Cholecystectomy is a common surgical procedure, with over 750,000 performed annually in the United States and 200,000 in Brazil. Popularized in the early 1990s, laparoscopic cholecystectomy (LC) is now considered the gold standard for routine cases of benign gallbladder and biliary pathology. LC has clear advantages over the traditional open approach, such as lower morbidity, less pain, and faster recovery. However, it is associated with a three to five times increase in bile duct injury (BDI). Major BDI can be a catastrophic complication, significantly increasing mortality. Additionally, patients who suffer a BDI often require further interventions, have a higher risk of additional complications, and experience a reduced quality of life. BDI is a common cause of legal litigation and remains one of the most frequent reasons for monetary compensation.
Correct Anatomical Identification The “classic injury” to the bile duct occurs when the common bile duct is mistaken for the cystic duct. This typically happens in the setting of severe acute or chronic inflammation, where the gallbladder may fuse to the lateral wall of the common hepatic duct, predisposing the surgeon to misidentify the biliary anatomy. This can result in a major BDI, where a segment of the common hepatic duct and bile duct is removed. Beyond this classic injury, other injuries to the biliary system can occur, such as sectional or segmental ducts disconnected from the liver with or without bile leakage, bile leakage from the cystic duct stump, long-term strictures due to thermal or iatrogenic damage, or combined vasculobiliary injuries.
Critical View of Safety (CVS) The Critical View of Safety (CVS), introduced by Strasberg et al. in 1995, is a method of safe anatomical identification that serves as a set of criteria to ensure the proper identification of the appropriate anatomy before ductal structures are ligated. These criteria include separating the lower end of the gallbladder from the liver to expose at least the lower third of the cystic plate, cleaning all fibrous and fatty tissue within the hepatocystic triangle, and seeing only two structures entering the gallbladder. The CVS mirrors the safe identification that occurs in traditional open cholecystectomy. While there are no level 1 data to support its use (due to the large sample size required to discriminate between an injury that occurs at a relatively low incidence), there is a body of literature of over 6000 cases where CVS was achieved without any major BDI.
Culture of Safety in Cholecystectomy (COSIC) Strict adherence to CVS is crucial to reducing BDI, but it is only part of the Culture of Safety in Cholecystectomy (COSIC), which requires that safety be at the forefront. Besides achieving CVS in total cholecystectomy cases, COSIC also requires proper patient selection and evaluation, adjustment of surgical technique in non-routine cases, use of bailout procedures, and avoiding complex cases when appropriate expertise is unavailable. The American Society of Gastrointestinal and Endoscopic Surgeons (SAGES) has developed a six-step program to enhance cholecystectomy safety:
- Understanding CVS and using it for identifying the cystic duct and artery.
- Considering an intraoperative pause before clipping or cutting any structure.
- Understanding aberrant anatomy.
- Liberal use of cholangiography or other intraoperative imaging means of the biliary system.
- Recognizing when dissection is approaching a significant danger zone and terminating the operation by a safe method, other than cholecystectomy, if the conditions around the gallbladder are too dangerous.
- Seeking assistance from another surgeon when conditions are difficult.
Bailout Procedures: When and How to Opt Deciding when to stop dissection of the hepatocystic triangle and opt for a bailout procedure rather than total cholecystectomy can be challenging. To make this decision before any biliary or vascular injury occurs, the surgeon must constantly ask: “Is it possible to safely achieve CVS?” When the answer is “No” or “I am not sure,” we recommend considering a bailout procedure. Early adoption of a bailout procedure is believed to reduce the difficulty of making this decision and avoid inadvertent injuries to the biliary system while trying to dissect in difficult and obstructed planes. It is essential always to remember that this operation is performed for benign pathology.
There are three clear bailout options in difficult cases:
- Stop the Operation (Stop, Drain, and Refer): Stopping the operation may conflict with the surgeon’s goal of “solving a problem,” but it should be considered and is a viable and safe option to avoid BDI. The patient should continue with a short course of antibiotics or even undergo postoperative drain placement and/or percutaneous cholecystostomy. A second attempt at cholecystectomy can be considered in 2–3 months.
- Surgical Cholecystostomy: The gallbladder’s fundus can be opened after placing a purse-string suture, the contents are aspirated, and a drainage catheter is placed in the gallbladder lumen. This method works as a temporary measure since definitive cholecystectomy will likely be necessary in 2–3 months.
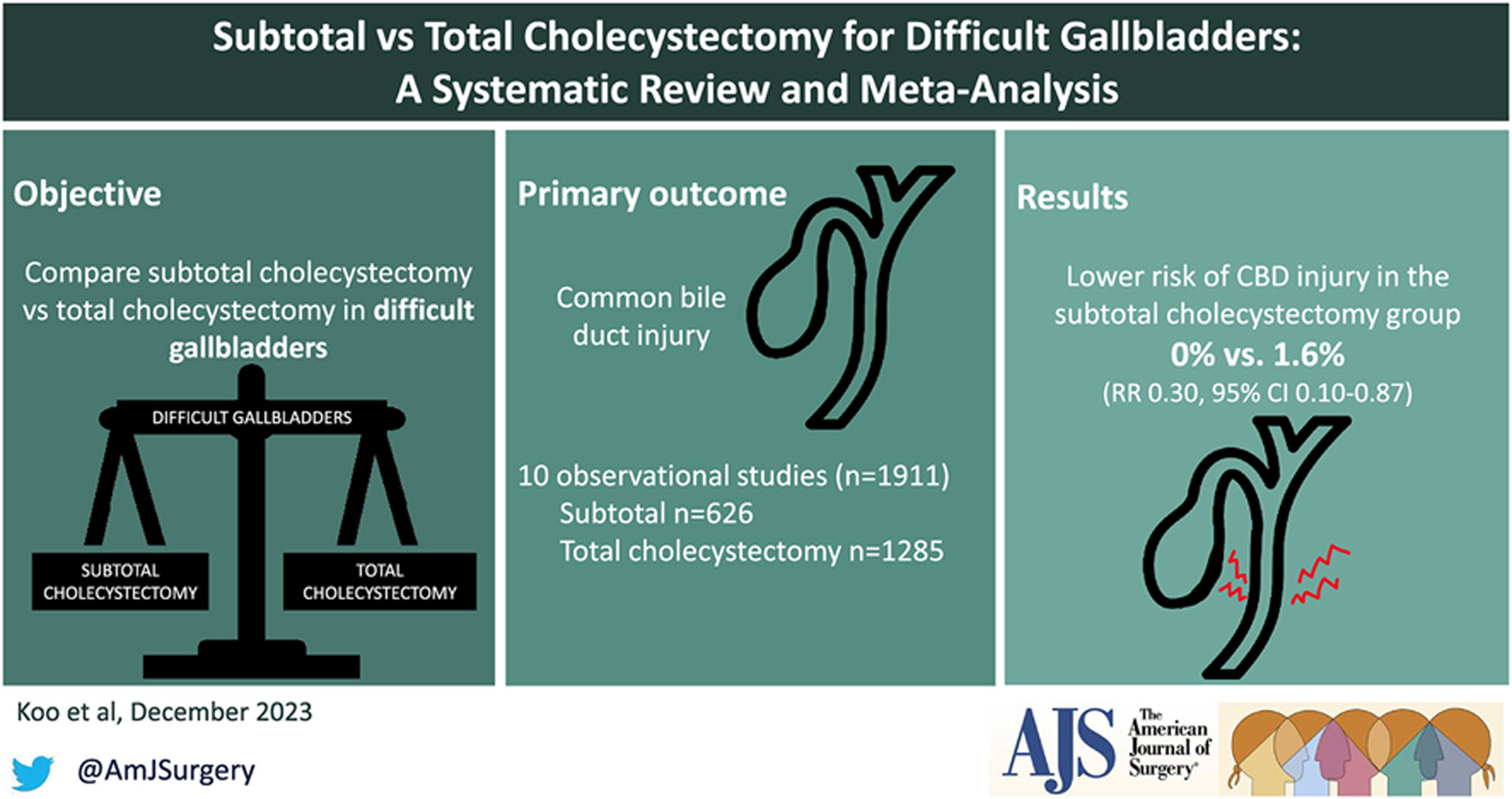
- Subtotal “Fenestrating” Cholecystectomy: Subtotal cholecystectomy has been a surgical option for over 100 years. In 2016, an attempt was made to define subtotal cholecystectomy into two distinct subtypes to allow for improved study and dissemination of the technique. When a new gallbladder remnant is created, this is called “reconstituting” subtotal cholecystectomy. When the gallbladder is left open with a remaining portion, this is called “fenestrating” subtotal cholecystectomy. Recent systematic reviews have demonstrated the safety of these procedures. Fenestrating subtotal cholecystectomy is recommended as the most definitive bailout procedure.
Once the decision is made to proceed with fenestrating subtotal cholecystectomy, the surgeon should consider their experience and either convert to an open procedure or continue laparoscopically. This procedure can be safely performed laparoscopically with minimal “advanced” laparoscopic maneuvers, but it can also be easily performed using an open technique.
Fenestrating Subtotal Cholecystectomy Procedure The first step involves incising the anterior (peritonealized) wall of the gallbladder at the fundus. By initially leaving the gallbladder body intact, its contents can be evacuated more easily. It may be advisable to place a surgical sponge or “endobag” under the gallbladder to facilitate catching any stones that might spill upon opening. The incision should continue towards the infundibulum, removing most of the anterior wall of the gallbladder. A very important consideration of this technique involves leaving a portion of the anterior infundibulum wall intact to avoid inadvertent entry into the hepatoduodenal ligament. Once most of the anterior wall is removed and the gallbladder contents, including all stones, are evacuated, the internal aspect of the gallbladder can be examined. It is essential to identify whether continuous biliary drainage from the gallbladder is present. In most “difficult” gallbladders requiring fenestrating subtotal cholecystectomy, the cystic duct is obliterated and does not require formal ligation. However, in the rare instances where the duct is patent and bile continues to drain from it, the internal orifice of the cystic duct should be closed with non-permanent sutures from the internal aspect of the gallbladder. At no point should external ligation of the cystic duct be attempted, which could potentially injure the bile duct. A drain should be left in the hepatorenal recess. No drain is needed inside the gallbladder lumen. The drain should be monitored for biliary drainage. Although generally rare, if a postoperative biliary fistula occurs, standard management should proceed. Routine postoperative endoscopic sphincterotomy is not recommended unless the biliary fistula is persistent, as most of them are self-limiting.
The main goal of laparoscopic cholecystectomy is “safety first, total cholecystectomy second.” While most laparoscopic cholecystectomies are straightforward, the surgeon must always keep this safety culture at the forefront and remain vigilant to anticipate dangerous situations. COSIC will help minimize (or eliminate) BDI and assist the surgeon in managing difficult operating conditions or clinical scenarios. Safe management of the difficult gallbladder is possible with operational adjustments and liberal use of bailout procedures, specifically fenestrating subtotal cholecystectomy.











[…] um sinal de fracasso ou imperícia, mas como uma manobra tática de extrema sabedoria cirúrgica (bailout procedure) para garantir a segurança e a vida do […]
[…] Momento de Parar (Bailout Procedures): Em casos de colecistite aguda severa, síndrome de Mirizzi ou fibrose intensa (vesícula […]
[…] o cirurgião reconheceu a “vesícula difícil” e utilizou manobras de bailout (subtotal, fundo–primeiro, conversão, […]