergoing major demographic and workforce shifts. The leadership of American surgery has a unique role to play in the formulation of a new healthcare system for the 21st century. This task will require commitment to quality of care and patient safety, and it will depend on harnessing the trust and support of the American public. Advances in science and technology—particularly in minimal access surgery, robotics, and simulation technology—provide unprecedented opportunity for surgeons to continue to make landmark contributions that will improve surgical care and the human condition. I believe it is also crucially important that we train surgeon-scientists who will keep surgery at the cutting edge in the genomic and bioinformatics era. Ours is a noble profession imbued with eminence, dignity, high ideals, and ethical values. It has a rich and proud heritage… and I quote, “The highest intellects, like the tops of mountains, are the first to catch and reflect the dawn.”
Source: Lecture from Haile T. Debas, MD (UCSF School of Medicine, San Francisco, California) Presented at the 122nd Annual Meeting of the American Surgical Association, April 25, 2002, The Homestead, Hot Springs, Virginia.
Vascularização da Árvore Biliar
O Fio da Navalha na Prevenção da Isquemia e Estenose
Autor: Prof. Dr. Ozimo Gama (Tempo de Leitura: 11 minutos)
Introdução
No campo minado que é a cirurgia hepatobiliar, existe um princípio fisiológico que não admite margem para erro: enquanto o parênquima hepático é um órgão privilegiado, nutrido por um duplo suprimento sanguíneo (arterial e venoso portal), a árvore biliar é alimentada exclusivamente pelo sistema arterial. Para o estudante de medicina e o residente de cirurgia, a compreensão desta premissa muda drasticamente a forma como o bisturi e o cautério são manuseados em torno do hilo hepático. A esqueletização excessiva de um ducto biliar não é um sinal de dissecção meticulosa, mas sim a antessala anatómica de uma complicação catastrófica: a isquemia, seguida de necrose e estenose biliar. Neste artigo, dissecaremos a anatomia vascular da árvore biliar, as armadilhas do ducto cístico e os fundamentos anatómicos da cirurgia oncológica da vesícula.
1. A Vesícula Biliar: Topografia e Peculiaridades Histológicas
A vesícula biliar repousa no equador que divide o fígado direito do esquerdo — uma linha imaginária conhecida como Linha de Cantlie (ou linha de Rex-Cantlie), que cursa entre os segmentos IVb e V em direção à veia cava inferior posteriormente.
A vesícula é maioritariamente peritonizada, exceto na sua face posterior, que assenta diretamente na placa cística. No entanto, o seu verdadeiro “Calcanhar de Aquiles” reside na sua histologia: a vesícula biliar não possui muscularis mucosae, não possui submucosa e apresenta uma camada muscular descontínua.
- Implicação Cirúrgica Oncológica: Estas especificidades anatómicas removem as barreiras naturais contra a progressão tumoral, facilitando a invasão direta do cancro da vesícula biliar para o parênquima hepático. É por este motivo que o tratamento cirúrgico curativo exige uma Colecistectomia Radical (que inclui a ressecção em cunha dos segmentos hepáticos IVb e V) sempre que o estadiamento tumoral (T) for superior ou igual a T1b.

2. O Labirinto Anatómico do Ducto Cístico e da Via Biliar Principal
A partir do infundíbulo cónico da vesícula, o ducto cístico estende-se como o limite inferior do triângulo hepatocístico em direção ao hilo, unindo-se ao ducto hepático comum (DHC) para formar o ducto colédoco (VBP). Contudo, na via biliar, a variação anatómica é a regra, não a exceção. O ducto cístico pode correr paralelamente ao DHC, espiralar posteriormente a este e inserir-se na sua face medial. Mais perigoso ainda é quando o cístico se insere no Ducto Setorial Posterior Direito (RPD), uma variação que ocorre em cerca de 4% dos fígados. Esta configuração é notoriamente perigosa, expondo o RPD a um risco altíssimo de secção inadvertida durante uma colecistectomia de rotina. Distalmente, o colédoco entra na cabeça do pâncreas e une-se ao ducto pancreático (Wirsung) para formar a ampola hepatopancreática, controlada pelo Esfíncter de Oddi.
- O Canal Comum Longo: Quando a junção entre o colédoco e o ducto pancreático ocorre de forma anómala (antes do complexo esfincteriano), ocorre o refluxo de enzimas pancreáticas ativadas para a árvore biliar. Este trauma químico crónico é o principal fator de risco para a formação de cistoss do colédoco e para o desenvolvimento de Colangiocarcinoma.
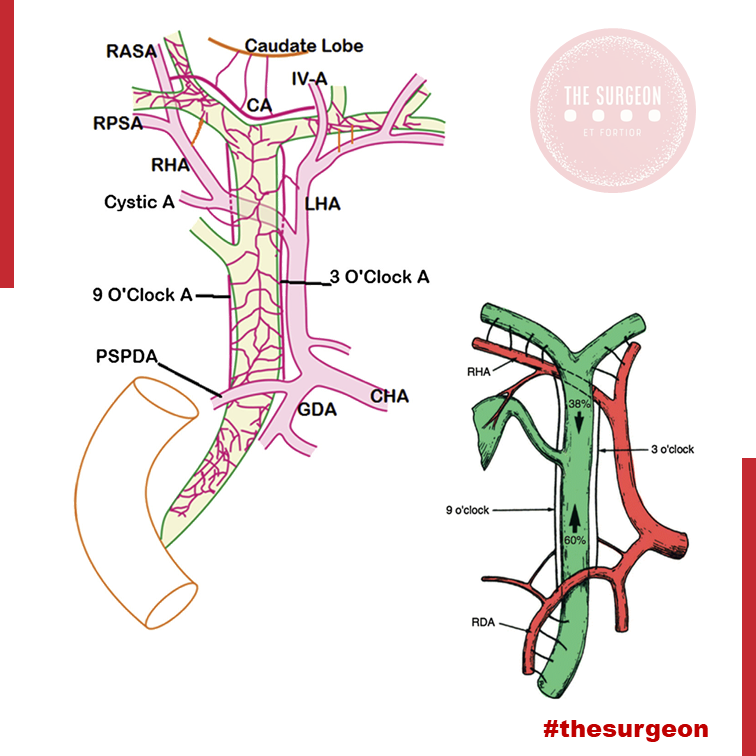
3. O “Tendão de Aquiles”: A Vascularização Arterial da Via Biliar
Como mencionado, a árvore biliar depende de um fluxo arterial ininterrupto. O suprimento segue um padrão de perfusão que ascende e descende ao longo dos ductos:
- O Suprimento Distal (Ascendente): O ducto colédoco recebe a sua irrigação inferior a partir de arteríolas emparelhadas provenientes da Artéria Gastroduodenal (GDA) e da Artéria Pancreatoduodenal Superior Posterior (PSPDA). Esta última representa o suprimento arterial mais importante e constante para o colédoco distal.
- O Suprimento Proximal (Descendente): Proximamente, o colédoco é alimentado por arteríolas originadas da artéria hepática direita (AHD).
- As Artérias Marginais: Estes vasos superiores e inferiores anastomosam-se para formar as artérias marginais, que correm paralelamente ao longo do ducto colédoco, situando-se tipicamente nas posições das 3 e 9 horas (lateral e medialmente). Desnudar (esqueletizar) o colédoco deste suprimento arterial para criar uma anastomose ou durante uma linfadenectomia não regrada acarreta um risco altíssimo de isquemia e estenose cicatricial a longo prazo.
4. O Plexo Epicoledociano Hilar e as Variações Arteriais
No interior do hilo hepático, uma rica rede de capilares liga as artérias hepáticas direita e esquerda. Este leito vascular, denominado Plexo Epicoledociano Hilar, fornece uma circulação colateral crítica que pode manter o suprimento arterial para um lado do fígado caso o vaso ipsilateral seja lesado. A preservação deste plexo e do suprimento sanguíneo arterial para o fígado remanescente é absolutamente crucial na criação de uma anastomose biliodigestiva (hepaticojejunostomia). A isquemia hilar resulta na temível colangiopatia isquémica e no desenvolvimento de abcessos hepáticos intratáveis.
O Papel das Variações Arteriais no Colangiocarcinoma Hilar
Na cirurgia do colangiocarcinoma hilar (Tumor de Klatskin), a complexidade aumenta devido às variações arteriais. A artéria hepática direita cruza posteriormente ao ducto hepático na maioria dos casos, mas em 25% cruza anteriormente. Mais relevante ainda é a presença de uma Artéria Hepática Direita Substituída (ou Acessória), com origem na Artéria Mesentérica Superior (AMS). Ao contrário da anatomia clássica, este vaso cursa lateralmente ao ducto colédoco (e não medialmente), estando extremamente vulnerável à iatrogenia se o cirurgião não o identificar durante a dissecção do ligamento hepatoduodenal. Combinações destas variações com a localização exata do tumor ditarão se uma lesão hilar é ressecável ou irresecável.
Pontos-Chave para a Prática Diária
- A Regra das 3 e 9 Horas: Lembre-se sempre de que o suprimento axial do colédoco viaja nos seus flancos laterais. Evite dissecções circunferenciais extensas da via biliar principal.
- Histologia e Neoplasias: A ausência de submucosa na vesícula biliar dita a necessidade de cirurgia hepática radical (ressecção em cunha do leito) em tumores T1b ou superiores.
- Inserções Anómalas do Cístico: A inserção num ducto setorial direito (RPD) é uma armadilha clássica. A Visão Crítica de Segurança (CVS) e a colangiografia são as únicas formas de evitar a transecção de um ducto principal aberrante.
- O Perigo do Canal Comum: A junção biliopancreática anómala exige vigilância ou tratamento cirúrgico devido ao elevado risco de colangiocarcinoma derivado da inflamação enzimática crónica.
Conclusões Aplicadas à Prática do Cirurgião Digestivo
O respeito pela árvore biliar transcende a mera identificação do tubo que transporta a bílis; exige uma veneração profunda pela sua microvascularização. O cirurgião que descasca a via biliar como se tratasse de um cabo elétrico condena o seu doente a um futuro de estenoses isquémicas, colangites de repetição e reintervenções de extrema complexidade. O domínio da variabilidade anatómica vascular (como as artérias substituídas da AMS) e o conhecimento tático do plexo epicoledociano não são meros detalhes de rodapé dos livros de anatomia; são a linha que separa o triunfo cirúrgico oncológico da catástrofe iatrogénica irreparável.
“A anatomia biliar não segue regras absolutas, apenas tendências. Operar no hilo hepático assumindo a normalidade é o primeiro passo para o desastre. O cirurgião deve dissecar com a expectativa constante da variação.” — Aforismo clássico da cirurgia hepatobiliar.
Gostou ❔Deixe-nos um comentário ✍️, partilhe nas suas redes sociais e|ou envie a sua dúvida pelo 💬 Chat On-line na nossa DM do Instagram.