PÓLIPOS COLORRETAIS
Os pólipos colorretais são estruturas que se projetam na superfície da camada mucosa do intestino grosso, podendo ser neoplásicos ou não. Foi Morson, em 1976, quem melhor estabeleceu uma classificação para os diversos tipos de pólipos e a importância da progressão adenoma-câncer. Os pólipos foram divididos em: pólipos neoplásicos, caracterizados pelos adenomas e os carcinomas, e os pólipos não-neoplásicos, que incluem os tipos epiteliais hamartomatosos, inflamatórios, hiperplásicos ou metaplásicos. Os pólipos adenomatosos, que correspondem a cerca de 70% de todos os pólipos, são conhecidamente lesões pré-malignas que antecedem, em 10 a 15 anos, o câncer colorretal. Por conta dessa progressão lenta, a detecção de lesões pré-neoplásicas no intestino grosso é relevante na prevenção do surgimento e complicações do câncer colorretal. Os pólipos podem ser ressecados (polipectomia) antes da sua malignização, diminuindo sobremaneira a taxa de morbimortalidade do câncer colorretal.

A colonoscopia é o padrão-ouro para o diagnóstico do câncer colorretal e para a detecção e ressecção endoscópica das lesões precursoras. A realização de polipectomias e biópsias permite, através da histopatologia, avaliar o tipo histológico, o grau de displasia e as margens de ressecção a fim de quantificar seu potencial de malignização. O câncer colorretal é a quinta neoplasia maligna mais frequente no Brasil, e se estima que 26.990 novos casos tenham sido diagnosticados no ano de 2008, o que evidencia sua alta frequência. Estes valores correspondem a um risco estimado de 13 casos novos a cada 100 mil homens e 15 para cada 100 mil mulheres. Associado a isso, a grande maioria dos tumores malignos se origina dos adenomas, e a detecção e retirada precoces evitam a progressão para o câncer.
Risk for POSTOPERATIVE INFECTION
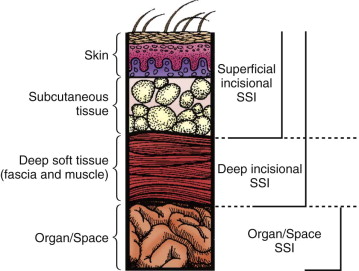
Surgical site infections (SSIs) are a common surgical complication that affects between 2% and 5% of the 30 to 40 million operations that occur in the United States per year. SSIs are the most common nosocomial infection among surgical patients and are consistently the second most common healthcare-associated infection overall. Mortality rates after SSI are markedly higher when compared with patients without an SSI, as are the patient’s length of stay (mean, 7 days), hospital readmission rates, and direct patient costs ($500 to $3000 per infection).
Risk Factors
Development of an SSI requires microorganism contamination at the surgical site. During an operative procedure in which skin is incised, endogenous skin flora, the most common source of pathogens, are introduced into the exposed tissue. Additional sources of bacteria include patient colonization, mucous membrane or hollow viscous pathogens encountered during the operation, surgical personnel, operative instruments, and the operating room environment. An accepted surrogate for bacterial contamination at the surgical site is the wound classification. The risk of SSI increases with the degree of contamination and higher wound classifications. Wounds are classically defined as clean, clean-contaminated, contaminated, or dirty/infected. The NHSN developed a risk index by which the risk of an SSI can be predicted based on three major criteria: wound classification, American Society of Anesthesiologists (ASA) score, and duration of the operation. The SSI risk category is based on the number of factors present at the time of operation, including a wound class of 3 (contaminated) or 4 (dirty), an ASA class of 3 or greater, and an operation lasting longer than the 75th percentile of the duration of the specific operation. Each independent factor is given a single point if present, which determines the NHSN risk index category (0 to 3).
- 1. Smoking
- 2. Diabetes
- 3. COPD: Chronic obstructive pulmonary disease
- 4. CAD: coronary artery disease
- 5. Nutritional status
- 6. Immunosuppression
- 7. Chronic corticosteroid use
- 8. Low serum albumin
- 9. Obesity
- 10. Advanced age
Retromuscular Prefascial Mesh Hernia Repair (Jean RIVES – René STOPPA)
An incisional hernia is usually defined as a chronic postoperative defect of the abdominal wall through which intra-abdominal viscera protrude. Progress in surgical techniques, even with laparoscopic surgery, has not led to the elimination of incisional hernias. On the contrary, the incidence of this complication seems to be increasing as more major and lengthy operations are being performed, especially in elderly patients with concomitant organic disease. The incidence of this condition has been reported to be as high as 11% of all laparotomies. Surgical repair is difficult in the patient with a large abdominal wall defect, especially if the herniated viscera has “lost its right of domain” in the abdominal cavity. It must be remembered that surgical repair of an incisional hernia is not the same thing as closure of a laparotomy. Weakening of the abdominal wall and the consequences of decreased abdominal pressure on diaphragmatic mobility and respiratory function must also be considered. Placement of a prosthetic mesh is essential because without mesh, the recurrence rate is prohibitive, varying from 30% to 60%. The which is the subject of this article, was popularized by Jean Rives and has been used in our department since 1966.
RIVES_STOPPA_HERNIA_REPAIR
SIGMOID DIVERTICULITIS : OPTIONS OF TREATMENT

Sigmoid diverticulitis is a common disease which carries both a significant morbidity and a societal economic burden. Recently published data indicate that sigmoid diverticulitis does not mandate surgical management after the second episode of uncomplicated disease as previously recommended. Rather, a more individualized approach, taking into account frequency, severity of the attacks and their impact on quality of life, should guide the indication for surgery. On the other hand, complicated diverticular disease still requires surgical treatment in patients with acceptable comorbidity risk and remains a life-threatening condition in the case of free peritoneal perforation. Laparoscopic surgery is increasingly accepted as the surgical approach of choice for most presentations of the disease and has also been proposed in the treatment of generalized peritonitis. There is not sufficient evidence supporting any changes in the approach to management in younger patients. Conversely, the available evidence suggests that surgery should be indicated after one attack of uncomplicated disease in immunocompromised individuals.
SIGMOID DIVERTICULITIS_ REVIEW ARTICLE
Ethics in Surgery : R.I.S.K.
Renewed public attention is being paid to ethics today. There are governmental ethics commissions, research ethics boards, and corporate ethics committees. Some of these institutional entities are little more than window dressing, whereas others are investigative bodies called into being, for example, on suspicion that financial records have been altered or data have been presented in a deceptive manner. However, many of these groups do important work, and the fact that they have been established at all suggests that we are not as certain as we once were, or thought we were, about where the moral boundaries are and how we would know if we overstepped them. In search of insight and guidance, we turn to ethics. In the professions, which are largely self-regulating, and especially in the medical profession, whose primary purpose is to be responsive to people in need, ethics is at the heart of the enterprise.
Responsibility to the patient in contemporary clinical ethics entails maximal patient participation, as permitted by the patient’s condition, in decisions regarding the course of care. For the surgeon, this means arriving at an accurate diagnosis of the patient’s complaint, making a treatment recommendation based on the best knowledge available, and then talking with the patient about the merits and drawbacks of the recommended course in light of the patient’s life values. For the patient, maximal participation in decision making means having a conversation with the surgeon about the recommendation, why it seems reasonable and desirable, what the alternatives are, if any, and what the probable risks are of accepting the recommendation or pursuing an alternative course.
This view of ethically sound clinical care has evolved over the latter half of the 20th century from a doctor-knows-best ethic that worked reasonably well for both patients and physicians at a time when medical knowledge was limited and most of what medicine could do for patients could be carried in the doctor’s black bag or handled in a small, uncluttered office or operating room. What practical steps can be taken by clinicians to evaluate patient attitudes and behavior relative to the patient’s cultural context so that the physician and patient together can reach mutually desired goals of care? Marjorie Kagawa-Singer and her colleagues at the University of California, Los Angeles, developed a useful tool for ascertaining patients’ levels of cultural influence. It goes by the acronym RISK:
Resources: On what tangible resources can the patient draw, and how readily available are they?
Individual identity and acculturation: What is the context of the patient’s personal circumstances and her degree of integration within her community?
Skills: What skills are available to the patient that allow him to adapt to the demands of the condition?
Knowledge: What can be discerned from a conversation with the patient about the beliefs and customs prevalent in her community and relevant to illness and health, including attitudes about decision making and other issues that may affect the physician-patient relationship.
TRATAMENTO DA TROMBOSE HEMORROIDÁRIA

A trombose hemorroidária é uma condição dolorosa e desconfortável que ocorre quando um coágulo de sangue se forma dentro de uma hemorróida. Essa condição é mais comum em gestantes, pessoas com constipação intestinal crônica, e em situações que aumentam a pressão intra-abdominal, como exercícios físicos intensos e levantamento de peso. Neste artigo, exploraremos as causas, sintomas e opções de tratamento para a trombose hemorroidária, ajudando você a entender melhor essa condição e a buscar a melhor abordagem para o seu caso.
Causas da Trombose Hemorroidária
A trombose hemorroidária geralmente está relacionada a fatores de estilo de vida e hábitos pessoais. Os principais gatilhos incluem:
- Obstipação (prisão de ventre): O esforço excessivo para evacuar aumenta a pressão nas veias do ânus, e as fezes endurecidas podem causar traumatismo no tecido anal.
- Gravidez: A pressão adicional no abdômen durante a gravidez pode contribuir para o desenvolvimento da trombose.
- Esforços prolongados e levantamento de peso: Atividades que aumentam a pressão intra-abdominal são fatores de risco.
- Higiene inadequada: A falta de cuidados apropriados na região anal pode exacerbar a condição.
- Fatores adicionais: Permanecer sentado por longos períodos, consumo excessivo de alimentos picantes e bebidas alcoólicas, e prática de sexo anal.
Sintomas da Trombose Hemorroidária
Os principais sinais de trombose hemorroidária incluem:
- Dor intensa na região anal: A dor é geralmente súbita e pode ser bastante severa.
- Sangramento: Frequentemente observado durante a evacuação.
- Inchaço e aumento de volume: Um nódulo na região anal pode se tornar arroxeado ou preto, indicando a presença de um trombo.
Tratamentos Indicados
O tratamento da trombose hemorroidária varia conforme a gravidade da condição. Entre as abordagens recomendadas estão:
- Uso de analgésicos e pomadas anestésicas: Para alívio da dor e desconforto.
- Banhos de assento: Utilizar água morna para aliviar os sintomas e reduzir o inchaço.
- Correção dos hábitos alimentares: Aumentar a ingestão de fibras e líquidos para prevenir a obstipação.
- Tratamento cirúrgico: Em casos mais graves, pode ser necessário realizar uma cirurgia para remover a hemorróida e o trombo.
Se você apresenta sintomas semelhantes, é crucial consultar um médico para uma avaliação adequada e receber o tratamento adequado.
Gostou ❔ Nos deixe um comentário ✍️, ou mande sua dúvida pelo 💬 Chat On-line.
Lembre-se: A informação aqui fornecida é para orientação geral. Sempre consulte seu médico para aconselhamento específico sobre sua situação.
Não Deixe Sua Saúde Esperar! Entre em Contato Conosco Agora!
☎️ CHAT ONLINE 📞
Entre em contato conosco através da nossa central de atendimento dedicada. Nossos especialistas estão prontos para fornecer orientações personalizadas e responder a todas as suas perguntas. Juntos, podemos trabalhar para garantir o melhor para a sua saúde.
🩺(98)991304454 & (98)988664454📲
ATENDIMENTO REMOTO (TELEMEDICINA)
🤳🏻 Agende com os nossos #especialistas pelo WhatsApp ou Telefone
📲 👩🏽⚕️ Clínico: (98) 9 9130 4454
📲 👨🏻⚕️ Cirúrgico: (98) 9 8866 4454
#TromboseHemorroidária #SaúdeDigestiva #TratamentoHemorroidário #BemEstar #CuidadosComASaúde