MANAGEMENT
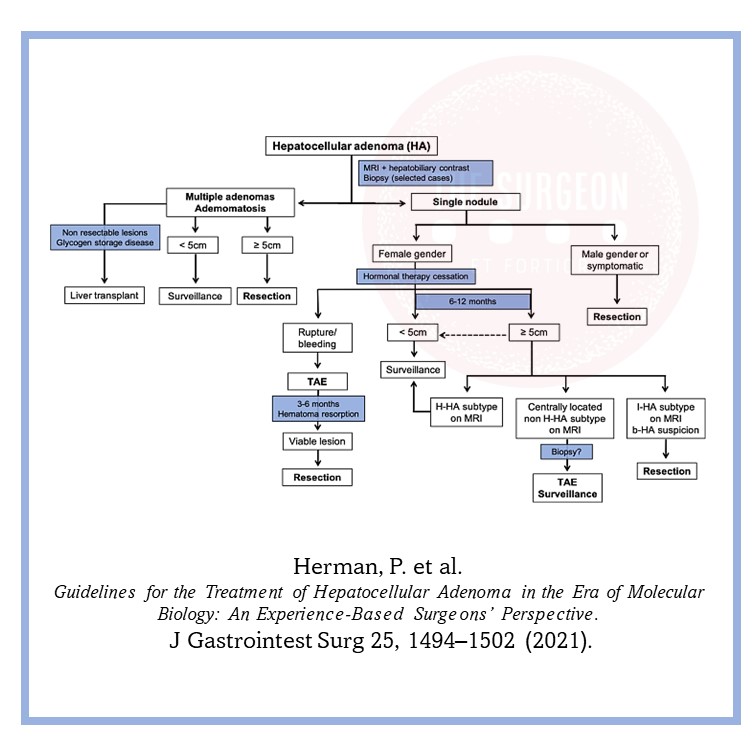
At a minimum, cessation of exogenous hormones is recommended, followed by serial imaging, as these lesions will shrink when the inciting hormone has been removed. In general, to obtain either CT or MRI every 6 months for the first 2 years and then once annually for lesions that we are following. Intervention is dictated by the risk of hemorrhage and malignant transformation, which is directly correlated to size. Hepatocellular carcinoma is seen in 5% of patients with lesions exceeding 8 cm. The rate of rupture is strongly associated with size > 5 cm.
Surgical resection is recommended for lesions ≥ 5 cm, those that are enlarging, those for which malignancy cannot be excluded, and those that are symptomatic. Additionally, adenomas in men, regardless of size, and especially those that are associated with anabolic steroid use, those with glycogen storage disease, and those that harbor ß-catenin mutations should also be given serious consideration for surgical extirpation.
Pregnant women with HA pose a management challenge. Since adenomas respond to hormones, they can increase in size with pregnancy and thus put the patient at risk for rupturing and bleeding. For women who would like to become pregnant, close monitoring without discouraging the patient’s wish is
recommended for lesions < 5 cm. However, for those patients with lesions > 5 cm or those who had complications from the adenomas from previous pregnancies, we recommend surgical resection prior to proceeding with the pregnancy. In situations where HA is discovered during pregnancy, we recommend close monitoring for lesions < 5 cm. However, for lesions > 5 cm, surgical resection should be considered during the second trimester but delayed in the third trimester since surgical intervention during this trimester is fraught with complications.