Chronic pancreatitis is a progressive, destructive inflammatory process that ends in destruction of the pancreatic parenchyma resulting in malabsorption, diabetes mellitus, and severe pain. The etiology of chronic pancreatitis is multifactorial. About 65–70% of patients have a history of alcohol abuse, the remaining patients are classified as idiopathic chronic pancreatitis (20–25%), including tropical pancreatitis, a major cause of childhood chronic pancreatitis in tropical regions, or unusual causes including hereditary pancreatitis, cystic fibrosis, and chronic pancreatitis-associated metabolic and congenital factors. Current evidence suggests that a combination of predisposing factors, including environmental, toxic, and genetic, are involved in most patients rather than one single factor. The best-known hypotheses about the pathogenesis of chronic pancreatitis include necrosis-fibrosis, toxic-metabolic, oxidative stress, plug and stone formation with duct obstruction, and primary duct obstruction. Repeated episodes of inflammation initiated by autodigestion, one or more episodes of severe pancreatitis, oxidative stress, and/or toxic-metabolic factors lead to activation and continued stimulation of parenchymal pancreatic stellate cells. These stellate cells cause the fibrosis characteristic of chronic pancreatitis. Nevertheless, multiple hypotheses exist to explain the pathophysiology in the various subgroups of patients with chronic pancreatitis, but to date there is no single unifying theory.
OPERATIVE TREATMENT
There are several different concepts for the operative treatment of chronic pancreatitis. The concept of preservation of functioning pancreatic parenchyma (drainage operations) would be the goal for protection against further loss of pancreatic function. The second main concept is based on resective procedures either in the situation where there is no dilation of the pancreatic duct, if the pancreatic head is enlarged, or if a pancreatic carcinoma is suspected in the setting of chronic pancreatitis. These two concepts involve different operative procedures.
Drainage procedures
Sphincterotomy of the pancreatic duct was one of the first operative procedures proposed for patients with a dilated pancreatic duct in chronic pancreatitis with presumed obstruction or stenosis at the papilla Vater. Unfortunately, this procedure was associated with minimal lasting success for the amelioration of pain, indicating that a stenosis at the papilla of Vater is not the cause of pain in chronic pancreatitis nor the cause of ductal dilation. In contrast, direct ductal-enteric drainage by the original Puestow procedure or its modification by Partington and Rochelle is more successful in patients with chronic pancreatitis and a dilated pancreatic duct. The original Puestow procedure included resection of the tail of the pancreas with filleting open the pancreatic duct proximally along the body of the pancreas with anastomosis to a Roux-en-Y loop of jejunum. Partington and Rochelle modified the Puestow procedure by eliminating the resection of the pancreatic tail. A recent procedure involves a wedge-shaped opening of the pancreatic duct (even when the duct is <5 mm) with a subsequent pancreatico-jejunostomy. The preservation of functional tissue and reduction of operative mortality to less than 1% and morbidity to less than 10% are the goals and benefits of this operation. Unfortunately, large series have reported persistence or recurrence of pain at long-term follow up (>5 year) in 30–50% of patients; in addition, patients with a dominant mass in the head of the pancreas and a non-dilated pancreatic duct do not appear to profit from a drainage procedure at all. A recent randomized controlled trial demonstrated that operative drainage in selected patients with a large duct was more effective than endoscopic treatment in patients with obstruction of the pancreatic duct.
Pancreatic Resections
Pancreatoduodenectomy (Kausch-Whipple procedure). For many surgeons, a pancreatoduodenectomy is the gold standard for patients with the pain of chronic pancreatitis, although the newer, duodenum-preserving procedures are good (and possibly better) alternatives as well (see below). The approach of resection of the proximal gland is based on Longmire’s tenet that the ‘‘pacemaker’’ of pain is in the head of the pancreas. The indications for pancreatoduodenectomy in patients with chronic pancreatitis and pain are:
(1) a non-dilated pancreatic duct (diameter < 6 mm measured in the body of the gland),
(2) an enlarged head of the pancreas, often containing cysts and calcifications,
(3) a previous, ineffective ductal drainage procedure, and/or
(4) when there is the possibility of malignancy in the head of the gland.
This latter subgroup comprises up to 6–10% of patients undergoing operative intervention for chronic pancreatitis. After pancreatoduodenectomy, > 80% of patients have permanent pain relief, which is greater than after a drainage operation. In experienced centers, a pancreatoduodenectomy can be performed with a low operative mortality rate (< 2%), and a morbidity of 40%. Although the classic pancreatoduodenectomy has these advantages, there is some long-term morbidity in chronic pancreatitis patients, especially regarding quality of life. In addition to development of diabetes, patients experience postoperative digestive dysfunction, including dumping, diarrhea, peptic ulcer, and dyspeptic complaints. To address these effects of the classic pancreatoduodenectomy which involved a distal gastrectomy, ‘‘organ-preserving’’ operations like the pylorus-preserving pancreatoduodenectomy. Symptoms of dumping and bile-reflux gastritis can be decreased by preserving the stomach, the pylorus, and the first part of the duodenum. In addition, regarding quality of life, a pylorus-preserving technique provides better results than the classic pancreatoduodenectomy procedure; weight gain occurs in 90% of the patients postoperatively while still leading to long-lasting pain relief in 85–90% of the patients. Pylorus-preserving resections, however, appear to have a greater incidence of transient delayed gastric emptying postoperatively (20–30% of the patients) as well as the risk of cholangitis and the long-term occurrence of exocrine and endocrine pancreatic insufficiency (seen in >45% of patients), representing the possible drawbacks of this operation in chronic pancreatitis patients. The relevant studies (level I and II) comparing classic with pylorus preserving pancreatoduodenectomy could not demonstrate a clear advantage for either resection. One should remember, however, that pancreatoduodenectomy was originally introduced to treat malignant pancreatic or periampullary disease by an oncologic resection. Therefore, for a benign disorder such as chronic pancreatitis, there is no reason – other than the occasional inability to exclude pancreatic cancer definitely – to remove peripancreatic organs (the distal stomach, the duodenum, and the extrahepatic bile ducts), which are involved only secondarily in chronic pancreatitis. This concept stimulated the development of organ-preserving pancreatic resections.
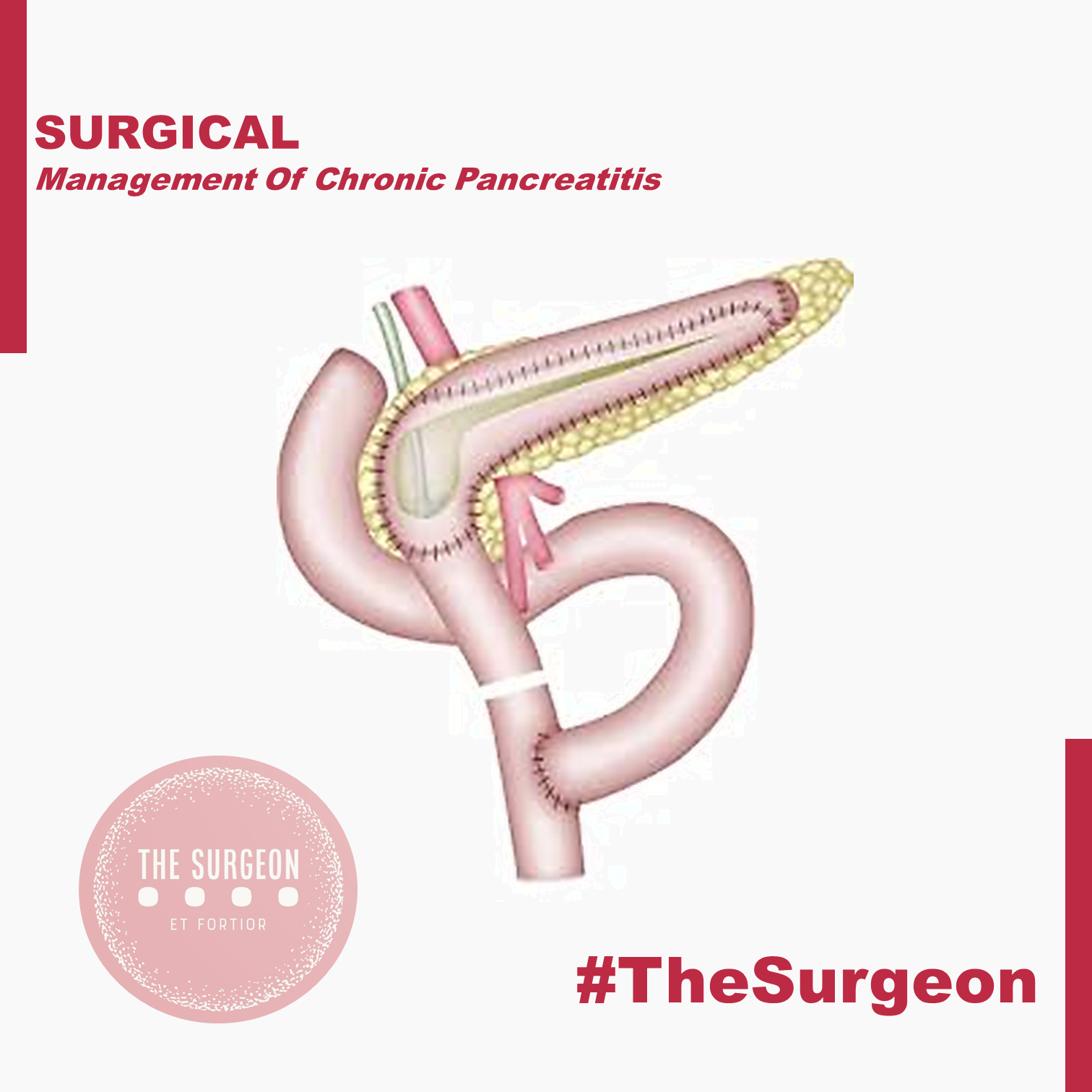
Duodenum-preserving pancreatic head resection (DPPHR).
This procedure addresses patients with a dominant mass in the head of the pancreas with or without a dilated main pancreatic duct. The duodenum-preserving resection (Beger procedure) includes a ventral dissection and dorsal mobilization of the head of the pancreas. After division of the pancreas anterior to the porto-mesenteric vein (as with a pancreatoduodenectomy), the resection is carried out toward the papilla of Vater. A subtotal resection of the pancreatic head is carried out leaving a small margin of pancreatic tissue associated with the duodenum containing the common bile duct; a small rim of pancreatic tissue toward the vena cava should be preserved as well during removal of most all of the uncinate process. In most patients, it is possible to free the bile duct from the surrounding scarring without disrupting continuity with the ampulla of Vater, thereby avoiding the need for a bilio-digestive anastomosis.
In some patients (20%), the common bile duct is obstructed and should be opened, so that the bile will drain into the cavity of the resected pancreatic head which is drained into a Roux-en-Y limb of jejunum. The standard reconstruction consists of a Roux-en- pancreaticojejunostomy to the distal pancreatic remnant (body and tail of pancreas) and a pancreatojejunostomy to the rim of pancreas at the duodenum (including the opened bile duct if needed). In up to 10% of patients, this DPPHR procedure is combined with a lateral pancreaticojejunostomy to drain multiple stenoses of the main pancreatic duct. The mortality rate is low (1%), and the morbidity rate is around 15%, less than after pancreatoduodenectomy.
When compared with pancreatoduodenectomy in patients with chronic pancreatitis, the DPPHR offers the advantage of preserving the duodenum and extrahepatic biliary tree, and its superiority over even the pylorus-preserving resection has been shown in prospective studies. Patients who underwent the DPPHR had greater weight gain, a better glucose tolerance, and a higher capacity for insulin secretion. In long-term follow-up, about 20% of the patients developed new onset of diabetes mellitus, like the incidence of diabetes after pancreatoduodenectomy. There is some evidence that endocrine function may be better preserved after DPPHR when compared with patients with chronic pancreatitis not undergoing operation, secondary to the relief of pancreatic ductal obstruction/hypertension. Regarding pain status, 90% of patients after DPPHR have long-term relief of pain. Regarding quality of life, 69% of the patients in one study were rehabilitated professionally, 26% retired, and only 5% of the patients were unimproved. Considering the better pain status, a lesser frequency of acute episodes of chronic pancreatitis, especially in those patients with an enlarged pancreatic head, marked decrease in the need for further hospitalization, low early and late mortality rate, and the restoration of a better quality of life, evidence suggests that DPPHR may delay the natural course of the disease of chronic pancreatitis.
The DPPHR was modified by Frey and colleagues to include a longitudinal pancreatico-jejunostomy combined with a local ‘‘coring out’’ of the pancreatic head without the need for an extensive dissection near the superior mesenteric vessels as with the DPPHR. The Frey and DPPHR have undergone evaluation in multiple comparative trials, confirming their effectiveness as operative procedures for chronic pancreatitis. A modified technique (Bern procedure) of the Beger and Frey procedures has been described recently in patients with chronic pancreatitis. This extended Frey procedure combines the advantages of the Beger and Frey procedure by maintaining a non-anatomic, subtotal central pancreatic head resection but without the need for transsection of the gland over the superior mesenteric vein (SMV), the most tedious part of the DPPHR procedure which was the major advantage offered by the Frey procedure. This modified technique reduces the risk of intraoperative bleeding which is especially increased in the presence of portal hypertension.
Left-sided pancreatic resection (distal pancreatectomy)
Most surgeons believe that the pancreatic head is the pacemaker in chronic pancreatitis, and therefore, pancreatic head resections should be the target for most patients with chronic pancreatitis affecting the entire gland. There is, however, a small and carefully selected group of patients in whom a left-sided pancreatic resection is the appropriate treatment. This subgroup is selected by imaging techniques, including CT, ERCP, or MRI outlining inflammatory complications, such as pseudocysts, fistula, and pancreatic duct stenosis, involving only (or primarily) the body and/or tail region of the pancreas. A good example is the patient who develops a mid-ductal stricture after an episode of necrotizing pancreatitis secondary to gallstone pancreatitis. Similarly, suspicion of a neoplasm or recurrent acute pancreatitis believed secondary to an isolated, mid-ductal stricture may be justification for a left-sided pancreatic resection. Overall, about 10% of all patients who undergo operative intervention for chronic pancreatitis may be candidates for a distal pancreatectomy. These distal pancreatectomies for benign disease can be performed without splenectomy, but conservation of the splenic artery and vein can be difficult and is time-consuming. Nevertheless, the advantage of avoiding the possibility of overwhelming postsplenectomy sepsis should be taken into consideration as well as the importance of the spleen for maintenance of the host defense system. Thus, preservation of the spleen is desirable if there is no clear indication for splenectomy, such as perisplenic pseudocyst or inflammatory/fibrotic encasement of the splenic vessels.
Central pancreatectomy (middle segmentectomy).
Benign lesions of the neck and proximal body of the pancreas, such as the exceedingly rare focal chronic pancreatitis or post-traumatic pancreatitis, pose an interesting operative challenge. If the lesions are not amenable to simple enucleation, surgeons may be faced with the choice of performing a right-sided resection (pancreatoduodenectomy) or a left-sided resection (distal pancreatectomy) to include the lesion, resulting in resection of a substantial amount of otherwise functioning pancreatic parenchyma. Central pancreatic resections have been reported primarily for benign or low-grade neoplasms with Roux-en-Y pancreatojejunostomy reconstruction. Central pancreatectomy affords the possibility of saving functional pancreatic tissue in attempt to avoid the complications of pancreatic insufficiency. Further studies, however, must prove the effectiveness of such an operation for patients with chronic pancreatitis. Central resections in patients with chronic pancreatitis must be viewed with caution and considered only in highly selected cases.
Pancreatic resection with islet cell autotransplantation.
Because of the concerns of pancreatic endocrine insufficiency after any pancreatic resection for chronic pancreatitis, renewed interest has focused on the possibility of performing a total pancreatectomy, isolating the islets, and reinfusing (autotransplanting) the islets into the liver. Improvements in islet cell harvesting and preservation for islet cell allotransplantation for diabetics have allowed new enthusiasm in this technique for patients with chronic pancreatitis. Results to date are encouraging, but the inability to harvest reliably an adequate number of islets and to prove successful engraftment within the liver remain current limitations. This approach may be more effective early in the disease when islets have not been depleted.
OUTCOMES
In summary, definite evidence for the best operative method for treating painful chronic pancreatitis is still not fully accepted. The study designs in the few randomized controlled trials (evidencebased Level I data) available today have some limitations in design and reporting of morbidity and include only small numbers of patients. Nevertheless, the different variations of the DPPHR, Beger, Frey, and Bern procedures appear to be as equally successful in achieving long-term pain control as pancreatoduodenectomy, but they have fewer postoperative complications and appear to be superior with regard to preservation of pancreatic function and quality of life.










