LIFE AS A SURGEON

Life as a Surgeon
Surgical careers begin long before one is known as a surgeon. Medicine in general, and surgery in particular, is competitive from the start. As the competition begins, in college or earlier, students are confronted with choices of doing what interests them and what they may truly enjoy vs doing what is required to get to the next step. It is easy to get caught up in the routine of what is required and to lose track of why one wanted to become a doctor, much less a surgeon, in the first place. The professions of medicine and surgery are vocations that require extensive knowledge and skill. They also require a high level of discretion and trustworthiness. The social contract between the medical profession and the public holds professionals to very high standards of competence and moral responsibility. Tom Krizek goes on to explain that a profession is a declaration of a way of life ‘‘in which expert knowledge is used not primarily for personal gain, but for the benefit of those who need that knowledge.’’
For physicians, part of professionalism requires that when confronted with a choice between what is good for the physician and what is good for the patient, they choose the latter. This occurs and is expected sometimes to the detriment of personal good and that of physicians’ families. Tom Krizek even goes so far as to question whether surgery is an ‘‘impairing profession.’’ This forces one to consider the anticipated lifestyle. In sorting this out, it is neither an ethical breach nor a sign of weakness to allocate high priority to families and to personal well-being. When trying to explain why surgery may be an impairing profession, Krizek expands with a cynical description of the selection process. Medical schools seek applicants with high intelligence; responsible behavior; a studious, hard-working nature; a logical and scientific approach to life and academics; and concern for living creatures. He goes further to explain that in addition to these characteristics, medical schools also look for intensity and drive, but are often unable to make distinctions among those who are too intense, have too much drive, or are too ingratiating.
Medical School
There are many ethical challenges confronting medical students. As they start, medical students often have altruistic intentions, and at the same time are concerned with financial security. The cost of medical education is significant. This can encourage graduates to choose specialty training according to what will provide them the most expedient means of repaying their debt. This can have a significant, and deleterious, impact on the health care system in that the majority of medical graduates choose to pursue specialty training, leaving a gap in the availability of primary care providers. As medical students move into their clinical training, they begin interacting with patients. One concern during this time is how medical students should respond and carry on once they believe that a mistake on their part has resulted in the injury or death of another human being. In addition, the demands of studying for tests, giving presentations, writing notes, and seeing patients can be overwhelming. The humanistic and altruistic values that medical students have when they enter medical school can be lost as they take on so much responsibility. They can start to see patient interactions as obstacles that get in the way of their other work requirements. During their clinical years, medical students decide what field they will ultimately pursue. For students to make an informed decision about a career in surgery, they need to know what surgeons do, why they do it, and how surgery differs from other branches of medicine. It is important for them to be aware of what the life of a surgeon entails and whether it is possible for them to balance a surgical career with a rewarding family life.
Surgical Residency
Beginning residents are confronted with a seemingly unbearable workload, and they experience exhaustion to the point where the patient may seem like ‘‘the enemy.’’ At the same time, they must learn how to establish strong trusting relationships with patients. For the first time, they face the challenge of accepting morbidity and death that may have resulted directly from their own actions. It is important that residents learn ways to communicate their experience to friends and family, who may not understand the details of a surgeon’s work but can provide valuable support. The mid-level resident confronts the ethical management of ascending levels of responsibility and risks, along with increasing emphasis on technical knowledge and skills. It is at this level that the surgical education process is challenged to deal with the resident who does not display the ability to gain the skills required to complete training as a surgeon. Residents at this level also must deal with the increasing level of responsibility to the more junior residents and medical students who are dependent on them as teacher, organizer, and role model. All of this increasing responsibility comes at a time when the resident must read extensively, maintain a family life, and begin to put long-range plans into practice in preparation for the last rotation into the chosen final career path. The senior surgical resident should have acquired the basics of surgical technique and patient management, accepting nearly independent responsibility for patient care. The resident at this level must efficiently and fairly coordinate the functioning team, engage in teaching activities, and work closely with all complements of the staff. As far as ethics education is concerned, residents at this stage should be able to teach leadership, teamwork, and decision-making. They should be prepared to take on the value judgments that guide the financial and political aspects of the medical and surgical practice.
The Complete Surgeon
The trained surgeon must be aware of the need to differentiate between the business incentives of medical care and doing what is right for a sick individual. As financial and professional pressures become more intense, the challenge increases to appropriately prioritize and balance the demands of patient care, family, education, teaching, and research. For example, how does the surgeon deal with the choice between attending a child’s graduation or operating on an old patient who requests him rather than an extremely well-trained associate who is on call? How many times do surgeons make poor choices with respect to the balance of family vs work commitments? Someone else can
competently care for patients, but only parents can be uniquely present in the lives of their children. Time flies, and surgeons must often remind themselves that their lives and the lives of their family members are not just a dress rehearsal.
Knowing When to Quit
A 65-year-old surgeon who maintains a full operating and office schedule, is active in community and medical organizations, and has trained most of her surgical colleagues is considering where to go next with her career. Recently, her hospital acquired the equipment to allow robotic dissection in the area where she does her most complicated procedures. She has just signed up to learn this new technology, but is beginning to reflect on the advisability of doing this. How long should she continue at this pace, and how does she know when to slow down and eventually quit operating and taking the responsibility of caring for patients? Murray Brennan summarizes the dilemma of the senior surgeon well. The senior surgeon is old enough and experienced enough to do what he does well. He yearns for the less complicated days where he works and is rewarded for his endeavors. He becomes frustrated by restrictive legislation, the tyranny of compliance, and the loss of autonomy. Now regulated, restricted, and burdened with compliance, with every medical decision questioned by an algorithm or guideline, he watches his autonomy of care be ever eroded. Frustrated at not being able to provide the care, the education, and the role model for his juniors, he abandons the challenge.
Finishing with Grace
Each surgeon should continuously map a career pathway that integrates personal and professional goals with the outcome of maintaining value, balance, and personal satisfaction throughout his or her professional career. He or she should cultivate habits of personal renewal, emotional self-awareness, and connection with colleagues and support systems, and must find genuine meaning in work to combat the many challenges. Surgeons also need to set an example of good health for their patients. Maintaining these values and healthy habits is the work of a lifetime. Rothenberger describes the master surgeon as a person who not only knows when rules apply, recognizes patterns, and has the experience to know what to do, but also knows when rules do not apply, when they must be altered to fit the specifics of an individual case, and when inaction is the best course of action. Every occasion is used to learn more, to gain perspective and nuance. In surgery, this is the rare individual who puts it all together, combining the cognitive abilities, the technical skills, and the individualized decision-making needed to tailor care to a specific patient’s illness, needs, and preferences despite incomplete and conflicting data. The master surgeon has an intuitive grasp of clinical situations and recognizes potential difficulties before they become major problems. He prioritizes and focuses on real problems. He possesses insight and finds creative ways to manage unusual and complex situations. He is realistic, self-critical, and humble. He understands his limitations and is willing to seek help without hesitation. He adjusts his plans to fit the specifics of the situation. He worries about his decisions, but is emotionally stable.
Cystic Disorders of the Bile Ducts
 OVERVIEW
OVERVIEW
Cystic disorders of the bile ducts, although rare, are well-defined malformations of the intrahepatic and/or extrahepatic biliary tree. These lesions are commonly referred to as choledochal cysts,which is a misnomer, as these cysts often extend beyond the common bile duct (choledochus).
EPIDEMIOLOGY
Cystic disorders of the bile ducts account for approximately 1% of all benign biliary disease. Also, biliary cysts are four times more common in females than males. The majority of patients (60%) with bile duct cysts are diagnosed in the first decade of life, and approxi-mately 20% are diagnosed in adulthood.
CLASSIFICATION
Cystic dilatation of the bile ducts occurs in various shapes—fusi-form, cystic, saccular, and so on—and in different locations through-out the biliary tree. The most commonly used classification is the Todani modification of the Alonso-Lej classification.
ETIOLOGY
The exact etiology of biliary cysts is unknown.
CLINICAL PRESENTATION
The initial clinical presentation varies significantly between children and adults. In children, the most common symptoms are intermittent abdominal pain, nausea and vomiting, mild jaundice, and an abdom-inal mass. The classical triad of abdominal pain, jaundice, and a pal-pable abdominal mass associated with choledochal cyst is observed in only 10% to 15% of children, and it is rarely seen in adults. Symp-toms in adults often mimic those seen in patients with biliary tract disease or pancre-atitis.
SURGICAL MANAGEMENT
The definitive treatment of bile duct cysts usually includes surgical excision of the abnormal extrahepatic bile duct with biliary-enteric reconstruction. This approach relieves biliary obstruction, prevent-ing future episodes of cholangitis, stone formation, or biliary cirrho-sis and thus interrupting the inflammatory liver injury cycle. It also stops pancreatic juice reflux, and more importantly, it removes tissue at risk of malignant transformation.
Transanal Endoscopic Microsurgery for Rectal Tumors

Cancer of the rectum is the fifth most common form of cancer in adults worldwide. In 2012, an estimated 40,300 new rectal cancers will be diagnosed in the US with a median age 69 years. Five-year survival rates for rectal cancer are high for early stage disease (90% for Stage I disease) but drop significantly with worsening stage (7% for metastatic Stage IV disease). Recently, advances in neoadjuvant and adjuvant therapy have decreased the rate of local recurrence and improved long-term survival for some patients. Although the treatment for rectal cancer has become increasingly multimodal, surgical excision of the primary tumor remains essential for eradication of disease.
For a long time there has been a debate about the best surgical approach to early stage rectal cancer, whether treatment should involve radical excision (excision of the rectum) or local excision (tumor alone). Proponents of radical surgery argue that excision of the rectum with its surrounding lymphatic drainage offers the best chance for cure. On the other hand, advocates of local excision feel that a less-aggressive approach can avoid the potential ramifications of major pelvic surgery such as sepsis, poor anorectal function, sexual dysfunction, and difficulty with urination and can eliminate the potential need for a permanent stoma. Although the debate has gone back and forth on the adequacy of local excision, there is a growing body of scientific data that suggests that local excision can be sufficient in patients with early rectal cancer of the mid and distal rectum with good histologic features and preoperative imaging (computed tomography, magnetic resonance imaging, and endorectal ultrasound) that shows no evidence of lymph node involvement.
Traditionally, transanal excision has been performed with the conventional technique using traditional equipment. Although this conventional technique can give surgeons operative access to most distal rectal lesions, it can be difficult to conduct on mid-rectal tumors or in large patients with a deep buttock cleft. The technical difficulties experienced under such circumstances can lead to poor visualization, inadequate margins, or specimen fragmentation. In response to the technical limitations of conventional transanal excision, in the 1980s Professor Gehard Buess from Tubingen, Germany, began to develop the technique of transanal endoscopic microsurgery (TEM).

In collaboration with the Richard Wolf Company in Germany, Dr Buess developed the specialized instruments necessary to perform endoscopic surgery transanally. TEM was introduced into clinical practice in 1983, and was gradually implemented in several European countries and eventually introduced in North America and Asia. The last decade has witnessed international growth in the application of TEM yielding a significant amount of scientific data to support its clinical merits and advantages and also shedding some light on its limitations.
Câncer de Esôfago
Epidemiologia, Diagnóstico Precoce e a Complexidade do Tratamento Multimodal
Autor: Prof. Dr. Ozimo Gama
Categoria: Oncologia Cirúrgica / Cirurgia do Aparelho Digestivo
Tempo de Leitura: 9 minutos
CEC
Introdução
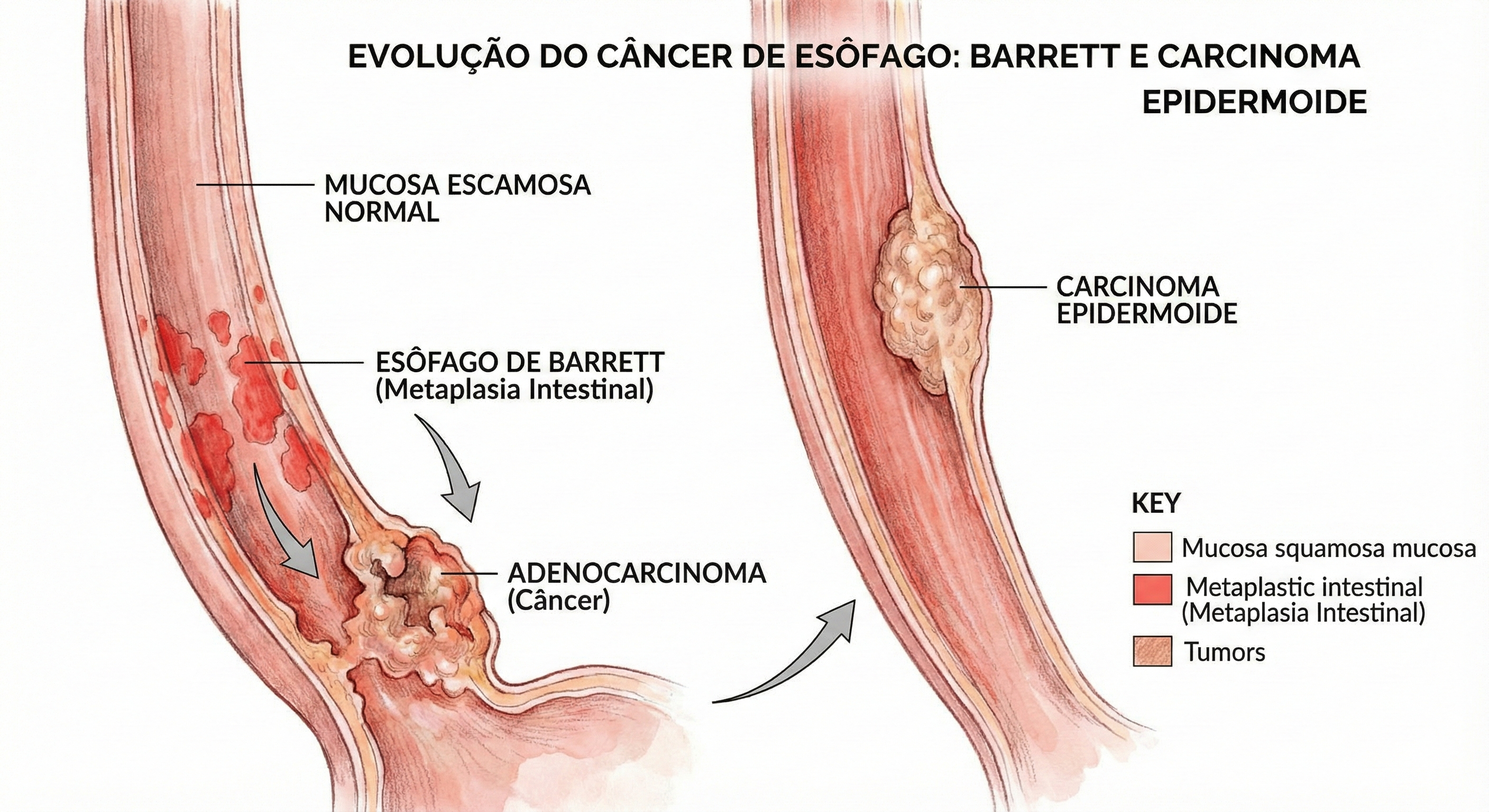
O esôfago, um tubo musculomembranoso de aproximadamente 25 a 30 centímetros, desempenha a função vital de transportar o bolo alimentar da hipofaringe ao estômago através de peristalse coordenada. Apesar de sua anatomia aparentemente simples, desprovida de serosa, este órgão é sítio de uma das neoplasias mais agressivas e desafiadoras para o cirurgião do aparelho digestivo: o câncer de esôfago. Esta patologia é caracterizada por sua latência clínica. Em fases iniciais, a doença é assintomática, o que retarda o diagnóstico e compromete o prognóstico. Para o estudante de medicina e o residente de cirurgia, compreender a dualidade histológica predominante — Carcinoma Epidermoide (CEC) versus Adenocarcinoma — e seus respectivos fatores de risco é fundamental para a suspeição clínica e o rastreamento adequado.
Epidemiologia e o Cenário Brasileiro
O câncer de esôfago é uma questão de saúde pública global, com alta incidência em regiões do “cinturão do câncer de esôfago” (que se estende da China ao norte do Irã). No Brasil, a doença mantém-se relevante e letal. Dados atualizados da Estimativa 2023-2025 do Instituto Nacional de Câncer (INCA) projetam cerca de 10.990 novos casos anuais no país. A incidência é marcadamente maior no sexo masculino, ocupando a 6ª posição entre os tipos de câncer mais frequentes nos homens (excetuando-se o câncer de pele não melanoma). Historicamente, o Carcinoma Epidermoide representa a grande maioria dos casos (cerca de 96% em séries históricas brasileiras), intimamente ligado ao tabagismo e etilismo. Contudo, observamos uma transição epidemiológica importante: o Adenocarcinoma distal tem apresentado um crescimento exponencial, impulsionado pela epidemia de obesidade e pela Doença do Refluxo Gastroesofágico (DRGE) que culmina no Esôfago de Barrett.
Fatores de Risco e Prevenção
A gênese do câncer esofágico é multifatorial, e a prevenção passa pela mitigação destes agentes:
- Tabagismo e Etilismo: A combinação destes dois fatores tem efeito sinérgico, multiplicando exponencialmente o risco para o tipo Epidermoide.
- Hábitos Alimentares: O consumo frequente de bebidas em temperaturas muito elevadas (comum em certas culturas regionais brasileiras) causa dano térmico crônico à mucosa. Dietas pobres em frutas e vegetais também são fatores predisponentes.
- Condições Precursoras:
- Acalasia: A estase alimentar crônica promove inflamação da mucosa.
- Tilose: Hiperqueratose palmoplantar associada a alto risco de CEC.
- Esôfago de Barrett: A metaplasia intestinal causada pelo refluxo ácido crônico é a lesão precursora do Adenocarcinoma.
- Outros: Síndrome de Plummer-Vinson, ingestão de cáusticos e infecção pelo HPV.
Quadro Clínico: O Desafio do Silêncio
O grande obstáculo no manejo do câncer de esôfago é a ausência de sintomas precoces. A distensibilidade da parede esofágica permite que o tumor cresça significativamente antes de causar obstrução. Quando sintomático, o paciente tipicamente apresenta:
- Disfagia Progressiva: Inicialmente para sólidos, evoluindo para pastosos e líquidos.
- Perda Ponderal: Frequentemente severa (>10% do peso corporal), devido à disfagia e ao catabolismo tumoral.
- Odinofagia e Dor Retroesternal: Indicativos de invasão local ou ulceração.
Propedêutica e Diagnóstico
O padrão-ouro para o diagnóstico é a Endoscopia Digestiva Alta (EDA) com biópsia.

CEC
Para o cirurgião e endoscopista, o uso de cromoscopia é vital. O Lugol é utilizado para corar o epitélio escamoso normal (rico em glicogênio), deixando áreas neoplásicas ou displásicas “não coradas” (amarelo-claras), facilitando a biópsia dirigida no Carcinoma Epidermoide. Já o Azul de Toluidina ou métodos digitais (NBI/FICE) auxiliam na detecção do Barrett e Adenocarcinoma precoces. O estadiamento deve ser rigoroso, utilizando Tomografia Computadorizada (tórax e abdome superior) e, idealmente, a Ecoendoscopia (Ultrassom Endoscópico) para avaliar a invasão da parede (T) e linfonodos regionais (N), além do PET-CT para exclusão de metástases à distância.
Abordagem Terapêutica: Multimodalidade
O tratamento depende estritamente do estadiamento e da localização tumoral (Cervical, Torácico ou Junção Esôfago-Gástrica).
- Doença Precoce (Tis/T1a): Pode ser passível de Ressecção Endoscópica (Mucosectomia ou ESD), preservando o órgão com taxas de cura elevadas (98%).
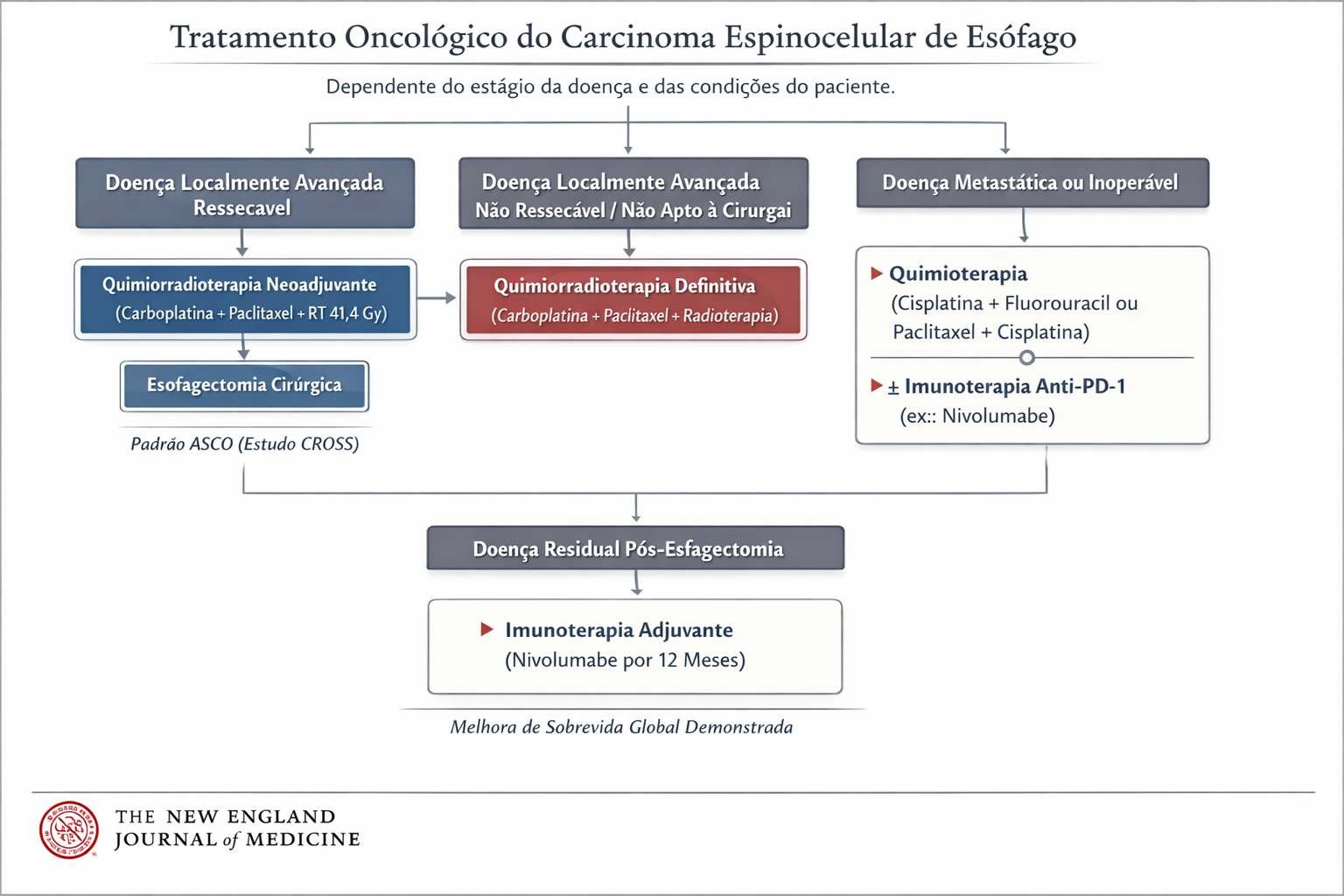
- Doença Localmente Avançada: A cirurgia isolada raramente é suficiente. O padrão atual envolve Terapia Neoadjuvante (Quimioterapia + Radioterapia pré-operatória) seguida de Esofagectomia com Linfadenectomia. A cirurgia é de alta complexidade, podendo ser realizada por via aberta, laparoscópica ou robótica (técnicas de Ivor Lewis ou McKeown).
- Doença Metastática ou Irressecável: O foco torna-se paliativo. A inserção de próteses autoexpansíveis (stents) endoscópicos restaura a via oral e a dignidade do paciente. A radioterapia e braquiterapia também desempenham papel no controle local da disfagia e sangramento.
Fluxograma
Pontos-Chave para a Prática Cirúrgica
- Rastreamento: Pacientes com DRGE crônico (há mais de 5-10 anos) ou sintomas de alarme devem ser submetidos a endoscopia para rastreio de Barrett.
- Anatomia: O esôfago não possui serosa, o que facilita a invasão precoce de estruturas mediastinais (traqueia, aorta, pericárdio).
- Diagnóstico: Disfagia em adulto deve ser investigada com EDA imediatamente; não assuma benignidade sem visualização direta.
Conclusão
O câncer de esôfago exemplifica a necessidade da medicina moderna ser multidisciplinar. O cirurgião do aparelho digestivo não atua isolado, mas em concerto com o oncologista clínico, o radio-oncologista e o endoscopista. O diagnóstico precoce continua sendo a arma mais poderosa; contudo, mesmo em estágios avançados, a evolução das técnicas cirúrgicas e das terapias adjuvantes tem oferecido novas perspectivas de sobrevida e qualidade de vida aos nossos pacientes.
“A abordagem cirúrgica do esôfago foi, até recentemente, uma história de frustração. (…) O esôfago é um órgão que tolera a cirurgia mal, exceto quando executada com precisão absoluta.” — Ivor Lewis (1946), cirurgião galês que revolucionou o tratamento do câncer de esôfago com a técnica de esofagectomia transtorácica.
Gostou ❔Nos deixe um comentário ✍️ , compartilhe em suas redes sociais e|ou mande sua dúvida pelo 💬 Chat On-line em nossa DM do Instagram.
Hashtags: #CancerDeEsofago #CirurgiaDoAparelhoDigestivo #Oncologia #Esofagectomia #MedicinaBaseadaEmEvidencias