Mirizzi’s Syndrome

INTRODUCTION
First described by Pablo Mirizzi in 1948 as “functional hepatic syndrome”, Mirizzi’s syndrome was initially thought to be the result of a “physiologic sphincter” of the hepatic duct. It is now understood to be a result of mechanical obstruction of the common hepatic duct secondary to an impacted stone in the gallbladder neck, Hartmann’s pouch, or the cystic duct. The syndrome is very uncommon in Western populations with a reported prevalence of 0.05%-5.7% in large modern series of patients undergoing biliary surgery. With chronic stone impaction, inflammation and recurrent cholangitis can develop with subsequent erosion into the common bile duct (CBD) and resultant biliobiliary fistula between the gallbladder and CBD.
CLASSIFICATION
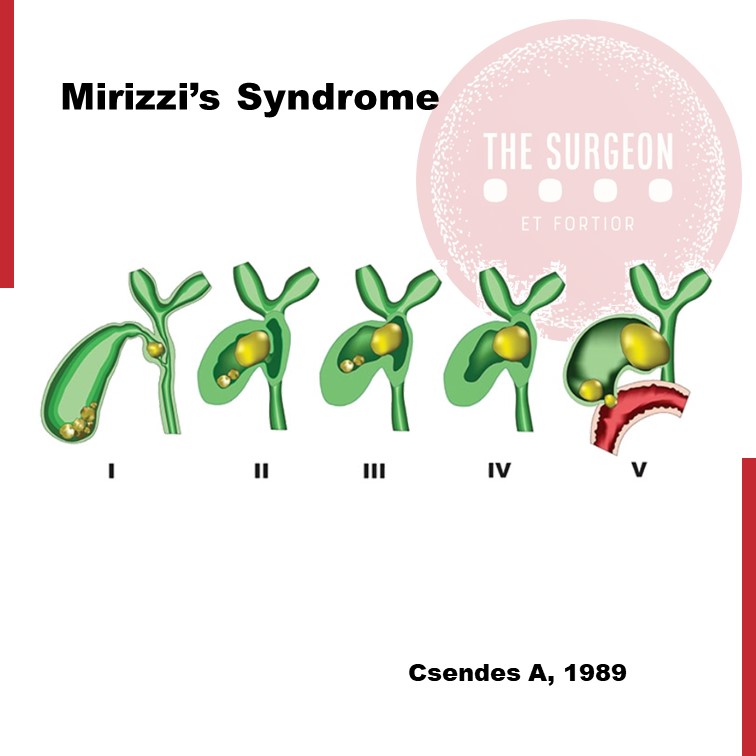
The syndrome encompasses a spectrum of disease. Broadly speaking, Mirizzi’s syndrome can be grouped into two major categories: (1) external compression of the CBD without a fistula (Type 1), and (2) erosion into the CBD causing a cholecystobiliary fistula (Type II-IV). Csendes classification is currently being used to reflect the above classification. Retrospective studies have identified an association between Mirizzi’s syndrome and gallbladder cancer, with an incidence as high as 28%, relative to an incidence of 1-2% in patients with uncomplicated gallstone disease. As with other malignant processes of the biliary tract, biliary stasis and chronic inflammation have been suggested to play a role. In general, it is difficult to distinguish benign Mirizzi’s syndrome from a neoplastic process preoperatively, although older patient age, significantly elevated Ca 19-9, and imaging features suggestive of invasion into the liver or a mass filling the gallbladder should raise suspicion for malignancy.
CLINICAL FINDS
The most common presenting symptoms are right upper quadrant pain, jaundice, nausea/vomiting, and fever. This spectrum of findings overlaps with several other pathologic processes of the hepatobiliary tract, making preoperative diagnosis difficult. Additionally, the clinical picture may be complicated by the concurrent presence of acute cholecystitis, pancreatitis, or even gallstone ileus. Mirizzi’s syndrome should be suspected in any patient presenting with right upper quadrant pain and abnormal liver enzymes (particularly elevated bilirubin and alkaline phosphatase) or imaging suggestive of an impacted stone. Three findings on imaging together suggest a diagnosis of Mirizzi’s: 1) dilation of the biliary system above the level of the gallbladder neck, 2) the presence of a stone impacted in the gallbladder neck, and 3) an abrupt change to a normal width of the common duct below the level of the stone. Such findings should prompt further imaging to better define the biliary tree, either indirectly though magnetic resonance cholangiopancreatography (MRCP), or directly through endoscopic retrograde cholangiopancreatography (ERCP) or percutaneous transhepatic cholangiography (PTC). No imaging modality is entirely sensitive for Mirizzi’s syndrome and the key is to maintain a high index of suspicion.
MANAGEMENT
Management of Mirizzi’s syndrome depends on the degree of fistula. In Type I disease, laparoscopic cholecystectomy is usually achievable, either total (classic) or subtotal, depending on the specific intraoperative findings. If the view of safety can be attained with the critical structures isolated, a classic cholecystectomy may be performed. If the view of safety cannot be achieved due to inflammation or adhesions, the gallbladder is taken down retrograde and opened near the cystic duct orifice. All stones are removed, including any impacted stones, and the cystic duct orifice is examined for the presence of bile to determine whether it is patent. If the cystic duct is patent, it should be ligated (if possible), or the remnant gallbladder should be sutured closed over it (choledochoplasty). An external closed suction drain may be left in the gallbladder fossa and removed the following day if drainage is non-bilious. More commonly, the cystic duct is obliterated, and a subtotal cholecystectomy with removal of all stones is sufficient.
Management of Mirizzi’s syndrome in the presence of a biliobiliary fistula is more complex. If the fistula involves <1/3 of the CBD circumference (Type II), options include primary repair using absorbable suture, closure over a T-tube, or choledochoplasty using the remnant gallbladder. The last approach is preferable to maintain the diameter of the CBD and minimize the risk of subsequent stricture but requires that sufficient gallbladder remnant be available to allow closure. In the presence of a more extensive fistula (Type III or IV), bilioenteric anastomosis is usually the best option.










