Surgical Technique of Liver Resection for the Treatment of HCC
The incidence of HCC is increasing in the worldwide. Surgery in the form of liver resection or transplantation remains the mainstay of curative treatment for HCC, even though selected patients with small tumours may also be cured with ablation. Liver resection and transplantation are not necessarily two binary choices in most patients and, despite all the debates, are often complementary treatment modalities ideally suited to different patient groups. Thus characterisation of patient and tumour characteristics to guide decision making is vital to achieve the best outcome for patients.
1.Anatomical Resection or Not?
The aim of liver resection in patients with HCC and CLD is that it should be curative with resection of tumour vascular territories and also preserve as much liver volume as possible to prevent postoperative liver failure. EASL guidelines recommend anatomical resection of HCC, whereby the lines of resection match the limits of one or more functional segments of the liver. This is based on evidence suggesting superior oncological outcomes in addition to a reduction in the risk of bleeding and biliary fistula. Although there are no randomised data, a meta-analysis including 2000 patients from 12 non-randomised comparative trials did not show any benefit of anatomical compared with non-anatomical resection in 1-, 3- and 5-year survival, recurrence rate, postoperative morbidity or blood loss . It is practice to perform an anatomical resection for tumours >2 cm, and for smaller tumours in anatomically favourable positions, a wedge with adequate margin is often sufficient. Modifying techniques to maximise parenchymal preservation preserving adequate margins are often the key in these patients.
2. Anterior Approach
The anterior approach, as described by Professor Belghiti , has been advocated for large right-sided tumours. This technique involves transection of the liver parenchyma to the IVC without mobilisation of the liver with the theoretical advantage of less tumour seeding. A prospective randomised controlled trial compared the anterior and conventional approach on 120 patients with large (>5 cm) HCCs. The anterior approach group had less blood transfusion requirements and a significantly longer overall survival (68.1 v 22.6 months; p = 0.006).
3.Parenchymal Transection
As in liver resection for other indications, there is no good evidence to indicate that a single method of parenchymal transection, application of fibrin sealants or intermittent inflow occlusion is beneficial in surgery for HCC. There is also no evidence to suggest that using special equipment for liver resection is of any benefit in decreasing the mortality, morbidity, or blood transfusion requirements. Surgeons should use techniques in which they have been trained and can demonstrate acceptable outcomes.
4. Laparoscopic Approach
Laparoscopic HCC resections are gaining popularity as the approach is more widely adopted across centres. It is important that patients for laparoscopic resection are selected based on the technical capabilities of the surgeon and centre, and the proper mentoring takes place during the learning curve. A summary of published metaanalyses concluded that the laparoscopic approach was associated with improved short-term outcomes (blood loss, complication rates and hospital length of stay) without compromising long-term oncological outcomes. It is worth noting that there are no randomised data; however a number of trials are in progress. Furthermore,their analysis suggested that the incidence of postoperative ascites and liver failure is decreased in the selected group of laparoscopic liver resections . A further metaanalysis of cirrhotic patients up to Child-Pugh B undergoing laparoscopic compared with open liver resection for HCC confirmed these perioperative benefits .
5. Robotic Approach
Although still very much in its infancy, the application of robotic surgery to HCC resection can theoretically yield similar advantages in short-term outcomes to the laparoscopic technique. The only comparative study between robotic and open liver resection for HCC included 183 patients undergoing robotic hepatectomy who were compared using propensity scoring with a cohort of 275 open resections. The robotic group required longer operating time (343 vs 220 min), shorter hospital stays (7.5 vs 10.1 days) and lower dosages of postoperative patient-controlled analgesia (350 vs 554 ng/kg). The 3-year disease-free survival of the robotic group was comparable with that of the open group (72.2% vs 58.0%; p = 0.062), as was the 3-year overall survival (92.6 vs 93.7%; p = 0.431). The associated financial costs of robotic surgery still pose a limitation to its adoption, and it is unclear if this approach is associated with any significant advantages over laparoscopic rather than open resection.
6. Associating Liver Partition with Portal Vein Ligation for Staged
Hepatectomy (ALPPS)/TAE/PVE
ALPPS is still considered an experimental technique in which a first-stage procedure consisting of physical liver splitting and portal vein ligation is followed by a second stage of resection of the HCC and associated liver segments. The advantage seen in colorectal liver metastases is that of rapid hypertrophy for the FLR. There are only limited data describing outcomes of ALPPS for HCC; however an analysis of 35 patients in the international ALPPS registry showed an impressive FLR hypertrophy of 47% following the first stage of the procedure that was associated with a 31% perioperative mortality rate. The majority of these patients were in the intermediate-stage category of the BCLC algorithm. Further evaluation is required prior to routine use of ALPPS for HCC resection, and it is the view of the authors that ALPPS may be a procedure best reserved for carefully selected patients who have bilateral disease.
7. Combined Resection with RFA for Bilobar HCC
For patients with multiple or bilobar HCC in whom resection is contraindicated due to inadequate FLR, combined resection and radiofrequency ablation (RFA) may yield better results than alternative treatments. A single-centre study compared patients with bilobar liver HCCs who underwent resection (n = 89), combination of resection and RFA (n = 114) and TACE (n = 161). The results showed that 1-, 3- and 5-year survival was better in both resection and combined resection, and RFA groups compared with TACE and survival and disease-free survival were comparable between both surgical groups. They concluded that resection combined with RFA provided a chance for cure in patients with bilobar HCC, and provided liver function is preserved, aggressive treatment can improve prognosis.
Anatomia Cirúrgica Pancreática
A anatomia cirúrgica do pâncreas é um dos tópicos mais fascinantes e desafiadores da cirurgia do aparelho digestivo. Conhecer detalhadamente a estrutura e a topografia do pâncreas é crucial para a realização de procedimentos cirúrgicos seguros e eficazes. Neste artigo, vamos explorar os aspectos mais importantes da anatomia pancreática, abordando pontos-chave para estudantes de medicina e residentes de cirurgia do aparelho digestivo.
Estrutura Anatômica do Pâncreas
O pâncreas é uma glândula retroperitoneal situada transversalmente no abdome, na altura das vértebras L1-L2, abrangendo os principais vasos sanguíneos e a coluna vertebral. Ele é composto por cinco partes principais: cabeça, colo, corpo, cauda e processo uncinado.
- Cabeça: Localizada à direita da linha média, cercada pelo duodeno. A cabeça do pâncreas possui uma extensão inferior chamada processo uncinado, que está intimamente relacionada com a veia mesentérica superior e a artéria mesentérica superior.
- Colo: Uma parte estreita entre a cabeça e o corpo, situada anteriormente à veia porta, definida pela localização anatômica anterior à formação da veia porta, geralmente pela confluência das veias mesentérica superior e esplênica.
- Corpo: Estende-se para a esquerda, posterior ao estômago, com a superfície anterior coberta pelo peritônio, formando parte da parede posterior do saco menor.
- Cauda: Parte terminal que se estende até o hilo esplênico, confinada entre as camadas do ligamento esplenorrenal juntamente com a artéria esplênica e a origem da veia esplênica.
- Processo Uncinado: Considerado uma parte distinta do pâncreas devido à sua origem embriológica diferente, estendendo-se posteriormente aos vasos mesentéricos superiores.
Peso e Dimensões Normais
Em um adulto saudável, o pâncreas tem um peso médio de aproximadamente 80 a 120 gramas. As dimensões normais do pâncreas variam, mas geralmente medem cerca de 15 a 20 cm de comprimento, 4 a 5 cm de largura na cabeça, e 1,5 a 2,5 cm de espessura.
Vascularização do Pâncreas
A vascularização do pâncreas é complexa e vital para a compreensão cirúrgica. As principais artérias que irrigam o pâncreas são:
- Artéria Pancreatoduodenal Superior: Ramo da artéria gastroduodenal que irriga a cabeça do pâncreas.
- Artéria Pancreatoduodenal Inferior: Ramo da artéria mesentérica superior que também fornece sangue à cabeça do pâncreas.
- Ramos Pancreáticos da Artéria Esplênica: Irrigam o corpo e a cauda do pâncreas.
As veias pancreáticas drenam para a veia esplênica, veia mesentérica superior e, eventualmente, para a veia porta.
Ductos Pancreáticos
O pâncreas possui dois principais ductos: o ducto pancreático principal (ducto de Wirsung) e o ducto pancreático acessório (ducto de Santorini).
- Ducto Pancreático Principal (Ducto de Wirsung): Começa na cauda do pâncreas e percorre o corpo até a cabeça, onde geralmente se junta ao ducto biliar comum na ampola de Vater, regulada pelo esfíncter de Oddi. O diâmetro normal do ducto pancreático principal varia de 1 mm na cauda até 3 mm na cabeça.
- Ducto Pancreático Acessório (Ducto de Santorini): Corre superior e paralelo ao ducto de Wirsung, drenando parte da cabeça do pâncreas na papila duodenal menor.
O esfíncter de Oddi é uma estrutura única de fibras musculares lisas que regula o fluxo das secreções biliares e pancreáticas para o duodeno e impede o refluxo do conteúdo intestinal para o sistema ductal pancreatobiliar.
Considerações Cirúrgicas
Entender a anatomia pancreática é essencial para evitar complicações durante procedimentos cirúrgicos. Algumas das considerações importantes incluem:
- Ressecção Pancreática: Procedimentos como a pancreatoduodenectomia (procedimento de Whipple) requerem um conhecimento detalhado das relações anatômicas para garantir a remoção eficaz do tumor com a menor morbidade possível.
- Drenagem Biliar: A proximidade do pâncreas com o ducto biliar comum exige precisão ao evitar danos durante as cirurgias.
- Anastomoses Pancreáticas: A criação de anastomoses seguras entre o pâncreas e o intestino é crítica para prevenir complicações pós-operatórias, como fístulas pancreáticas.
Variações Anatômicas
As variações anatômicas do pâncreas e dos ductos pancreáticos são comuns e podem impactar significativamente a abordagem cirúrgica. Uma compreensão detalhada dessas variações é essencial para a personalização do plano cirúrgico. Por exemplo, o pâncreas anular é uma condição em que o tecido pancreático forma um anel ao redor do duodeno, podendo causar estenose duodenal.
Conclusão
A anatomia cirúrgica pancreática é um campo complexo e detalhado que exige estudo e prática contínuos. Compreender as nuances dessa anatomia é fundamental para qualquer cirurgião do aparelho digestivo. Como disse o renomado anatomista Andreas Vesalius: “A anatomia é a fundação de todas as ciências médicas.”
Gostou? Nos deixe um comentário ✍️, ou mande sua dúvida pelo 💬 Chat On-line em nossa DM do Instagram.
Hashtags
#AnatomiaPancreática #CirurgiaDigestiva #EstudantesDeMedicina #ResidentesDeCirurgia #Pancreas

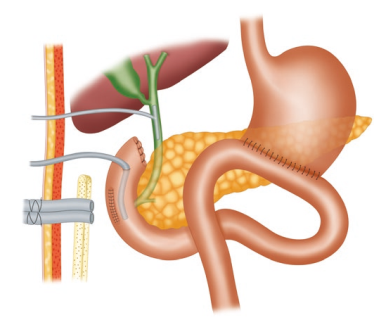
Dumping Syndrome After Gastric Bypass (RYGB)
Obesity is one of the most significant health problems worldwide, and the prevalence has been increasing over the past decade. Despite improvement in the performance of bariatric surgery, complications are not uncommon. These complications vary according to baseline patient characteristics, the duration of time since the operation, and the type of bariatric surgery performed. Endoscopy is the cornerstone in the diagnosis of postoperative complications after bariatric surgery, and may even be performed in the early postoperative course. With an increasing number of patients being referred for endoscopic evaluation following bariatric surgery, it is essential to develop an understanding of the anatomic changes for optimal assessment and appropriate treatment of these patients.

Early and late dumping syndrome occurs not uncommonly in patients who have undergone gastric bypass surgery when large quantities of simple carbohydrates are ingested. Early dumping typically occurs within 15 minutes of ingestion and has been attributed to rapid fluid shifts from the plasma into the bowel from hyperosmolality of the food. Late dumping occurs hours after eating and results from hyperglycemia and the subsequent insulin response leading to hypoglycemia. When hypoglycemia is severe, treatment with a low carbohydrate diet and an alphaglucosidase inhibitor may be effective. Furthermore, restoration of gastric restriction using an endoscopic approach to reduce the aperture of the GJA has also demonstrated to be effective in management of this condition.
TREATMENT
The initial management of dumping syndrome is dietary modifications. Recommendations include consuming smaller meals by dividing daily calorie intake into six meals and delaying liquids at least 30 min after meals Rapidly absorbable simple carbohydrates should also be avoided. Adjuncts to diet modification include pectin and guar gum, which slow down gastric emptying by increasing food viscosity. Acarbose, which interferes with carbohydrate absorption in the small intestines, has also proven to relieve symptoms in small studies. After dietary modifications, medications such as somatostatin analogs (e.g., octreotide) alleviate symptoms by delaying gastric emptying and small bowel transit time, as well as inhibiting gastric hormones and insulin secretion. Multiple studies have evaluated both short- and longterm somatostatin therapies, with results showing sustained symptom control in patients refractory to dietary modifications. In severe cases refractory to medical management, surgical interventions, such as narrowing of the anastomosis, conversion of the prior bariatric surgery, and using jejunostomy parenteral feeding, may help. Follow-up with gastrointestinal specialists and the patient’s bariatric surgeon is strongly recommended if dumping syndrome is suspected.
Differential Diagnosis
An important metabolic complication which is attracting increasing interest is postprandial hyperinsulinemic hypoglycemia (PHH), characterized by hypoglycemic symptoms developing 1–3 h after a meal accompanied by a low blood glucose level. This condition should be distinguished from early dumping syndrome where symptoms develop within minutes to 1 h after a meal of caloric dense food, caused by the rapid and unregulated emptying of food into the jejunum, which induces rapid fluid entry into the small bowel. Early dumping often occurs early in the postoperative period, most commonly after Roux-en-Y gastric bypass, whereas PHH may develop months to years after surgery.
Symptoms related to post-PHH usually develop late after surgery in contrast to early dumping. Symptoms are wide ranging, but are usually related to Whipple’s triad: symptomatic hypoglycemia, a low plasma glucose level, and resolution of symptoms after the administration of glucose. Symptoms of hypoglycemia may include anxiety, sweating, tremors, palpitations, confusion, weakness, lightheadedness, dizziness, blurred vision, disorientation, and possibly loss of consciousness.
Because of variability in degree of symptoms and the absence of a clear pathophysiology, management of this condition can be challenging. Fortunately, a significant percentage of patients with milder forms of the condition can be managed with dietary modifications consisting of frequent small meals with a low glycemic index. This requires supervision by a dietitian and long-term patient compliance. Additional benefit has been obtained by the addition of acarbose, an α glucosidase inhibitor in doses 100–300 mg. Successful management has been also reported in case reports or small case series with diazoxide, calcium channel blockers, and somatostatin analogues. The role of GLP-1 in the pathogenesis of this condition is supported by the observation that infusions of GLP-1 antagonists corrected hypoglycemia in these patients. These agents are investigational at present, but provide opportunity for additional future treatment approaches. For patients with persistent symptoms despite medical treatment, reversal of the bariatric procedure should be considered. Partial pancreatectomy, although used in the past, is now not recommended because of the significant morbidity and poor long-term symptom control. Postprandial hyperinsulinemic hypoglycemia is an important, potentially dangerous late complication of metabolic surgery. Successful diagnosis and management of this condition requires multidisciplinary specialty resources and essential long-term follow-up capabilities.
Nutritional Management of Acute Pancreatitis
Acute pancreatitis is a common intra-abdominal inflammatory condition of varied aetiology. The disease is mild in the vast majority of patients and has a favourable outcome. The acute severe form of the disease on the other hand is a lethal form with a high mortality and morbidity. A number of strategies have provided clinical benefit in severe acute pancreatitis (SAP). Of these, nutritional management is by far the most effective. SAP is associated with persistent end-organ failure, commonly respiratory, circulatory and renal. Treatment is targeted to support these organs. As of now there is no definitive therapy for acute pancreatitis. Patients are managed with fluids, analgesics, antibiotics and nutritional supplements besides adequately treating local complications such as pseudocyst and walled-off pancreatic necrosis by suitable interventional methods, be it endoscopic or percutaneous. The focus here is nutritional support in the management of SAP.
Which Form of Nutrition: Parenteral or Enteral?
This depends largely on the functional integrity of the stomach and small intestine. Patients of SAP often have poor gastric emptying and paralytic ileus, which is made worse with the use of narcotics. Moreover, local complications of pancreatitis (peripancreatic fluid collections) can have a pressure effect on the stomach and/or duodenum. As a result oral feeds may not be possible in these patients. Patients on ventilator support also cannot be given oral feeds.
Enteral feeding through the nasogastric or nasojejunal tubes is often not tolerated by patients because of discomfort. In addition, these tubes often get displaced or withdrawn. Reinsertion of the tubes, under endoscopic or radiological guidance, is cumbersome in such patients. All these factors favour parenteral feeding. The distinct advantage of enteral nutrition is that it prevents mucosal atrophy and transmigration of bacteria (an important causeof sepsis in SAP). Also, enteral feeding augments intestinal motility and is cheaper than parenteral preparations. Enteral nutrition improves motility in patients with paralytic ileus. The relative merits of these forms of nutritional therapy have been evaluated in a systematic review. Eight published randomized trials including a total of 348 patients were included. Enteral feeding was given through a nasojejunal tube and parenteral nutrition through a catheter placed in a central vein. Enteral nutrition was shown to reduce mortality, multi-organ failure, systemic infection and surgical intervention in comparison with parenteral nutrition. The length of hospital stay too was shown to be reduced. In view of these, enteral nutrition appears to be a better option while managing patients of SAP and has been recommended by the American College of Gastroenterology, American Gastroenterological Association and International Association of Pancreatology.
When should enteral feeding be started?
Patients with mild acute pancreatitis can usually be started on oral feeds in 2–3 days. Those with moderately severe acute pancreatitis can be started on oral feeding only after a variable period and hence should receive enteral nutritional support. Early enteral feeding has been shown to avoid end-organ failure in a large series of patients (1200).
Enteral feeding started within 48 h of onset of illness was associated with organ failure in 21% of patients as opposed to 81% when enteral feeding was started after 48 h. This benefit of early enteral feeding has also been shown in a recent meta-analysis. However, there was no benefit in mortality with early enteral feeding. In yet another randomized controlled trial, early enteral feeding (within 24 h) was compared with on-demand enteral feeding after 72 h.
The primary endpoint of this study was major infection or death. The study did not detect any significant difference in the primary endpoint in either group (early or on-demand feeding). However, it did show that patients receiving on-demand nutrition tolerated oral feeds without using a tube.
- Nasogastric or Nasojejunal
Should the feed be administered in the stomach through a nasogastric (NG) tube or in the jejunum through a nasojejunal (NJ) tube? Gastric feeding is thought to increase pain and aggravate pancreatitis due to food-induced pancreatic stimulation. In view of this, NJ feeding is practised. However, placement of a NJ tube is cumbersome and needs a skilled endoscopist or radiologist. It causes more inconvenience to patients. A nasogastric (NG) tube is thus an alternative. A number of studies have been published comparing NG and NJ feeding. The results of these studies can be summarized as follows: There was no difference in mortality. Feeds were equally tolerated in the two groups and NG feeding is simple. NG feed was not shown to increase pain and is thus as good as NJ feeding. A meta-analysis subsequently published showed no difference in mortality, hospital stay and infection rate between the two groups. Both forms of feeding were equally well tolerated. NJ feeding thus is not advised in the management of most patients with SAP. However, it still has a place when the patient has a high risk of aspiration. Also, patients on a ventilator and those not tolerating NG feed should be fed through NJ tube. The other issue concerning enteral feeding in SAP is the composition of the feed.
- Type of Formulation
Various commercially available formulations include (1) polymeric formulations comprising complex lipids, carbohydrates and proteins and (2) elemental formulations comprising simple amino acids, carbohydrates and free fatty acids. Other formulations used are glutamine-rich feeds and feeds with probiotics, fibres, etc. Immuno-nutrition using arginine, glutamine and polyunsaturated fatty acids has been evaluated in multiple studies and compared with standard feeding. A metaanalysis showed some benefit in mortality but not for prevention of infection, end-organ failure or inflammatory response. This benefit was not seen with the use of probiotics or fibre-based feeds. A systematic review did not show any benefit of immuno-nutrition or probiotics. It also showed that polymeric formulations are as well tolerated as oligomeric ones (elemental).
ERCP Induced Perforations
In the epoch of minimally invasive management of biliary and pancreatic disorders, endoscopic retrograde cholangiopancreatography (ERCP) combined with endoscopic sphincterotomy (ES) has become a prevalent procedure all over the world. Even though ES is a safe procedure, it carries a small but significant number of serious complications which include pancreatitis, bleeding, cholangitis and perforation. As per old literature, ERCP-related perforations were reported in 0.5–2.1% of sphincterotomies with a mortality rate of 16–18%. However, the improvement in the experience and skill of the endoscopy specialists combined with advancements in technology have reduced the incidence of perforation to <0.5% over the years. Sphincterotomy (56%) and guidewire manipulation (23%) are widespread causes of perforations related to endoscopic retrograde cholangiopancreatography (ERCP). There is a dearth of evidence-based strategies with respect to the proper management of ERCP perforations. While one set of investigators promote on-demand conservative and surgical management, based on a clinical course, the others support operative repair in all cases on account of the complications associated with the delayed operative intervention.
INDICATIONS OF SURGICAL MANAGEMENT
1. Large extravasation of contrast at the time of ERCP defined as incomplete dissipation of contrast after 1 min on follow-up plain film.
2. If there is only a small amount of contrast extravasation, where there is complete dissipation after 1 min of ERCP, on follow-up plain film, then a UGI with contrast injection on fluoroscopy is performed in 2–8 h. If this shows extravasation, we recommend surgical exploration.
3. Follow-up CT scan showing a collection due to perforation in the retroperitoneum or intraperitoneum.
4. Retained hardware unable to be removed by endoscopy along with perforation.
5. Massive subcutaneous emphysema.
6. Failure of conservative management.
A delay in diagnosis or in surgery will lead to death. The reason is that there is a massive autodigestion of body tissues which is due to a constant release of enzymes, and this eventually leads to sepsis. The principle of treatment by surgery is the same as endoscopic treatment. Any case that is suspected to have ERCP-induced perforation is kept nil by mouth, and the gastric contents are decompressed by Ryles tube and intravenous antibiotics.
This is done by diverting bile, enteric and pancreatic juices away from the site of perforation. However simple drainage will also cause the juices to flow through the perforation site and body cavities before draining out of the tubes. This could be avoided by diverting the juices through well-controlled different paths which could be done by the following procedures:
1. T-tube in CBD;
2. Placement of duodenostomy tube—lateral/end duodenostomy;
3. Duodenal diverticulization;
4. Pyloric exclusion;
5. Roux-en-Y duodenojejunostomy.
The disadvantage of using Roux-en-Y duodenojejunostomy is that if the edges are inflamed, then the sutures will not hold properly. However other procedures can be used even when the edges are inflamed. Even though duodenostomy appears to be simple, a part of gastric and duodenal contents pass across the perforation site.
Duodenal diverticulization involves three things: (1) tube to divert duodenal and pancreatic juice, (2) T-tube in CBD to divert bile and (3) distal
gastrectomy and Billroth II anastomosis to provide an alternate pathway for food and gastric juice, thereby preventing these from passing through the site of perforation. Although this procedure has been proved to be successful, it is less widely used due to its complex nature. Pyloric exclusion is a simpler form in which the pylorus is closed by purse string by long-standing absorbing sutures like PDS 2.0 instead of distal gastrectomy. Similar to duodenal diverticulization, T-tube drainage of the CBD and loop gastrojejunostomy are done. The duodenal perforation is closed over a duodenostomy tube.
Whenever there is collection which is localized to the retroperitoneum, retroperitoneal surgical approach can be carried out. Advantages of this procedure are (1) it permits gravitational drainage, (2) avoids septic complication of the peritoneal cavity, (3) directs retroperitoneal necrosectomy with post-operative washes and (4) avoids complex intra-abdominal surgeries. However the disadvantage of this procedure is that it can be used only for retroperitoneal-contained perforations.